
Abstract
Background:
Autistic people face multiple barriers to health care. To recognize specific barriers in a standardized way, autistic people, health care providers, and researchers need a suitable measure. The Academic Autistic Spectrum Partnership in Research and Education successfully developed the Barriers to Healthcare Checklist—Short Form (BHC-SF). It remains unclear whether (1) a German version of the BHC-SF performs well in terms of psychometric properties and (2) the BHC-SF consists of multiple constructs (i.e., assessing structural validity).
Methods:
We created a translated and culturally adapted version of the 17-item BHC-SF and used it with 345 autistic people in Germany. Psychometric analyses included calculations to test for internal consistency reliability (Cronbach’s α) and construct validity (i.e., a priori hypothesis tests for correlations with previous treatment termination and statements about barriers to health care in terms of lack of knowledge, participation, autism-specific needs, lack of services, access/financing and collaboration). We conducted an exploratory factor analysis (EFA) to investigate the presence of BHC-SF subscales (i.e., structural validity) and performed reliability and validity calculations where appropriate.
Results:
The average BHC-SF total score was mean = 8.05 (standard deviation = 4.05), with more barriers for persons who identified as female compared with males. The BHC-SF total score revealed good internal consistency reliability (Cronbach’s α = 0.82). The assessment of construct validity mainly supported the hypothesized associations. The EFA identified four BHC-SF subscales, for which we found lower psychometric support with respect to internal consistency reliability and construct validity.
Conclusions:
The German version of the BHC-SF demonstrates good internal consistency reliability and construct validity. We identified four different constructs underlying the BHC-SF. The derived subscales need further psychometric testing. Use of the BHC-SF total score could potentially help health care providers and researchers systematically identify and address barriers to health care for autistic patients.
Community Brief
Why is this an important issue?
Autistic people often have trouble getting health care. A questionnaire about previous problems could help make appointments in the future easier and reduce barriers.
What was the purpose of this study?
The Barriers to Healthcare Checklist—Short Form (BHC-SF) is a short questionnaire developed by the Academic Autistic Spectrum Partnership in Research and Education. This questionnaire lists 17 barriers to healthcare that autistic people often face. People report whether or not they have experienced each barrier. The purpose of the study was to see if a German translation of the questionnaire works well. We also wanted to understand whether we should treat all barriers listed in the BHC-SF questionnaire as one big group or whether it is better to think of them as smaller groups.
What did the researchers do?
We created a German version of the BHC-SF questionnaire and tested it on 345 autistic adults. We counted the number of barriers each participant experienced (BHC-SF total score) and used these data to investigate if the BHC-SF total score changed with respect to age or gender. We checked the psychometric properties of the BHC-SF questionnaire (internal consistency reliability and construct validity) to see if the German version works well. In addition, we examined whether the BHC-SF questionnaire has subscales (representing smaller groups of barriers) and checked their psychometric properties (reliability and validity), too.
What were the results and conclusions of the study?
We successfully developed a German version of the BHC-SF questionnaire. The mean number of reported barriers was 8 out of 17. Women reported more barriers to health care than men. The psychometric analyses revealed very good results regarding the test’s global ability to measure barriers to health care. As predicted, people who reported more barriers in the BHC-SF questionnaire more often reported treatment termination and higher agreement with other statements about barriers to health care (i.e., in terms of lack of knowledge, autism-specific needs, and access/financing). Thus, the BHC-SF total score seems to be a good tool to assess barriers to health care in a structured way. In addition, we identified four potential BHC-SF subscales, reflecting different types of barriers. However, the results of psychometric analyses for these subscales were not as strong. Further research is needed to check if these subscales can be improved. In conclusion, the German version of the BHC-SF works well and is a brief tool for identifying barriers to health care for autistic people. Use of the BHC-SF could provide health care professionals with important information about barriers experienced by autistic people.
What is new or controversial about these findings?
This is the first assessment of the German translation of the BHC-SF. At the moment, it seems more reasonable to see the barriers listed in the BHC-SF as one large group. We found the first hints that different smaller groups are represented in the BHC-SF list, but the questionnaire’s structure might need improvement to reliably measure them.
What are potential weaknesses in the study?
The results reflect only a subsample of autistic people who were able to participate in a comprehensive online survey.
How will these findings help autistic adults now or in the future?
A better understanding of barriers to health care can help health care professionals try to improve access to health care and reduce barriers for autistic people.
Background
Autistic people have poorer physical and mental health compared with the general population.1–3 Many autistic individuals have significant difficulties accessing the demands of daily life4,5 and experience premature mortality.6–8 In particular, autistic adults have increased health needs compared with adults without autism.9–12 This finding includes a higher prevalence of physical and mental health problems,12–15 suicidality and suicide attempts, 16 emergency contacts,17,18 as well as reduced overall quality of life19,20 and health-related quality of life.21,22 Despite these increased health needs,1,10–12,18 autistic adults are less likely to receive needed care11,21,23–26 and to experience less satisfaction with provided care 26 compared with the general population.
Barriers to access health care are a priority issue for autistic people regarding the overall use of health services.11,18,26 Several review articles reported a wide range of multifactorial barriers at the individual level (e.g., verbal communication skills), professional level (i.e., knowledge about autism), and organizational level (e.g., complexity of the health care system) that impede access to health care for autistic individuals.24,27–29 The impact of barriers changes across the lifespan, with barriers such as lack of services, limited insurance, difficulties in communicating with physicians, and limited awareness of the health needs of older adults being particularly significant for autistic people. 30 Consequences of barriers included increased levels of anxiety in autistic individuals during treatment or reduced self-rated quality of health,2,3 and adverse health outcomes, like lack of consultation for necessary treatment or screening programs, or extensive treatment due to late presentation. 31 The literature includes several proposals to improve access to health care for autistic people,21,24,25,32–34 but larger empirical studies and evaluations are lacking to date.
