
Abstract
Objective:
To study the safety and reproducibility of high-voltage integrated nanosecond pulse irreversible electroporation (INSPIRE) administered through a single applicator and grounding pad approach in a healthy liver model.
Methods:
A percutaneous approach to the liver was made under ultrasound guidance in female pigs weighing between 25 and 35 kg. INSPIRE treatments at 3000 V, 4500 V, and 6000 V using 1000 ns or 2000 ns waveforms, with a 0.02 s dose and a 45°C temperature set point were delivered using an actively cooled single applicator and distal grounding pad. Ablation size, muscle stimulation, and cardiac safety were evaluated.
Results:
All INSPIRE treatments were completed successfully without cardiac synchronization or break-through muscle stimulation. Ablations were visible on ultrasound shortly after treatments were complete. Treatments were completed within approximately 2–8 minutes. The largest ablations, achieved with the 2000 ns waveform at 6000 V, measured 4.4 ± 0.7 cm by 2.9 ± 0.1 cm.
Conclusion:
INSPIRE can be safely used to achieve significantly larger ablations significantly faster than current irreversible electroporation (IRE) technologies using a simplified single-applicator and grounding pad approach.
Significance:
INSPIRE overcomes technical and procedural challenges facing IRE including ablation size limitations, muscle stimulation, the need for cardiac synchronization, long procedure times, and the lack of visualization during procedures.
Keywords
Introduction
Focal cancer therapies are becoming an increasingly popular treatment for surgically unresectable tumors 1 due to their minimally invasive nature. Irreversible electroporation (IRE) is a uniquely suited focal ablation methodology for treating highly vascular organs2,3 where heatsinking effects can diminish the efficacy of thermally mediated ablation modalities such as radiofrequency, microwave, and cryoablation. Using high-voltage electrical pulses, IRE induces cell death via nanoscale defects in the cell membrane.2,3 The localization of these defects to the cell membrane preserves the surrounding extracellular matrix, 4 potentially sparing nerves and blood vessels.5,6 This makes IRE ideal for treating tumors located near critical structures where complete destruction of tissue microarchitecture would result in adverse effects.4,7–13
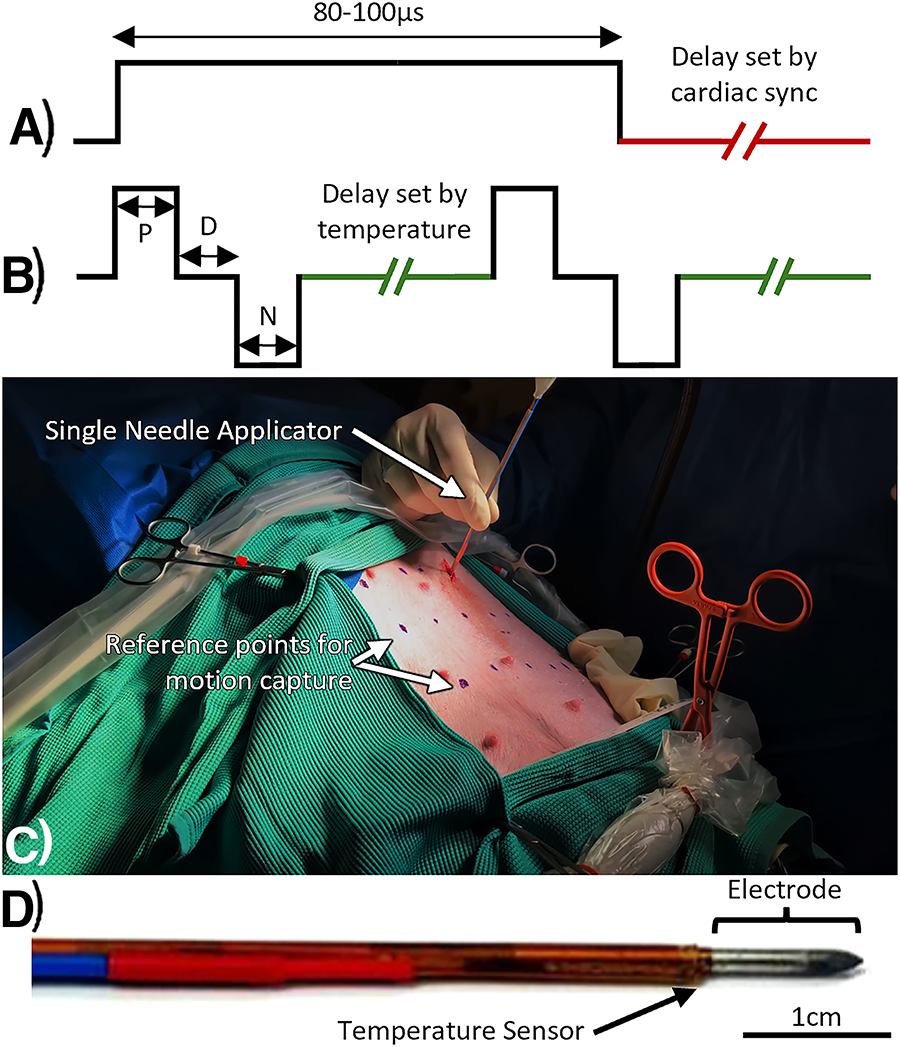
The NanoKnife, the first FDA-approved clinical IRE device (NK-IRE), delivers 80–100 µs (80,000–100,000 ns) monopolar pulses (Fig. 1A) with amplitudes up to 3000 V between pairs of applicators inserted into a tumor.14,15 Cell death occurs in areas exposed to electric field strengths above 500 V/cm.16,17 The electric field strength decreases exponentially with distance from the electrodes resulting in submillimeter transition zones between live and dead tissue. 16 Due to this precision, and its unique ability to preserve critical structures, NK-IRE has been used to treat solid tumors found in various organs including the liver,12,13,18,19 prostate,19–22 kidney, 19 pancreas,10,11,19,23,24 and lung.4,8,9 However, there are several clinical challenges that have yet to be overcome.
