
Abstract
Introduction:
Electrochemotherapy (ECT) is a widely accepted treatment modality for skin cancers that are not amenable to first-line therapies. It is extensively used in both human and veterinary medicine. Various electrode designs exist, with needle tips differing by manufacturer and application. In human medicine, electrodes commonly feature conical tips, while veterinary electrodes typically have sharper, beveled tips to better penetrate the tougher skin of animals. A recurrent issue among ECT practitioners—both physicians and veterinarians—is the progressive loss of needle sharpness during treatment. This degradation increases tissue trauma, potentially delaying recovery, particularly when treating healthy surgical margins. In addition, blunted needles are prone to deflection upon insertion, which alters the inter-needle spacing. This, in turn, can compromise the uniformity of electric field distribution and leave regions of the target tissue insufficiently permeabilized.
Materials and Methods:
Three needle tip geometries—conical, beveled, and triangular—were evaluated. All needles had a diameter of 7 mm. COMSOL Multiphysics® simulations were performed to assess electric field distribution for each tip type. Insertion force and the number of insertions until noticeable loss of sharpness were evaluated using an ex vivo model. In addition, the use of a guiding mask integrated into the electrode design was tested to minimize needle deflection during insertion.
Results:
COMSOL simulations showed that near the needle tip, the electric field intensity in the space between needles remained below the minimum threshold for effective tissue permeabilization, with similar patterns across all tip types. Conical tips required the highest insertion force, followed by beveled and then triangular tips. Sharpness degradation occurred most rapidly in conical needles, with significant dulling after approximately 50 insertions. Beveled tips retained functional sharpness for about 150 insertions, while triangular tips maintained it for up to 200 insertions. Triangular needles demonstrated superior insertion efficiency and durability. The inclusion of a guiding mask substantially reduced needle deflection, improving parallel alignment and maintaining electric field uniformity.
Introduction
Electrochemotherapy (ECT) is an accepted treatment used for cutaneous primary and secondary tumors of varied histologies. It consists of the application of a cytostatic such as bleomycin or cisplatin, followed by the delivery of electric pulses that enhance cell membrane permeability. 1
The procedure consists of the administration of bleomycin (in most of the cases) followed by the application of an electric field in the tumor and margins. The electric field is applied by means of an electrode, typically consisting of rows of parallel needles. The user needs to pinch the whole tumor and margins with the needle electrodes. It is important to note that even slight variations in the parallelism of the needles can produce significant electric field inhomogeneities that ultimately lead to tumor recurrence due to insufficient treatment. 2 Loss of needle parallelism may result from inadequate application technique or insufficient needle sharpness. It can also arise when the tissue is excessively lax or in fibrotic lesions that are too rigid to be effectively penetrated by the electrodes.
The therapy is a standard of care in veterinary medicine for cutaneous, subcutaneous, and oral tumors in dogs, cats, and horses.3,4 It can provide an objective response rate that is around 80% regardless of the tumor type. 5 It has been successfully used in squamous cell carcinoma, 6 oral melanoma, 7 mast-cell tumors, 8 and sarcoids,9,10 among others. 11 The development of new electrodes extended the use of this therapy to tumors in very difficult-to-reach locations, 12 particularly nasal duct tumors. 9
The treatment in veterinary medicine is well extended in Europe, United States, and Latin America.
