
Abstract
Real-time electrochemical measurements of ionic fluxes and bioelectric signals are set to refine cancer diagnosis and longitudinal follow-ups with the goal of targeting electrophysiological features of clinically useful matrices. Nanoengineered electrodes translate biomolecules and ions into robust electrochemical signals for both laboratory workflows and point-of-care testing. The translational aim is to integrate electrochemical sensing into coherent, physiology-grounded readouts that resolve tumor ion channel dysfunction, membrane depolarization, pericellular acidification, and redox imbalance. Realizing this vision now depends on practical engineering and clinical integration. To advance this ongoing development, researchers are building stable, disposable, portable, and miniaturized electrochemical platforms that couple detection with microfluidics to enrich tumor cells, vesicles, and bio ionic markers for multiplexed cancer measurements. The integration of wearable and implantable systems with machine learning and patient-specific digital twins will enable real-time maps of tumor electrophysiology and model-driven forecasts of treatment response. This perspective outlines a translational roadmap for electrochemical detection of bioelectric biomarkers in cancer, wherein biomarker classes are systematically mapped to corresponding transduction strategies and mechanistic fidelity is reconciled with practical assay design constraints to identify key challenges and opportunities for advancing these technologies from foundational research to validated clinical implementation in precision oncology.
Introduction
The development of cancer results from genetic and biochemical alterations together with disrupted sensing, signaling pathways, and coordination problems in the tumor microenvironment (TME).1,2 Among these factors, bioelectricity has emerged as a critical yet underexplored regulatory axis, built on three interconnected elements: the transmembrane potential (Vm), ionic fluxes, and endogenous electric fields shaped by the coordinated activity of ion channels, pumps, and gap-junction coupling. 3 Bioelectricity refers to the natural electrical signals produced by cells and tissues, which include Vm, ion fluxes, and local electric fields. The coordinated function of ion channels, pumps, and transporters regulates Vm through their control of Na+, K+, Ca2+, Cl−, H+, and Zn2+ ions.4–6 These ionic events alter charge transfer, impedance, and redox activity, making electrochemistry an ideal platform to interrogate bioelectric states in cancer.
In cancer, cells tend to lose their normal electrical balance and exhibit altered Ca2+ signaling pathways, which enable their migration and growth and protect them from cell death. 7 Tumors exhibit distinct ion-channel fingerprints that expose dysregulated bioelectric signaling. In colorectal cancer, the K+ channel potassium voltage-gated channel subfamily Q member 1 (KCNQ1) retains β-catenin at cell-cell junctions to preserve epithelial identity, whereas its loss triggers epithelial-mesenchymal transition (EMT) and invasion. Clinically, elevated KCNQ1 together with its subunit KCNE3 associates with improved relapse-free survival, consistent with a tumor-suppressor role. 8
Ion channels translate genetic and microenvironmental cues into electrical signals that shape cellular phenotype. In breast cancer, the neonatal Nav1.5 splice variant (nNav1.5) boosts motility and invasion, and its in vivo activity accelerates tumor growth and dissemination. 9 Bridging excitability with the microenvironment, Nav1.5 also potentiates Na+/H+ exchanger-dependent proton efflux, facilitating matrix degradation and invasion. 10 Proton fluxes can be quantified with electrochemical pH sensors and impedance spectroscopy, translating channel activity into measurable extracellular acidification. In prostate cancer, the Ca2+-selective channel transient receptor potential vanilloid subfamily member 6 is upregulated in aggressive tumors and drives proliferation via Ca2+/NFAT signaling, illustrating a direct channel-to-transcription pathway. 11 Because Ca2+ influx generates distinctive ionic signatures, electrochemical sensors and field-effect transistor (FET) platforms enable real-time monitoring of these dynamics. In melanoma, transient receptor potential cation channel subfamily M member 1 (melastatin) is regulated by microphthalmia-associated transcription factor (MITF) and exhibits isoform complexity; its downregulation during progression underscores how lineage-specific transcription factors wire channel programs into tumor evolution. 12 Collectively, these examples identify aberrant ion-channel activity as both driver and biomarker reservoir, transforming bioelectricity from a mechanistic phenomenon into a clinically relevant diagnostic class.
Ion channels provide two biomarker modes: static readouts of expression, localization, and isoforms, and functional readouts of electrical and chemical effects in vivo and in biofluids. Functional sensing needs high signal-to-noise ratios in complex samples, as shown by urine-compatible electrochemical methods such as label-free voltammetry for prostate cancer antigen 3 (PCA3) RNA and printed assays for urinary exosome microRNAs (e.g., miR-21, miR-451) that track tumor stage.13,14 These achievements demonstrate that electrochemical systems validated through nucleic acid analysis can detect ionic targets.
Conventional cancer diagnostics, including histology, immunohistochemical (IHC), molecular tests, protein immunoassays, and centralized laboratory instruments, remain essential in clinical practice.15,16 In parallel, point-of-care (POC) electrochemical formats now discriminate patients from controls using serum or blood within minutes, at low cost and with quantitative readouts.17–20 Bridging central-lab precision with POC speed defines a practical path for bioelectric diagnostics.
