
Abstract
In science, one needs to have a eureka moment from time to time, in order to avoid falling into depression—it is not easy every day to be a researcher. Sometimes, these eurekas are the result of SERENDIPITY. However, in most of the cases, these eurekas are the result… of (experimental) RESULTS, that is, of WORK. But there is another category, the GREAT EUREKAS, that do not hit your mind many times in your life. I believe that I had only one GREAT EUREKA that, however, dictated my projects, experiments and successes for several decades.
Early Days
Following my PhD at the University of Toulouse, I started my post-doc in 1984, trying to solve the delicate issue of producing large amounts of Langerhans islets Beta cells, to help the insulin-dependent diabetics through the development of bio-engineered implants able to produce a regulated secretion of insulin. To this end, as a biochemist by education and cell biologist by training, my project involved the transfection of primary beta cells (an extremely fragile and difficult to obtain cellular material) with immortalizing oncogenes (recently discovered in the early 80s).
Among many awards, Professor Mir received the Balthazar van der Pol Gold Medal of the International Union of Radio Science (URSI) in 2017, the Giulio Milazzo Prize of the International Bioelectrochemical Society (BES) in 2021, the Honor Medal of the CNRS in 2023 and the D’Arsonval Award of the International Society on Bioelectromagnetics (BioEM) in 2024.

My First Eureka in “Bioelectricity”
To transfect the cells, in 1984, only chemical methods were available, and they were extremely deleterious for the cells. Almost no fragile cell, such as a primary beta cell, was able to survive to these procedures. This was an obstacle that could ruin my project. A colleague gave me an article published in PNAS in December 1984. In this paper, Potter et al. described an “electrical” method to transfect cells. 1 In a few words: “take a spectrophotometer plastic cuvette, prepare two strips from an aluminum foil, glue them to two opposite faces of the cuvette, and put an ISCO 494 electrophoresis generator in short-circuit by touching the two aluminum foils with the wires connected to the output of the current generator.” Simple, isn’t it? I had an ISCO 494 generator and a plasmid coding for a reporter gene. I tried on robust cells (an established cell line), and it worked: eureka!
But a limited eureka… a eureka “to survive”! Indeed, the only conceptual paper was the seminal 1982 paper of Pr. Eberhard Neumann. 2 In this, the term “electroporation” was used for the first time. Moreover, Potter’s system had no flexibility at all to adapt to other cells, in particular, fragile cells. I tried with a very safe Swedish electrophoresis generator: no transfection at all, as there was no leak when putting it in short-circuit. I tried with a French electrophoresis generator, apparently not safe at all, as it immediately burned when I put it in short-circuit (a pity for the colleague who had lent it to me)!
A More Interesting Initial Eureka: My Seminal Paper-Mir et al. (1988)
Thanks 3 to the director of the laboratory in Villejuif (near Paris), I was put in contact with Dr Justin Teissié, who later became an incredible colleague and friend, as well as his PhD student (at that time), Dr. Marie-Pierre Rols. Justin had developed an electric pulse generator able to deliver square pulses with independent control of the pulse duration, output voltage, frequency of the pulses repetition, and of the number of pulses (using a button “start pulsing/stop pulsing” and counting the pulses). The beginning of the eureka surged from the decision to use the Lucifer Yellow (LY) as an indicator of “poration” or “permeabilization”. Indeed, LY (from the firefly) is a highly fluorescent molecule that cannot cross the intact cell membranes. The experiment was simple: “mix the cells and the LY, pulse, wash the LY by centrifugation and observe the cells under the fluorescence microscope with the appropriate filters” (nowadays, this type of protocols are routine experiences). Interestingly, three types of cells could be observed under the fluorescence microscope: (1) “black holes” distinguished in the background fluorescence, (2) “highly fluorescent disks,” and (3) clusters of fluorescent spots occupying, more or less, the size of a cell. The first ones, displaying no fluorescence at all inside the cells, were cells exposed to the electric pulses but not permeabilized. The second ones were cells reversibly permeabilized (the LY could enter the cell, and when the cell membrane resealed, the LY remained entrapped inside the cell). The third group were cells permeabilized by the electric pulses in a way that the membrane could not reseal and the LY could be released, with part of the LY remaining in cytoplasmic pockets, heterogeneously distributed. These last cells were thus “irreversibly” permeabilized cells. Thus, using one single and simple test, it was possible to simultaneously determine transient and permanent cell permeabilization (therefore reversible and irreversible electropermeabilization) and to easily explore many different combinations of pulse parameters, what I did in a very systematic way.