In human medicine, the treatment is well established as a rescue therapy in patients with cutaneous and subcutaneous tumors that did not respond to first-line therapies. The exception to this is basal-cell carcinomas, where ECT can be the first-treatment option in selected cases. 13 Evidence shows very high response rates regardless of tumor histology, with minimum side effects. 14 Also, the development of new electrodes and protocols allows the use of ECT in deep-seated tumors with very good results.15–17
ECT offers the distinct advantage of targeting rapidly dividing cells. Consequently, fast-replicating tumor cells are predominantly eliminated through apoptosis, while slower-replicating healthy tissues are preserved. This selectivity enables the treatment of extensive areas with excellent esthetic outcomes. 13 In addition, ECT induces a robust local immune response due to the effects of the electric field and bleomycin, which is the drug of choice for this therapy. The increased permeability of cell membranes further exposes intracellular antigens, altering the tumor microenvironment and enhancing susceptibility to other immunostimulatory treatments. 18 Notably, combining ECT with immunotherapies has demonstrated superior outcomes compared with immunotherapy alone, significantly improving one-year overall survival. 19 Furthermore, repeated ECT sessions can enhance local responses even in immunocompromised patients by training the innate immune system. 20
The electrodes used are also similar, but with some differences that are as follows. Veterinary electrodes typically consist of conical or beveled needles. Some manufacturers provide reusable electrodes, while others provide disposable electrodes. Human medicine electrodes are solid 21 G conical tip needles and are always disposable. The veterinary electrodes are sharper than humans, so it is easier to penetrate the skin of the animal. In the same way, users of ECT in human medicine complain about the lack of sharpness in the needles, which makes the treatment rather difficult.
Previous studies on medical engineering have examined how tip design of the needles influences the insertion force and trajectory within different tissue models for different medical applications. In models that closely resemble real tissues, in general it is accepted that beveled and triangular tips require less insertion force than conical tip needles,21–23 and also they provide better comfort for the patient. 24 However, the particular case of ECT electrodes is different from these studies, as multiple needles are inserted simultaneously. Also, it is important to consider that the needles penetrate the tissue at a 90° angle with respect to the surface where the tumor sits; according to the veterinary guidelines, this helps the acting professional to apply the electric field uniformly and cover the whole tumor and margins.3,25