To improve access to health care, the systematic exploration of existing barriers for autistic people seems necessary. Such data could help to decide which adaptations are needed to improve access and would enable the evaluation of these interventions. 30 Most previous studies collected data on barriers by using in-depth questionnaires/surveys2,31,35 or interviews/focus groups.36–38 Raymaker and colleagues (2017) reported on a short version of the Barriers to Healthcare Checklist (BHC; 41 items). The BHC was developed by the Academic Autistic Spectrum Partnership in Research and Education (AASPIRE), 39 and the authors reported sufficient content and construct validity for the original version as well as a short version called Barriers to Healthcare Checklist—Short Form (BHC-SF; 17 items). 35 Health care providers can use data from the BHC-SF in two ways: First, the BHC-SF total score can be a quantitative indicator for experienced barriers (i.e., how many barriers did a person experience). Second, responses to individual items can be a qualitative indicator for experienced barriers (i.e., in which area did a person experience barriers). The authors discussed as a potential limitation that this instrument may not be sufficient for the full spectrum, but it seemed appropriate for autistic adults without co-occurring intellectual disability (ID). Interestingly, the BHC and BHC-SF reported different patterns of barriers within autistic adults compared with other populations (i.e., non-autistic, disabled adults and non-autistic, non-disabled adults). Thus, the authors reported patterns of barriers specific to autistic people, including issues such as emotional reactions, communication with health care providers, sensory sensitivity, and navigating through the health care system. 35 An intervention study reported sufficient responsiveness to change between pre- and post-assessment with the BHC-SF (Cohen’s d = 0.55). 38 These previous results make the BHC-SF a promising brief tool to assess barriers to health care in autistic adults without co-occurring ID.
We had two aims for the current study. Aim 1: To develop a translated and culturally adapted version of the BHC-SF. For this purpose, we analyzed different aspects of measurement properties: (i) Reliability: We investigated the internal consistency. (ii) Construct validity: (a) Using hypotheses testing, we hypothesized that a higher BHC-SF total score would be associated with experience of treatment discontinuation and higher agreement with statements about barriers to health care (identified in a previous study 37 ); (b) structural validity using confirmatory factor analysis (CFA), which tests the assumption that the BHC-SF total score reflects mainly one factor. Aim 2: In case that the CFA for the BHC-SF total score does not fit the data, we planned to investigate whether the BHC-SF consists of subscales reflecting different types of barriers using exploratory factor analysis (EFA, i.e., principal component analysis [PFA]). As reported in the literature, different types of barriers to health care exist,27,29,30 and their recognition could help to improve access for autistic people. Thus, identifying different types of barriers could help to guide the implementation of specific measures to facilitate access for an autistic person. Overall, the current study hopes to contribute to the evaluation of potential field applications of the BHC-SF as a standardized, time-sensitive questionnaire for use in different health care settings.
Methods
We collected the reported data in a Germany-wide participatory research project (BarrierfreeASD) while investigating barriers and facilitators in the health care of autistic adults without co-occurring ID. 40 In this project, we examined three groups of people: autistic adults, relatives, and health care professionals. The BarrierfreeASD working group is a neurodiverse team, and we worked in close collaboration with various partners. These partners included associations of autistic adults or their families, service providers and clinicians, and health care researchers. We regularly discussed our research project with these cooperation partners and jointly reviewed, discussed, and adapted study materials. The local psychological ethics committee of the Centre for Psychosocial Medicine at the University Medical Center Hamburg-Eppendorf (LPEK-0227) approved this study. For the purposes of this article, we limit our analysis to a subsample of data collected from autistic people in one of the online surveys conducted in the research project BarrierfreeASD.
Participants
A total of 408 autistic adults participated in this study. Inclusion criteria for autistic people were as follows: (1) confirmed diagnosis of autism spectrum disorder, (2) at least 18 years of age, (3) sufficient German and language skills, and (4) no confirmed diagnosis of co-occurring ID. We excluded participants whose data did not meet the inclusion criteria or who did not provide information on the inclusion criteria. To ensure the authenticity of participant responses and adherence to inclusion criteria, several validity checks were incorporated to identify non-genuine responses. Responses failing these checks were excluded from analyses.
Procedure
To recruit participants, J.P., N.D., and S.D. disseminated study information through cooperation partners, social media, and freely accessible online contacts (e.g., public homepages). All participants gave written informed consent before completing the online survey. 41 Participants reported on the requested inclusion criteria during the first section of the online survey (self-report). First, participants reported sociodemographic data, followed by questions about barriers to health care. Last, participants reported on several clinical outcomes (for details, see the “Materials” section). Data collection was anonymous, and participants did not receive compensation. Data were collected, processed, and stored in accordance with the EU General Data Protection Regulation. Data were collected as part of a larger nationwide online survey, 40 programmed in LimeSurvey. The survey consisted of several sections, asking for inclusion–exclusion criteria, sociodemographic variables, previous experiences with health care, and clinical outcomes. In addition, the survey asked about use of health care and quality of life (this information is not part of the current article and will be reported elsewhere). Completion of the survey lasted between 20 and 45 minutes.
Materials
Sociodemographic variables and clinical outcomes
Sociodemographic variables included age (in years), gender (female, male, other), education (more than 10 years, 10 years, 9 years, not graduated, still in school), monthly income (less than 500 Euro, increasing by 250 Euro steps up to 1500 Euro, increasing by 500 Euro steps up to 4000 Euro, more than 4000 Euro), work situation (full-time, part-time, student, unemployed, other), and type of health insurance (public, private). We did not collect specific data on race/ethnicity.
Clinical variables included the presence of somatic and/or mental co-occurring conditions (number), intensity of social support in the past 6 months (in days), and treatment discontinuation (“Did you ever discontinue medical treatment because you felt that your difficulties as an autistic adult were not properly identified and/or treated?”; yes/no). Participants rated the severity of their autistic characteristics according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) 42 criteria by using items that were formulated by our research group: (1) Autistic characteristics related to interaction “How much support do you need because of difficulties with interpersonal communication and social interactions?” (DSM-5 Interaction), (2) Autistic characteristics related to behavior “How much support do you need because you persist in behavioral habits, routines, or interests that are important to you (e.g., difficulties with self-organization or dealing with change)? (DSM-5 Behavior). Participants responded to each item on a 5-point Likert scale with the options “none—little—moderate—quite—very.”
