
Abstract
Background:
Research shows the unique challenges that being autistic can pose in the perinatal period, including sensory sensitivities. Further challenges may relate to health care systems designed for non-autistic people and a lack of practitioner awareness. Literature exploring autistic people assigned female at birth’s (AFAB) experiences of baby loss is more limited, but this can be traumatic, as reported in key literature.
Methods:
This qualitative study used Interpretative Phenomenological Analysis (IPA) to understand how six autistic people AFAB made sense of their experiences of baby loss through miscarriage, stillbirth, and neonatal death.
Results:
Participants described the unpredictability, trauma, and absence of care from practitioners throughout baby loss, which left them feeling unsafe, neglected, and not believed. Participants shared how baby loss heightened their autistic experiences and was perceived to intensify their distress. They reported shame, guilt, and blame in relation to their autistic and gender identity perpetuated by the silencing and stigmatising societal discourses surrounding baby loss. Participants described a sense of continuous embodied physical and emotional pain of being without their babies. They felt that autistic grief may be different from non-autistic grief. Reconnecting with their babies through continuing bonds in more practical ways was important.
Discussion:
Many clinical implications arose that add to existing research, including the necessity for improved practitioner awareness and knowledge in perinatal settings, along with the unique experiences of baby loss and grief for autistic people AFAB, which this research adds. Trauma-informed care provided in line with needs and preferences is imperative.
Community Brief
Why is this an important issue?
Baby loss is an often-devastating experience across neurotypes. However, there have not been many studies exploring autistic people assigned female at birth’s (AFAB) experience, and completed research has mostly utilized surveys to help understand this experience.
What was the purpose of this study?
We wanted to speak to autistic people AFAB about what it is like to experience baby loss. We hoped to build on the previous, but limited, research to inform how we better support autistic people AFAB who may go on to lose a baby.
What did the researchers do?
Six autistic participants talked to one of the researchers about their experience of baby loss in an online research interview. We used a research method focused on understanding the meaning and experience of baby loss called Interpretative Phenomenological Analysis. We looked for similarities and differences across their experiences and wrote about them in this research.
What were the results and conclusions of the study?
We constructed five main themes to capture participants’ experiences of baby loss as shared in the interviews:
Participants described the Baby loss was a Baby loss was often experienced as The death of a baby was an Reconnecting and experiencing bonds with baby were important, with participants finding personal, uniquely practical ways to remember their babies.
What is new or controversial about these findings?
We found similar things to previous research. The new things we found were the impact of unpredictability and not receiving enough information. We also found that autistic people AFAB blamed themselves as disabled people for the deaths of their babies.
What are potential weaknesses in the study?
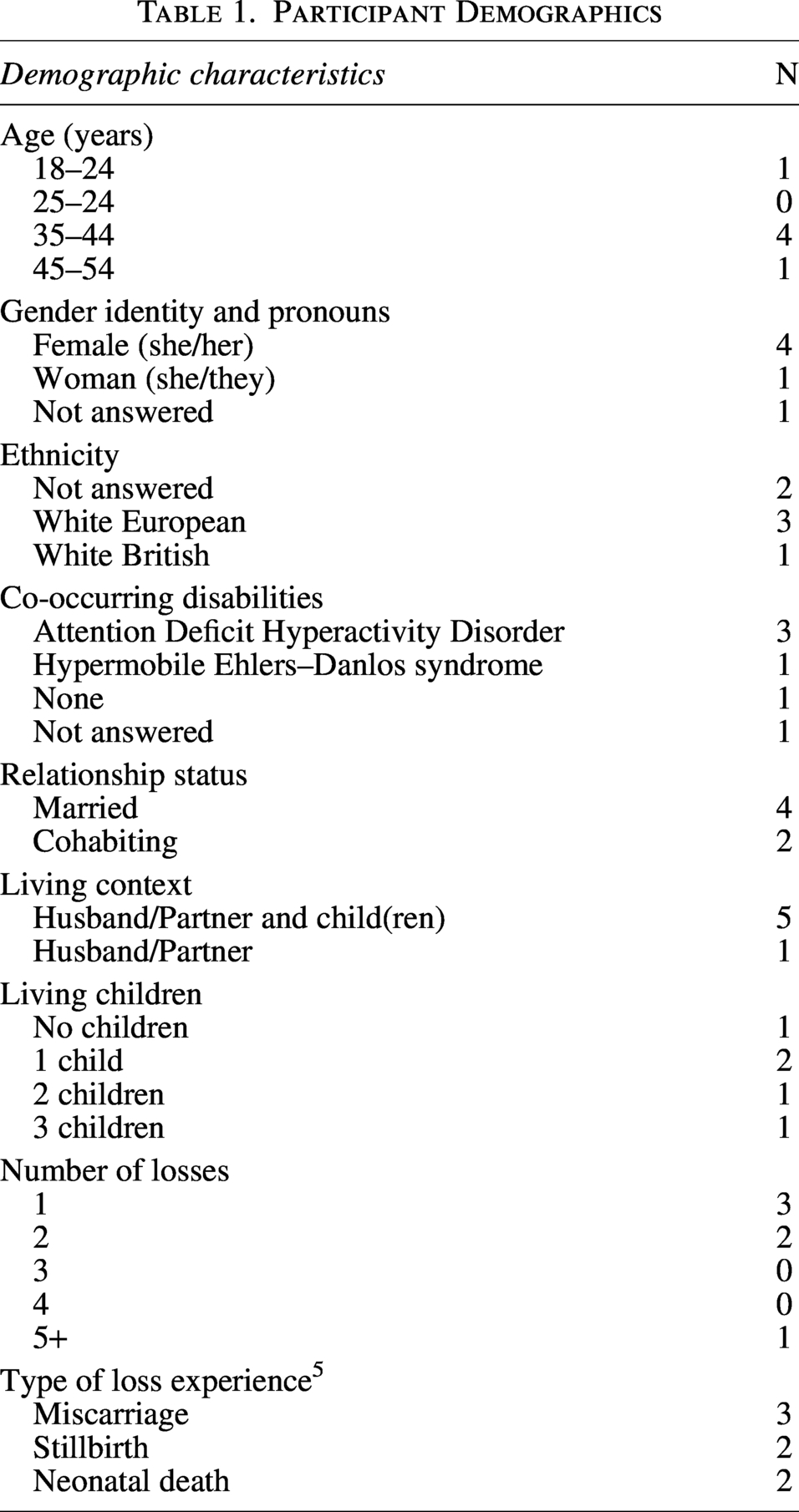
The participants were mostly white, western, cis-gendered, speaking women aged between 35 and 45 years old. We asked participants about a range of different types of baby loss experiences. This means there may be differences among their experiences.