The relatively long monopolar pulses used in NK-IRE induce intense muscle stimulation,25–27 requiring intraoperative paralytics. 28 However, break-through contractions can still occur at the high-voltage settings. 29 The risk of cardiac stimulation also requires NK-IRE pulses to be delivered during the absolute refractory period of the heart to avoid potentially life-threatening cardiac complications.14,15,30 Because of this stimulation, a simplified single applicator and grounding pad approach is contraindicated. Instead, energy is delivered via pairs of electrodes which must be precisely placed in parallel.7,31
Electronics limitations with the NK-IRE system (3000 V, 50 A maximum) restrict ablation zone sizes produced in a single treatment. 32 Applicators cannot be separated more than approximately 1.5–2.0 cm without deteriorating the electric field needed to induce cell death, requiring more applicators for larger tumors. 32 Clinicians therefore use a “treat-and-retract” approach wherein two to six electrodes are placed around the tumor.23,32,33 Treatments are then delivered between all electrode pairs to treat a small segment of the tumor.32,33 The probes are then incrementally retracted and treatment repeated to ensure complete tumor coverage.23,32,33 Treatment of a 3 cm tumor with NK-IRE typically requires the placement of four applicators at the tumor margins and have a mean IRE pulse delivery time of 35 minutes. 23
High-frequency IRE (H-FIRE) reduces muscle stimulation25,34 by delivering rapid bursts of ultrashort (250–2000 ns), bipolar pulses,35–39 enabling a single applicator and grounding pad approach.35,40–42 However, clinical H-FIRE systems (e.g., Aliya Pulsed Electric Field (PEF) System, Galvanize Therapeutics) are still limited to 3000 V and require cardiac synchronization, 43 resulting in relatively small treatment zones43,44 requiring over 2 hours of pulse delivery to treat a 3 cm tumor. 43 Additionally, poor intraprocedural ablation visibility makes it difficult to ensure treatments will overlap sufficiently, leading to incomplete tumor coverage. This limits its use to cases in which all other options are contraindicated. 43
Integrated nanosecond pulse irreversible electroporation (INSPIRE) is a next-generation approach which aims to reduce treatment complexity, decrease treatment times, and increase treatment volumes while maintaining a high safety profile. INSPIRE continuously delivers an ultrashort bipolar waveform45–50 throughout the cardiac cycle via a single applicator and grounding pad approach.35,40,42,50 Significant reductions in muscle stimulation with this waveform enable the use of greater voltages and production of larger treatment zones than possible with a single NK-IRE treatment49,51,52 and H-FIRE35,53 treatments. As higher voltages introduce additional Joule heating, INSPIRE implements active temperature control to dynamically adjust the rate at which pulses are delivered (Fig. 1B) to achieve and maintain a target tissue temperature, preventing thermal damage.48,49 This is supplemented with active applicator cooling to enable faster rates of energy delivery. 52 This study sought to evaluate and characterize in vivo outcomes of INSPIRE at voltages beyond the capabilities of current clinical NK-IRE and H-FIRE systems.
Methods
Large-animal liver ablations
All studies were conducted under an approved IACUC protocol (23–181) at the NCSU College of Veterinary Medicine. Healthy YorkX swine (Palladium BioLabs, North Carolina, USA) were fasted for 12 h, premedicated with a Fentanyl patch (50–100 mcg/h) and sedated under general anesthesia using 0.022–0.044 mL/kg TKX (50 mg/mL each of tiletamine, zolazepam, ketamine xylazine) solution. Animals were maintained with 1%–3% isoflurane inhalation in an operating suite. Neuromuscular stimulation was managed with a 1–1.5 mg/kg IV induction dose of Rocuronium and a continuous rate infusion of 0.1–0.6 mg/kg. Follow-up boluses of 0.75 mg/kg were administered between treatments as necessary to maintain a 0 of 4 twitch score on a neuromuscular transmission monitor (Stimpod NMS450X, Xavant Technology, Pretoria, South Africa). Vital signs including heart rate, respiration, and rectal temperature were monitored every 5 minutes. Blood samples were drawn prior to treatment initiation, following treatment, but prior to recovering the animal and prior to euthanasia. Complete blood counts (CBCs) and troponin levels, a measure of cardiac safety, were completed for all blood samples.
All treatments were administered via a percutaneous approach (Fig. 1C) using a single applicator and grounding pad. The applicator comprised a 20 cm long stainless steel 18-gauge needle sheathed in polyimide to leave a 1.0 cm long exposure at the tip. The proximal end of the applicator housed the cooling lines and electrical connections. A fiber-optic temperature sensor (TS5, Micronor Inc., Camarillo, CA) was then secured to the electrode at the end of the polyimide sheath using heat shrink (1.0 cm from the distal tip, as seen in Fig. 1D). The grounding pad was placed approximately 2 cm superior of the tail on the dorsal side of the animal. The area was shaved before placing the pad. A layer of clear ultrasound transmission gel (Aquasonic, Michigan, USA) was used to ensure complete grounding pad contact on the skin. Each animal received three treatments in separate regions of healthy liver parenchyma during the same anesthetic event.