Translation and cross-cultural adaptation of the BHC-SF
We followed the standardized procedure of the European Organization for Research and Treatment of Cancer Quality of Life Group. 43 Two German native speakers (J.P. and T.H.) independently translated all the items of the original BHC-SF 35 from English into German. A third person (N.D.) reviewed the two translated versions before a group of coauthors (J.P., N.D., S.D., P.G., H.K., H.S.) discussed and agreed on the final German translation. No Germany-specific adaptations were necessary after inspection of the final item set. Two native English speakers (professional translators) independently back-translated the agreed BHC-SF version into English. Three of the authors (J.P., N.D., S.D.) compared these back-translated versions with the original English version and discussed and resolved any discrepancies. J.P. discussed remaining issues with the original authors (D.R., C.N.). Two autistic project members who were not involved in the previous translation process piloted the German version of the BHC-SF and provided feedback on its applicability and feasibility. After this step, we considered the cross-cultural adaptation complete. Following the original English version of the BHC-SF, 35 the German version consisted of 17 items. Each item reflected a barrier to health care, and participants responded by checking “yes” or “no” (binary response). To calculate a BHC-SF total score, we summed all “yes” responses across barriers. The resulting BHC-SF total score ranges from 0 to 17.
Statements about barriers to health care (BarrierfreeASD)
It includes 32 items that aim to assess potential themes of barriers to health care for autistic adults. The six themes are: (T1) knowledge (5 statements), (T2) participation (3 statements), (T3) autism-specific needs (4 statements), (T4) lack of services (16 statements), (T5) access/financing (3 statements), (T6) collaboration (1 statement).
Each item is a statement, and participants score their level of agreement with each statement on a 5-point Likert scale (from 1 = “not true” to 5 = “very true”). In addition, an “I don’t know” response was available. To calculate a total score of agreement for each theme (T1–T6), we calculated the mean value of the corresponding items (again ranging from 1 = “not true” to 5 = “very true”). For scoring purposes, we conservatively scored “I don’t know” responses as “not true” responses (value = 1). As a result, we calculated six scores for each person (one for each theme). These scores reflect the level of agreement with the presented statements about barriers to health care in Germany.
The provided statements are based on results of a previous study 37 and were reviewed by the BarrierfreeASD research group and agreed upon jointly (for details, see Supplementary Table S1). Consensus was reached based on the procedure for nominal group processes. 44
Data analyses
Of the N = 408 participants, N = 61 terminated the online survey before starting the BHC-SF and N = 2 started but did not complete the questionnaire. This results in a final sample of N = 345 persons. Missing data were not imputed, and all statistical calculations were performed with SPSS version 27. 45
We calculated the mean (M), standard deviation (SD), and mode of the BHC-SF total score. To test the normality of the data, we calculated the skewness and kurtosis. For interpretation, we considered a skewness <−1 or >1 high, a skewness between −1 and −0.5 or between 0.5 and 1 moderate, and a skewness between −0.5 and 0.5 approximately symmetric. We considered a kurtosis of <3 to indicate fewer and less extreme outliers than the normal distribution and a kurtosis >3 to indicate more outliers than the normal distribution. We investigated whether to include age or gender when interpreting the BHC-SF total scores. For this purpose, we calculated Pearson’s correlation between the BHC-SF total score and age and performed a one-way analysis of variance with the factor gender (simple contrast: female). We checked whether the BHC-SF score was normally distributed (skewness and kurtosis) as described above prior to these analyses. We calculated the corrected item–total correlation for each item of the BHC-SF. A value of <0.3 indicates that the corresponding item may not correlate very well with the total score of the scale.
Psychometric analyses of the BHC-SF were adapted from the COSMIN checklist for PROM.46,47 With respect to internal consistency reliability, we calculated Cronbach’s α to examine internal consistency. To assess construct validity, we tested the hypotheses that the BHC-SF total score is positively associated with experience of treatment termination (Hypothesis 1) as well as higher agreement with statements about barriers to health care based on lack of knowledge (T1), participation (T2), autism-specific needs (T3), lack of services (T4), access/financing (T5), or collaboration (T6) (Hypotheses 2–7). For construct validity analyses, we conducted hypothesis testing and calculated Pearson’s correlations between the BHC-SF total score and statements about barriers to health care (BarrierfreeASD) as reflected in the six mean scores (T1–T6), and Spearman’s rho between the BHC-SF total score and treatment discontinuation (yes/no). A conservative power calculation using G*Power 48 indicated a required minimum sample size of n = 112 for the detection of a medium effect size of r = 0.30 49 with the planned correlations, based on the parameters power = 0.90 and p = 0.05. In terms of interpretation, we considered r = 0.30 (medium effect size) to be sufficient. 50 In addition, we assessed structural validity and used a CFA (maximum likelihood estimation) with all BHC-SF items on one factor to test for unidimensionality (IBM AMOS 29). We interpreted results according to the following goodness-of-fit indices and cutoffs for a good fit 51 : comparative fit index (CFI) ≥0.95, Tucker–Lewis Index (TLI) ≥0.95, root mean squared error of approximation (RMSEA) ≤0.06, standardized root mean squared residual (SRMR) ≤0.08. We planned to test the existence of multiple constructs underlying the BHC-SF with an EFA if we could not confirm unidimensionality.
To ensure the data are appropriate for EFA, we calculated the Kaiser–Meyer–Olkin (KMO) measure and the Bartlett’s test for sphericity. To conduct the EFA, we calculated a PCA followed by varimax rotation. We considered all factors with eigenvalues greater than 1 as relevant. We interpreted factor loadings as follows: ≥0.71 = excellent, 0.64–0.70 = very good, 0.55–0.63 = good, 0.46–0.54 = fair, and 0.32–0.45 = poor. 52 We considered factor loadings below 0.32 to be too low because such a factor can only explain approximately 10% of the variance in the variable and did not consider them. For each potentially identified BHC-SF subscale, we planned the calculation of the corrected item–total correlation and internal consistency reliability. To investigate construct validity for identified BHC-SF subscales, we plan to define and test a priori hypotheses between the potential subscales and corresponding sample characteristics.
Results
Participants
We have summarized sociodemographic and clinical characteristics in Table 1. A total of 345 autistic adults with a mean age of 38.7 years (SD = 11.5, range 18–65 years) completed the German version of the BHC-SF, of whom 55.9% identified themselves as female. A large proportion of the sample had at least 12 years of education (69.6%), were currently unemployed/permanently not working (23.2%), had a monthly household income of <2000 Euros (50.1%), and were members of the German mandatory statutory health insurance system, which covers most of health care costs (91.6%).
