
Abstract
Background:
Many autistic adults are interested in having more and better-quality friendships and dating relationships, but there are too few evidence-based interventions that support building healthier peer relationships. Healthy Relationships on the Autism Spectrum (HEARTS) is a six-session, online class codeveloped with autistic people and co-delivered by teams that include at least one autistic expert who operates from the core idea that autistic people can be their authentic selves and can create and maintain healthy, supportive, mutual intimate partnership and friendship relationships.
Methods:
This preregistered randomized controlled trial study investigated the effects of HEARTS for autistic individuals aged 18 years old and older. Autistic individuals (N = 92) were randomly assigned to either HEARTS or an active control condition (ACC). The purpose of this study was to find out if the HEARTS class had an impact on participants’ self-directed relationship satisfaction goals, social motivation, experiences with aggressive acts in dating relationships, attitudes toward rejection, or hostile automatic thoughts 12 weeks after the HEARTS class ended.
Results:
Compared with the ACC group, participants in HEARTS showed statistically significant improvement in relationship satisfaction. There were no improvements in experiences with aggressive acts in dating relationships, social motivation, hostile automatic thoughts, or rejection sensitivity.
Conclusions:
HEARTS is feasible to implement and was generally well-received by the community as well as effective for improving relationship satisfaction.
Community Brief
Why is this an important issue?
Many autistic adults want to date, have friends, and have better relationships with friends, intimate, and sexual partners. Healthy relationships information that was designed with input from autistic people is rare, as are classes that are taught to autistic people by autistic people. The Healthy Relationships on the Autism Spectrum, or HEARTS, program was designed by autistic and non-autistic people together and is delivered online by pairs of autistic and non-autistic experts.
What was the purpose of this study?
The purpose of this study was to find out if the HEARTS class had an impact on participants’ relationship satisfaction, social motivation, experiences with aggressive acts in dating relationships, attitudes toward rejection, or hostile automatic thoughts.
What did the researchers do?
The researchers divided a group of 92 autistic individuals into two groups. Half (n = 44) received the HEARTS intervention, and half (n = 48) attended an online discussion group, which was the “control” condition. The researchers collected data before the online groups began and 12 weeks after the groups began.
What were the results and conclusions of the study?
Participants in HEARTS showed greater improvement in relationship satisfaction compared with those in the control condition. However, participants in HEARTS did not show improvement in social motivation, experiences with aggressive acts in dating relationships, hostile automatic thoughts, or rejection sensitivity compared with the people in the control group.
What is new or controversial about these findings?
HEARTS may be able to help autistic adults who want to improve relationships and feel more satisfied with them.
What are potential weaknesses in the study?
The study did not test whether HEARTS worked better than nothing at all. The study tested whether HEARTS worked better than an online discussion group, which was similar to HEARTS. Since the online discussion group worked well for autistic people, the added benefits of HEARTS may be relatively small compared with the benefits of an online discussion group.
How will these findings help autistic adults now or in the future?
These findings will help autistic adults decide if they want to participate in the HEARTS class. The findings also help researchers think about how HEARTS or similar interventions can be improved for autistic participants.
Background
Many autistic adults are interested in having more and better-quality friendships and dating relationships (“peer relationships” herein),1–3 but there are too few evidence-based interventions that support building healthier peer relationships. Healthy relationships are ones that make people feel supported, respected, and are mutual, compared with unhealthy relationships, which may be abusive, controlling, manipulative, or toxic.4,5 Healthy peer relationships can buffer against anxiety and depression for autistic people,6–9 even though navigating them can cause stress because of the stress posed by social interaction. 10 As many as 60% of autistic people are dissatisfied with the number of friends that they have compared with 18% of non-autistic people. 3 A recent analysis involving data from 220,000 U.S. college students found that only 24% of autistic students had intimate partners, compared with 46% of non-autistic students, 11 even though autistic people are as likely as non-autistic people to want sexual and romantic relationships. 1 Importantly, social isolation and its sequelae, which can include depression, anxiety, and suicidality, have been identified as substantive problems for autistic adults—and thus a current priority to address. 12
There are multiple reasons why autistic adults tend to have fewer peer relationships than they might wish. Autistic people experience social interaction challenges due to stigma, 13 discrimination, 14 noninclusive environments and cultural norms, 15 social communication differences, 16 reduced sensitivity to social rewards,17,18 alexithymia, 19 and lack of access to support.15,20 The risks for these adverse social experiences are exacerbated by the fact that autistic people do not receive sufficient information about making and keeping friends or dating partners, or how to stay safe from interpersonal abuse, through school. Nearly all U.S. K–12 schools (83%) offer social and emotional skills programming, 21 but the curricula taught in mainstream schools are not always adapted to be relevant and accessible for autistic people, and many autistic students may find it challenging to apply the lessons to their own social experiences.22,23
Experiences of being bullied, socially rejected, or physically, emotionally, and sexually victimized make it more difficult for people to want to remain open to new relationships or to put effort into developing new social connections.24,25 One logical consequence of being rejected is developing rejection sensitivity or hypervigilance toward social cues that might signal rejection and the interpretation of ambiguous social cues as signs of rejection, triggering social withdrawal. 26 Autistic people are more likely than non-autistic people to experience rejection sensitivity. 27 Another logical consequence of experiencing repeated rejection or victimization is to ascribe negative intent to others even when no ill-will is intended, which has been called hostile attribution bias in the research literature, 28 and may disproportionately affect autistic people.29,30 Hostile attribution bias makes it more difficult to make or keep friends or dating partners.31,32 Moreover, the expectation that other people are likely to be rejecting or hostile may be part of the reason that autistic people tend to experience lower social motivation than non-autistic people,33,34 which leads to fewer social relationships.
While there are some social skills groups for youth that have attempted to address some of the aforementioned issues, education about healthy relationships may be uniquely beneficial. While the term “social skills” is generally used to refer to interaction and communication skills such as turn taking in conversation, 35 making eye contact, 36 and making small talk, 37 healthy relationships skills pertain to distinguishing abusive and controlling behavior from supportive behavior, setting boundaries, resolving conflict, and expressing affection in mutually acceptable ways.38,39 A recent systematic review of healthy relationship programming for autistic people found that there are only three curricula that are evidence based, including Supporting Teens with Autism on Relationships, Tackling Teenage Training, and Peers Engaged in Effective Relationships-Decision Making. All three of these programs were designed for autistic adolescents rather than adults. 40 Therefore, a notable gap exists in services and support for autistic adults pertaining to healthy relationships education, which is exacerbated by the more general loss in services (e.g., “service cliff”) that affects autistic adults. 41
Previously, our team conducted a small, one-arm pilot test of an online healthy relationships class for autistic adults called Healthy Relationships on the Autism Spectrum (HEARTS). 42 The content of the class was informed by formative research with 25 autistic individuals and developed collaboratively by two non-autistic interventionists and seven autistic individuals. 43 The pilot found statistically significant improvement from the baseline pretest to 3-month follow-up on variables that included hostile automatic thoughts, experiences with aggressive acts in dating relationships, flourishing, coping with rejection and jealousy, social motivation, self-compassion, and positive thinking, although interpersonal competence and loneliness did not change. 42
The present study was designed to evaluate the effect of HEARTS in a larger and more diverse sample through a two-arm, experimental design with an active control condition (ACC). Unlike the prior feasibility test, this randomized controlled trial (RCT) included randomization to one of two conditions, included more participants, and investigated two outcomes that were assessed through independent evaluators who interviewed participants, whereas the prior feasibility test relied solely upon self-reported survey data. The specific hypotheses (H) tested were: The majority of HEARTS participants will attend ≥4 of the 6 class sessions. The HEARTS content will be delivered with fidelity and the HEARTS participants will rate the content as acceptable. Those in the HEARTS condition will experience greater reductions in hostile automatic thoughts, rejection sensitivity, experiences with aggressive acts in dating relationships at follow-up compared with those in the ACC, and greater increases in relationship satisfaction and social motivation compared with those in the ACC.