A custom 6000 V, 200 A pulse generation system with a 200 W average power limit was used to administer all treatments. INSPIRE waveforms consisted of a single positive polarity and single negative polarity pulse separated by 1000 ns. Constitutive pulse widths of either 1000 ns or 2000 ns were evaluated in this study. Pulse amplitudes were set to 3000 V, 4500 V, or 6000 V. All treatments administered equivalent integrated doses of 0.02 s calculated as the sum of all pulse durations administered. Therefore 1000 ns treatments administered 10,000 waveforms consisting of 20,000 total pulses and 2000 ns treatments administered 5000 waveforms consisting of 10,000 total pulses. All treatments were replicated a minimum of three times (N = 3). A temperature control set point of 45°C was used to prevent extreme heating of the tissue. Active cooling was achieved by perfusing the internally cooled applicator with room temperature water at a rate of 10 mL/min using a peristaltic pump.
Following successful treatment, animals were survived for 7 days at which point contrast-enhanced CTs were acquired under general anesthesia and the animals were euthanized to collect the livers for gross analysis. Ablation cross sections were obtained by palpating the liver to identify treatment sites and sectioning along the midline of the site. Cross sections were photographed, and the long and short axes of each ablation cross section were visually identified by a change in gross tissue appearance and measured using calipers. Due to potential for off-center cuts to bias long-axis measurements, only short-axis measurements were analyzed. CTs were imported into Slicer3D (V5.6.0, 54 ) for treatment zones reconstruction. Volumes and circularity (long axis divided by the average of shorter axes) of each treatment zone were then determined.
Cardiac safety & muscle stimulation
Blood samples were acquired pretreatment, immediately post-treatment, and prior to euthanasia. Standard hospital procedures were followed for a CBC and blood chemistry. In addition, troponin levels were quantified as a measure of cardiac safety.55,56
To further demonstrate the advantages of INSPIRE, an investigation into muscle stimulation was conducted. Using the same general procedure described above, animals were treated with the applicator and ground pad approach using either NK-IRE (three 100,000 ns pulses) or INSPIRE (1000 ns waveform administered for 10 s) with or without neuromuscular paralytic. Starting at 125 V, voltage was sequentially increased until muscle stimulation was deemed intense enough to risk applicator movement within the liver tissue parenchyma. Stimulation was quantified using an array of visual markers drawn on the skin. Treatments were recorded on video and marker movement was approximated by tracking the markers’ centroids in MATLAB. These positional data were then used to calculate the local acceleration of the marker.
Computational model
COMSOL Multiphysics 6.0 was used to simulate the temperature dependent electric field within the liver. Geometric domains representing the liquid-cooled applicator, distal grounding pad, and liver parenchyma were used to create a 2D axisymmetric model. Details of the model are included in Supplementary Data. Using this model, integrated volumes of tissue exposed to various field strengths were calculated and compared to experimental ablation volumes seen on CT to approximate the lethal electric field strength for each treatment.
Temperature and field intensity data along a cutline perpendicular to the electrode, originating from the center of the exposed portion (the center of each ablation), were exported into MATLAB for analysis. These data were evaluated at a simulation time corresponding to the average treatment duration for each experimental group (120 s, 193 s, and 265 s for the 3000 V, 4500 V, and 6000 V groups, respectively).
Statistical analysis
A two-tailed Student’s t-test with equal variances was used to determine if differences between treatment outcomes (short-axis length, CT volume, lethal field strength) were significantly different (a = 0.05, p < 0.05).
Results
Large-animal liver ablations
All treatments were completed without intraoperative adverse events caused by INSPIRE treatments. Intraoperative paralytics adequately addressed muscle stimulation. Treatment zones were visible intraoperatively on ultrasound as a region of mild hypoechogenicity (Fig. 2). This contrast between the treated tissue and healthy parenchyma increased with time and ablation zones were readily identifiable at the time of necropsy.
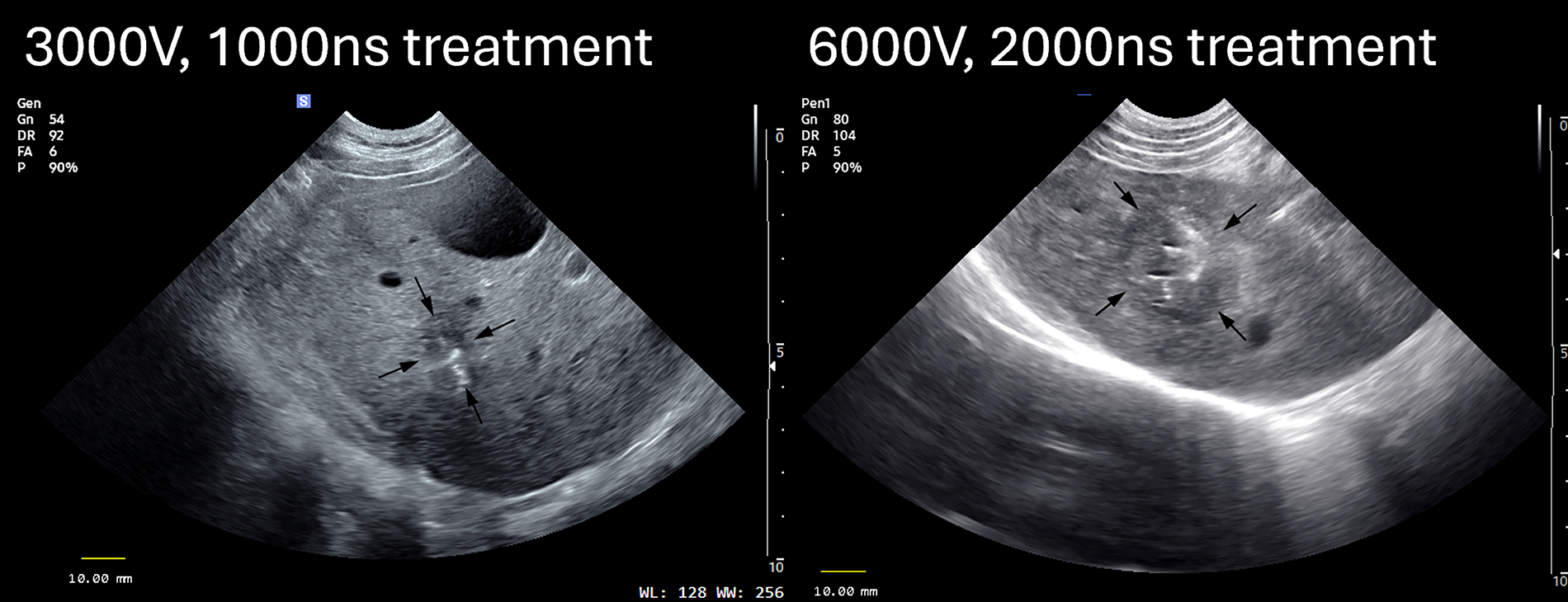
INSPIRE treatments were visible on ultrasound shortly after completion. This enables clinicians to ensure complete tumor coverage during the procedure, rather than afterwards—a procedural challenge faced by current IRE technology. INSPIRE, integrated nanosecond pulse irreversible electroporation; IRE, irreversible electroporation.