Sample Characteristics (N = 345)
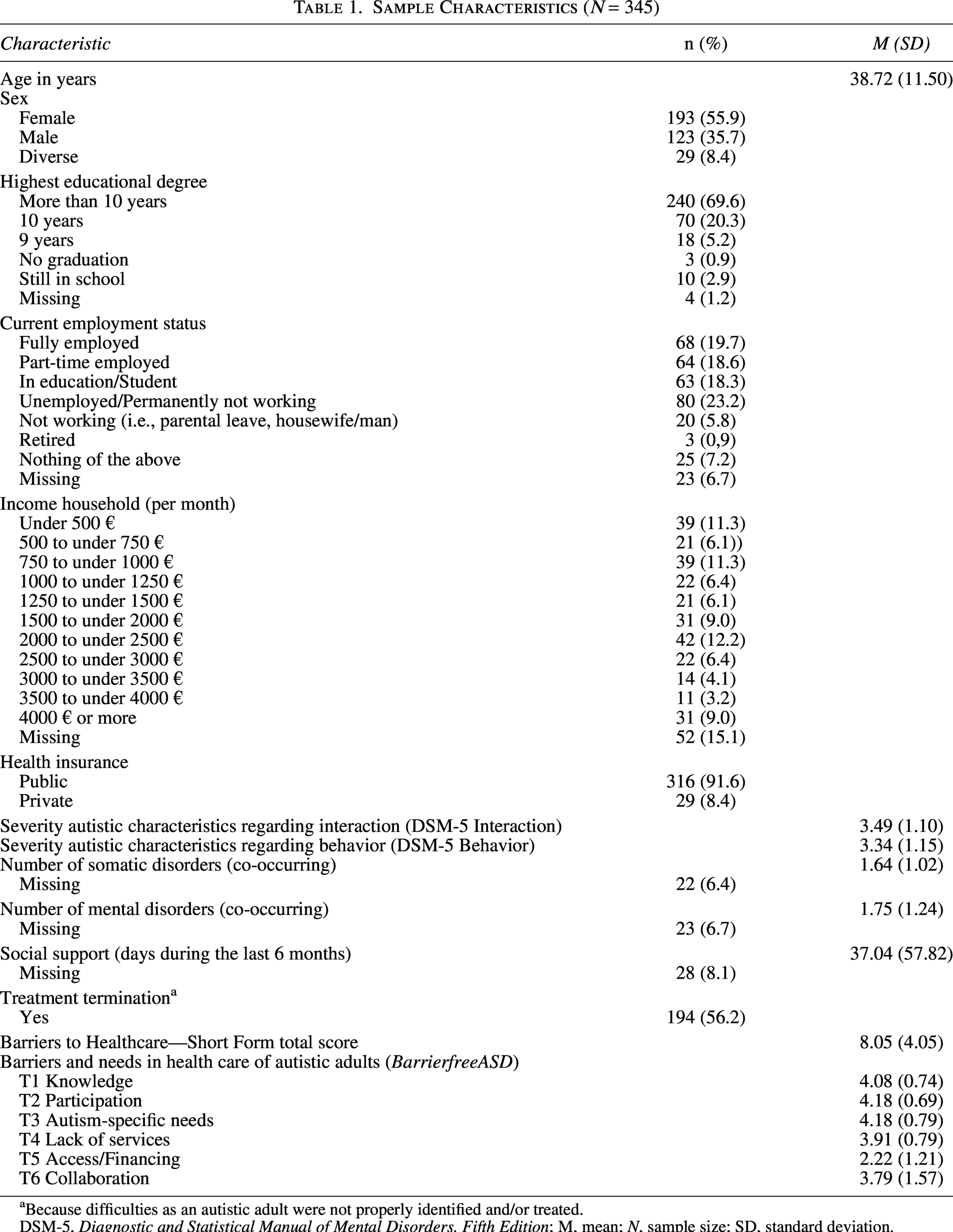
Because difficulties as an autistic adult were not properly identified and/or treated.
DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; M, mean; N, sample size; SD, standard deviation.
Barriers to Healthcare Checklist—Short Form
The frequency of BHC-SF total scores within the current sample is shown in Figure 1. The total score of the BHC-SF showed the following parameters: M = 8.05, SD = 4.05, range from 0 to 17, median = 8, and mode = 11. The skewness was −0.1, indicating that the distribution was slightly skewed to the left but can be considered approximately symmetric. The kurtosis was −0.83, indicating that the distribution tends to produce fewer and less extreme outliers than the normal distribution. Based on these results, we still consider the data to be normally distributed.

Frequency of BHC-SF total scores (N = 345). BHC-SF, Barriers to Healthcare Checklist—Short Form.
We found no association between the BHC-SF total score and age (r = 0.09, p = 0.097). With respect to gender categories, the BHC-SF total score differed over groups [F(2,342) = 8,59, p < 0.001]. The difference in BHC-SF total scores between persons who identified as female (n = 193, M = 8.44, SD = 3.83) or as male (n = 123, M = 6,99, SD = 4.21) was significant (−1.45, p = 0.002), the difference between persons who identified as female or as diverse (n = 29, M = 9,93, SD = 3.76) was not significant (+1.49, p = 0.060).