Another problem with the needle use through the treatment is that its sharpness is quickly lost, particularly with needles with conical tips. This provokes trauma to the tissue, slowing recovery, especially when treating healthy margins. The damage of the healthy tissue provoked by the needles was documented in veterinary patients, i.e., cats with squamous cell carcinoma in the nose. The nose of the cat is very sensitive to trauma, inducing several days of anorexia. By means of a thinner electrode and sharper needle with beveled tip, the treatment was less traumatic, the anorexia was significantly reduced, and the recovery times improved. 6 Another problem aroused from the loss of sharpness is its deflection inside the tissue, which introduces variations in the distance of the needles. 2 The voltage-to-distance ratio applied between electrode needles should be 1,000 V/cm. This value ensures that, despite local inhomogeneities, the entire region between the needles receives adequate treatment coverage. If the electric field falls below the reversible electroporation threshold in any area, permeabilization will not occur, increasing the risk of disease relapse.25,26
In this work we will compare different electrode tips and simulate electric field distribution, and compare insertion force. The number of insertions until the sharpness is lost will be measured, and a mask for reducing needle deflection inside the tissue is presented.
Materials and Methods
Three types of needles with different tips were evaluated. Conical, beveled, and triangular shaped tips (see Fig. 1). All of them had a diameter of 0.7 mm. The electric field distribution and force required for insertion was evaluated.
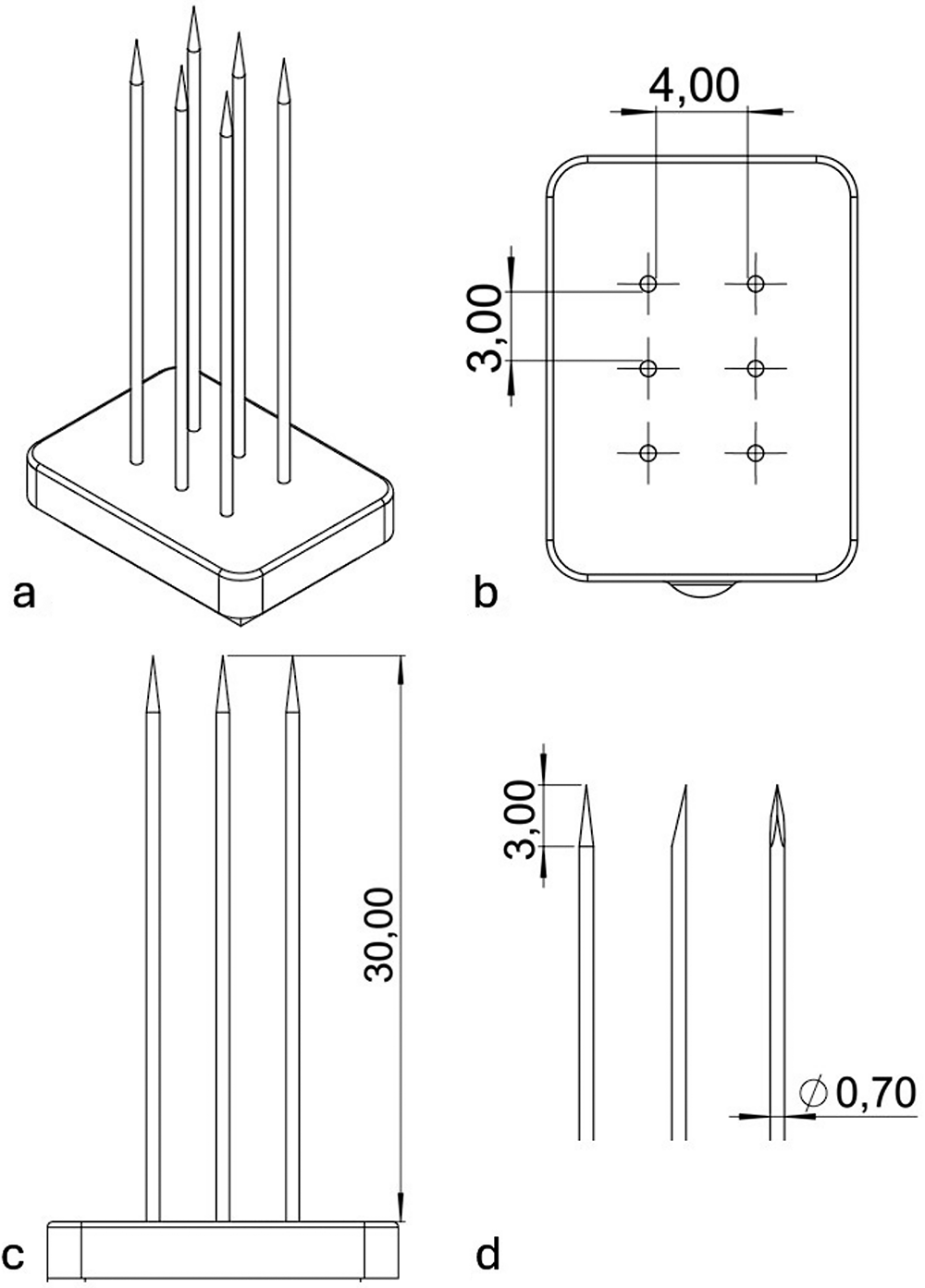
Scheme of the electrode design and needles tested. In
For evaluating the electric field produced in the tip of different types of needles
We compared the electric field distribution between different needle types with COMSOL Multiphysics 4.3 simulations: conical needle, beveled needle, and triangular needle. To study how the type of edge affects the distribution of the electric field, we simulated two needles with each type of edge. The needles were placed inside a simulated tissue with a conductivity of 0.7 [Ω.m] at 25°C. The applied pulse parameters were 400 V. The needles were 4 mm apart. Isosurfaces were calculated with the minimum electric field intensity required for reversible permeabilization of tissues of 480 V/cm. 27 Images of the electric field were captured and processed in ImageJ to calculate the relative size of the permeabilized area with respect to the total size of the image and compare them between the needles.
For evaluating the insertion force and sharpness wear
To evaluate the difference in the insertion force required to pass through the tissue, and to mimic a real use, three different types of electrodes were fabricated. The first one has six conical needles in two rows of three needles, separated 4 mm from each other. The second one was the beveled needle electrode, and finally the triangular needle electrode. Each electrode was inserted in the ex-vivo model tissue (chicken muscular tissue bought from a local retailer) placed in a scale (see Fig. 2). Four different operators performed four insertions up to half of the needle with each type of electrode, and the weights were registered. Average, minimum, and maximum values were registered.