Treatments were administered with a temperature set point of 45°C with active cooling. The temperature control algorithm resulted in minor temperature overshoot at the beginning of the treatment before settling to the target temperature. For the 1000 ns treatments, the 3000 V treatments required 2.00 ± 0.37 minutes to complete while 4500 V and 6000 V treatments required 3.22 ± 0.21 minutes and 4.43 ± 1.35 minutes to complete, respectively. For the 2000 ns treatments, the 3000 V, 4500 V, and 6000 V treatments required 1.96 ± 0.07 minutes, 3.54 ± 1.72 minutes, and 6.10 ± 1.02 minutes to complete, respectively. Variation in delivery times was due to the pulse delivery rate being modulated in real time in response to changing tissue temperatures which may have been affected by the presence or absence of local vasculature.
Treatment sites were easily palpated following liver excision as denser, oblate spheroidal regions. Bisected treatment zones appeared heterogeneous (Fig. 3A–F). Tissue structure was generally intact with a fibrous capsule surrounding a region of pale or slightly yellow-pigmented tissue (Fig. 3A–F).
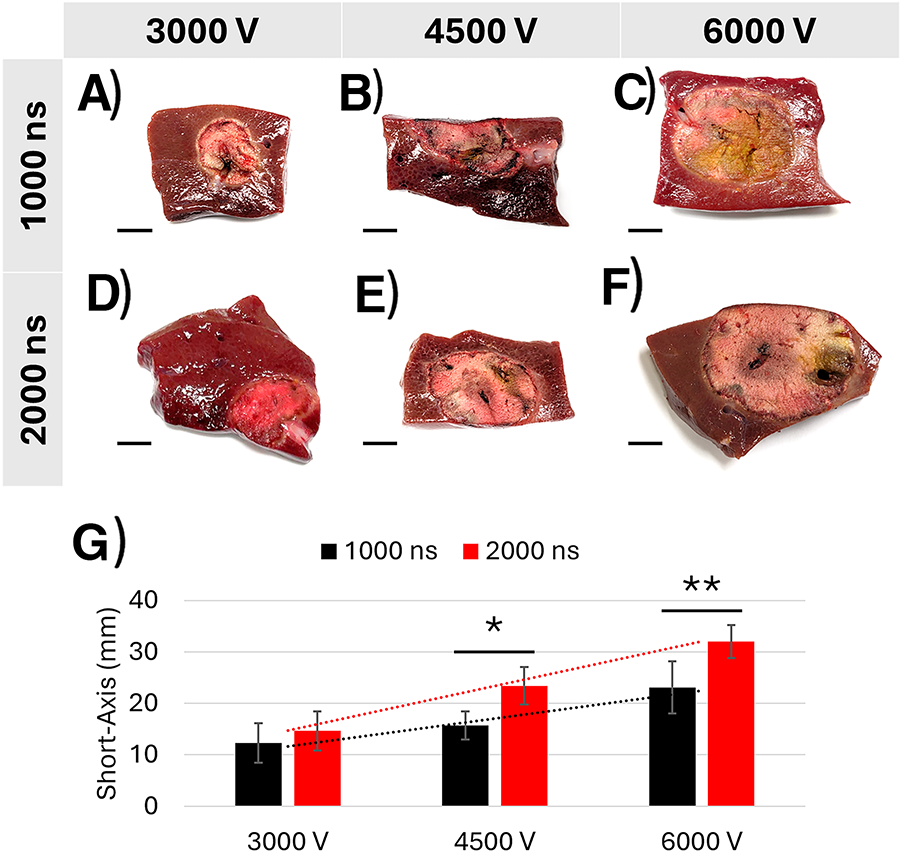
Short-axis length increased proportionally with voltage for all treatments. Treatments utilizing a 2000 ns waveform demonstrated a larger increase than treatments utilizing a 1000 ns waveform (Fig. 3G). Linear fits of short-axis lengths achieved with each waveform were calculated. Furthermore, 1000 ns treatments resulted in the equation y = 5.407x + 6.220 (R2 = 0.95700); 2000 ns treatments resulted in the equation y = 8.676x + 6.003 (R2 = 0.99996). Significant differences in short-axis length between waveforms were found at 4500 V (p < 0.05) and 6000 V (p < 0.01), but not 3000 V (p > 0.05).