Therefore, I could establish “optimized” conditions under which there was the death or the loss of less than 10% of the cells, more likely due to the cell manipulation, including cells trypsinization and centrifugation, rather than to the electric pulses. Among the more than 90% surviving cells, 98% were reversibly permeabilized, and only 2% of the cells exposed to the electric pulses were not permeabilized at all. These conditions (8 pulses of 100 µs duration and 1000–1350 V/cm field amplitude, delivered at a repetition frequency of 1 Hz) were approaching me to the possibility of transfecting “my” fragile cells, the primary beta cells, which needed the survival of the transfected cells.
Thus, eureka! But this eureka was not just an eureka “to survive”: it was a eureka “to help pushing” research toward new horizons. Indeed, since I had done my PhD in a laboratory of pharmacology, I understood that it was now possible to perform a new type of pharmacology using transiently and reversibly electropermeabilized cells, a new concept that led me to the EUREKA of my scientific career.
Serendipity and Results
Note the use of capital letters for this eureka! Actually, there were two eurekas, and one of them being a real one, a “major” EUREKA in bioelectricity. The minor eurekas are achievements that directly result from the experiments you have planned, even if these results are not only unexpected but even astonishing. The “major” ones are more “intellectual” and they provoke a shock: I really said “EUREKA.”
The facts were the following: with Stephane Orlowski, one of my first students (I was starting to have a “team”), we explored the possibility of changes in the pharmacology of the anticancer drugs known at this moment (1987) by exposing transiently electropermeabilized cells to these anticancer drugs. Many results were achieved in a very short time with drugs involved in the classical multidrug resistance mechanism of tumor cells or with drugs actively transported into the cells through the leucine or folate transporters. For those interested, I recommend the lecture of the article published with Stéphane in 1988 (Orlowski et al, 1988). 4 Because Stéphane worked quite well and fast, he still had a few weeks before finishing his stay in the team. What else to do? Directly or indirectly, all the anticancer drugs known at this time had been tested, but BLEOMYCIN. Thus, Stephane exposed the cells to bleomycin, a very different drug compared to all the others tested before and a drug for which the mechanism of penetration in the cells was unknown. Stephane was an excellent operator who was always successful doing experiments with cells, but I had to tell him: sorry, for the first time, you made a mistake since ALL the cells are dead. Start again. The experiment was done repeatedly, and then at lower concentrations of bleomycin. It became necessary to accept the huge (up to 10,000-fold) increase of the bleomycin toxicity if the cells were exposed to the electric pulses (Fig. 1). The latter is direct transcription of the experimental data, and it was reported in the Orlowski et al. (1988) 4 as well as in many of my presentations, and even in presentations by colleagues. Such an increase in bleomycin activity, which is the kind of increase that is never (or almost never) found in pharmacology, was already an important eureka, but not yet a major one. It was rather a product (important product, of course) driven by the RESULTS and the SERENDIPITY.

Increased uptake of bleomycin induced by exposure of the cells to electric pulses. Chinese hamster lung fibroblasts (DC-3F cells) were used as a model. Use of semi-logarithmic coordinates demonstrates the increased toxicity very clearly. Adapted from Orlowski et al. (1988). 4
The EUREKA of my Scientific Career
The MAJOR EUREKA came later. Figure 1 displays the huge increase of toxicity, but it did not allow us to explain what was really occurring. This curve was fitting none of the classical pharmacological models used for molecular toxicity at the time. Worst: because the increase in toxicity was so important, I had to use logarithmic coordinates for the X axis (molar concentration of bleomycin). Then, Y axis in Figure 1 was in linear coordinates as the dogma was that it was necessary to avoid double logarithmic coordinates (under which all the curves would be “artificially linearized”). However, the semilogarithmic coordinates in Figure 1 were not the traditional ones (usually, X axis/concentration is in linear coordinates, while Y axis/cell survival is in logarithmic coordinates). So, in the absence of any appropriate model, what could I do to understand the toxicity depicted in Figure 1?
After many days of questioning, I dared to use double logarithmic coordinates (Fig. 2, panel A). As expected, the cytotoxicity curves were linearized. Different linear segments were identifiable. Is there a meaning of the toxicity, or a rational explanation of it, contained in these linear segments? No clear explanation, no understandable behavior…

Various linear segments of bleomycin-induced toxicity revealed using double-logarithmic coordinates. Curve 1-cytotoxicity of bleomycin on cells not exposed to the electric pulses. Curve 2-cytotoxicity on cells exposed to the optimal electropermeabilization conditions (98% of reversibly permeabilized cells and 2% of nonpermeabilized cells in spite of the exposure to the electric pulses). Curve 3-cytotoxicity on cells exposed to bleomycin and to suboptimal electric pulses (of lower field amplitude) resulting in 88% of permeabilized cells and 12% of nonpermeabilized cells.