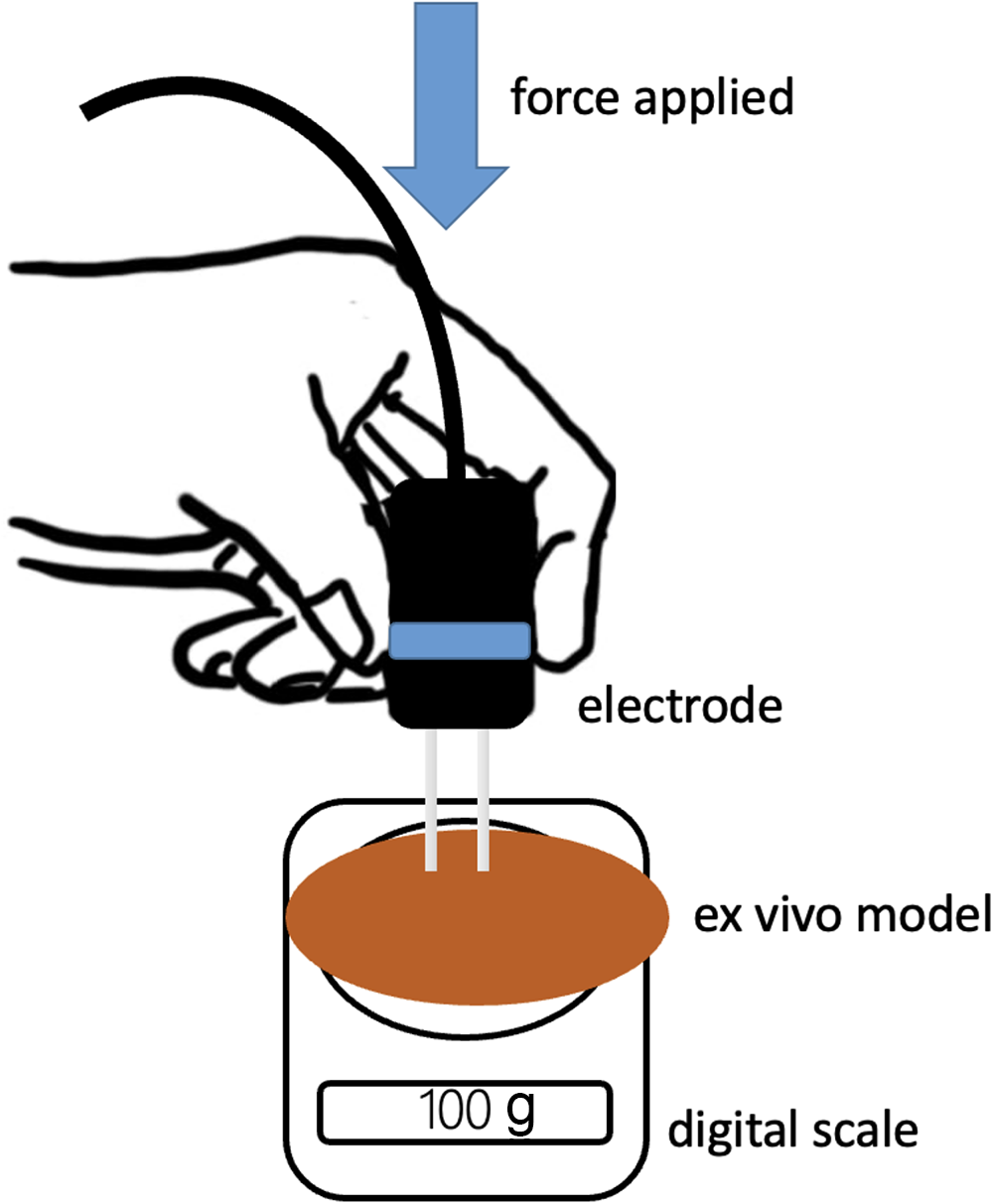
Experimental setup.
After the insertion force using new needles was registered for each type of electrode, the insertions were repeated more than 200 times by three operators in the same manner. After each insertion, more force was expected to be required as the sharpness of the needles deteriorated. The loss of sharpness was considered when 25% more force was needed (with respect to the initial insertions) to insert the electrode in the tissue.