Item analysis
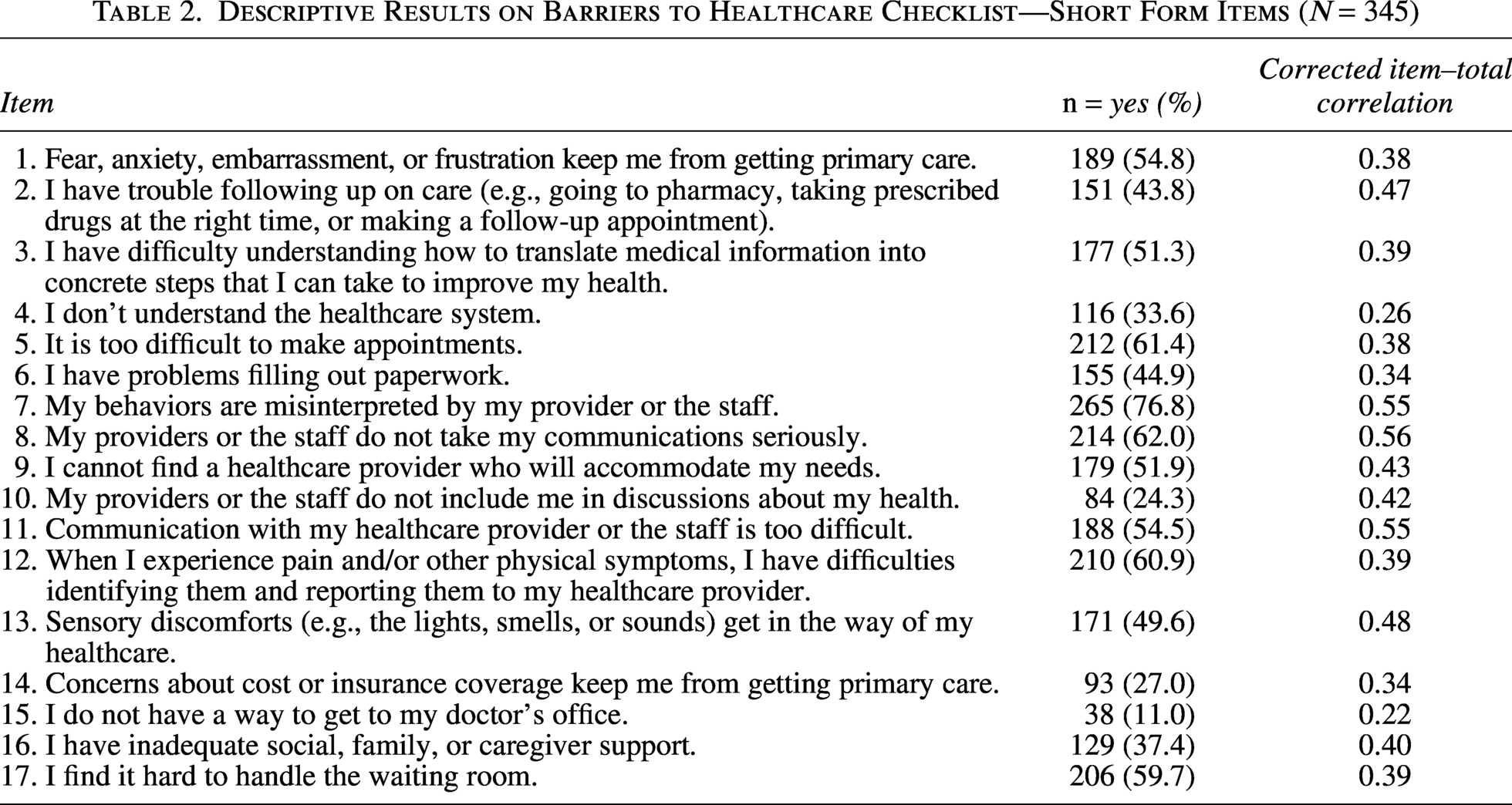
Table 2 shows the results for each of the BHC-SF items. The four most frequently reported barriers to healthcare were “My behaviors are misinterpreted by my provider or the staff.” (reported by 76.8%), “My providers or the staff do not take my communications seriously.” (reported by 62.0%), “It is too difficult to make appointments.” (reported by 61.4%), and “When I experience pain and/or other physical symptoms, I have difficulties identifying them and reporting them to my health care provider.” (reported by 60.9%). The three least frequently reported barriers were “I do not have a way to get to my doctor’s office.” (reported by 11.0%), “My providers or the staff do not include me in discussions about my health.” (reported by 24.3%), and “Concerns about cost or insurance coverage keep me from getting primary care.” (reported by 27.0%). As shown in Table 2, the corrected item–total correlations ranged from 0.22 to 0.56.
Descriptive Results on Barriers to Healthcare Checklist—Short Form Items (N = 345)
Reliability
Internal consistency was very good for the BHC-SF total score (Cronbach’s α = 0.82) and did not improve with item deletion.
Construct validity
Hypotheses testing
For construct validity, we found weak to moderate positive correlations for the BHC-SF total score with statements about barriers to health care (T1–T6), with significant correlation coefficients between r = 0.16 (p = 0.004) and 0.43 (p < 0.001). Correlations of at least 0.30 were revealed for lack of knowledge (T1; r = 0.30, p < 0.001), autism-specific needs (T3; r = 0.43, p < 0.001), and access/financing (T5; r = 0.34, p < 0.001). We found a moderate positive correlation of the BHC-SF total score with previous treatment terminations (r = 0.41, p < 0.001). Detailed information about correlations between the BHC-SF total score and validity constructs is shown in Table 3.
Correlations Between Barriers to Healthcare Checklist—Short Form Total Score and Validity Constructs (N = 345)
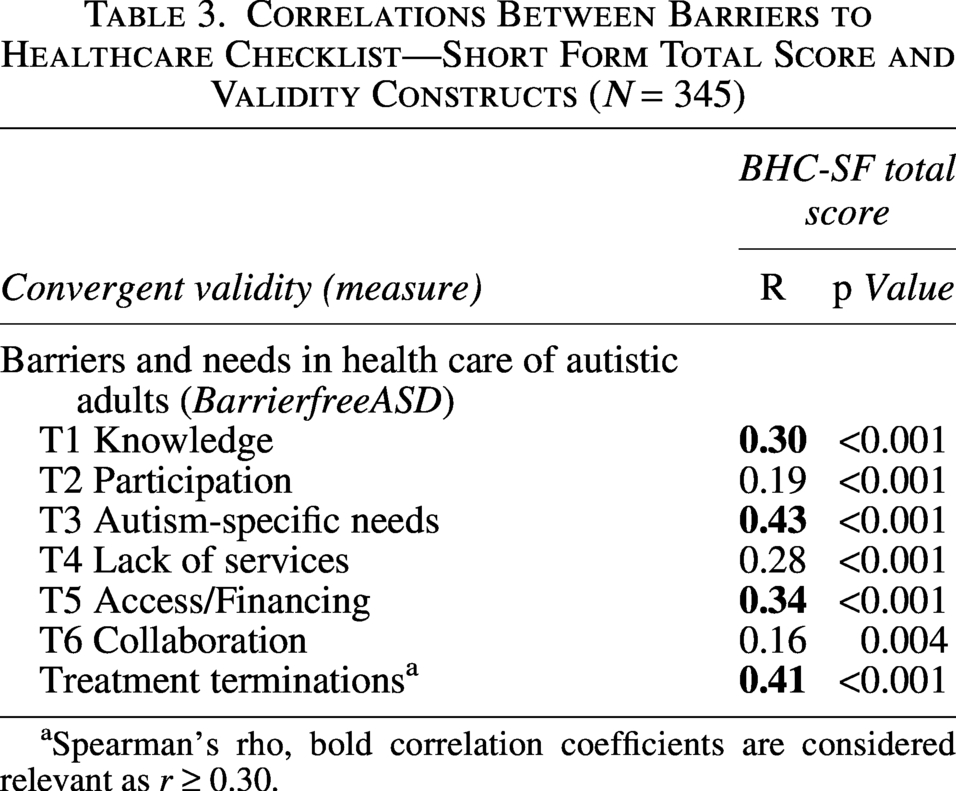
Spearman’s rho, bold correlation coefficients are considered relevant as r ≥ 0.30.
