
Abstract
Surgeons face serious challenges removing cancer fully during surgery, with incomplete cancer removal posing significant risks to patients. To address this problem, Lucell Diagnostics Inc. is developing an innovative cancer detection platform called membrane voltage profiling (MVPro; patent pending). This groundbreaking method exploits the discovery that cancer cells exhibit a physiological biomarker, depolarization, as revealed by fluorescent voltage-sensitive dyes. Cancer cells fluoresce in specific patterns and intensities that differ from normal cells, allowing precise identification. We present here our preliminary results on the feasibility of using voltage to locate cancer cells. The aims were: to perform controls showing whether MVPro affects the normal pathology process; to optimize tissue transfer for margin cell collection; to confirm that the VSD DiBAC4(3) is appropriate for MVPro of skin cells; to determine whether MVPro finds cancer in the same specimens as pathological analysis. These studies on nonmelanoma skin cancer specimens reveal that MVPro is low risk to the patient, integrates with existing surgical protocols, finds cancer in the same specimens as does pathology, and presents no complications for pathological analysis. Once development of this methodology is complete, MVPro will yield an annotated, 2D heat map covering the entire surgical margin, indicating the location of cells with a high likelihood of being cancer. This will empower surgeons to confirm a negative surgical margin before closing. This simple type of intraoperative imaging, performed in or near the operating theater, has the potential to improve surgical outcome, cut health care costs, and enhance post-surgical quality of life by preserving healthy tissue. Because the setup costs are relatively small and the reagents are inexpensive, we believe MVPro could be of great benefit to underserved areas. Indeed, MVPro could benefit health care systems globally, from cutting-edge hospitals to small clinics in underserved regions.
Keywords
Introduction
Achieving complete resection of malignant cells is the goal of cancer surgery; however, in the United States. approximately 9% of cancer resections result in a positive surgical margin (PSM), indicating cancer cells left in the patients. 1 This unacceptably high percentage results from the delay of at least 48 h between surgery and margin analysis by a pathologist. A PSM usually necessitates postsurgical interventions, including chemotherapy, radiation, and/or repeat surgeries. These treatments impose emotional burdens on patients and doctors and financial burdens on patients and health care systems, and they adversely affect patient quality of life.
Intraoperative imaging (IOI), which enables real-time analysis of the surgical margin, holds significant promise for improving surgical outcomes by reducing the likelihood of PSMs.2–8 Among existing approaches, Mohs surgery is the only widely used IOI technique. Mohs is the iterative removal of thin layers of tissue, one procedure at a time, followed by cryosectioning of each layer and staining using H&E and analysis by the surgeon. This allows the surgeon to excise only as much tissue as required to remove the cancer, thereby saving healthy tissue. While highly effective, Mohs requires significant financial resources and space, plus approximately 30 min per layer, making it impractical for widespread application. Mohs is used mostly for dermatological surgeries on cosmetically important areas such as the face. Other approaches to IOI involve sophisticated equipment and trained personnel. None of these is likely to be available to underserved regions. 9
An assay that meets the twin criteria of accuracy and sensitivity and is also rapid, inexpensive, small, and simple to employ could address these persistent global challenges. By enabling surgeons to assess surgical margins during procedures, this innovation could reduce the frequency of incomplete removal, thereby reducing the need for repeat surgeries, (of particular interest to medical insurers and hospitals) as well as optimizing preservation of healthy tissue, of particular interest to patients and physicians. These advancements would not only improve clinical outcomes but address certain disparities in treatment availability. Indeed, multiple approaches are being studied (for review see 8 ) but none, so far, achieves a practical combination of speed, utility, ease, affordability, and quality.
Decades-old electrophysiological studies have established that malignant and rapidly proliferating cells exhibit depolarization of Vm compared to differentiated, quiescent cells; that is, the cell membrane potential of cancer cells is more positive than the cell membrane potential of noncancerous cells. 10 Advances in voltage-sensitive dyes (VSDs) now enable simultaneous measurement of cell membrane polarization across thousands of cells for hours to days. This capability could make it possible to distinguish cancer cells from normal cells based on the intensity and pattern of the signal emitted by a VSD. MVPro employs these modern VSDs.