A specially designed mask following the specifications of the electrode depicted in Figure 1b and c was made. To evaluate the effect of including a mask in the electrode to avoid the deviation of the needle during its insertion, the following experiment was conducted. The electrode was inserted through a slice of a simple vegetable (potato), allowing the tips to surpass the slice. The separation of each pair of needles was measured in two different conditions: with the insertion mask placed over the slice of vegetable and without it. Considering 4 mm of gap the optimal separation for this electrode, the deviation from this value was calculated. In total, 72 insertions were performed.
Statistical analysis
For the insertion force, normality tests were calculated with the Shapiro–Wilk test and also T-test; significance was considered with p < 0.05.
For comparing the deviation of the needles inserted with and without a mask, the Mann-Whitney U test was performed.
Results
Electric field distribution: differences between needles
Figure 3 shows the electroporation area above the threshold of 480 V/cm. This area was 2% smaller with beveled tips compared with conical tips and 6% larger with triangular tips. Despite these modest variations, the electric field generated between all tip types remains insufficient to achieve effective tissue permeabilization. Even in the case of triangular tips, where a larger electroporated surface was calculated, a substantial untreated region persists between the tips. This highlights that the distal 3 mm of the tip should not be relied upon for treating deep tumor margins, and electrodes must therefore be inserted beyond this depth.

Simulations of the electric field above 480 V/cm in the different types of needles, including the first 3 mm of the tip. Views from different sides are presented. As can be seen, the electric field produced above the reversible threshold was very similar. All the needle types provided similar electric field distribution with some minor differences. If we consider the surface of the electric field above the reversible electroporation threshold, the conical tip needle provided an electric field 0.6% larger than beveled tip needles, and the triangular tip provided a field 2.37% larger than beveled. This means that the best electric field distribution was provided by the triangular tip needles. The space between the tips, in all cases, shows that an important area between the tips of the needles is not permeabilized during the treatment.
Insertion force: differences between needles