Methods
Design and setting
This two-site, two-arm RCT was conducted by researchers at Boston University and University of Alabama and preregistered (Clinical Trials Identifier NCT05608083). All procedures were reviewed and approved by the Institutional Review Board at Boston University. Autistic participants were randomly assigned to receive either HEARTS or the ACC and then crossed over to receive the other condition after data collection was finished. Thus, all participants had the opportunity to receive both treatment conditions. The goal was to recruit 60 individuals, which we exceeded. Based on social motivation scores from the feasibility study, we determined sample size of given two study arms, with each HEARTS class comprising 20 individuals. We estimated that we would have 80% power to detect a medium effect size (Cohen’s d = 0.65).
Recruitment and eligibility
Autistic participants in this research study were recruited between July 2023 and July 2024. All research study participants were recruited from the pool of individuals who registered for a 12-week online class that they were told would involve 6 weeks of the HEARTS curriculum and 6 weeks of a discussion group. The class was offered to the public by the Association for Autism and Neurodiversity (AANE), which is a U.S.-based not-for-profit organization that provides autistic individuals, families, and professionals with online and in-person education, community, and support. AANE advertised for the study via their existing membership roster and using their standard public-facing methods, and the research team also advertised the class on social media and using their own prior research databases. Individuals who registered for the 12-week class paid $0–150, to AANE, for the class, using a sliding scale. Once individuals were registered, they were then emailed research-related information and a research consent form and invited to participate in a one-on-one online interview with a member of the research team. During the intake interview, those who met the research eligibility criteria were invited to take part in the research. People had the option of participating in the class without research involvement. Inclusion criteria were: (1) ≥ 18 years old; (2) proficient in English; (3) diagnosed with autism by a health care provider or other professional; (4) willing to be randomized; and (5) not having participated in the HEARTS class previously. Being actively suicidal was an exclusion criterion because HEARTS was not designed to provide safety to those in crisis. In total, 129 individuals were assessed for research eligibility (see Fig. 1). Research participants were remunerated based on the number of surveys or assessments that they completed and could earn up to $300 for completing all of them.
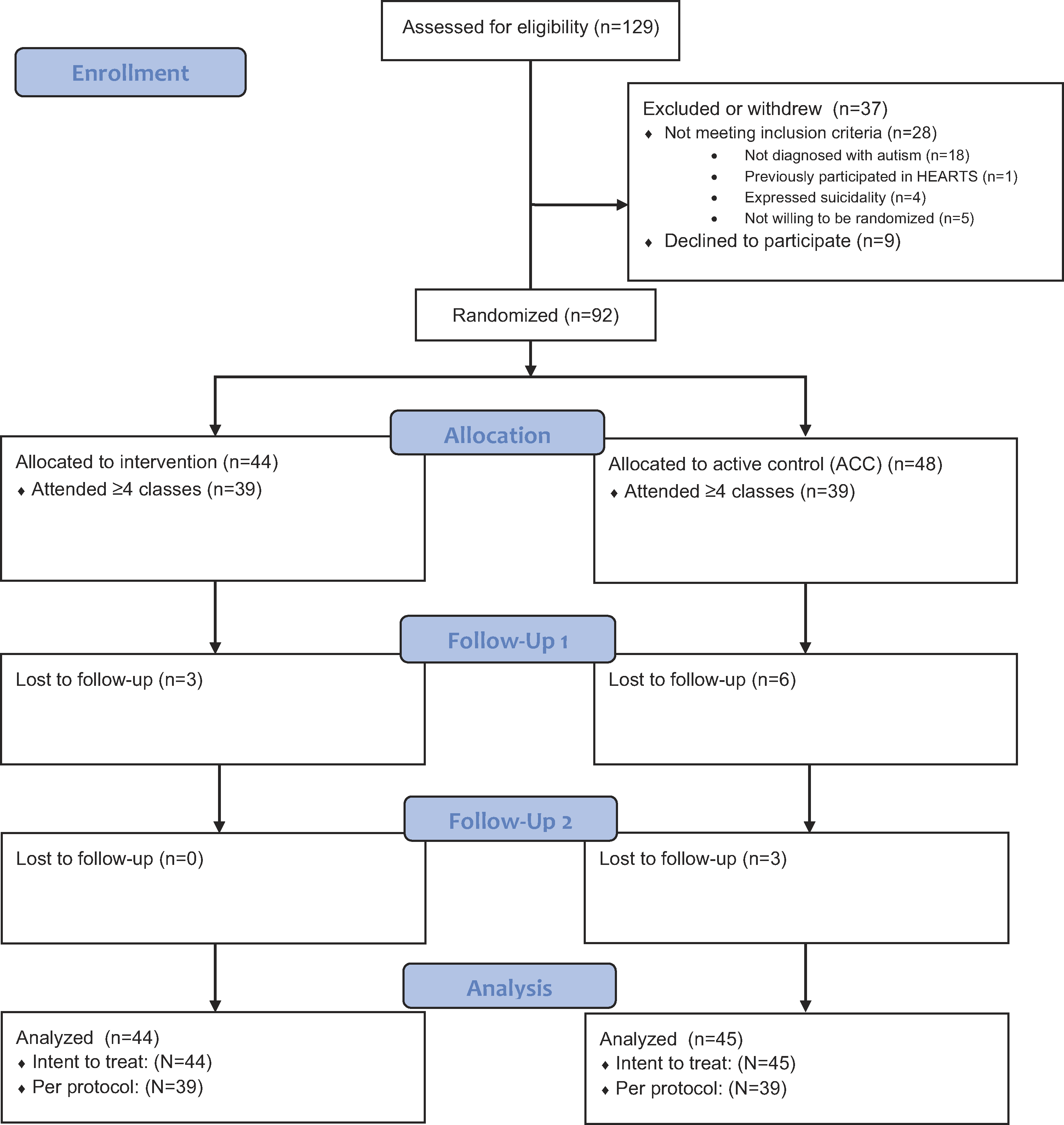
CONSORT diagram of enrollment, allocation, follow-up, and analysis.