How will these findings help autistic adults now or in the future?
These findings suggest that while baby loss is distressing for everyone who might experience this, there are unique challenges for autistic people. These findings are important to consider in health care to improve the experiences of autistic people AFAB who may lose a baby.
Keywords
Background
In the perinatal period, autistic people AFAB can draw on strengths, such as sensory sensitivities to attune to baby’s needs,1,2 however, can encounter unique challenges. Sensory challenges can be experienced across pregnancy, labour, and birth, such as hyper- and hyposensitivities to interoception (awareness of internal sensations) and proprioception, 3 for example, heightened experiences of pain throughout labour and birth, which can be distressing. 4 In addition, sensory challenges in the hospital environment, which feel misaligned to an autistic neurotype, have been reported. 1 Such challenges can precipitate traumatic experiences of labour and birth, increase feelings of anxiety and overwhelm 1 and can lead to shutdowns (retreating from the environment) or meltdowns (externalised expressions of distress), both in response to emotional and sensory overload. 5 This can in turn impact communication, which may increase vulnerability and trauma. 6 Moreover, labour and birth can feel out of control for autistic people AFAB, in the absence of safety in predictability (safety gained through information and knowing what to expect). 4
Further systemic challenges have been reported in maternity settings, 4 such as experiences of invalidation, 7 pain not being believed, and knowledge of autistic people AFAB’s bodies dismissed (e.g., needing to push in labour) by practitioners. 5 Such challenges have been reported to stem from a lack of awareness and understanding of autism, 4 and systemic, neuro-normative approaches to maternity care. 8 This can prevent sharing of diagnosis due to fear of negative judgment and stigma from practitioners. 4
Baby loss is an often-devastating reality, enshrouded in stigma.9–11 Universally, those experiencing baby loss describe the silence 12 and discomfort felt by others, 13 including practitioners, friends, and family, which can lead to their grief becoming disenfranchised (not societally recognised). 11 Systematic reviews have described universal experiences of grief following baby loss, such as feeling heartbroken, numb, and an embodied sense of emptiness.14,15 Pregnant people experiencing baby loss may also describe strong feelings of shame, blame, and guilt, 15 attributed to a personal failure of themselves and their bodies for the death of their babies.16,17 Furthermore, baby loss can be a traumatic experience, including the process of learning about the prognosis of their pregnancy and interactions with practitioners. 18
Little research exists about the specific experiences of baby loss for autistic people AFAB. However, the limited research has highlighted that baby loss can be traumatic. 19 Autistic people noted differences in communication with practitioners as a source of difficulty, which included not being given enough information. Experiences of feeling belittled, ridiculed, invalidated, or abandoned, and a lack of emotional warmth and care from practitioners were reported. These interactions were experienced in an environment that felt unsupportive and not systemically adapted to autistic needs. Key recommendations from this research include asking autistic people about their needs and preferences, such as pain and communication, especially during labour and birth, and the provision of neurodiversity-affirming training to practitioners to increase understanding. 19
Taken together with the unique challenges of the perinatal period, potential psychological impact, and the currently under-represented evidence base, further research is needed to understand the experiences of autistic people AFAB’s experiences of baby loss. Therefore, this study utilised IPA to gain a deeper understanding of autistic people AFAB’s experiences of baby loss.
Method
Positionality and reflexivity statement
The first author identifies as a white, cis-gendered, autistic, woman. The second author identifies as a white, cis-gendered, non-autistic woman who has experienced baby loss through miscarriage. The third author identifies as a white, cis-gendered, non-autistic woman. Reflexive journaling by the first author and regular reflexive conversations in the research team aided awareness of insider- and outsider-researcher positions and the possible influence on the research process.