For 1000 ns treatments, short-axis lengths were 1.23 ± 0.38 cm for the 3000 V treatments (N = 3), 1.57 ± 0.27 cm for the 4500 V treatments (N = 3), and 2.31 ± 0.50 cm for the 6000 V treatments (N = 9) as measured during necropsy (Fig. 3B).
For 2000 ns treatments, short-axis lengths were 1.47 ± 0.38 cm for the 3000 V treatments (N = 3), 2.34 ± 0.36 cm for the 4500 V treatments (N = 3), and 3.20 ± 0.32 cm3 for the 6000 V treatments (N = 5) as measured during necropsy (Fig. 3B).
Treatment zones were identifiable on CT as regions of hypodense tissue (Fig. 4A–F). Ablation volumes further confirmed the proportional relationship between voltage and ablation size. Treatments utilizing a 2000 ns waveform demonstrated a more substantial increase in ablation volume with increasing voltage than treatments utilizing a 1000 ns waveform (Fig. 4A–F). For both waveforms, a highly linear relationship was found [1000 ns treatments: y = 3.041x − 1.303 (R2 = 0.98771); 2000 ns treatments: y = 10.097x − 9.127 (R2 = 0.96999)]. Significant differences in ablation volume between waveforms were found at 4500 V (p < 0.05) and 6000 V (p < 0.05), but not 3000 V (p > 0.05).
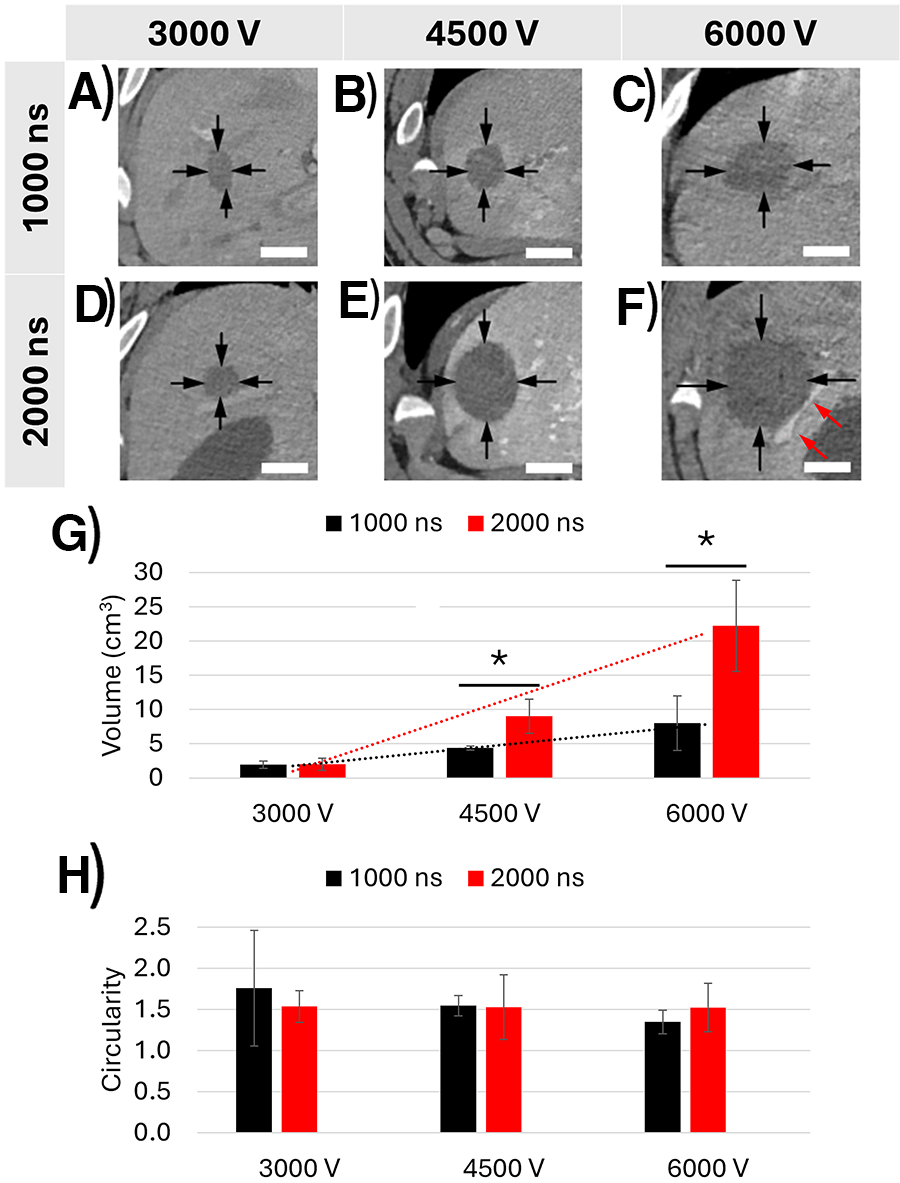
For 1000 ns treatments, ablation volumes were 1.93 ± 0.54 cm3 for 3000 V treatments (N = 3), 4.39 ± 0.31 cm3 for 4500 V treatments (N = 3), and 8.02 ± 3.98 cm3 for 6000 V treatments (N = 8) as measured on CT (Fig. 4G).