Randomization
The 92 eligible individuals who agreed to participate in the research were stratified based on sex assigned at birth and randomly assigned to one of two conditions. The first condition, “HEARTS,” involved receiving the 6-week HEARTS intervention first (i.e., the intervention group), participating in data collection related to the study, and then taking part in a 6-week discussion group after research participation ended. The second condition, “ACC,” involved receiving 6 weeks of a discussion group first, participating in data collection related to the study, and then engaging in the 6-week HEARTS program after research participation concluded. The REDCap randomization module assigned participants without investigator input. 44 Investigators were not naïve to random assignment, but the independent evaluators who conducted baseline and follow-up interviews (i.e., to assess relationship satisfaction using the Clinical Global Impressions-Severity/Improvement [CGI-S and CGI-I] and to assess social motivation using the Autistic Social Health Interview [ASHI]) were naïve to participants’ condition. The study’s design required offering two sections of the class on the same day of the week at the same time, each taught by different sets of teachers. This setup allowed us to randomly assign interested students to either section without causing inconvenience. Among those eligible and willing to participate in the research, 44 were assigned to HEARTS and 48 were assigned to ACC. Sample characteristics are described in (Table 1).
Demographic Characteristics of the Sample (N = 92)
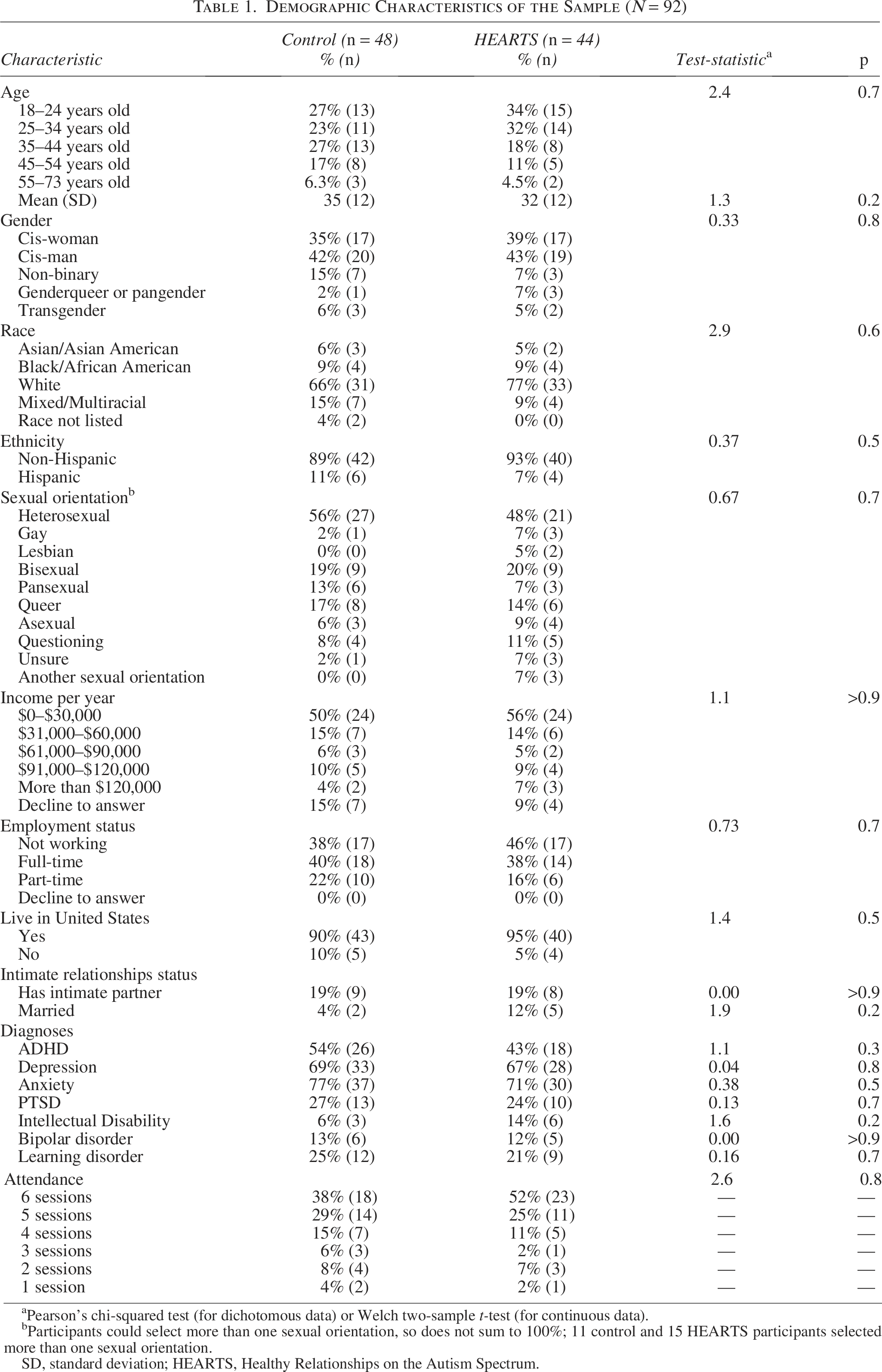
Pearson’s chi-squared test (for dichotomous data) or Welch two-sample t-test (for continuous data).
Participants could select more than one sexual orientation, so does not sum to 100%; 11 control and 15 HEARTS participants selected more than one sexual orientation.
SD, standard deviation; HEARTS, Healthy Relationships on the Autism Spectrum.
Intervention procedures
An outline of the HEARTS content is presented in Table 2. The development of the HEARTS intervention is described in detail elsewhere. 43 In brief, HEARTS was designed as an online psychoeducational class for autistic adults to be delivered by a pair of teachers, one of whom is autistic and one of whom is non-autistic and a relationships expert.