To address the above limitations, we investigated the utility of membrane voltage profiling (MVPro) to examine surgical margins. MVPro is Lucell’s rapid, simple, and cost-effective ex vivo assay for detecting cancer cells in tissue margins. MVPro captures variations in cell membrane potential, also known as cell membrane voltage (Vm), a physiological biomarker present in all living cells. Research has highlighted Vm’s role in regulating key cellular activities, including processes that are profoundly altered in cancerous cells.11–18 These changes are correlated with distinctive Vm patterns that can be exploited for cancer detection.19–22 Previous researchers have proposed leveraging VSDs for cancer detection 23 ; we present here our investigation of the practical aspects and show, in a nonmelanoma skin cancer sample, that with MVPro, it will maybe be possible to achieve the desired IOI. Specifically, we demonstrate that the VSD DiBAC4(3) (DiBAC) fluoresces with significantly different intensities and patterns in basal and squamous cell skin cancers (Basal Cell Carcinoma [BCC] and Squamous Cell Carcinoma [SCC], respectively) when compared with normal skin. We confirmed this correlation using nuclear counterstaining and by comparison with histological examination. These findings support the feasibility of developing MVPro as a rapid IOI assay for cancer cell detection in surgical margins that can be used in any health care setting with access to fluorescence imaging.
Materials and Methods
Informed consent and deidentified specimen collection
Under contract to Lucell Diagnostics, two approved surgeons, Drs. D. Greenstein (standard resection) and O. Badri (Mohs surgery) of Northeast Dermatology Associates (NEDA, Beverly, MA), collected all informed patient consents according to BRANY Institutional Review Board-approved protocol LDI-2021-01; data are available upon request. To maintain patient confidentiality, specimens were given a Lucell Record Number (LRN) pre-printed on labels for all containers. Only approved staff at NEDA had access to both the LRN and patient name; at no time was identifying information available to Lucell staff. Our sample (n = 27) comprised 4 normal, 10 SCC-, and 13 BCC-containing skin specimens; most BCC and SCC specimens also contained normal regions. An additional two specimens were used to confirm the lack of autofluorescence of skin in the Green Fluorescent Protein (GFP) and UV channels of the microscope, and 4 more specimens were used to test different tissue transfer substrates. Only nitrocellulose membranes (NV), (not Polyvinylidene Fluoride [PVDF], glass, or tissue culture plastic), yielded consistently useful transfers.
Tissue transfers and prints
The timing of all steps was recorded. Within 3 min of excision, tissue transfer 24 from resected specimens was accomplished by lightly pressing the margin onto NC. We define a “print” as the thin layer of transferred cells, while the “transfer” is the print plus the NC membrane. Fiduciary marks showing the boundaries of the print were made by puncturing the NC with a pin. For some specimens, a second print was made in a different area of the same NC to test whether a second print would be superior to the first because the first would “clear away” any dead and dying cells; this was not found to be the case. Following transfer, the specimen was immediately placed in an LRN-labeled vial of formalin for pathological analysis. For these preliminary experiments, the lab could not be near the operating suites; in clinical use, the transfer could immediately be stained and imaged. The transfer was placed in an LRN-labeled vial of Eagle’s minimum essential medium (EMEM) for transfer to the laboratory; EMEM was found to be optimal for maintaining the viability of skin cells for up to 55 min.
Transport to the laboratory
Transfers were transported by car to the laboratory, a trip of under 15 min. To determine how long cells were viable, some transfers were stained and then imaged every few minutes for up to an hour. Following the determination that no change in signal was visible up to 55 min, all staining and imaging was thereafter performed within 40 min of transfer, but usually in fewer than 30 min. In clinical settings, there will be no transport needed, and the assay can be run immediately.
Staining with hoechst 33342 and DiBAC4(3)
On arrival, some of the specimens were immediately submerged in a pre-made 20 μM solution of the DNA stain Hoechst 33342 (hereinafter Hoechst; Tocris) for 5 min to identify the locations of all the cells in the print. The transfer was then rinsed once. All transfers were placed into freshly made dye solution of 2 μM DiBAC4(3) (hereinafter DiBAC; Biotium) in EMEM in a BCW 2 × 2 coin snap, (hereinafter cassette; Amazon). Optical clarity of cassettes was compared with standard coverslip preparations and were found to be equivalent. More dye solution was then added to remove bubbles and fill the cassette, which was then closed. After 5 min, the cassette was moved to the microscope stage.
Fluorescence microscopy
The open access software Micromanager (μManager™) 25 was used to control the upright, epifluorescence microscope, a Nikon E800 with Chroma 89400—ET—DAPI/FITC/TRITC/Cy5 Quad filter set. The specimens were all too large for a single image using the 10X objective, so we define the individual views “sub-images,” while the full image is the assembly of all the sub-images into a complete picture of the entire print. The multidimensional acquisition function of μManager™ was used to set the boundaries of the full image by reference to the fiduciary pinholes in the NC membrane. The software computed the number and location of sub-images required to image the entire specimen, i.e., create the full image. Then, one complete scan in the GFP channel (appropriate for DiBAC4(3)) was run to quench signal coming from the NC membrane and to confirm that the entire specimen was captured in the sub-images making up the total image. The full imaging scan was collected using first the GFP filter set then the UV filter set, then named with the LRN of the specimen. At the end of imaging, for each specimen, a dark field image and a flat field image were collected for each filter set. Microscopy took approximately 5 min per transfer.