The highest insertion force was obtained with the conical needle, followed by the beveled needle and then the triangular needle (see Fig. 4). A successive loss of sharpness was seen during insertion, making the use of the electrode more difficult. The conical needle showed a loss of sharpness after 25 insertions. The beveled needles were easier to insert in the tissue and showed greater tolerance to sharpness wear, resisting around 150 insertions. The triangular needles required the least force for inserting them in the tissue, and there was an adequate sharpness after 200 insertions (see Fig. 5). Beveled vs triangular: the difference is statistically significant, p = 0.0005, [95% Confidence interval (CI): −77.33 to −23.37]. Conical vs beveled: the difference is statistically significant, p ≤ 0.0001, [95% CI: −224.29 to −288.91]. Triangular vs conical: the difference is statistically significant, p ≤ 0.0001, [95% CI: −331.78 to −282.12].
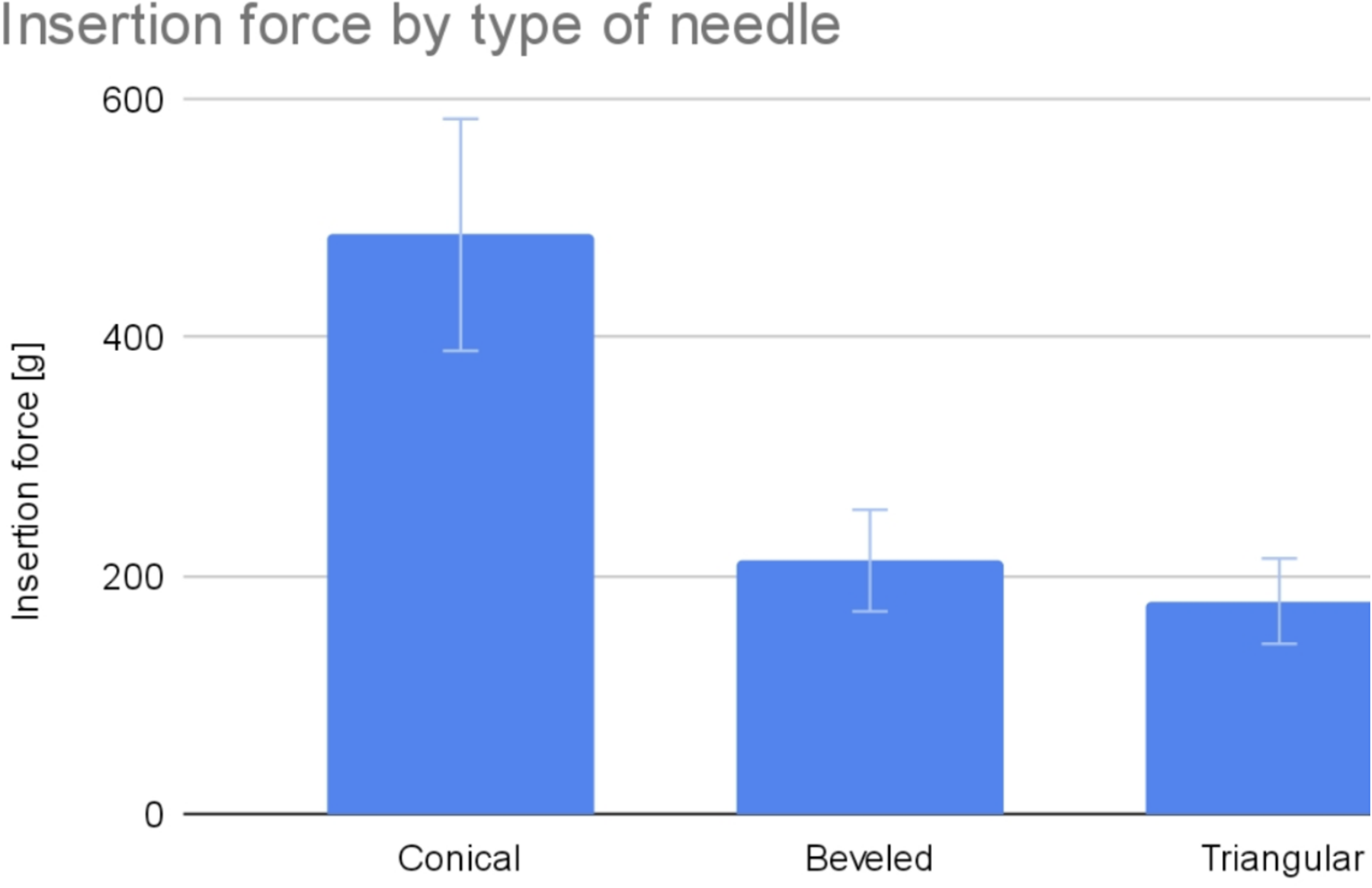
Comparison of the force needed to penetrate the ex vivo tissue model with the different types of needles. The conical required an average force of 485 (370–560) g, the beveled tip 213 (170–259) g, and the triangular tip 178 (130–220) g.

Plots comparing the median insertion force evolution every 10 insertions with each needle: Triangular: Adequate sharpness after 200 insertions (green). Beveled needles required showed a loss of sharpness after 150 insertions (orange). Finally, the conical tip presented the fastest loss of sharpness, significantly increasing the insertion force after 25 insertions (blue). The differences are statistically significant.
We observed that the triangular needle has certain advantages over the bevel and conical needles. The triangular needle requires less insertion force, which probably produces fewer local adverse effects due to less insertion trauma, and it remained sharp even after 200 insertions.
With respect to the use of the insertion mask, we considered the ideal deviation of 0 mm; negative values implied that the needles were closer than 4 mm, and positive values that the needles were more separated than 4 mm. Results show that without mask, the median deviation of the needles was −1.4 mm, ranging from −2.9 to 1 mm. When the insertion mask was used, the median deviation was 0 mm, ranging from −0.8 to 0.7 mm. The addition of a mask to guide the insertion of the needles provided a more uniform insertion and thus maintained the parallelism in the deeper parts of the tissue. The differences are statistically significant with a p < 0.00001 (see Fig. 6). The deviation of the needles was clearly seen at plain sight in the vegetable model (potato) when comparing the insertion with and without the mask (see Fig. 7).