For 2000 ns treatments, ablation volumes were 2.00 ± 0.87 cm3 for the 3000 V treatments (N = 3), 9.02 ± 2.50 cm3 for the 4500 V treatments (N = 3), and 22.19 ± 6.66 cm3 for the 6000 V treatments (N = 5) as measured on CT (Fig. 4G).
All groups resulted in oblate spheroidal treatment zones with the 3000 V 1000 ns treatments resulting in the least spherical ablations. However, higher voltages resulted in more spherical ablations (e.g., circularity approached 1.0) (Fig. 4H).
This finding was in general agreement with the numerical model of the electric field, which also transitioned from an oblate shape to a more spheroidal one at higher voltages (Fig. 5A). The model was used to estimate the electric field strength at the edge of each ablation to calculate a lethal electric field threshold (Fig. 5B). For the 1000 ns treatments, thresholds were calculated to be 730 ± 146 V/cm, 650 ± 29 V/cm, and 546 ± 96 V/cm for the 3000 V, 4500 V, and 6000 V groups, respectively. For 2000 ns treatments, thresholds were calculated to be 758 ± 268 V/cm, 426 ± 87 V/cm, and 322 ± 61 V/cm for the 3000 V, 4500 V, and 6000 V groups, respectively.
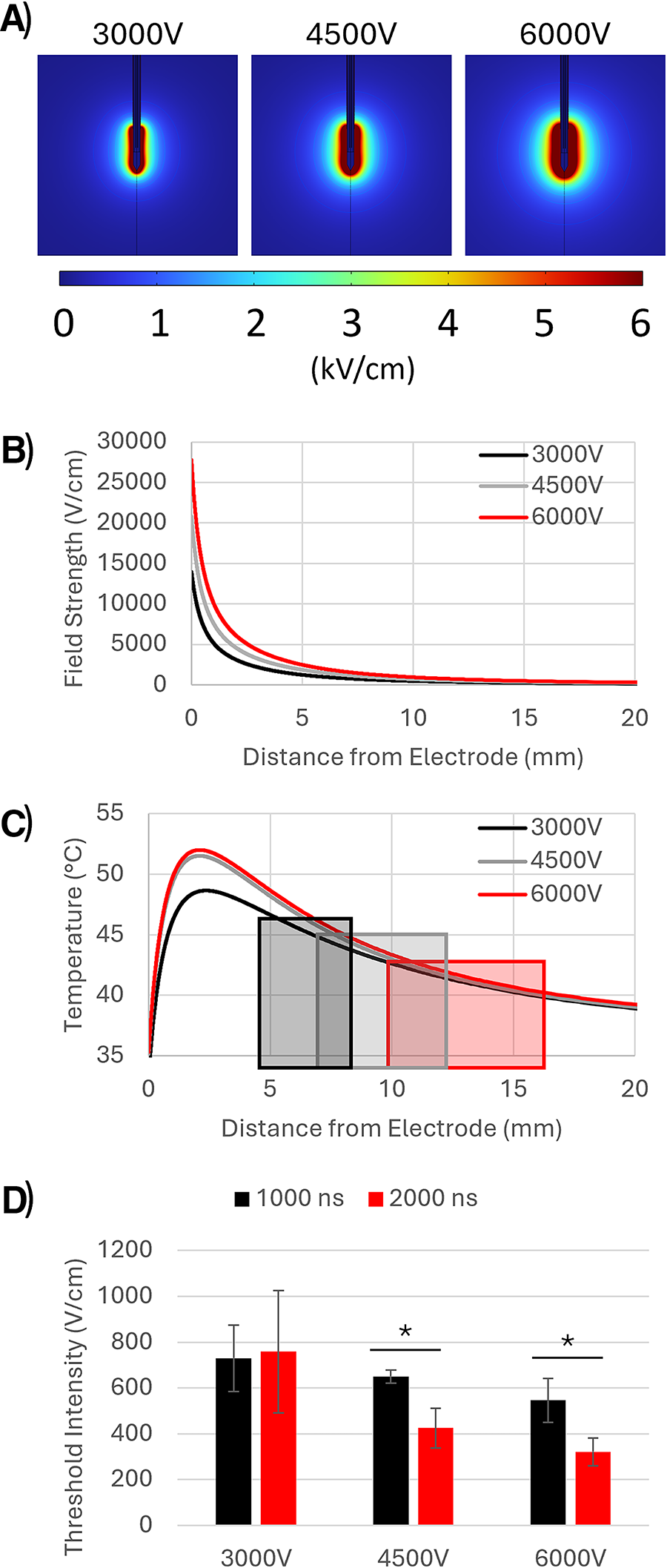
Additional numerical analysis revealed that the temperature profile of the 3000 V treatments differed from the 4500 V and 6000 V groups (Fig. 5). Temperatures along the cutline at the middle of the ablation for the 4500 V and 6000 V groups were almost identical, with temperatures peaking approximately 2 mm away from the electrode. The 3000 V group followed this same general shape, with the hottest point also located approximately 2 mm from the electrode, but the peak temperature was approximately 3°C lower than the 4500 V and 6000 V groups.
Cardiac safety & muscle stimulation
No elevated troponin levels indicative of cardiac damage were found for any INSPIRE treatments. However, elevated troponin levels were observed in the NK-IRE group during the muscle stimulation experiments, which increased from 0.252 ng/mL prior to treatment to 2.98 ng/mL after treatment. After 1 week, the troponin level returned to a value below the detection threshold of 0.2 ng/mL.