Then, the TRUE EUREKA, the big one, suddenly exploded in my brain. This did not happen in the bath, as for the Greek philosopher Archimedes, nor whilst taking a shower. It happened one morning, in my car, when I was driving towards the laboratory. In a matter of seconds, everything became clear, transparent, luminous, great. All the linear segments acquired their own “personality” (Fig. 3). The 98% of the reversibly permeabilized cells exposed to optimal electric pulses conditions (and the 88% under suboptimal pulses conditions, at a lower field amplitude) were ALL killed below 10 nanomolar bleomycin. The behavior of the 2% (or 12%) of cells exposed to the electric pulses but not permeabilized was IDENTICAL to the behavior of the control cells NOT exposed to the electric pulses, the curves displaying the same slope.
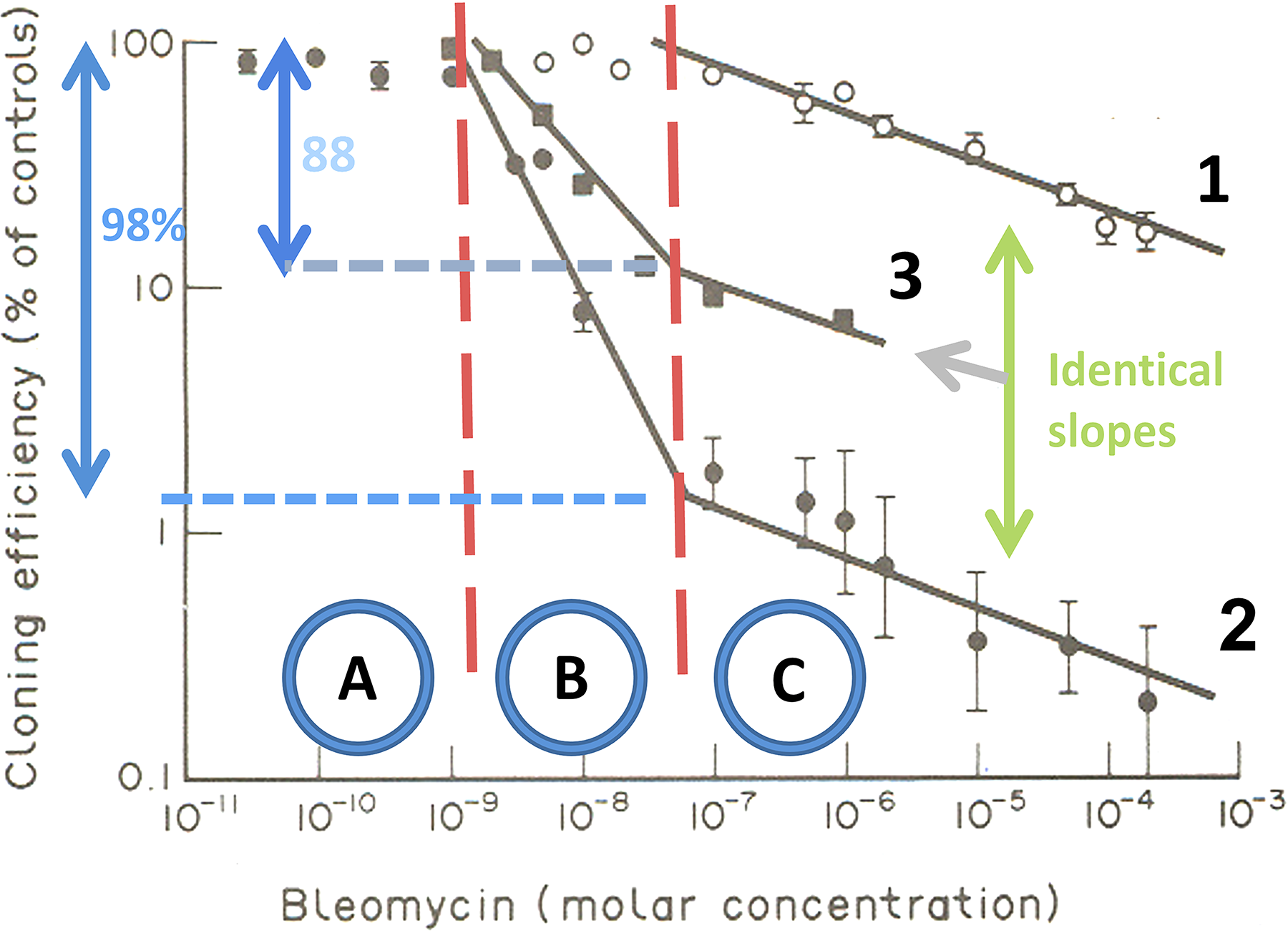
Data from Figure 1 plotted on double-logarithmic coordinates. This analysis showed that nM bleomycin killed the cells maximally only if they were electropermeabilized. The meaning of the three zones (A, B, and C) is detailed in the text.