Patient and public involvement and engagement
Two bereaved autistic parents acted as Expert by Experience (EbE) consultants and were recruited through Sands Baby Loss Charity by the first author. Consultation informed and shaped the use of gender-inclusive terminology to recognize and represent the views and identities of the autistic community, as research suggests gender-diverse adults are three to six times more likely to be autistic than cisgender adults. 20
Consultation informed all recruitment processes and development of research materials, leading to changes including regular trigger warnings, specific questions related to experiences with practitioners, and check-in processes during sensitive points in the interview. Consultants were paid for their time in line with the institute guidance.
Design
The study used IPA due to its focus on exploring idiographic, first-hand accounts of lived experiences. 21 Semi-structured, one-to-one interviews were chosen in methodological alignment with IPA. 22 A semi-structured interview schedule was constructed in line with the research question, aims, Smith’s guidelines, 22 and with EbE input. A framework of the interview questions was shared in advance, as an equitable requirement, to build safety in predictability.
Recruitment
Participants were recruited using purposive sampling via three pathways focused on baby loss or autistic parent contexts, including Sands Baby Loss Charity, Autistic Parents UK, and Maternity Autism Research Group. A research Twitter/X account was created later during the recruitment phase. Recruitment involved sharing a research poster with a short description and supporting alt text.
A clear process for recruitment was developed (Supplementary Data). Autistic needs were foregrounded throughout, including communication and information processing differences and providing safety in predictability through information as part of informed decision making.
Participants
Participants were invited to take part if they identified as an autistic person AFAB, which included both formal and self-diagnosis. Participants had all experienced baby loss, including miscarriage, stillbirth, or neonatal death.
Potential participants were not included in this study if they had experienced baby loss within the last 6 months at the time of recruitment, due to the understandable rawness of distress in the early months following bereavement. Participants who were currently pregnant, trying to conceive, experiencing high levels of psychological distress or in mental health crisis were also excluded from the study to minimise additional distress due to the sensitive nature of the topic. These factors were discussed in collaboration with each prospective participant to value their knowledge of themselves.
Six autistic people AFAB took part in the study. As part of this, demographic information was collected (Table 1).
Participant Demographics
Data Collection
Interviews were conducted by the first author via Microsoft Teams. Several measures were included to enhance equity, participation, and well-being. Participants were given a choice about how to communicate (e.g., speaking or typing answers) and all chose to communicate through speaking. They were also given a choice with relation to visibility, and most interviews occurred with cameras switched off. The interviews ranged in length from 92 to 133 minutes. Each interview was recorded for transcription purposes. Following each interview, participants had access to a debrief space to explore their experience and discuss post-interview care and were given information about support options.
Ethics
Ethical approval was granted by the University of Hertfordshire ethics committee (protocol number: LMS/PGR/UH/05620). All participants provided informed consent to participate. In line with guidance from bereavement research, 23 participants were given the choice about using theirs and their babies’ own names in the study, or to use pseudonyms. All participants gave informed consent to use theirs and their babies’ names to honour their lives and continue bonds. Participants were aware that any further personally identifiable information would be removed. Due to the emotive nature of the topic, specific care was taken to support participant well-being, which included following a clear distress and disclosure protocol, debrief process, ensuring the right to not answer any questions, to pause or end the interview, and withdraw from the study.
Data Analysis
Data analysis began with transcribing each interview and immersion in the data. The steps for IPA analysis 21 were followed. This began with initial noting, attending to segments with a clear phenomenological lens, beginning at a descriptive level, to linguistic, to a higher conceptual and interpretative level. Experiential statements were constructed to capture the essence of participant experience, sense-making, and interpretation before searching for connections across experiential statements to construct personal experiential themes, illustrated with participant quotes. These steps were repeated for each participant before searching for patterns across participant accounts to develop Group Experiential Themes (GETs). The final stage of analysis involved writing a narrative.
Results
Following rigorous data analysis and interpretation of six autistic participants’ experiences of baby loss, five GETs and subthemes were constructed to describe their experiences of baby loss. All participants named their babies before they died and spoke about them during the interviews in detail, which is reflected in both the duration of the interviews and the meaning of taking part. Participants thanked the researcher for using the name they chose for their babies, and some felt that participating made their babies “real” (see Table 2).
Names of Participants and Their Babies
Each GET and subtheme is described and illustrated with participant quotes to hear their voices and evidence the researchers’ interpretations (see Table 3). The data presented contains themes of difficult health care experiences and trauma, which may be distressing.