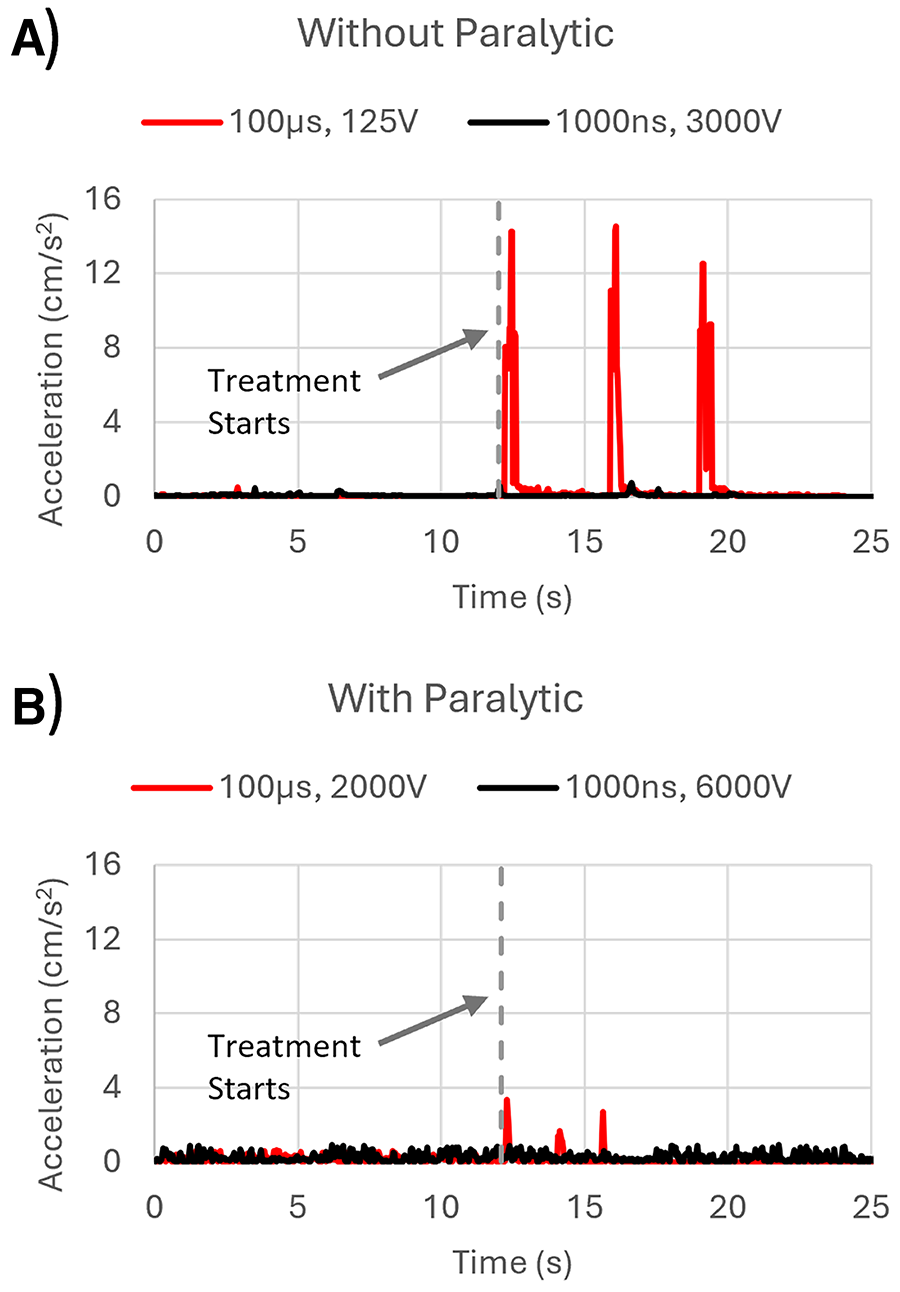
Significant muscle stimulation, which caused intense movement in the abdomen and limbs occurred in the NK-IRE treatment at the starting voltage of 125 V when delivered without a paralytic. With a neuromuscular paralytic, NK-IRE induced minor muscle stimulation starting at 500 V with sufficient stimulation to move the electrode applicator occurring at 2000 V.
INSPIRE treatments without neuromuscular paralytic did not have significant stimulation until delivery at 3000 V, which resulted in a localized tetanus around the applicator for the duration of the treatment. With a neuromuscular paralytic, no muscle stimulation was observed for INSPIRE treatments at the highest testable voltage of 6000 V. Figure 6 records the motion-capture-derived acceleration data for each of these treatments.
Discussion
INSPIRE reduces muscle stimulation and avoids cardiac synchronization
INSPIRE overcomes several current challenges associated with clinical NK-IRE and H-FIRE. The waveforms utilized by INSPIRE greatly reduced muscle stimulation compared with NK-IRE as has been shown previously.25,40,50 This enables the use of a single applicator and grounding pad approach as seen with H-FIRE systems which also use ultrashort bipolar pulses.43,44,57 However, unlike H-FIRE, INSPIRE does not use cardiac synchronization.
Additionally, INSPIRE can achieve significantly larger ablations in significantly less time than NK-IRE and H-FIRE, overcoming two major challenges seen in these current systems. NK-IRE is limited to small treatment volumes due to break-through muscle stimulation and hardware limitations (3000 V, 50 A).25–27,29 This necessitates a treat-and-retract approach which can treat a 3 cm diameter tumor in 35 minutes. 23 Clinical H-FIRE systems such as the Aliya PEF System simplify the approach by enabling the use of a single applicator, but still have hardware limitations (3000 V, 50 A) which result in treatment zones that are ∼1 cm in diameter, thus requiring multiple treatments that can take over 2 hours to treat a 3 cm tumor. 43 By preventing break-through muscle stimulation and by developing a system capable of utilizing higher voltages than currently seen clinically, INSPIRE demonstrates here its ability to treat much larger volumes much more quickly, achieving 3 cm diameter ablations in <8 minutes, without adverse effects such as muscle stimulation which breaks through paralytic or cardiac damage.