Cell lines
Human cells were purchased from American Type Culture Collection (ATCC) to ensure proper identification. RWPE-1 (https://www.atcc.org/products/crl-11609) a normal prostate epithelial cell, and Pheochromocytoma (PC)-3 ((https://www.atcc.org/products/crl-1435) grade IV prostatic adenocarcinoma from a bone metastasis, were used for the first test of the algorithm. RWPE was grown to confluence. PC-3 cells were then detached, labeled with Mitotracker greenTM (Thermo-Fisher Scientific), and added to the monolayer of cells. A VSD (Akita Innovations) was then added to the mixed culture, and the PC-3 mitochondrial label and VSD were imaged in situ.
Image processing
The open-source software FIJI™26,27 was used to process all images. First, darkfield and flatfield corrections were made to each sub-image. The stitching function27 was then used to combine the sub-images into the final, full image. No other manipulation of the images occurred. To create the frequency diagram, pixel values were normalized to the median value of the 25 darkest pixels, defined as the background.
Pathological analysis of specimens
Analysis was performed under contract to Dr. Julie Reimann of Massachusetts General Hospital Dermatopathology Associates. She is board certified in dermatopathology and anatomical pathology.
Data analysis
Frequency analysis and determination of statistically and biologically significant correlations were performed using Excel. All error bars are standard deviation. To correct for any variation in illumination and dye signal strength, frequencies of pixels at each signal intensity (0–255) were normalized to the frequency of pixels in “dark areas” defined as the median frequency of pixels measured at intensity = 1 to intensity = 25.
Results
Mvpro of nonmelanoma skin cancers
The main steps of the MVPro process are shown in Figure 1 along with the timeline of tissue processing for pathological analysis. The steps as they would be performed in a clinical setting are as follows:
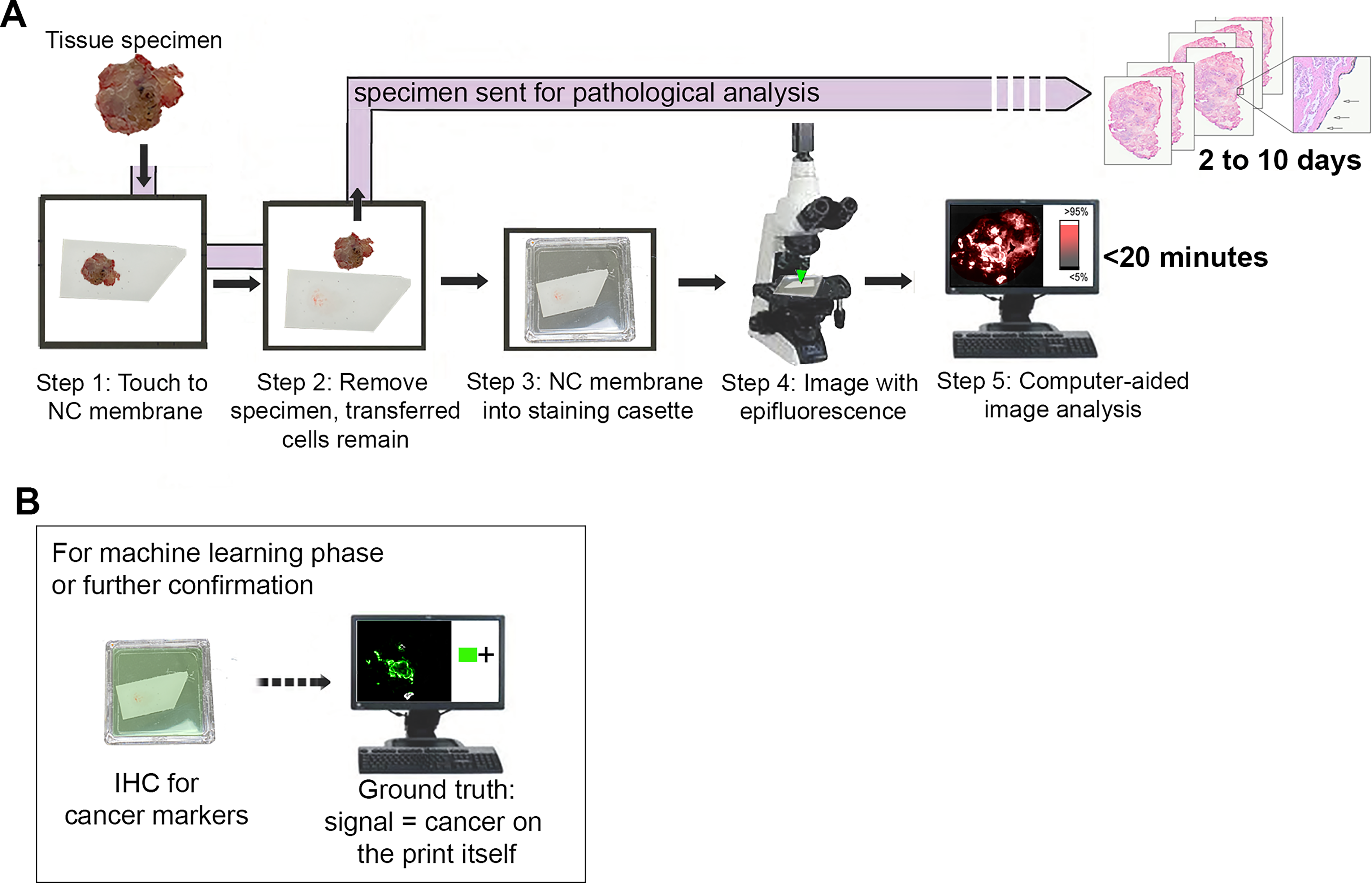
Illustration comparing MVPro with the standard protocol for pathological analysis.
Collect the “print”: a thin layer of cells from the entire surgical margin is collected via tissue transfer wherein the cut surface of the tissue (the surgical margin) is pressed, for about 10 s, to a NC, making the transfer.