Weekly Outline of Healthy Relationships on the Autism Spectrum Group Sessions and Basis for Fidelity Scoring
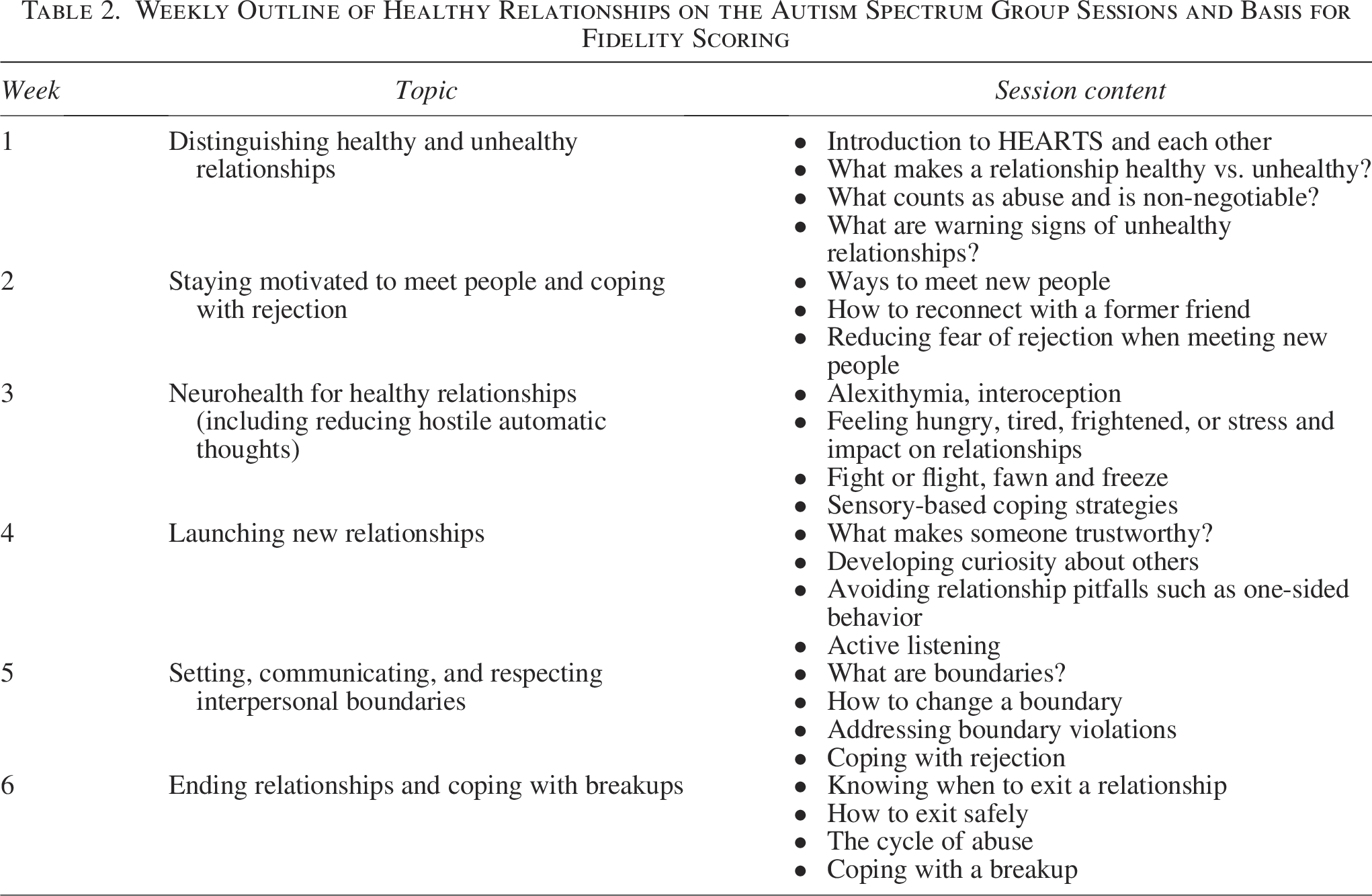
HEARTS was manualized and is available as a set of slide decks. The slide decks cover the following topics: (1) Healthy versus Unhealthy Relationships; (2) Staying Motivated to Meet People and Coping with Rejection; (3) Neurohealth for Healthy Relationships (including reducing hostile automatic thoughts); (4) Launching Relationships; (5) Boundaries; and (6) Ending Relationships and Coping with Breakups (Table 2). Classes were once per week for 90 minutes. Classes use a mixture of teaching strategies, including discussions, card sorting, brainstorming, and didactic presentation of material. The slide decks were shared with participants several days before each class session, so they could familiarize themselves with the material in advance.
This RCT involved three rounds of HEARTS/ACC group implementation. Each time HEARTS was implemented it was taught by a pair of teachers, one autistic and one non-autistic. Teachers were recruited through the social networks of the first author, E.F.R. In total, our pool of teachers included three autistic people and two non-autistic people. Qualifications for teachers, whether autistic or non-autistic, included: (1) having experience using dating apps or dating websites to meet a potential dating partner, (2) comfort discussing polyamory, kink, same-sex sexuality, pornography, and asexuality, (3) a commitment to anti-racist, anti-ableist, and gender and sexual minority supporting practice; (4) experience making one or more friends; (5) experience ending one or more friendships; (6) experience falling in love; (7) experience ending a serious intimate relationship; (8) experience facilitating online group discussions or classes; and (9) familiarity with Zoom. All teachers participated in a 4-hour training with the first author who had extensive prior experience facilitating healthy relationships groups online for autistic participants. The two non-autistic teachers were people who had worked in community domestic violence programs for more than a decade and had also previously collaborated closely with E.F.R. Two of the three autistic teachers had taught HEARTS previously in the prior feasibility test phase, and the third was an autistic HEARTS participant who displayed leadership qualities and stepped in to the teaching role when one of the original HEARTS teachers could no longer participate. A fidelity monitor attended each intervention session and noted if the class covered each subtopic as planned.
Active control condition
The ACC was an online discussion group that, consistent with trial methodology guidance, was structurally equivalent to HEARTS, to isolate impacts due to HEARTS core elements.45,46 The ACC convened once per week for 90 minutes. Topics covered during the 6 weeks of the ACC included discussions of where in the world people would enjoy traveling, hidden talents, hobbies, favorite animals, fictional characters people would like to meet, and favorite movies and TV shows. Each session was co-facilitated by two teachers (one autistic, one non-autistic). ACC groups were informed that discussion about healthy relationships information was off-limits. A fidelity monitor attended each ACC session and made a note of instances when healthy relationships topics were raised and whether it might have contaminated the ACC.
Intervention fidelity
Fidelity was rated in two ways. First, we scored each session to determine if the content was presented as intended. Trained research assistants were present in each session of HEARTS to assess adherence of the HEARTS facilitators to the curriculum and to ensure that ACC sessions did not include essential content from HEARTS (e.g., content on healthy relationships). Fidelity to the curriculum was assessed in all sessions using a three-point rating scale for planned session activities (i.e., 1 = skipped this activity, 2 = partially completed, 3 = completed). Second, we scored each ACC session to determine if it was free of healthy relationships topics, to avoid contamination. For ACC sessions, fidelity monitors used a three-point rating scale to score whether essential elements of the HEARTS curriculum were addressed or raised by the group leaders (i.e., 1 = not brought up, 2 = brought up in a minor way, 3 = extended discussion on topic).