INSPIRE shows reproducibility and predictability in treatment volumes
In addition to safety and efficacy, this study also demonstrated the reproducibility and predictability of INSPIRE treatments. Ablation volumes and short-axis measurements were found to increase proportionally with the applied voltage for both waveforms, demonstrating the ability to use voltage as a means of predicting INSPIRE treatment volumes. INSPIRE treatment predictability was further enhanced in the 2000 ns treatments which consistently resulted in ablations with a length to width ratio of approximately 1.5 compared with 1000 ns treatments which varied from approximately 1.4 to 1.8 depending on the applied voltage (Fig. 4B). This overall ability to achieve a consistent ablation shape paired with the ability to predict the size of the ablation make INSPIRE treatments ideal for clinical applications.
Joule heating is a challenge, mitigated by temperature control
With the increase in voltage used for INSPIRE treatments in this study, Joule heating becomes a significant, but addressable, challenge. IRE currently fulfills a niche of treating tumors near critical structures that would be destroyed with thermal ablation modalities. 4 The pulse generation system used here was sufficiently powered to rapidly reached the set point of 45°C, which, if left unaccounted for, would have allowed the temperature to continue to increase, leading to profound thermal damage. However, the use of temperature control and an actively cooled applicator adequately addressed heating concerns as seen by the proximity of blood vessels to treatment sites, which were still perfused following treatment (Fig. 4F), indicating that ablations were predominately due to nonthermal effects.
Tissue heating aids in achieving ablations, despite not being the main cause
However, while not the cause of cell death, heating of the tissue likely did still play a role in achieving the ablations seen here. Increased voltages and the use of longer waveforms, which deliver more energy per pulse, contributed to faster heating of the tissue. This is evident in the longer treatment times associated with higher voltages and the longer treatment times for the 2000 ns treatments compared with the 1000 ns treatments. It has been shown that increases in temperature significantly decrease lethal thresholds for ultrashort bipolar pulses, achieving thresholds similar to those of NK-IRE (500 V/cm) when delivered at 37°C in vitro.45,46 In this study, INSPIRE treatments routinely reached 45°C at the temperature sensor and upon modeling in COMSOL, it is likely that portions of the tissue reached temperatures higher than this (Fig. 5C). The increase in temperature may explain why lethal thresholds differed significantly between waveforms at higher voltages and why 2000 ns thresholds at 4500 V and 6000 V were lower than those seen in NK-IRE. While INSPIRE treatments have been shown to result in lower thresholds than NK-IRE previously, 50 further investigation into the relationship between temperature and lethal thresholds for INSPIRE treatments will be needed to fully validate these results.
Limitations
There are several important limitations of this study. There was some variability in treatment volumes within groups. This is likely due to size of the livers relative to the treatment zone size, sub-optimal placement of the applicators, and movement of the applicator during longer treatments. Some treatment zones bisected liver lobes resulting in additional outcome variability. Only a single electrode exposure (1 cm) was investigated in this study. Previous studies have shown no significant differences in ablation sizes for INSPIRE treatments delivered with 1000 ns or 2000 ns waveforms at 6000 V and a 0.02 s dose with a 2 cm electrode exposure. 50 Thus, additional experiments will be necessary to determine how electrode exposure and its interactions with other parameters affects treatment times and sizes. Treatments were administered to healthy liver parenchyma and, while some treatment sites were adjacent to small blood vessels, it will be necessary to further evaluate these treatments when delivered near major blood vessels, bile ducts, the gallbladder, stomach, and intestines to completely assess safety in proximity to these structures. Finally, while INSPIRE has demonstrated anti-tumor efficacy in veterinary animal models of skin cancer,58,59 a percutaneous approach has yet to be tested.
Conclusion
INSPIRE uses temperature-regulated, ultrashort bipolar pulses to overcome challenges associated with other IRE technologies (NanoKnife, Aliya PEF System). Using novel INSPIRE protocols, this study achieved successful liver ablations at voltages up to 6000 V using a single applicator and grounding pad approach. This simplifies the treatment procedure and drastically reduces treatment time, achieving 2–3 cm diameter ablations in <8 minutes following probe placement, a significant improvement over similar commercial technology. Additionally, ablations were able to be visualized soon after treatment (within 10 minutes) on ultrasound, which in a clinical setting, would allow clinicians to easily ensure complete tumor coverage during a procedure, a current limitation of some systems that has hindered widespread adoption.
Authors’ Contributions
R.H.W.: Conceptualization, investigation, methodology, formal analysis, data curation, writing—original draft, visualization. J.A.F.: Conceptualization, methodology, investigation, software, writing—review & editing. J.D.: Methodology, investigation, data curation, project administration. L.R.: Methodology, investigation, software, visualization. N.N.: Methodology, investigation, supervision. A.I.: Methodology, investigation, supervision. D.G.: Supervision. M.B.S.: Conceptualization, methodology, software, investigation, resources, writing—review & editing, supervision, project administration, funding acquisition.
Footnotes
Author Disclosure Statement
M.B.S. has intellectual property related to the subject of this article. M.B.S. and J.A.F. have ownership in Gradient Medical Inc., a company commercializing PEF-related technologies. M.B.S. receives royalties from AngioDynamics Inc. All other authors have no conflicts to declare.
Funding Information
Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under award numbers R01CA276232, R01CA272550, R41CA275587 and by the NCSU Chancellor’s Innovation Fund.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.