Immerse the print in a fast-acting VSD: the transfer is then placed cell-side down into a drop of solution on one side of the cadette. The cassette is then filled completely, snapped shut, and carried to the fluorescence imaging device.
Image the dye signal using epifluorescence illumination: following imaging, the separate images are corrected for dark noise and uneven illumination. The individual images are then stitched together to create a single picture of the entire margin.
Apply custom machine learning algorithms to analyze and annotate the images: while not yet realized, when finished, the algorithm will indicate by a heat map those areas of the whole image that are likely to be cancerous, and it will provide a measure of statistical certainty.
The total time needed for these four steps is under 20 min.
Mvpro does not affect pathological status
By comparing five instances of single cut planes where one side had been tissue printed while the other had not, we found no evidence that MVPro compromises tissue integrity or interferes with subsequent histological analysis (data not shown). These results confirm that MVPro can safely be performed on resected tissue before fixation without negatively affecting pathological examination.
DiBAC finds areas of similar size and shape to those found by histology (compare Fig. 2A and B). Figures 2C–E are closeups of the boxed area in B, showing an area of tissue with unusually shaped nuclei characteristic of polyploid nuclei found in tumors. When present, we used these abnormal nuclei to help identify tumor tissue. There was a strong relationship between the number of bright pixels in SCC MVPro and the area of cancer in sections from the same specimen (r2 = 0.79; Fig. 2F). There was no strong relationship between BCC MVPro bright pixels and the area of cancer sections from the same specimen. This is not surprising, as the two images are not of the same plane. The goal for our next series of experiments is to use antibodies to known cancer antigens to mark the positions of cancer on the prints themselves, thereby removing any doubt about the colocation of cancer and bright pixels.