Summary of GETs and Subthemes
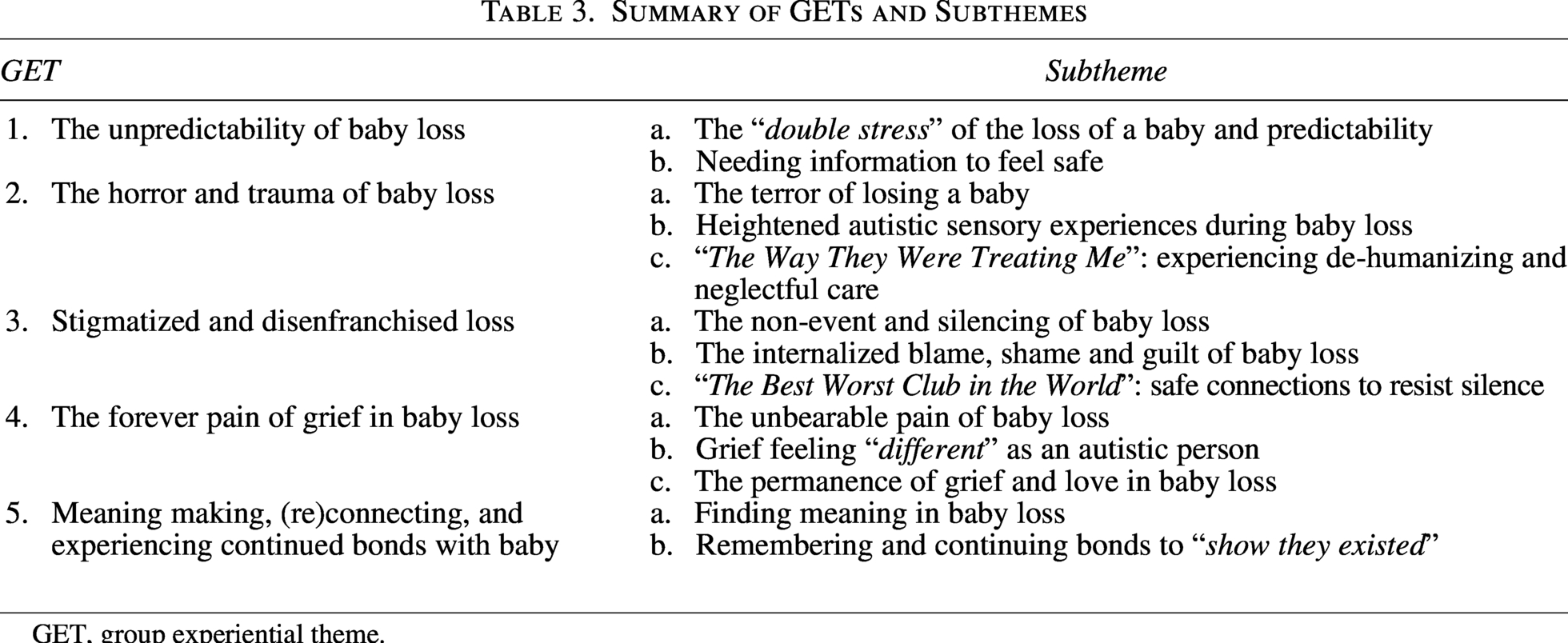
GET, group experiential theme.
The unpredictability of baby loss
Being suddenly thrust into the experience of baby loss, where predictability was lost, was distressing. Access to information to restore safety and predictability was important, which participants actively sought for themselves when practitioners failed to provide it. Some participants described glimpses of personalised care, particularly when practitioners provided clear information, that helped them to restore a sense of control and safety.
The “double stress” of the loss of a baby and predictability
The impact of losing a baby and the secondary loss of not knowing “what was going to happen” (Han) was described by participants. For some, pregnancy and birth were new experiences, as was losing their baby. Participants reported feeling “scared” and anxious for different reasons, for example, how long their babies would live, and “not knowing how labour worked” (Adrienne), while navigating a new, medical environment, which “I hadn’t been to” (Han).
I knew that there wasn’t gonna be a good outcome or if it was […] it was gonna be brief. And I was scared, and I didn’t know what was gonna happen (Jem).
Needing information to feel safe
Participants described the strong need to obtain predictability to feel safe, through seeking information to understand what was happening. The “lack of information […] had quite an impact on me […],” which “felt out of control” (Han) and could lead to “shut down,” due to “continually trying to get more information” (Jem). Participants reported “reading lots” and searching for information themselves to relieve the unpredictability and compensate for the absence of information from practitioners. This self-obtained information (e.g., found on the internet) was not always helpful, or heightened their sense of distress and the unpredictability of baby loss.
I had no information from the early pregnancy unit […] what I had Googled wasn’t what happened. I didn’t know if it was safe or do I need to tell you, tell someone and do I need to take medication to make it […] I didn’t know what to do (Hayley).
Conversely, glimmers of helpful interactions with practitioners who provided more information about aspects of the loss experience, which were personalised and attuned to their experiences, were shared. This included practitioners who “drew us a picture of the heart, explained it all, that stuff sticks in my mind, I liked it” (Liz). Such moments were reported as particularly meaningful.
The horror and trauma of baby loss
Fear, distress, and despair arising from baby loss were described, which many named as a traumatic and terrifying experience. Heightened sensory experiences, for example, internal triggers like pain and external triggers like the hospital environment, added to their distress. This was compounded by the way they were treated by practitioners, and exacerbated a sense of feeling powerless, frightened, and out of control.
The terror of losing a baby
Actively losing a baby or witnessing a baby die made sense of as being “traumatic” (Adrienne), across the different types of baby loss. Participants described the imprint of trauma and how this has stayed with them.
Suddenly I was in a lot of pain screaming on the bed […] and then that’s when I passed what looked like a baby […] I don’t know what I was thinking, but I remember just bursting out crying, […] I was confused and upset at the same time, and I think I probably was scared as well, like obviously didn’t know when I was pregnant, so I didn’t expect that to happen (Bethany).
Participants recalled distressing memories of watching their babies “fight” for their lives after being born and the fear they felt seeing their babies being “resuscitated” and remembering the “breath, the gasping” (Jem). This could lead to further experiences of shutdown, and feeling powerless in not being able to help their babies.