Intervention content acceptability
Participants in the HEARTS sessions were sent a brief survey each week after class to rate their satisfaction with the activities that took place during that session. Specifically, they were sent a survey question that said: “We are interested in finding out how useful you thought each class activity was today. When we say ‘useful,’ we mean to encapsulate these ideas: was it educational, helpful, interesting, meaningful, pleasant, and enjoyable? You can rate each item on a scale from 1 to 10, where 1 means it was not at all useful, and 10 means it was very useful.” Across the six sessions of HEARTS, participants scored a total of 29 activities. In addition, at the end of the six sessions, participants were asked about their overall satisfaction with HEARTS and to score it on a scale from 1 to 10 in terms of whether it was informative, enjoyable, and whether they would recommend it to other people. Participants in the ACC did not score the utility or acceptability of the discussion group activities.
Outcome 1: Relationship satisfaction
Relationship satisfaction was assessed using the interview on CGI-S and CGI-I, 47 a measure that has been used in prior studies with autistic individuals.48,49 The final author trained two evaluators on the CGI using established procedures. Training included didactic training and assigned readings, and then independent coding of three training vignettes. The evaluator was considered reliable when their scores were within one point of the final author’s training scores, and the final author co-coded live the first interview of each evaluator in this trial. During the trial, the two evaluators independently coded five live interviews and had 100% agreement on codes. These same two clinical evaluators completed the CGI with all participants.
The CGI focused on each participant’s subjective satisfaction with their interpersonal relationships. For example, CGI-S questions that participants were asked at baseline included: “Tell me about how things have been going for you with respect to your interpersonal relationships,” and “In general, is your social life how you want it to be?” The CGI-I interview at T2 involved repeating these questions, and the evaluator assessed improvement since baseline. Specifically, the evaluator answered the question: “Compared to the person’s condition at baseline, how much has the person changed?” Evaluators selected one of seven response options that ranged from “very much worse” (7) to “very much improved” (1). 47 CGI-I scores of 1, 2, or 3 (corresponding to “very much,” “much,” or “minimally” improved) at T2 were considered treatment responders.
Outcome 2: Social motivation
Social motivation was assessed via the ASHI, an adaptation of the Social Motivation Interview, 50 which has been used in prior studies with young autistic people. It was adapted to ensure appropriateness for autistic adults with input from the autistic advisory board for the present study. The ASHI assesses the following dimensions of social health: person’s satisfaction with their interpersonal relationships, motivation to socialize, quantity of social relationships and encounters, and willingness to persist in social interaction. Two experienced independent evaluators, naïve to treatment condition, conducted ASHI assessments at baseline and after 3 months (T2). One of the evaluators was a licensed clinical psychologist. The second was a bachelor’s degree-level coordinator. During the interview, the interviewer inquired about behaviors over the prior 2 weeks. The total ASHI score can range from 0 to 24, with higher scores indicative of greater overall social health. Each participant received an ASHI score at baseline and a second ASHI score at T2.
Outcome 3: Experiences with aggressive acts in dating relationships
To assess involvement in unhealthy dating relationships, participants completed a 14-item self-report survey that asked them about both victimization and perpetration of dating abuse in the past 3 months. We used the short version of the Measure of Adolescent Relationship Harassment and Abuse, 51 which has been used in prior studies with autistic people.42,52 Participants were asked if they dated, hooked up with, or were in a romantic relationship with anyone in the past 3 months. Those who responded yes were then asked if they had experienced, or done, seven behaviors. These included, for example, “I hit, punched, kicked, or choked them,” and “They slapped, pushed, shoved or shook me.” Participants responded yes, no, or prefer not to answer for each item. Those who responded yes to any item were classified as having been involved in an unhealthy dating relationship. The Cronbach’s alpha in the present sample at baseline was α = 0.87.
Outcome 4: Hostile automatic thoughts
Hostile automatic thoughts (HATs) are negative thoughts about other people that include aggression, revenge, or represent having a negative attitude toward others as a default, rather than a pro-social or positive orientation. The HAT scale (Snyder et al., 1997) asks participants to respond to a series of items such as “This person is a loser,” and “I have to get revenge on this person” according to how frequently they had that thought or one similar in the past week using a Likert-type scale where a value of 1 indicates “not at all,” 2 indicates “sometimes,” 3 indicates “moderately often,” 4 indicates “often,” and 5 indicates “all the time.” The original scale included 29 items, 53 but for the present study four items were removed because of ethical concerns (e.g., “I want to kill this person” and “If I could get away with it, I’d kill this person”). We created a summary score by adding the values of responses to items 1 through 25, using item level within person imputation for missing values. The lowest possible score was a 25, and the highest possible score was 125. A higher score represents more HATs. The Cronbach’s alpha in the present sample at baseline was α = 0.96. The HATS has been used in a prior study with autistic people. 42
Outcome 5: Rejection sensitivity
Rejection sensitivity is the expectation of being socially rejected by others. We adapted the Rejection Sensitivity Questionnaire (RSQ), 54 which had also been used in this form in a prior study with autistic people. 42 The original RSQ is an 18-item self-report measure that was developed from interviews with undergraduate students in the early 1990s, and many items are not relevant to the HEARTS context such as borrowing notes in class. We therefore created a new version for our context. Sample items include: “I put up a profile on a dating website but nobody messages me,” and “I send a text message to a person I met but I never hear back from them.” The measure presents participants with 10 scenarios. For each scenario, participants rate (1) how worried they would be that they caused the rejection (i.e., the concern score), and (2) how likely they think it is that they are disliked (i.e., the expectation score). For example, a scenario is: “I ask a friend to get together and hang out but they say they are too busy.” The participant is then asked to use a scale of 1 to 6 to rate how concerned they are that it is their fault, where 1 is not at all concerned and 6 is very concerned. Next, the participant is asked how likely it is that the friend doesn’t like them anymore on a scale from 1 (very unlikely) to 6 (very likely). The concern score is multiplied by the expectation score for each situation. A total score is computed by summing each of these 20 scores. We used item level within person imputation for missing values. The lowest possible score was 20, and the highest possible score was 720. A higher score represents more rejection sensitivity. The Cronbach’s alpha in the present sample at baseline was α = 0.95.