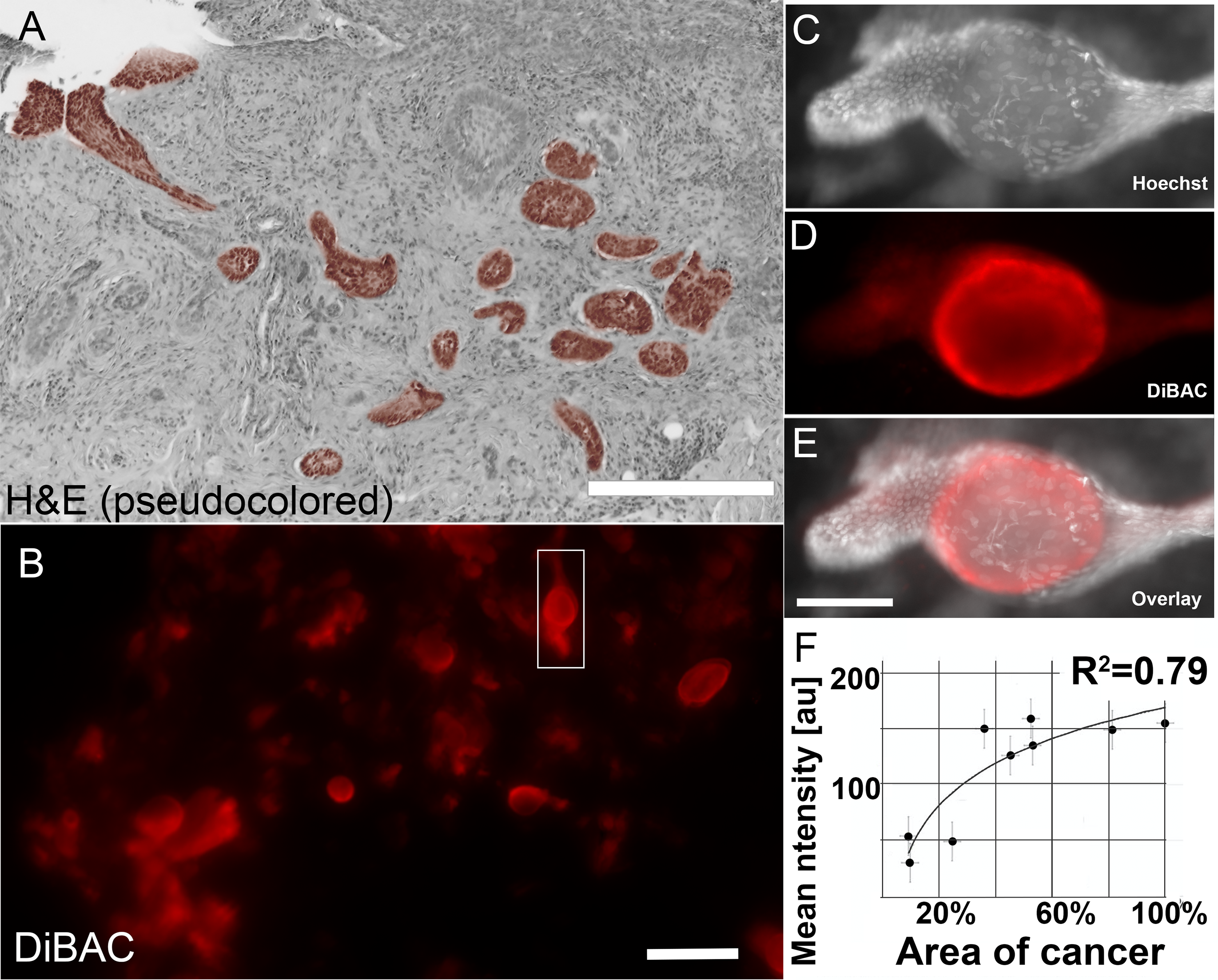
Comparison of standard pathological analysis to MVPro. Because tissue transfer removes a thin layer of cells from the margin, and because H&E sections are not perfectly flat samples of the entire margin, comparison of pathological analysis with MVPro cannot be direct. This figure illustrates samples of each from the same specimen but should not be considered comparable views.
To take the first step of analyzing differences between cancerous cells and normal cells, we graphed the frequency distribution of pixels of different intensities (brightness) from darkest (0) to lightest (255; Fig. 3). The shapes of these frequency distributions, two from cancers and one from normal cells, differ in significant ways, especially when looking at the brightest pixels. Most obvious is the difference between cancer and noncancer, adding further evidence to our contention that cancer cells will emit a brighter signal. These differences, and additional features of the images, for example, entropy (Fig. 4) would be used in the ultimate analsys to find cancer cells. Indeed, image analysis algorithms will be developed using convolutional neural networks and deep machine learning to detect multiple relevant features to make an annotated heatmap of the MVPro image that indicates which areas contain cells likely to be cancer. This software will be provided to users as part of a kit containing reagents, equipment, and instructions.