Thus, there are 3 zones as a function of the concentration of bleomycin. Below about 1 nanomolar, bleomycin is not cytotoxic (zone A). Between about 1 and 30 nanomolar, only the electropermeabilized cells, but ALL of them, are sensitive to the bleomycin and are killed by the drug (zone B). Above 100 nanomolar, the cells not exposed to the electric pulses, or exposed but not permeabilized, start to be killed by the bleomycin (zone C).
The main consequence was that, provide the cell is permeabilized, the bleomycin at a few nanomoles concentration will kill the cell, and if translatable in vivo, a new treatment of the tumors was possible. This MAJOR EUREKA not only allowed me to explain results that remained obscure until that moment, but moreover, it allowed me to anticipate and to perform magnificent experiments in bioelectricity in the next steps of my scientific career.
The Consequences of the Major EUREKA
It is not wrong to say that a major eureka moment transforms your life. Understanding that very small amounts of bleomycin, not toxic, could be extremely efficient in killing the cells IF and ONLY IF the cells are nonlethally (reversibly) electropermeabilized allowed to reach a number of achievements, each one being also a eureka!
Moreover, it happened that I had the chance to move from one eureka to the next one quite rapidly. The first push was given to me by Pr. Enrico Mihich, from the Roswell Park Cancer Institute and director of the Grace Cancer Drug Center, with whom the director of my new lab (Pr. Claude Paoletti) had regular meetings. I presented my results and Pr. Mihich asked me: What’s the next step? I started to say that I needed to confirm with other cell lines, then with aggregates of cells… STOP! yelled Pr. Mihich: move immediately to mice with tumors!
I followed his advice. Just a few days later, I performed the first experiment with my colleague Jean Belehradek Jr, who initiated me to the mice tumor models, whether transplanted or spontaneous. The in vitro optimized electric pulses parameters were delivered locally to tumors transplanted in mice, after injecting (or not) the bleomycin intravenously 3 min before the delivery of the pulses (with plate parallel electrodes directly inspired from the cuvettes for the in vitro experiments). While the tumors treated with the pulses alone grew as the controls (as expected from REVERSIBLE electropermeabilization that does not kill the cells), and the tumors treated with the bleomycin alone also grew as the controls (as expected from the injection of a single low dose of bleomycin), in the case of the tumors treated both with bleomycin AND the electric pulses, all tumors went in complete regression. Later on, we observed early recurrences at about 5–10 days, when the mice of the other groups had already to be euthanized because of the continuous growth and size of their tumors. We also observed late recurrences, but, already in the first experiment, several mice were CURED (no recurrence for more than 60 days after the occurrence of the complete regression of the tumor). All in all, a new incredible eureka.
I coined the term “electrochemotherapy” (ECT) and published these results in 1991. 5 Supplementary eureka: similar interesting results were achieved on spontaneous tumors in mice, an important issue because the relations between the host and a transplanted tumor or a spontaneous tumor are quite different. 6 The work with murine spontaneous tumors was very important because in humans, tumors are never transplanted, but always spontaneous.
More Eurekas Followed…
The next eureka was the first-in-human application of electrochemotherapy. 7 The Ethics Committee of Gustave Roussy, the largest cancer center in Europe, where the CNRS laboratory was located, authorized us to treat one single permeation node of epidermoid carcinoma per patient. We followed the recommendation for the first patient, who actually displayed five superficial nodules. The one treated nodule disappeared in less than 7 days, while the 4 other nodules continued to grow. The patient himself asked us to treat the four other nodules, a request that was impossible not to fulfill. In the next patient, more than one nodule (actually all the visible nodules) were treated. This was also an incredible eureka!