Statistical analysis
The analyses were conducted using R version 4.4.3 on Boston University’ s shared computing cloud. First, we checked the data distribution and ensured that the necessary assumptions were met for linear mixed-effects models. Each outcome had less than 10% missing data, and we used person-mean imputation for item-level missingness in the measures to calculate the overall scores. We also explored using multiple imputation, but doing so had no effect on results, and the use of multiple imputation involves uncertain assumptions in a randomized study with repeated measurements. We used the Last Observation Carried Forward (LOCF) method for imputation. 55 Separately, and not shown, we also conducted per-protocol (PP) analyses limited to individuals who attended four or more of their assigned sessions, using LOCF with the PP analysis, but results were unchanged from the Intent to Treat (ITT) analysis. Participant satisfaction data were analyzed and presented as mean scores with standard deviations (SDs). Linear mixed-effects models (LMMs) were used to evaluate social motivation (ASHI), HATs, and rejection sensitivity (RSQ). The outcome measure for relationship improvement (CGI-I) and experiences with aggressive acts in dating relationships were integer valued; therefore, a Poisson mixed-effects model with a log-link function was used. 56 There were two time points as follows: baseline and follow-up, which was 12 weeks after baseline. In each model, we included a time-point indicator and their interaction as the primary fixed effects, along with individual-level random effects to account for individual variability. Confidence intervals (CIs) and p-values were calculated using the Kenward–Roger Wald method for LMMs, and profile likelihood-based CIs were used for the experiences with aggressive acts in dating relationship models. The significance level was set to p < 0.05 for all tests. We did not adjust for multiple comparisons due to the risk of inflating Type II error and because the study was exploratory rather than confirmatory.57,58
Community involvement
The content of the HEARTS and ACC conditions was codeveloped by autistic and non-autistic individuals. Each HEARTS and ACC session was co-delivered by a teaching team that included one autistic and one non-autistic individual. The research study protocols were developed with consultation with a paid autistic advisory board, who were not involved with the delivery of HEARTS or the ACC. In addition, one of the autistic HEARTS codevelopers and teachers is a coauthor on this article.
Results
Participants
Of the 129 individuals screened for study eligibility, 28 did not meet inclusion criteria and 9 declined to participate in the research study (Fig. 1). Of the 92 eligible individuals who consented to participate, 44 were randomized to the HEARTS condition and 48 to the ACC (see Fig. 1). Demographic characteristics were examined for treatment condition comparability using two-sample t-tests and Pearson’s chi-squared tests (Table 1). These tests showed no significant differences between the groups on any characteristic, supporting the assumption of intergroup comparability before the trial. See Table 4 for outcome variable descriptive statistics at baseline, T1, and T2, as available (Table 4). Attrition was minimal in both conditions. In the PP subsample, 100% of participants contributed data at baseline, T1, and T2 (Fig. 1). The majority of HEARTS participants will attend ≥4 out of the 6 class sessions.
Among those in the HEARTS condition, 88% attended 4 or more of the 6 sessions, and in the ACC, 82% attended 4 or more of the 6 sessions (p = 0.8, Table 1). Across all participants and all class sessions, there was a total of 42 absences. Analysis of reasons for absences revealed that 33% (n = 14) were for medical appointments or illness, 24% were because the person forgot, 17% were due to travel, 10% gave no reason, 7% were dissatisfied with class, and 9% had work, school, or family commitments that conflicted. The HEARTS content will be delivered with fidelity, and HEARTS participants will rate the content as acceptable.
Fidelity was maintained in both the HEARTS condition and the ACC. In the HEARTS condition, 94.3% of planned content was delivered as intended, and in the ACC 99.1% of content was delivered as planned (not shown). As planned, the ACC groups did not bring up HEARTS topics; mean fidelity ratings for ACC sessions purity (i.e., not including HEARTS content) ranged from 1.0 to 1.2, where 1.0 was the most desirable score and 3.0 was the least desirable score. Average scores provided by the teachers for acceptability (range = 6.5–10 M = 9.12, SD = 0.90), feasibility (range = 7.3–10.0 M = 9.43, SD = 0.67), and appropriateness (range = 8.0–10.0 M = 9.65, SD = 0.54) reflect good to excellent ratings. 59
On a scale from 1 to 10 where 10 was the best possible score, participants rated the class 7.0 (SD = 2.9) in terms of how informative it was, a 7.2 (SD = 2.6) for enjoyment, and rated themselves as likely (7.3, SD = 2.8) to recommend HEARTS to others (Table 3). Participants also rated the acceptability of each of the six sessions on a scale from 1 to 10, where 10 indicated the most acceptability. These scores ranged from 7.1 to 7.7 (Table 3).
Acceptability of Healthy Relationships on the Autism Spectrum Research Procedures, Intervention, and Weekly Content a
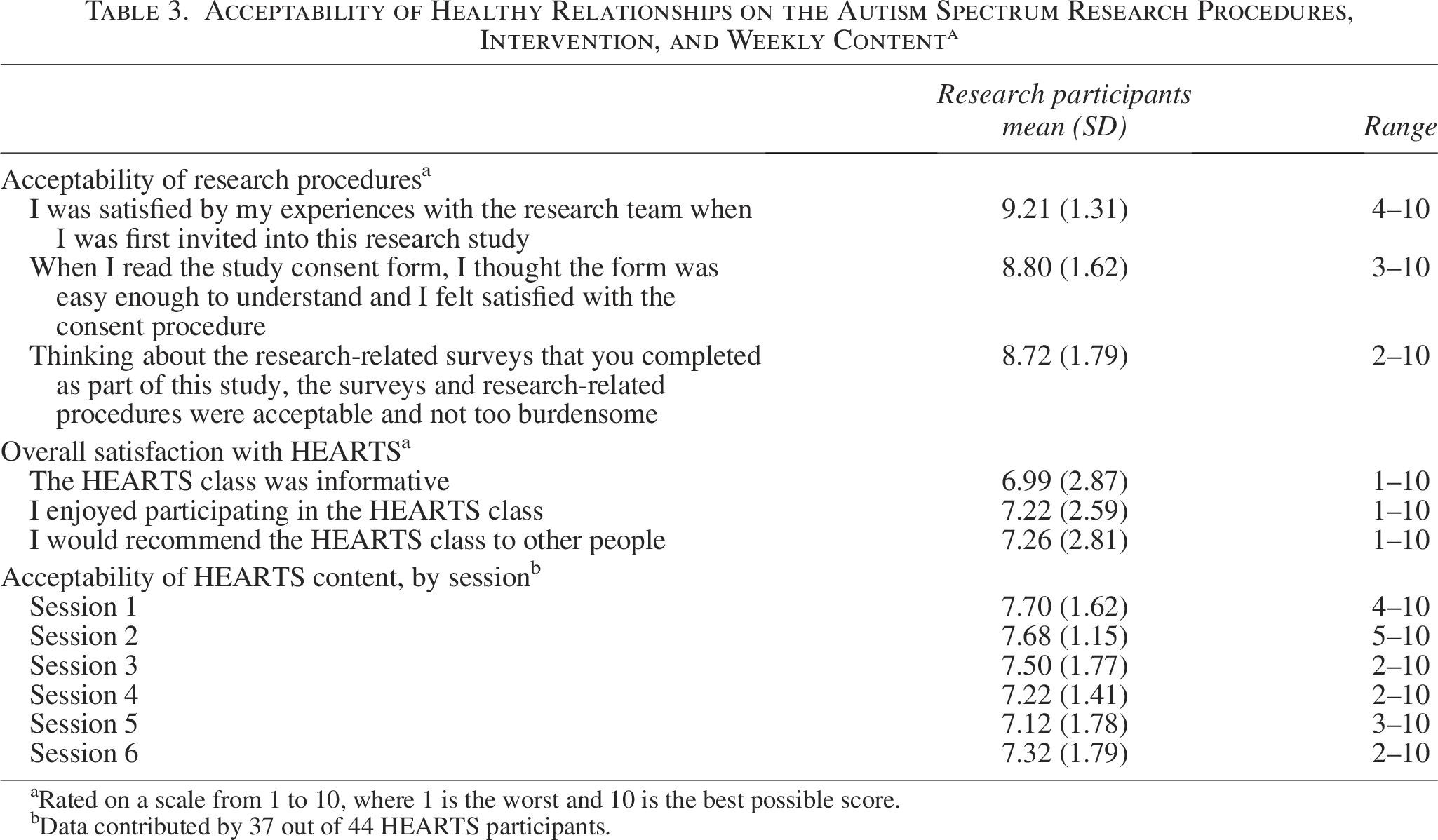
Rated on a scale from 1 to 10, where 1 is the worst and 10 is the best possible score.