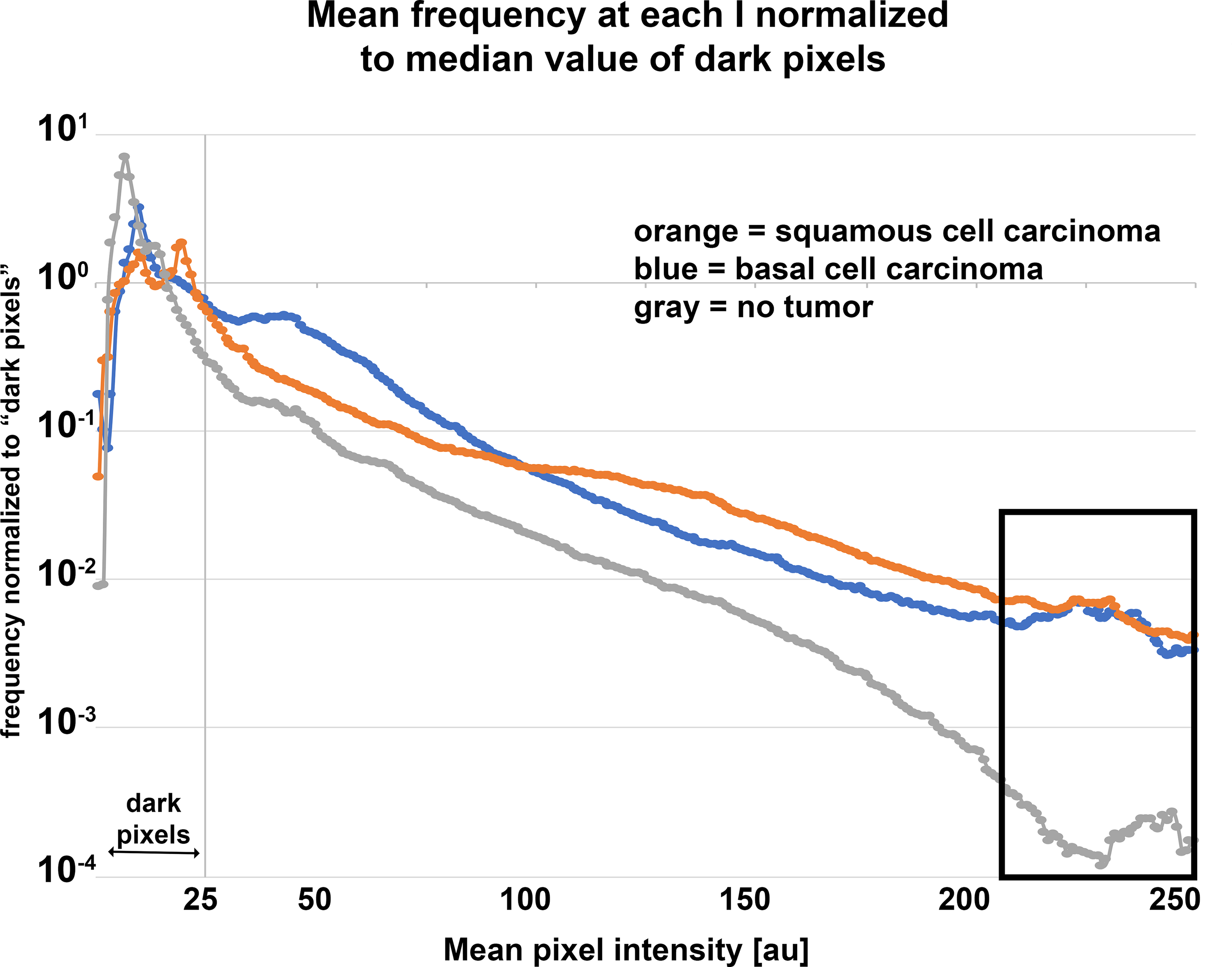
Comparison of mean pixel intensity frequencies. Mean frequency of pixel intensities in 8-bit MVPro images of BCC (blue), SCC (orange), and tissue with no tumor (gray). The frequencies have been normalized to the intensity of median intensity of the darkest 25 pixels in the image. The three cell phenotypes have different frequency distributions, the characterization of which will be one function of the algorithms to be developed using AI. Consistent with predictions, at higher intensities (boxed area) there can be >50X as many very bright pixels in cancer-containing specimens.