Structural validity
To assess structural validity, we conducted a one-factor CFA. Goodness-of-fit indicators were as follows: CFI = 0.766, TLI = 0.732, RMSEA = 0.080, SRMR = 0.067. Results indicated that all four parameters did not meet the specified thresholds for a good model fit, meaning the model’s theoretical structure is not an adequate representation of the data and relationships between variables.
Exploratory factor analysis
Based on the CFA’s results, we performed an EFA applying a PCA. The KMO index was 0.82, exceeding the recommended value of 0.6, 53 and Bartlett’s test for sphericity 54 reached statistical significance (χ2 = 1234.15, p < 0.001), indicating that our data were suitable for EFA. The eigenvalues from the exploratory PCA suggested a dominant first factor (eigenvalue 4.4; 26.06% of the variance), with the second through fourth factors having eigenvalues ranging from 1.44 to 1.08 (22.76% of the variance). See the Supplementary Material for details of the factor loadings and communalities for each of the BHC-SF items (Supplementary Table S2) and the screeplot (Supplementary Fig. S1). We used the four-factor solution to construct BHC-SF subscales.
BHC-SF subscales (description, reliability, and construct validity)
Based on the previously reported EFA, we defined the following BHC-SF subscales:
Subscale 1 (Interaction with health care providers): The first factor is based on items 7–11, all of which focus on communication difficulties (e.g., lack of understanding/inclusion; misinterpretation) between the autistic person and the respective health care providers. Subscale 2 (Intrapersonal difficulties in treatment): The second factor is based on items 1–3 and items 5 and 12, which primarily reflect difficulties that the autistic person experiences within themselves in the treatment situation (e.g., emotions; difficulties in performing the required task). Subscale 3 (Structural difficulties): The third factor is based on items 4, 6, 14–16, which focus on difficulties with more general aspects of health care access (e.g., paperwork, cost, lack of support). Subscale 4 (Sensory specificities): The fourth factor is based on items 13 and 17, which focus on difficulties due to sensory specificities (e.g., waiting room, sensory discomfort).
With respect to reliability, internal consistency scores of the subscales were heterogeneous, with Cronbach’s α ranging from low (0.54) to acceptable (0.77), with no improvement after item deletion (for details, see Supplementary Table S3). The subscales were significantly correlated with each other (all correlations above 0.30): Subscale 1 was significantly correlated with subscale 2 (r = 0.47, p < 0.001), Subscale 3 (r = 0.38, p < 0.001), and subscale 4 (r = 0.41, p < 0.001). Subscale 2 was significantly correlated with subscale 3 (r = 0.35, p < 0.001) and subscale 4 (r = 0.39, p < 0.001). Subscale 3 was significantly correlated with subscale 4 (r = 0.32, p < 0.001).
To explore construct validity, we formulated the following a priori hypotheses for each BHC-SF subscale: Subscale 1 (Interaction with health care providers) is positively associated with (i) severity of autistic characteristics regarding interaction and (ii) agreement with the statement “Based on my personal experience, the special needs of my way of communicating should be more considered in the treatment.” (cf. Supplementary Table S1, Item 9). Subscale 2 (Intrapersonal difficulties with treatment) is positively associated with the number of mental disorders (co-occurring). Subscale 3 (Structural difficulties) is positively associated with (i) agreement with statements about barriers to health care based on access/financing (T5), (ii) social support (days during the last 6 months, (iii) agreement with the statement “Based on my personal experience, I need more support to organize myself in order to benefit from my treatment.” (cf. Supplementary Table S1, Item 12). Subscale 4 (Sensory specificities) is positively associated with agreement with the statement “Based on my personal experience, the specifics of my stimulus processing should be taken into account more in the treatment.” (cf. Supplementary Table S1, Item 10). To test these hypotheses, we calculated Pearson’s correlations (for details, see Supplementary Table S4). Significant correlations of at least about 0.30 existed between:
Subscale 1 (Interaction with health care providers) and the statement “Based on my personal experience, the special needs of my way of communicating should be more considered in the treatment.” (r = 0.34, p < 0.001) and the statement “Based on my personal experience, the specifics of my stimulus processing should be taken into account more in the treatment.” (r = 0.34, p < 0.001); Subscale 3 (Structural difficulties) and the statement “Based on my personal experience, I need more support to organize myself in order to benefit from my treatment.” (r = 0.29, p < 0.001); Subscale 4 (Sensory specificities) and the statement “Based on my personal experience, the specifics of my stimulus processing should be taken into account more in the treatment.” (r = 0.36, p < 0.001).
Discussion
We successfully administered a translated and culturally adapted BHC-SF version to a large sample of autistic people in order to analyze the psychometric properties of the German BHC-SF. Based on the distribution of sociodemographic and clinical variables, we believe that our sample largely reflects a representative group of autistic people without co-occurring ID in Germany. The BHC-SF total scores in our sample ranged from 0 to 17, with an average of eight reported barriers. Looking at the most prominent barriers, over 75% reported that “My behaviors are misinterpreted by my provider or the staff,” and over 60% reported that “My providers or the staff do not take my communications seriously,” “It is too difficult to make appointments,” and “When I experience pain and/or other physical symptoms, I have difficulties identifying them and reporting them to my healthcare provider.” Thus, consistent with other research,30,32 communication with professionals appeared to be a key barrier for autistic adults. We found higher BHC-SF total scores in persons who identified as female compared with persons who identified as male. This finding is in line with previous research that reported more barriers to access health care for women and girls, as well as other gender persons on the autism spectrum, compared with autistic men and boys.55–57 In our sample, we found that for persons who identified as diverse, the highest average BHC-SF total score was. Due to the small sample size (n = 29), the difference with persons who identified as female became insignificant. Still, recent findings pointed out that autistic people who identify as LGBTQ+ experience greater disparities in physical and mental health, as well as unmet health care needs.56,58 Overall, further research seems necessary to understand the impact of gender identity aspects on experienced barriers to healthcare for autistic adults and to provide sufficient adjustments.