Data contributed by 37 out of 44 HEARTS participants.
Those in the HEARTS condition will experience greater reductions in hostile automatic thoughts, rejection sensitivity, experiences with aggressive acts in dating relationships at follow-up compared with those in the ACC, and greater increases in relationship satisfaction and social motivation compared with those in the ACC.
There were no statistically significant differences between the HEARTS and ACC groups in terms of changes in experiences with aggressive acts in dating relationships, hostile automatic thoughts, rejection sensitivity, or social motivation (Table 4). Furthermore, no effects on these outcomes were found by condition when data were stratified by possible effect modifiers such as gender, sexual orientation, ADHD status, or other demographic variables.
Outcomes for Healthy Relationships on the Autism Spectrum and the Active Control Condition, Controlling for Sessions Attended (N = 92)
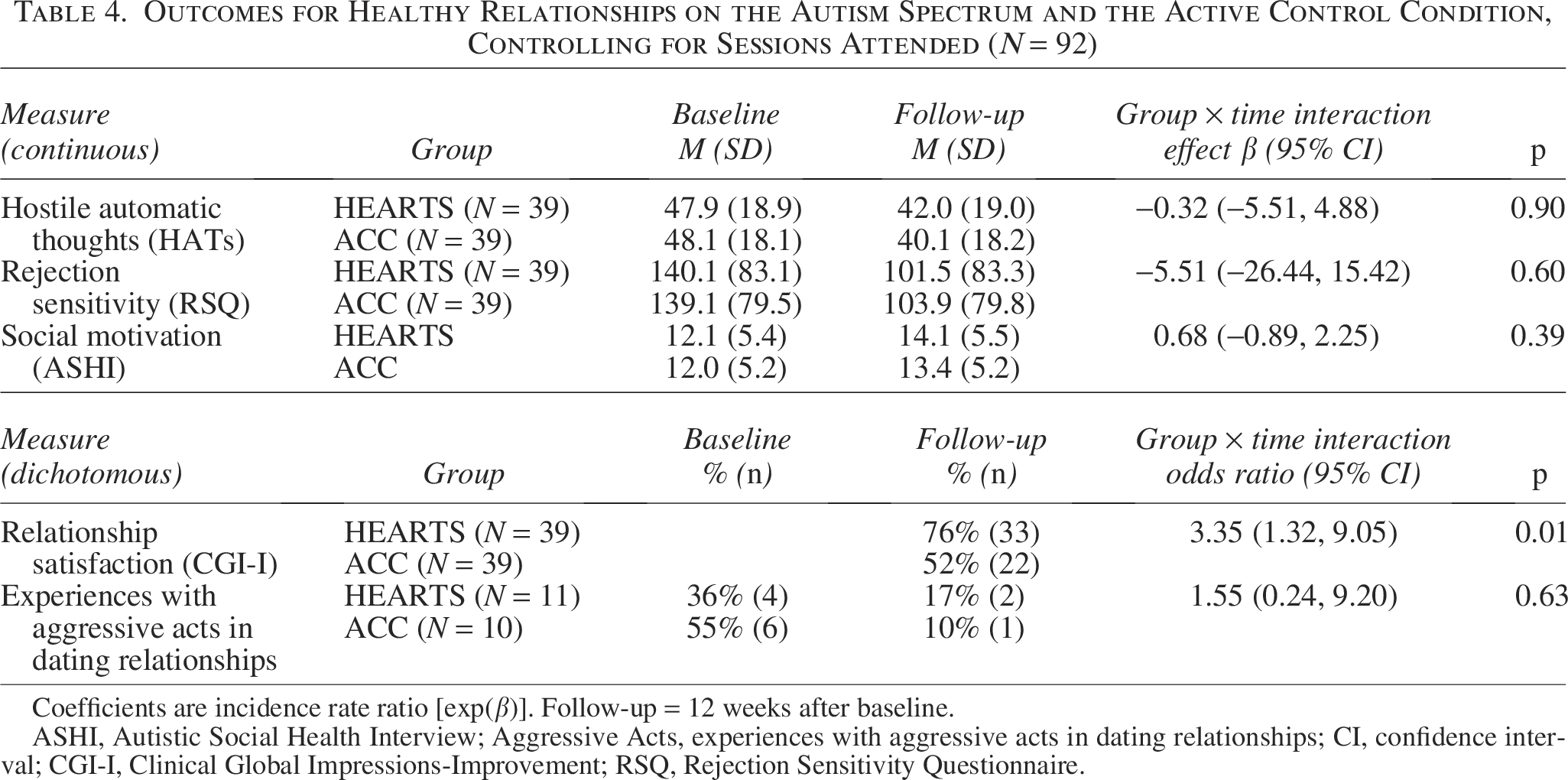
Coefficients are incidence rate ratio [exp(β)]. Follow-up = 12 weeks after baseline.
ASHI, Autistic Social Health Interview; Aggressive Acts, experiences with aggressive acts in dating relationships; CI, confidence interval; CGI-I, Clinical Global Impressions-Improvement; RSQ, Rejection Sensitivity Questionnaire.
There was more improvement in relationship satisfaction in the HEARTS group at follow-up compared with those in the ACC (Table 4). At follow-up, 76% of those in the HEARTS condition and 52% of those in the ACC were minimally improved or better in terms of relationship satisfaction (χ2 = 7.07, p = 0.0078). This is equivalent to a 46% increase in relationship satisfaction among HEARTS participants. The odds of improvement were 3.35 times higher in the HEARTS condition compared with the ACC condition (p = 0.01) (Table 4).
Discussion
This RCT found that the HEARTS program had a positive impact on relationship satisfaction for autistic adults. The HEARTS program is unusual because it was cocreated with a diverse group of autistic adults, is co-delivered by teams that include an autistic person, and uses a neurodiversity-embracing perspective—meaning that it doesn’t attempt to persuade autistic people to behave in ways that might be more acceptable to neurotypical people to enjoy healthy relationships. HEARTS embraces the core belief that autistic people can be their authentic selves and can create and maintain healthy, supportive, mutual intimate partnership and friendship relationships by understanding what counts as healthy versus unhealthy relationships, increasing skills for engaging in effective communication with partners or friends, coping with setbacks and rejections, and understanding how to exit or end relationships when necessary. HEARTS is also a rare program in that it’s offered online and is short duration, making it affordable to deliver.