Boxplot comparing the deviation of the needles inserted through a slice of vegetable tissue. As can be seen, masked insertions maintained the separation between the needles, deviating less than 1 mm from the optimal separation. On the contrary, unmasked insertions tend to deviate more than 1.5 mm, ranging from −3 to 1 mm.

A six-needle electrode without optimal sharpness was inserted through a potato. At left the divergence of the needles is marked. In the middle, the electrode design with a retractable mask was used, and the insertion in the potato repeated. At right, the position of the needles is greatly improved.
Discussion
This work was inspired by the initial difficulties that we experienced in the first translation from laboratory applications to veterinary use with the design of the electrodes. The veterinary electrodes were originally identical to the electrodes used in human medicine, i.e., conical shaped. The resistant and elastic skin of dogs and cats is very difficult to treat with these types of needles, as after only very few insertions, they completely lose their sharpness. Even when treating human patients, in extended and hard lesions, such as the breast cancer recurrences after radiotherapy, 28 the treatment is very difficult.
The use of triangular needles can overcome this difficulty and be less traumatic for the tissue. A clean insertion of the electrodes makes a treatment easier when compared with exerting too much force to insert them.
When treating very large tumors, the loss of sharpness can become a problem during the treatment and may be needed to use more than one electrode to complete the treatment without traumatizing the skin of the patient, especially in the safety margins. Other tumors that usually require very extensive areas of treatment, not only because of the invasion of the tumors, but also because they require extensive safety margins, such as the angiosarcomas.29,30
Tumors sitting in regions of the body where the skin is too lax are also difficult to treat if the electrodes are not very sharp. An example can be perianal tumors, where the force exerted to insert the electrode provokes the collapse of the skin, closing the needles between them and increasing the risk of a short circuit inside the tissue. This situation is not dangerous for the patient; however, when a short circuit is produced, the electric field becomes zero, and that region is not treated.
In the case of veterinary medicine, special cases constitute the feline injection site sarcomas. These tumors develop in the injection site of certain vaccines and present a high recurrence rate. 31 As the relapses occur over scar tissue, the treatment of these lesions is very difficult, and electrodes with adequate sharpness are needed. Otherwise, they are impossible to treat. Also for these cases, triangular needles could provide adequate sharpness for the treatment.
An interesting observation is that the three electrodes provided an insufficient electric field between the tips. This observation was previously reported by various authors,25,32 however, it has a crucial importance for tumors located very close to bony structures. The length of the tips is around 3 mm for most of the commercial needles. It is very important to ensure that the depth safety margins that need to be treated are located between the body of the needles and not between the tips. Otherwise, areas of the tumor located between the tips will be untreated; this situation can occur