[…] we watched him die slowly of heart failure. It was awful. His little abdomen swelled up, his head swelled up (sigh) […] we couldn’t do anything at that point […] so they delivered Oscar, he was very delicate. He’d been dead for six weeks (big heavy breath) […] Felix was in NICU […] we just stood there […] until his heart stopped again and all the machines, the flat lining noise […] (wavering, breathless; Liz).
Some participants “remember being really terrified that I was going to die” (Hayley) and that the fear was “like no fear I’ve ever experienced before, absolute terror” (Liz). Trauma was used as a word to make sense of aspects of their experience, with some sharing that they have been “diagnosed with PTSD because of it” (Jem). Some participants described having “blank spaces” (Liz), as their brains “way to kind of protect me” (Bethany).
Heightened autistic sensory experiences during baby loss
A range of heightened sensory sensitivities while losing their babies was reported as an additional layer of stress, for example, the hypersensitivity to the “feeling of blood on me,” during miscarriage, which felt “disgusting” (Bethany) and interoception, with “the taste of metal subsiding rather than increasing” (Hayley). Some participants described the “utter nightmare” of the hospital environment, like “the smells, sounds, lights” (Han), which were “just too much to go through” (Jem). Some described how “autistic and hospitals don’t mix” due to a lack of agency, choice, and a hypersensitivity to the “blue lights in NICU” (Liz).
Moreover, the heightened sensation of pain throughout losing their babies was described as “agony” (Han), “unlike any type of pain” (Bethany), and “a lot worse than I’d ever experienced before” (Hayley). Challenges in receiving pain relief were also reported during their miscarriages, due to practitioners failing to recognise experiences of pain, which may reflect the differences in expression and communication of pain. Furthermore, participants described finding it “hard for me” to express experiences of pain during baby loss “because I’m not someone who is like, “oh, ouch” (Adrienne). This may also reflect the differences in external, observable expressions of pain observable, compared with participant’s internal experience, which could have added to the intensity of these experiences.
“The way they were treating me”: experiencing dehumanising and neglectful care
Participants described their distress in response to the felt absence of care from practitioners throughout baby loss and the impact of these experiences, including the additional context of being autistic. They expressed feeling “neglected by the system, which was hurtful” (Bethany), “in a place where you should be safe” (Hayley), despite “knowing they’d seen my notes” (Jem) while accessing medical care in A&E and wishing to be “treated with a bit more humanity” (Han).
By this time my trousers are saturated with blood […] I’m regularly going backwards and forwards to the loo and I’m dealing with it. The only problem was on one occasion I got up to go to the loo and a nice police officer said I’m really sorry you can’t go in the loo […] basically the police officer was there with someone who was under arrest in handcuffs […] I was less important than a criminal who was under arrest during my miscarriage experience is how I felt (Han).
Some participants expressed a sense of pain and sadness at being placed on maternity wards, “which made my heart crush just listening to another woman with a heartbeat of her baby” (Adrienne), which reminded participants that “I didn’t have my baby” (Jem).
In addition, participants described feeling belittled during their experience of baby loss, in relation to differences in sensory experiences, often connected to pain and interoception. This could be triggered by practitioners’ perceptions of pain, for example, “you have a good pain threshold,” despite participants internally experiencing “so much pain” (Adrienne). Similarly, participants reported feeling that their internal sense of their bodies were infantilised, not believed or taken seriously, for example, a nurse doubting whether “you’ve not just wet yourself” (Jem) at the beginning of labor. This also conveyed a sense of internal questioning and having to prove this to others.
When I was having a miscarriage […] I was saying I felt these changes, I felt this and I felt that and people, midwives, GPs, consultants would say “no, no, you can’t have felt, it’s too early,” or “mothers don’t feel when that happens”, and I absolutely did (Hayley).
The impact of practitioners’ not respecting “my boundaries,” led to feeling “super vulnerable.” This was an additional layer in context of being autistic when “your stress response is to shut down and not be able to speak verbally” (Hayley). Participants reflected on how they may be perceived by others when attempting to communicate experiences of distress.
[…] I’m no good at turning up at the GP in floods of tears and a shivering mess for them to take me seriously […] I seem like I’m OK, so it’s a real struggle to get anyone to actually understand what my brain is thinking of, it’s actually mental torture (Han).
This appeared to further convey the differences between observable communications of pain and participants’ expressions of pain and interoception, adding to their distress throughout baby loss.
Stigmatised and disenfranchised loss
Participants’ experiences of baby loss were felt to be unrecognised, silenced, and invalidated by others, which they made sense of in the context of the societal taboo of baby loss. They described the psychological impact of this and the power of connection with others who had experienced baby loss to resist the silence.
The non-event and silencing of baby loss
The societal and “cultural” silence and “taboo” of baby loss across many layers was named by participants, which is “not talked about enough that it’s a fucking awful experience” (Han). Participants described “seeing the split of people who do a runner” (Liz), or “didn’t know what to say” (Jem), demonstrating the stigma surrounding baby loss. Furthermore, experiences of minimisation and invalidation from family and friends as reported by participants could have failed to recognise both the physical and emotional pain of losing a longed-for baby and future.
She said, “maybe it worked out for the best” […] that phrase, “maybe it was for the best”, when your whole body is cramping and releasing the thing that you want to keep the most is just a horrendous thing” (Hayley).