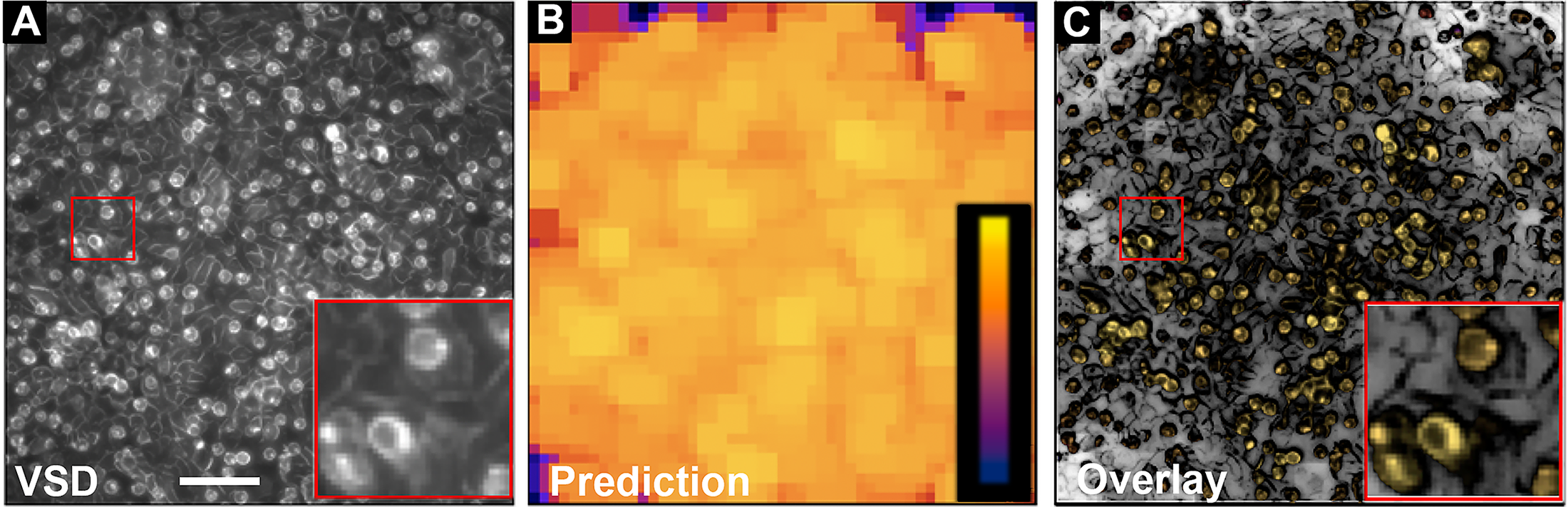
Preliminary AI algorithm finds cancer cells in vitro.
Preliminary modeling results
The results of preliminary experiments with an algorithm trained to analyze cells in vitro were based on the features of pixel brightness and entropy. Round, suspended, and labeled prostate cancer cells were added to an unlabeled monolayer of normal prostate cells displaying characteristic nonround shapes. The Akita VSD was then used to stain the mixture of cells, and the culture was imaged in situ (Fig. 4A). The prediction of the algorithm, where yellow indicates the highest likelihood of cancer, is shown in Figure 4B. The overlay of the negative of A and the positive of B (Fig. 4C) shows that the round cancer cells are labeled yellow while the normal background layer is not. In this simple system, the model produces exactly the correct result.
These results highlight the potential of MVPro to be a reliable and nondestructive technique for rapid cancer identification in surgical margins. Thus, it has the potential to be a useful IOI method and thereby improve surgical precision while preserving resected tissue for definitive histopathological diagnosis.
Discussion
The current reliance on H&E introduces significant challenges. The time-intensive nature of the process delays results. A global shortage of pathologists exacerbates the issue, particularly in resource-limited regions. These delays compromise patient care and may delay appropriate treatment. MVPro addresses these limitations by offering a real-time assay for cancer detection in living cells. The cells are collected by tissue transfer immediately after tissue is resected and just before the tissue is fixed for histological examination. The cells are then labeled with a VSD and imaged. MVPro rapidly produces an image of the VSD signal in the entire surgical margin in one 2D plane, allowing surgeons to identify residual cancer cells anywhere in the surgical margin. This approach has the potential to provide actionable data to the surgeon intraoperatively.
A rapid, accurate, and sensitive test for the presence of cancer cells has the potential to significantly enhance surgical outcomes and postoperative quality of life for patients. Such a test could provide invaluable real-time information to surgeons, enabling them to confidently balance complete tumor removal with the preservation of healthy tissue. This is quite different from the current practice of resecting a prescribed amount of tissue surrounding the believed area of cancer. Importantly, a portable and affordable assay could extend these benefits to diverse clinical settings, including private offices, field hospitals, and resource-limited clinics worldwide. Currently, for example, nitrocellulose is available in large sheets that, if cut to 4 cm × 4 cm, each MVPro membrane would be under $2.00 USD. A 25 mg bottle of DiBAC, containing enough dye for many thousands of cassettes, currently costs under $200 USD. Cassettes currently cost less than $1 USD and can be washed and reused. The only larger expense would be the setup cost of purchasing a fluorescence imager. Some facilities already have fluorescence microscopes; for others we hope to produce a dedicated imager that is customized for MVPro and would be available for under $5000 USD.