The positive result of this RCT is important for the field and, for autistic adults, in at least two important ways. First, the ways in which HEARTS has been successful in engaging autistic adults from across the United States and some other nations (e.g., Israel, Canada, Australia) demonstrate that the model of financially accessible, online classes may be very appealing and practical for many autistic adults who would otherwise be unable or disinclined to travel to in-person program at a university or clinic. This finding is consistent with prior research that has also found that brief, online educational programs for autistic people can be feasible and effective.60,61 Second, the fact that HEARTS was codeveloped with autistic people, is co-delivered with autistic people, and takes a neurodiversity-embracing perspective is rare and demonstrates that it is possible—if not preferable—that all programming for autistic people be developed with substantive input from autistic people. Too many therapeutic and educational approaches that are intended to benefit autistic people have been created without meaningful formative feedback from autistic individuals,62,63 and as a result, there are now many powerful claims from autistic survivors of these programs that they have been harmed by them. 64 At a minimum, the HEARTS program demonstrates that it is possible to center the lived experiences of autistic people in the development of psychoeducational programming and attain both feasibility and outcome success. Third, this study found that HEARTS improved relationship satisfaction in just 6 weeks for autistic adults, which is consistent with prior evidence that HEARTS participation was associated with positive improvement on multiple outcomes of interest. 42 The idea that it is possible to improve relationship satisfaction for autistic individuals is encouraging and means that with more attention to sharpening the impact of HEARTS that even better gains might be possible. If HEARTS can be adjusted in ways that produce even better effects, but it remains online and low-cost, the widespread dissemination could substantially alter contemporary approaches to healthy relationships education for autistic people.
Our team is unsure why the HEARTS program may have worked more effectively for some individuals rather than others. We investigated many possibilities during our analysis phase to see if perhaps there were observable treatment effects for subgroups, such as those with ADHD, sexual and gender minority individuals, younger versus older individuals, and those with lower baseline scores of rejection sensitivity and relationship satisfaction. There were no patterns that would help us understand why some individuals responded more than others. It is possible that a combination of motivation to learn about healthy relationships topics, engagement in class, identification with or enjoyment of facilitators, opportunities to practice skills outside of class, and unrelated life events and factors (e.g., having to move to a new apartment, loss of a job) could have influenced how people engaged in HEARTS or were able to apply the lessons to their own social lives. Pinpointing factors that predict treatment response is a worthwhile objective for subsequent research. We also reflected on why we did not observe an impact on social motivation or dating aggression. It is possible that the short duration of the HEARTS intervention and the short duration of the follow-up period postinvention limited our capacity to detect changes in these domains.
Results must be viewed within the context of at least eight limitations. First, we did not include a third no-treatment group. It is possible that one reason we saw no changes in four of the outcome variables is that socializing with other autistic individuals in an online discussion group was also beneficial. In fact, positive changes in social motivation, HATs, rejection sensitivity, and experiences with aggressive acts in dating relationships were observed among both ACC and HEARTS participants. We speculate that some autistic individuals prefer less structured, more open discussion groups, whereas others favor didactic skill-building groups. Allowing people to choose their preferred modality might improve results even further. Second, each online class enrolled up to 20 participants. Best practices for online engagement and learning suggest that students typically benefit from more interaction with instructors, 65 so smaller class sizes could have produced stronger outcomes. Third, the HEARTS intervention was brief—only 6 sessions. Some participants wrote in feedback on their evaluation surveys that indicated that they thought a longer program would be enjoyable and beneficial. A longer intervention might have yielded even more positive results, although one recent evaluation of short online group interventions for autistic adults found that even 6-session programs can be effective. 61 Fourth, autistic people who are self-diagnosed, and not professionally diagnosed, were excluded from this research. To be clear, self-diagnosed people were included in HEARTS classes, just not eligible for participation in the research. To be consistent with other federally funded RCTs, we opted to make professional diagnosis an eligibility criterion. The authorship team believes that self-diagnosed autistic people could benefit from HEARTS as much as diagnosed individuals, but that is a hypothesis to be tested in future research. Fifth, we neglected to collect disability status at baseline other than intellectual disability and selected psychiatric conditions, and disability status could be related to HEARTS effect. Sixth, the research could have provided better accessibility supports to participants. For example, although consent forms were written for a lower literacy level in an attempt to be inclusive, there was no plain-language alternative form, and Likert scales were not adapted for autistic participants. Seventh, the only outcome measure that indicated improvement was the CGI-I, and the CGI-I depended upon non-autistic interviewers rating the participants on improvement on healthy relationship skills that the participants had selected for themselves as goals. It is possible that the raters imposed neurotypical norms of improvement on the participants, which could have biased results toward the null. Eighth, every HEARTS activity was rated as unsatisfactory to at least one autistic participant. Efforts to understand why activities were unacceptable or unsatisfactory to a minority would benefit future iterations of HEARTS.
Despite these limitations, the results of this trial indicate that HEARTS is feasible to implement and was generally well-received by the community as well as effective for improving relationship satisfaction. Future recommendations for implementing HEARTS to enhance outcomes include reducing class size, narrowing the age and eligibility criteria to participants with fewer baseline skills and knowledge, preselecting individuals interested in learning skills for healthier relationships rather than just meeting people or making friends, and focusing on participants who are motivated to work on self-improvement and practice skills between sessions.
Conclusions
HEARTS, a healthy relationships program codeveloped with autistic individuals and delivered by autistic facilitators, significantly increased relationship satisfaction among autistic adults compared with an active control condition. While no differences were found in other outcomes, the results support further refinement and broader testing of HEARTS.
Footnotes
Acknowledgments
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors wish to thank autistic advisory board members, including Amelia Sanchez, Austin Montgomery, Reid Caplan, and Charlene Wooten, HEARTS and ACC teachers, including Brandy Haberer, Karen Lean, Jess Alder, Sarah DeCosta, and Victoria Reome, and AANE liaisons, Aaron Levinger and Nancy Schwartz.
Authorship Confirmation Statement
All authors reviewed and approved the final article and agree to be accountable for its content. Conceptualization: E.F.R. and S.W. Methodology: E.F.R., M.Y., and S.W. Formal analysis: M.Y. Investigation: E.F.R., J.C., and S.W. Data curation: M.Y. Writing—original draft: E.F.R. Writing—review and editing: E.F.R., M.Y., J.C., L.G.H., S.W., and K.L. Supervision: E.F.R. and S.W. Project administration: E.F.R. Funding acquisition: E.F.R. and S.W. The article has been submitted solely to Autism in Adulthood.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
Research reported in this publication was supported by NIMH under award number R34MH131919. All of the total project costs were financed with federal money. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.