The first aim of our study was a psychometric evaluation of the German version of the BHC-SF: The psychometric analyses for the BHC-SF total score yielded very good psychometric results in terms of internal consistency reliability (Cronbach’s α = 0.81) and item-scale characteristics. The corrected item–total correlation scores revealed that only 2 out of 17 items scored below 0.30, which supports the general structure of the German version of the BHC-SF. In addition, the lack of missing data in specific items supports the overall acceptability of this tool in autistic people.
To test for construct validity (hypothesis testing), we correlated the BHC-SF total score with statements about barriers to health care identified in a previous study (BarrierfreeASD) 37 and expected more agreement with statements in autistic persons who reported more barriers to healthcare in the BHC-SF.
In line with our hypotheses, we found positive associations between the BHC-SF total score and agreement with statements about lack of knowledge about autism (T1), lack of consideration of autism specific needs (T3), and difficulties with access and financing (T5). These associations appear to make sense, as individual items of the BHC-SF reflect experiences in specific treatment situations with practitioners and experiences with the care system. In these situations, the practitioner’s knowledge and ability to adapt to special needs, as well as the general context in terms of funding and access, are certainly of particular importance. Previous literature reported that lack of knowledge about autism and lack of consideration of autism specific needs are important barriers for access to health care.30,59 Accordingly, the level of training of health care professionals is highly relevant for successful access to health care for autistic people. 60 Publications include several options for adjustments to improve consultation settings, for example, the Online Healthcare Toolkit for Autistic Adults and their Primary Care Providers 38 provides materials (e.g., the Autism Healthcare Accommodations Tool, checklists and resources for autistic persons and health care providers) or suggestions on adapting the waiting room area or processes during the treatment situation. 61 Complexity beyond the usual role or the need for training to provide adequate treatment for autistic people were reported as limiting aspects for practitioners, 28 and further research is needed to investigate successful implementation of adjustments. In terms of financial barriers, statutory health insurance in Germany covers a large proportion of outpatient treatment costs. Treatment services for autistic adults are not always available as standard options, and autistic persons may face long wait times or have to use alternative funding systems to access them. Other studies also reported limited financial capacity and lack of services as highly relevant barriers.30,62
In contrast to our hypotheses, the BHC-SF total score showed only weak associations (r < 0.30) with statements about the three remaining themes (i.e., participation, lack of services, collaboration). These themes reflect types of barriers that occur more outside of the specific treatment situation (e.g., availability of structures and exchange between treatment providers) and might therefore not be represented in the BHC-SF total score. Since participation is strongly related to the communication between an autistic person and the practitioner, we were surprised to find no association with the BHC-SF total score. Further research is needed to further investigate this result.
Another aspect of construct validity was the relationship between previous treatment terminations and the BHC-SF total score. Over 50% of our sample reported treatment termination because their health care providers were not properly identifying and/or treating their difficulties as an autistic person. As assumed, a higher BHC-SF total score was associated with the experience of treatment termination (statistically reflected in a strong positive correlation). This finding is in line with research reporting adverse health care outcomes for autistic persons like untreated physical and mental health conditions 31 and higher rates of emergency contacts. 11 As we only asked about treatment termination in a yes/no format, no conclusions can be drawn about the individual reasons for discontinuation.
We interpret the psychometric results reported above as indicators of the successful cross-cultural validity of the German version of the BHC-SF. In terms of interpretability, the use of the BHC-SF total score indicates the number of barriers experienced, which may help health care providers assess support needs. In addition, information from individual items can be used to develop individualized adjustments to improve access to health care with the autistic person. Such an approach is consistent with projects such as the AASPIRE toolkit, 38 and recent proposals to improve communication with autistic adults in health care.61,63 The fact that assessment of barriers is relevant for autistic persons is supported by a recent study, which found that a higher number of barriers assessed by the BHC-SF was associated with lower confidence in individual and relationship-dependent health care self-efficacy, lower feelings of preparedness for visits, and lower likelihood to receive necessary accommodations. 64 Our own group recently showed that the BHC-SF total score was able to explain differences in health-related quality of life in autistic adults. 3 Thus, we suggest using the BHC-SF prior to appointments and sharing the results with health care providers.
The second aim of our study was to investigate whether the BHC-SF consists of subscales, reflecting different types of barriers: Looking at the literature on barriers to health care in autistic persons, several levels and types of barriers were previously reported.27,30,37 Consideration of such BHC-SF subscales could allow for more individualized suggestions to improve access to health care.
To investigate this question, we assessed the structural validity of the BHC-SF and found that the BHC-SF seems to reflect more than one factor. Based on the conducted EFA, we identified four BHC-SF subscales: (1) Interaction with health care providers, (2) Intrapersonal difficulties with treatment, (3) Structural difficulties, and (4) Sensory specificities. These BHC-SF subscales would fit into classifications of barriers, 24 for example, subscale 2 and subscale 4 reflect factors on the patient level, subscale 1 on the provider level, and subscale 3 on the system level. The psychometric evaluation of these identified subscales showed lower results for reliability (Cronbach’s α ranged from 0.54 to 0.77) compared with the BHC-SF total score. This may be due to the small number of items for individual scales. The subscales were moderately correlated with each other (r between 0.32 and 0.47). Thus, the subscales seem to share some variance, but the relationships are not extremely strong. This supports the idea that the separate subscales might reflect different subtypes of barriers. More research is needed to determine if different barriers are represented in the BHC-SF.
To examine first hints for construct validity of the identified BHC-SF subscales, we formulated hypotheses for associations between each subscale and corresponding data in our sample characteristics. We based our results on correlation coefficients >0.30.