The preliminary experiments described here, conducted on surplus tissue from dermatological surgeries, allowed us to develop procedures and establish MVPro as a promising tool for mapping the distribution of nonmelanoma skin cancer cells in skin specimens. The findings underscore MVPro’s potential as a method to provide surgeons with critical intraoperative spatial information. The final version will be made available only if accuracy and sensitivity are better than 90%. In addition, NC membrane is inexpensive, as are many of the VSDs, and both are readily available, putting MVPro within the reach of underfunded health care facilities.
The limitations of the data described herein come from reliance on H&E and the small sample size available. Using H&E for this study limited the accuracy with which we could assess our results. This is because the analyzed sections to which we had access could not be the same plane as the print. Therefore, in future experiments we will use immunohistochemistry (IHC) for known cancer markers on the MVPro images themselves. Using the same cells for MVPro and for IHC analysis will guarantee that regions of MVPro images will be correctly annotated with cell phenotype, making them the ideal ground truth for machine learning. Future developments will also include simplifying the procedure by creating kits that include precut NC membranes, dye, cassettes that can be used to both apply the dye and image the print, software for primary analysis, and, perhaps, a dedicated imager customized for MVPro. The limitations of the method in general will be determined by the suitability of resected tissue for tissue transfer and the determination of the correct VSD for each cancer type. While there is no guarantee that all cancers will be candidates for MVPro, there are no theoretical reasons why any solid tumor, with its depolarized cancer cells, could not be examined this way. Importantly, trying out the procedure has no impact on patient care.
Expanding mvpro beyond nonmelanoma skin cancers
An important question is whether MVPro can detect other types of cancers. Preliminary observations on prostate cancer and cell lines suggest yes, remembering that MVPro’s utility depends on the VSD chosen and its sensitivity to the Vm ranges of both normal and cancerous cells. Extending MVPro to other tissue types will require further experimentation; nonetheless, we are confident that the underlying science examined herein will remain relevant to most solid tumors as well as metastases. Indeed, prior studies on Xenopus epidermal layers demonstrated that Vm differences between cells can persist post-transfer, suggesting the necessary degree of resilience needed for MVPro.
Potential for liquid biopsies, aspirates, and fixed tissue
Another intriguing possibility is the application of MVPro to liquid biopsies, fine-needle aspirations, and smears. While theoretically feasible, these applications pose challenges related to maintaining Vm integrity. Sampling methods that alter Vm—through changes in pH, for example—or that disrupt cell-cell connections may introduce artifacts that obscure the distinction between normal and cancerous cells. However, because MVPro is simple and inexpensive, this can easily be tested. Unfortunately, because fixation disrupts the membrane and inhibits ion translocators, it is currently not possible to use MVPro on already fixed tissues. However, there are VSDs that can be fixed within the membrane, such as those that have long alkyl chains or bulky, charged headgroups, such as certain Amino Naphthyl Ethenyl Pyridinium family of dyes (ANEPPS) derivatives. VSDs that are chemically bound to membrane proteins can also be fixed in place. Genetically encoded voltage indicators that are not diffusing freely can also be fixed in place.
Conclusion
Currently, the standard of care for cancer surgery is resection followed by fixation, H&E staining, and analysis by expert and experienced pathologists. This process takes a minimum of 48 h to complete, meaning surgery is complete before the surgeon knows whether there is a PSM. Thus, it is widely agreed that a fast IOI method could vastly improve patient care. MVPro is a novel, simple-to-use, affordable IOI modality. The potential clinical applicability is thus vast. MVPro could put rapid, surgical margin analysis into the hands of oncological surgeons worldwide, in advanced research hospitals and local clinics serving small communities. This would not only save patients from the emotional hardship of waiting for a result, but it could also speed the onset of treatment in addition to markedly reducing the number of PSMs. We show here that it does not interfere with the current standard of care, important because H&E will remain the definitive diagnosis. In addition, because MVPro is performed ex vivo, it adds no additional risk to patients. Using tissue transfer, voltage-sensitive dye, and a fluorescence imager, the entire surgical margin can be viewed as a single 2D image; machine learning techniques will be created for use, providing unbiased interpretation of the images within seconds. We propose that MVPro can fill a critical gap in current practice, making a fast technique affordable for all.
Authors’ Contributions
D.A. conceived and performed all experiments, all analysis, and wrote the article. D.S. performed comparative assays on voltage sensitive dyes and did preliminary work on in vitro cell cultures. O.A.-K. conceived and created the preliminary algorithm used to analyze in vitro prostate cancer images.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions of Dr. D. Greenstein and Dr. O. Badri. The authors thank two reviewers for useful comments that improved this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.