Participants also shared the impact of navigating the silencing of baby loss from others, which could become internalised and lead to doubting their loss. Participants talked about “keeping [grief] to myself” (Bethany) and “stopping my feelings, my thoughts” (Adrienne) as examples. Moreover, participants appeared to be hypervigilant to the gaze of others, which could reflect experiences of invalidation and silencing, in turn leading to suppressing and hiding their internal experiences. Some were noted to apologise “if it’s too much” (Adrienne) and were tentative in sharing.
I was quite wanting to speak about it, so it was just […] it was difficult because when they’d ask me and I saw how uncomfortable it made them, I just didn’t speak about it anymore (tearful) I think that’s why I’ve […] suppressed a lot of my emotions about it and try to bury it deep down (Jem).
The internalised blame, shame and guilt of baby loss
A profound sense of shame, guilt, and internalised blame for the death of their babies as people AFAB was shared. Participants described blaming themselves “for it all” (Han) and self-criticism for not being able to do the “most innate basic function that my body is designed to do” (Hayley), which could be exacerbated by a context of multiple losses.
My body was like not a machine to procreate but a machine to get people dead, I was creating things that my body was killing […] it was awful. What’s wrong with me? My body is like a cemetery (Adrienne).
The sense of blame and guilt was also made sense of in relation to their autistic identity, which was “another reason to feel inadequate in life and useless again” (Han), with pregnancy initially feeling like “I was doing something right with my life […] I was like everybody else” (Jem) until then losing their babies.
It was tied into being a disabled person as well, and that my body had failed me and people going, that’s probably, you know, this is underlying […] this whole idea that Hayley’s not quite right, so no wonder she can’t do anything right […] like have a healthy pregnancy, so I think there’s ableism, kind of woven through (Hayley).
This describes the sense of internalised blame and fault, at the intersection of gender, autism, and baby loss, which may have heightened their distress.
“The best worst club in the world”: safe connections to resist silence
Safe connections with others who had experienced baby loss via online communities could bring relief from the societal stigma and silence that “no one talks about” (Han). Participants described the sense of care in re-enfranchising their babies’ lives through these communities, recognising their babies, for example, marking their birthdays. This evoked a sense of belonging and connection.
“I got a card through the door […] it was addressed to Seren and I opened it and it was someone from this community who’d sent Seren a birthday card and […] I have to ask family to write a card to Seren on his birthday, but to have that card come through the post without having to ask anybody, meant the world” (Bethany).
The forever pain of grief in baby loss
The deep, universal, and lifelong emotional and physical pain of baby loss and navigating life physically without them was described, along with the unique aspects of autistic grief.
The unbearable pain of baby loss
Participants shared subjective experiences of the rawness of grief as they began to navigate and process life without the physical presence of their babies. Grief in the early days was described as an embodied pain and “like an empty vessel, like part of me had died” (Jem).
“I never felt emptiness like this […] seriously, it was like I’d been cut, you know, like pumpkin at Halloween… and there was no light in it and it yeah, it felt like a deep hole” (Adrienne).
The rawness of such distress and grief could be intensified by a heightened sense of feeling internal sensations and pain, which some described as feeling as though “it was gonna kill me” (Liz). This may also be connected to the interoceptive and emotional processing differences autistic people can experience, adding a further layer of intensity to their grief. Participants expressed the sadness in different ways, for example, in all the hopes and dreams lost through their babies’ death.
“When I first lost Seren […] I was begging, begging for a day where I didn’t remember him, because every time I remembered him I’d get upset and […] I’d be like, please, just let me forget about him for one day […] it felt like a sort of physical pain, especially in my heart, like when I was crying […] it’s like a physical pain in my chest” (Bethany).
Grief feeling “different” as an autistic person
Participants described their sense of grief feeling “different to others” (Bethany), which added to their grief for their babies. Some participants described a sense of internal conflict between the logical strengths of their neurotype and the painful emotional manifestations of grief, which were unexpected and profound.
“My brain’s trying to rationalise it by saying that […] I’ve got enough medical knowledge to know that it’s quite common that miscarriages happen and scientific black or white point of view that miscarriages happen, however […] it’s quite shocking to me how much it really did impact me and actually […] it was awful (Han).”
Participants described the range of universal emotional experiences, particularly a sense of anger, which could be exacerbated by difficulties in identifying or making sense of internal emotions and physical sensations, as Han described, “I feel dot, dot, dot, as in I don’t know.” Distress and grief could also lead to an increase in autistic experiences, such as meltdowns, sensory and communication differences. While some appreciated connection with others, some spoke about the need to grieve alone, to avoid “talking or getting asked” (Liz), which often felt intentional to mitigate further experiences of stigma, particularly at the intersection of being autistic. Experiences of invalidation and silence may contextualise this further.
“We engineered the home […] to just shut the world out. It was something that we chose to do so we could heal in our own way in our own time” (Hayley).
The permanence of grief and love in baby loss
Grief for their babies changed over time but was always felt, reflecting the forever physical absence of their babies. Participants described grief for their babies as something they “live with, like in my bag or my pocket” (Hayley), which could fluctuate and be triggered by everyday reminders of being without their babies.
“Grief does come in waves, and when it does come as a wave, it creeps up on you like there’s been days where I’ve been absolutely fine and then all of a sudden bang, it just hits me […] I cry, and I say I want my baby back” (Bethany).