Many other eurekas followed. These included the first article of Electrochemotherapy in Veterinary Medicine in 1997. 8 A second paper (by another group) followed 5 years later. Other developments were the first combination of ECT with an immunological agent resulting in increased percentage of cured animals after a single ECT session. 9 There was also the combination of ECT and more potent immunological agents, which resulted in the achievement of systemic antitumor effects.10,11
Then, a new period in my career started. At the turn of the century (and millennium), I was still team leader, but I had the chance to get approved three major European Grants in the row and to coordinate the EU Projects Cliniporator, ESOPE, and Angioskin, from 2000 to 2009. The next eurekas were no longer my eurekas but those of a group of very dedicated and excellent teams. We produced the Cliniporator generator, CE marked and used in the clinics all around Europe (and nowadays also abroad). We wrote the European Standard Operating Procedures of the Electrochemotherapy using the Cliniporator 12 and validated them in a multicentric clinical trial. 13 We developed approaches for the transfer of genes using the electric pulses (two of the groups having been among the world pioneers in this field)—Rols et al. (1998) 14 and Mir et al. (1998,1999).15,16
In those European Projects, there is almost no possible eureka! Indeed, to get financed you need to write all that you will do and test, and there is limited room for serendipity and eurekas since unexpected, totally new results are not foreseen. I never wrote a project in which I anticipated the discovery of “electrochemotherapy”!
Eurekas Are Still Possible out of Formal Projects
Good news, there is still some room for new eurekas… With the development of ECT in the clinics to treat cutaneous and subcutaneous lesions, various groups started to apply ECT in the case of internal tumors (e.g., liver, pancreas) as well as of bone metastases, for which results were very interesting. Indeed, normal bone was already being regenerated in the volume previously occupied by the metastases while the ECT-treated bone metastases were still regressing, preventing secondary fractures due to the treatment. François Cornelis, working at that time at Hôpital Tenon, Paris, contacted me because he had a patient with a bone metastasis in the vertebra, suffering from an incapacitating, very intense pain, with no classical option to offer to his patient. François asked me: “Can I propose ECT to this patient?” I told him YES, we discussed on the approach, he placed needles in the vertebrae near the spinal cord, and performed the ECT. We (François and I) were really anxious at the moment of the treatment because it was the first time ECT being delivered close to such a sensitive and important structure like the spinal cord. The treatment went really well, the pain resumed very rapidly, and the metastasis regressed as well, even if metastasis regression followed a slower kinetics. 17 This result was also a eureka. Frédéric Deschamps, at Gustave Roussy, has now acquired tremendous experience for the treatment of vertebral metastases compressing the spinal cord. We published the results on the 40 initial patients. 18 He has treated more than 300 patients nowadays.
Eureka or Satisfaction?
Similarly, I still could have said eureka recently, but it was more a feeling of satisfaction, when I knew that exactly the same protocol and concept than ECT are being used to treat low-flow vascular anomalies (using “BEST”—Bleomycin ElectroScleroTherapy) 19 or fast-flow vascular anomalies (using “BEET”—Bleomycin ElectroEmboTherapy). It is a pleasure for me to contribute to the dissemination of ECT for the vertebral metastases and of BEST and BEET through masterclasses with Frédéric Deschamps, Walter Wolhgemuth and others. Vascular anomalies are not oncological situations, and BEST and BEET can work because of the use of REVERSIBLE ELECTROPORATION, meaning that the electric pulses are just a way to vectorize a drug (the bleomycin in that case), without causing cell death by themselves. This is still, maybe, a conceptual consequence of my very initial purpose: to transfer genes into very fragile primary beta cells. I also contributed to the development of the IRREVERSIBLE electroporation as an ablative method, 20 but I consider that my most important contributions are in the field of REVERSIBLE electropermeabilization.
The Best EUREKA of my Life!
Looking back at my scientific career in bioelectricity, with a part of serendipity and a part of work, and, by chance, many eurekas, I finally believe that the EUREKA of my life has not been receiving various distinctions (such as the Franck Reidy award in Bioelectricity, the Giulio Milazzo Price in Bioelectrochemistry, the D’Arsonval Award in Bioelectromagnetics and the Balthazar van der Pol Gold Medal in Radiosciences), nor academic recognition (three Doctorates Honoris causa, honor medal of the CNRS), but knowing that tens, hundreds, thousands, tens of thousands of patients are treated using the concepts and tools that I helped develop during my scientific career. Knowing that their oncologic conditions have been alleviated, that pain linked to some cases is relieved and that vascular malformations are corrected-that is my best EUREKA!
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.