frequently in tumors that are in close contact with the bone. In those cases, it is probably better to perform a surgical debulking and treat the tumoral bed (in contact with the bone) with plate electrodes (see scheme in Fig. 8). This approach was conducted by Taques et al. for treating a tumor in the skull. They debulked the tumor and performed ECT in the tumoral bed with very good results. They also noticed that plate electrodes are better for this case, as an insufficient electric field can be appreciated in the simulations using needle electrodes. 33 However, it has to be noted that in healthy bones it is rather difficult to insert the tips of the needles in it. For this reason, special needles are drilled inside the bone when treating bone metastasis to obtain the best results. 34
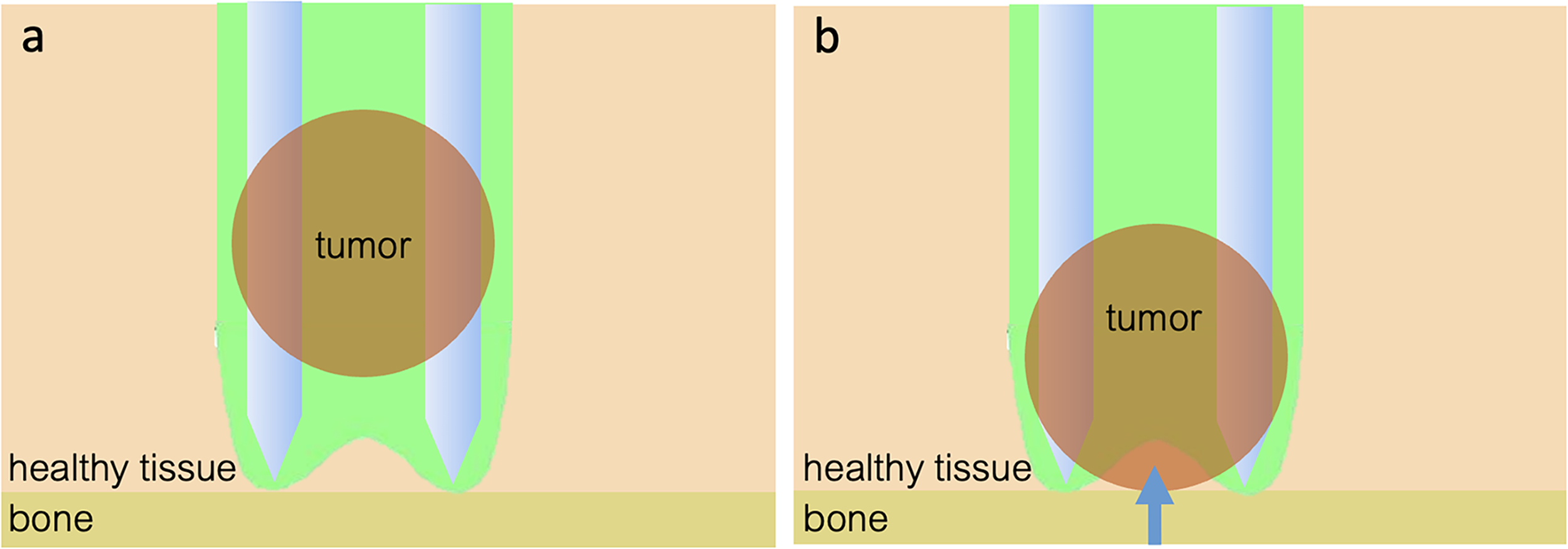
Scheme of the electrode inserted in a tissue for treating a tumor, in green the electric field above the threshold for reversible electroporation. In
Suarez et al. investigated the effects of conductivity increase and Joule heating on electric field distribution during pulse delivery. Although the permeabilized area may expand with the cumulative number of pulses, this phenomenon becomes relevant only at pulse numbers higher than those typically used in ECT. 35
In the study by Mir 36 on the principles and rationale of ECT, it was observed that objective response rates were lower when the electric current passing through the tissue was less than 1.5 A, compared with responses achieved with currents exceeding this threshold. Such low currents typically occurred when only the tip of the electrode needle was inserted into the tissue. This reduced efficacy was likely due to the inhomogeneity of the electric field at the needle tip. In contrast, higher currents—and thus more effective treatments—were associated with deeper needle insertion, which ensured a more uniform and adequate electric field within the tumor. To address this limitation, it was suggested that delivering an additional set of electric pulses orthogonally to the initial ones at the same location could enhance treatment effectiveness. This recommendation aligns with the hypothesis that the electric field at the needle tip is suboptimal and that orthogonal pulse delivery may compensate for this by improving field distribution in previously underexposed regions.
Finally, the sharpness wear induces the excursion of the needles inside the tissue, altering the distance between the needles and thus affecting electric field distribution. This happens not only in very hard tumors but also when treating subcutaneous tumors and the skin on the surface is excessive. The elasticity of the skin makes the needles penetrate with the tips closer, and they can almost touch inside the tissue. This problem can be solved by incorporating a mobile mask to the electrode.
Conclusions
Electrodes for ECT using triangular-shaped needle tips provide the best sharpness for treatment and an adequate electric field. However, an insufficient electric field could diminish treatment efficacy in tumors located in proximity to bony structures.
Authors’ Contributions
F.M.: Conceptualization, methodology, writing draft, investigation, and supervision. A.Campastri and A.Cilio equally contributed to this work: methodology, experiment conduction, data analysis, and investigation. M.R. and N.S.M.: experiment conduction, computer simulations, and data analysis. V.F., A.B., and S.D.M.: data analysis and supervision.