Participants described the sense of “pure sadness which has never left” (Jem), which also had an embodied, physical element to express the continued sense of grief over time.
“It still crushes my heart, but it doesn’t make me want to die […] Now it is more of a heaviness” (Adrienne).
Meaning making, (Re)connecting, and experiencing continued bonds with baby
Participants tried to ascribe and make meaning of their babies’ deaths and continue to reconnect, remember, and continue bonds with them in memory through intentional, practical actions.
Finding meaning in baby loss
Participants described the ways in which they made meaning through their experience of baby loss. The experience of loss could lead to a discovery of values, hopes, and dreams and new perspectives about themselves, for example, “because of him we know we are autistic” (Adrienne).
“My healthy happy neurodivergent children are everything that baby taught us we wanted […] so I heal a little bit more everyday” (Hayley).
Some participants described attempts to make “some sense” (Jem) from their babies’ deaths, for example, through organ donation, to gift the life their babies did not get to live. However, attempts to make meaning in this way were disrupted, which led to further hurt and sadness.
“I want to donate his heart to save someone so that it feels like this make some sense of it (tearful) […] they could have saved another baby […] but how could someone contaminate it” (Jem).
Others described how the meaning of the death of their babies influenced beliefs of safety and coping as an autistic person attempting to manage the anxiety of navigating a predominantly non-autistic world. Such coping skills were felt to no longer be meaningful or as adaptive as they once were before the experience of baby loss.
All the safety things I’ve built into my life […], were blown away […] it’s completely meaningless […] we had better odds of winning the lottery than what happened to us with the twins. So, my way of coping with anxiety […] was looking at stuff like that making sense of it by […] numbers, and none of that works anymore (Liz).
The experience of finding meaning in baby loss was varied, with some reporting more helpful and positive experiences, and others more difficult, perhaps adding to their grief.
Remembering and continuing bonds to “show they existed”
While this could be painful, the significance of remembering their babies and finding ways to reconnect and continue bonds to legitimise their lives and participants’ experiences was important. Participants often described physical and tangible ways of honouring, remembering and transforming grief to continue traditions as if their babies were physically alive. Subjective ways of marking their babies’ lives through objects were shared, such as teddy bears and earrings, which conveyed the sense of a forever-felt presence.
“This year […] he’s got a badge, some balloons that I’m going to blow up for him. We’ve got bunting. We’re having a picnic. He’s got a cake, got him some new ornaments for his grave. Some toys, some books that I can go and read, obviously, if he was here, he would be spoiled” (Bethany).
Discussion
The study heard how six autistic people AFAB made sense of their experience of baby loss. Consistent with autistic experiences across the perinatal period, the findings further our understanding of the deep distress caused by the loss of predictability for those whose babies died,4,24 with participants seeking information to obtain predictability and build safety. As seen in research on autistic perinatal experiences, the findings powerfully highlight the psychological impact of not being given enough information.19,25
Consistent with research on baby loss in the general population, participants’ experiences indicate the prevalence of trauma related to baby loss.26,27 Unique challenges may indicate additional layers of trauma for autistic people AFAB, for example, heightened sensory experiences in relation to hospital environments designed for non-autistic people and feeling belittled, misunderstood and not believed as identified in previous research on autistic experiences of baby loss. 19 Furthermore, a lack of practitioner awareness of autistic experiences undermined feeling safe, and perpetuated a sense of vulnerability, strengthening previous literature.6,19
Participant experiences highlight the disenfranchised and stigmatised nature of baby loss as previous baby loss research highlights.24,25 Participants described the strong sense of shame, guilt, and blame related to the deaths of their babies.13,17 For autistic people AFAB, a lifetime of being perceived differently, autistic stereotypes, and an internalised sense of worthlessness perpetuated these experiences. 28 Stigmatising narratives and stereotypes surrounding autism, for example, the lack of understanding of sensory differences, such as pain and interoception, might have contributed to participants’ sense of feeling belittled, infantilised, and not believed in relationship to practitioners. This adds to the broader stigma surrounding baby loss, with people AFAB feeling that their bodies do not meet societal and cultural norms in gestating and birthing a baby.29,30
As in baby loss research on the general population, participants described a profound grief, depicted by a sense of emptiness and embodied pain. 16 The findings strengthen understandings of the continued heightened sense of interoception that participants described, as highlighted in autistic perinatal research.4,19,25 Autistic alexithymia (difficulties in identifying and expressing internal experiences, such as emotions) 31 may further contextualize this experience and add to distress for autistic people by not having the words to describe internal experiences of emotions and grief. This could have added a layer of distress in finding the language to make sense of the strong, visceral, and physicality of grief experienced following baby loss. 32 Participants described the importance of continuing bonds, consistent with the baby loss literature more broadly.17,33
Implications for practice
Responding to autistic grief
The study highlights the need for practitioners to understand the breadth of autistic grief experiences and to consider ways to resist societal silence to re-legitimise their valid distress, grief, and baby loss through an autism lens. Signposting to peer-support services, such as Sands, and employing peer-support workers in clinical services could be ways to enact this. 34 This could facilitate connection with others who have experienced baby loss to re-enfranchise and de-stigmatise their experiences.