Subscale 1 included BHC-SF items related to aspects of interaction with health care providers: “My behaviors are misinterpreted by my provider or the staff,” “My providers or the staff do not take my communications seriously,” “I cannot find a health care provider who will accommodate my needs,” “My providers or the staff do not include me in discussions about my health,” and “Communication with my health care provider or the staff is too difficult.” Higher scores on subscale 1 were associated with higher agreement with the statement “Based on my personal experience, the special needs of my way of communicating should be more considered in the treatment” and the statement “Based on my personal experience, the specifics of my stimulus processing should be taken into account more in the treatment.” The a priori postulated association with the severity of autistic characteristics regarding interaction was not supported. Subscale 1 had the greatest impact on the eigenvalue and amount of variance explained in the conducted EFA. As we consider subscale 1 to reflect factors on the provider level, it seems reasonable that items from this subscale are associated with aspects of communication. Communication issues, for example, varying levels of verbal communication, have previously been identified as an important barrier to health care access,11,36 particularly in the context of interactions with health care professionals. 65
Subscale 2 included BHC-SF items related to intrapersonal difficulties: “Fear, anxiety, embarrassment, or frustration keeps me from getting primary care,” “I have trouble following up on care (e.g., going to pharmacy, taking prescribed drugs at the right time, or making a follow-up appointment),” “I have difficulty understanding how to translate medical information into concrete steps that I can take to improve my health,” “It is too difficult to make appointments,” and “When I experience pain and/or other physical symptoms, I have difficulties identifying them and reporting them to my health care provider.” The a priori postulated association with the number of co-occurring mental disorders was not supported.
Subscale 3 consisted of BHC-SF items related to structural difficulties: “I don’t understand the healthcare system,” “I have problems filling out paperwork,” “Concerns about cost or insurance coverage keep me from getting primary care,” and “I have inadequate social, family, or caregiver support.” Higher scores on this subscale were associated with higher agreement with the statement “Based on my personal experience, I need more support to organize myself in order to benefit from my treatment.” The a priori postulated association with higher agreement with statements about barriers to health care based on access/financing (T5) and level of social support (days during the last 6 months) was not supported.
Subscale 4 included BHC-SF items related to sensory specificities: “Sensory discomforts (e.g., the lights, smells, or sounds) get in the way of my health care” and “I find it hard to handle the waiting room.” Higher scores on this subscale were associated with higher agreement with the statement “Based on my personal experience, the specifics of my stimulus processing should be taken into account more in the treatment.” Previous research has reported on the impact of sensory specificities in autistic individuals and how they affect access to health care. 66 Strömberg and colleagues (2021) reported that autistic persons found background sound levels in treatment settings more often unacceptable compared with non-autistic persons. The authors point out that adjustments to the auditory domain are especially relevant for autistic persons. They also reported that autistic persons may have difficulties asking providers for adjustments to their sensory needs (e.g., to turn down the lights). This aspect might also explain the association between the statement “Based on my personal experience, the specifics of my stimulus processing should be taken into account more in the treatment” and subscale 1.
The conducted construct validity analyses for the BHC-SF subscales are meant to be the first explorations in this regard. Future research is needed to investigate the subscales in further detail and try to improve their psychometric properties. Since the response to the items was only binary, a next step might be to investigate a continuous response format (i.e., a 5-point Likert scale) that allows for a more specific differentiation between autistic persons. We expect that this could help to improve the psychometric results for the identified subscales. In conclusion, our findings suggest that the BHC subscales may be indicative of varying types of barriers. However, further refinements are necessary to enhance the subscales’ psychometric parameters, which would allow a meaningful evaluation of the BHC-SF at the scale level.
Our study has several limitations: The sample recruited did not reflect the full spectrum of autistic persons. As the overarching research project BarrierfreeASD had autistic persons without ID as the target group, only individuals who met the predefined inclusion criteria could participate. Most of our sample had achieved a high level of education, and many reported stable socioeconomic situations (i.e., employment status, household income). We collected no data on racial and ethnic diversity. Thus, the reported findings may not be fully generalizable to the global population of persons on the autism spectrum. We could not provide longitudinal data for psychometric analyses or potential changes in barriers over time, as data collection was cross-sectional. Future research needs to examine the sensitivity of the BHC-SF to time and intervention. Besides these limitations, our findings support the assessment of the German version of the BHC-SF. The BHC-SF is a useful tool for providing detailed information about experienced barriers that can help health care providers adapt access for autistic persons. The BHC-SF has several advantages for practical use: It is a short (17-item) instrument with a simple scoring procedure. The BHC-SF allows for different levels of interpretation (total score or single item level) and is sensitive to changes over time. 38 As a next important step, the BHC-SF should be evaluated in routine applications. It is important to explore the potential for individualized intervention applications based on an autistic person’s BHC-SF scores. Evaluation of such use is necessary to assess the potential for improving access to and quality of healthcare through the use of this tool.
Conclusion
We found the German version of the BHC-SF to have good internal consistency reliability in a sample of German autistic adults without co-occurring ID. It also has good construct validity, as demonstrated by expected associations with previous experience of treatment termination and with statements about experienced barriers in health care settings in Germany. We found evidence that the BHC-SF may not consist of only one factor representing barriers. We identified four potential BHC-SF subscales that need further psychometric testing.
Footnotes
Acknowledgments
The authors would like to acknowledge the support of our cooperation partners within the BarrierfreeASD project and all persons who participated in our studies and supported our research. They would also like to thank their student research assistant, Tabea Horstmann, who supported the programming of the survey in Lime Survey and the translation of the BHC-SF.
Authorship Contribution Statement
J.P.: Conceptualization, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, visualization, writing—original draft (lead), and writing—review and editing (lead). N.D.: Conceptualization, funding acquisition, investigation, methodology, project administration, writing—original draft (equal), and writing—review and editing (equal). S.D.: Investigation, methodology, project administration, resources, writing—original draft (equal), and writing—review and editing (equal). P.G.: Investigation, methodology, resources, writing—original draft (equal), and writing—review and editing (equal). D.S. and K.V.: Funding acquisition, resources, writing—original draft (equal), and writing—review and editing (equal). P.R.: Investigation, resources, writing—original draft (equal), and writing—review and editing (equal). A.K.: Funding acquisition, methodology, writing—original draft (equal), and writing—review and editing (equal). H.K.: Investigation, writing—original draft (equal), and writing—review and editing (equal). C.N.: Resources, validation, and writing—review and editing (equal). DM.R.: Resources, validation, and writing—review and editing (equal). H.S.: Conceptualization, funding acquisition, methodology, supervision, validation, writing—original draft (supporting), and writing—review and editing (lead).
Author Disclosure Statement
All authors declare that they have no conflicts of interest.
Funding Information
This study was conducted as part of a larger research project (BarrierfreeASD) funded by the Innovation Fund of the German Federal Joint Committee (Gemeinsamer Bundesausschuss; grant number: 01VSF19011).
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.