Autistic-informed perinatal care
The findings add to existing research highlighting the need for practitioners to understand the nuanced experiences of autistic people AFAB, including (1) the loss of safety in predictability, (2) sensory experiences, for example, hyper- and hypo-sensitivities to the seven senses, with specific consideration to interoception and pain, and (3) communication and information processing preferences, such as the necessity of clear, sensitive, specific, personalised and continuous communication. Conversations regarding neurodiversity could be facilitated at the point of service-engagement, which should be documented and inform care.
Collaboration and shared-decision making are also crucial within often unpredictable and changeable medical situations. Practitioners could facilitate sufficient space for autistic people AFAB to ask questions, provide clear explanations and honest answers in antenatal contexts 35 and adopt scripts to restore safety in predictability. 25
Trauma-informed responses to baby loss
The findings highlight the traumatic nature of baby loss and the unique autistic-felt absence of care from practitioners, resulting in feeling belittled, not believed, and infantilised. Trauma-informed principles may be an important approach for services to enact, particularly considering the possible trauma autistic people AFAB may have experienced relationally, and to reduce the risk of re-traumatisation, in line with current guidance.19,36,37
The findings highlight several clinical implications when working directly with autistic people AFAB experiencing psychological distress arising from baby loss. This could include compassion-focused approaches for blame, shame, and guilt as an evidence-based approach for shame-based difficulties with autistic adults.38,39 Process-based models of grief, such as the Dual-Process Model 40 and continuing bonds 32 to re-enfranchise grief could also be integrated into practice; however, consideration to adaptations and the evidence base should be given. Practitioners could hold autism as a lens through which to consider the differences in experiences of grief and support them in navigating bereavement and grief following baby loss, such as identifying more practical and tangible ways of marking and remembering the loss of a baby. This could include exploring the meaning of significant places or objects to remember and reconnect with their babies.
Strengths and limitations
To the best of our knowledge, this is one of the first empirical studies exploring autistic people AFAB’s experiences of baby loss utilising IPA to center subjective, lived experiences. This was a strength to re-legitimise and de-silence participants’ experiences in an area that is silenced, including baby loss and death, at the intersection with autism. A further strength was the adoption of neuro-affirmative approaches throughout the research process. Examples of implementation include the use of equitable requirements, which centered individual needs and preferences in line with each participant’s neurotype, to ensure that people could participate and share their experiences of baby loss more meaningfully.
However, one limitation is the small sample size. Most participants were between 35 and 54 years old, female, with she/her pronouns, from predominantly white western cultural backgrounds. While within an IPA methodology, representation and generalisability are not the aim, this poses the question of whose voices are not represented. Autistic people AFAB who have multiply intersecting marginalised identities might have different experiences, which could further deepen our understanding of autistic experiences of baby loss. 41 These would be valuable avenues for future research to inform equitable health care services for all autistic people AFAB.
Conclusions
Across neurotypes, baby loss is a devastating experience, but this research has helped us to understand the unique challenges experienced by autistic people AFAB. IPA facilitated hearing directly from participants to stand in their shoes, listen to, and feel the trauma, shame, blame, and grief they have endured through losing and living physically without their babies. We learnt of their babies’ meaningful and beautiful lives, and the need to resist the silence to ensure their lives are remembered and participants’ grief and pain honoured. These are important findings which should be utilised to reflect on and resist further layers of misinterpretations of the autistic experience that may limit us from listening to and better supporting autistic people AFAB in navigating the “heart crushing” reality, as described by Adreinne, of baby loss.
Authorship Confirmation Statement
Conceptualization: P.T. identified the ideas based on professional experience and consulted with L.N. with significant expertise in perinatal and family health research work. This work was initially developed as part of P.T. Doctorate in Clinical Psychology course. Formal analysis: P.T. completed formal data analysis independently as part of the Doctorate in Clinical Psychology course. Consultation with the L.N. and S.D. helped with this process as part of self-reflexivity and the reflective process. Funding acquisition: This was not applicable. Investigation: Data collection was completed independently by P.T. with regular check-ins and discussions with the L.N. and S.D. Methodology (development or design of methodology; creation of models): P.T. was responsible for the completion of this research, including delegating and making decisions as part of the requirements for the Doctorate in Clinical Psychology course. Consultation and discussion in research supervisory meetings with L.N. and S.D. supported this process. Project administration (management and coordination responsibility for the research activity planning and execution): P. T. was responsible for the completion of this research, including delegating and making decisions as part of the requirements for the Doctorate in Clinical Psychology course. Resources: P. T. created and constructed all study materials with consultation from EbE consultants and L.N. and S.D. Supervision: P. T. was responsible for the completion of this research, including delegating and making decisions as part of the requirements for the Doctorate in Clinical Psychology course. L.N. and S.D. were part of the wider research supervisory team with expertise in perinatal experiences and autistic experiences, respectively, to support with decision making. Validation: P.T. completed all associated works independently but with consultation from the wider research team (L.N. and S.D.), who can verify the output and findings and completion of this research. Writing—original draft, reviewing and editing: P.T. wrote the first draft of the article. L.N. and S.D. contributed to reviewing and editing, including managing the word count prior to submission. The article has been submitted solely to Autism in Adulthood.
Footnotes
Acknowledgements
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding required for this project, as this output arose from P.T.’s Doctorate in Clinical Psychology course.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.