Electrochemistry is well suited to this task, directly converting ion activity, interfacial charge, and impedance into sensitive, low-cost signals.21,22 Field-effect and impedance transduction can capture ionic signatures alongside protein and nucleic-acid markers on a single chip, maintaining lab-grade rigor through on-chip referencing and calibration. An extended gate FET and label-free impedimetric have quantified Zn2+ in urine and distinguished polycations, demonstrating label-free, portable readouts of voltage, current, and impedance.4,23 These platforms pair with high-precision electrochemical calibrators such as microfluidic poly-horseradish peroxidase immunoarrays and nanochannel-enhanced electrochemiluminescence (ECL) that match central-lab analyzer performance in serum, and use antifouling, ratiometric designs to maintain signal integrity in complex matrices.24–27 For nucleic acids, impedance/voltammetric PCA3 genosensors provide complementary urine-ready workflows and analytics that can double as on-chip controls and normalizers.28,29 Paired with immunomagnetic microfluidics and polymerization-based amplification, this enables early detection, therapy monitoring, and scalable POC use as a low-cost complement to histology, IHC, and molecular testing.30,31
Despite substantial progress, important clinical gaps persist. Current oncology diagnostics often deliver slow turnaround for molecular profiling, carry high sequencing costs, and lack functional biomarkers that dynamically track treatment response. Bioelectric signatures can address these shortcomings by reporting directly on tumor physiology. Unlike genomic or proteomic assays, they are dynamic, inexpensive, and deployable at the POC. Positioning bioelectric biomarkers alongside genomics and proteomics establishes them as a complementary pillar of multi-omics precision oncology. It adds functional context to molecular alterations, informing early detection, patient stratification, and therapy guidance. Electrochemical systems are portable and affordable, which extends access in resource-limited settings where advanced molecular diagnostics remain out of reach.
This perspective outlines a preclinical-to-clinical roadmap for electrochemical detection of bioelectric biomarkers in cancer. This approach positions the classes of biomarkers to the transduction strategies, the assay format and clinical matrices. Further, it combines mechanistic fidelity with practical assay design. It brings out performance standards, pre-analytical requirements and deficits in isoform specificity and reproducibility. It is aimed at rapidly translating bioelectric biomarkers to the next stage of life between academic concept and validated clinical tools to make electrochemistry a viable diagnostic pillar, which contributes to early diagnosis, risk stratification and real-time monitoring in cancer.
Translational Roadmap for Electrochemical Detection of Bioelectric Biomarkers in Cancer
A practical actionable pathway for electrochemical bioelectric biomarkers in oncology begins by defining target product profiles (TPPs) that align mechanistic readouts with concrete clinical decisions. The most immediate opportunities are in ex vivo applications that preserve cellular physiology: early discovery and patient stratification using live cells from resections or biopsies, pharmacodynamic monitoring of bioelectric responses during therapy titration, and diagnostic adjuncts that complement histopathology by reporting EMT state or metastatic potential. Impedance-based phenotyping already distinguishes EMT states in prostate cancer and separates metastatic lineages, motivating the framing of decision thresholds and turnaround times that could integrate with current diagnostic workflows.32–34 Because the ultimate aim is mechanism-informed measurement rather than mere classification, these TPPs should prioritize rapid assays on minimally processed samples under perfusion to preserve native ion-channel and transporter function. Once clinical decisions and assay constraints are defined, the next step is to identify the bioelectric variables to measure and link discrete ionic activities to whole-cell Vm.
The biomarker panel should couple specific ionic activities to whole-cell electrical properties to resolve the contributions of ion channels, pumps, and transporters that set the membrane potential. Localized extracellular potassium near the cell surface and single-cell calcium uptake are particularly informative because of their tight linkage to Vm and channel dysregulation in cancer. Recent potentiometric studies demonstrate near-membrane mapping with a K+-selective scanning electrochemical microscopy tip held micrometers above adherent breast cancer cells, resolving line-dependent differences and stimulus responsiveness, 35 while an all-solid-state Ca2+ microelectrode integrated with patch clamp quantifies real-time uptake at the single-cell level with nanomolar sensitivity. 36 Having identified the informative ions, we select transducers that can reliably read them in physiological media.
These ion-specific readouts can anchor mechanistic interpretation when combined with whole-cell transduction. On that front, field-effect architectures modeled for operation at physiological ionic strength can report Vm-sensitive changes without resorting to low-ionic buffers, 37 and organic electrochemical transistors (OECTs) equipped with crown-ether-functionalized gate polymers selectively transduce Na+ or K+ over physiological ranges at low voltages compatible with live-cell assays. 38 In parallel, frequency-resolved electrical impedance spectroscopy offers complementary dielectric parameters-membrane capacitance and, with rigorous fitting, membrane resistance-that contextualize ionic fluxes and cell–substrate interactions; recent implementations already correlate capacitance and spectra with metastatic potential and EMT transitions, though most stop short of explicit Vm-component deconvolution.32–34 To achieve effective clinical translation in the future, multi-sensing applications on one perfused microfluidic chip which most effectively aligns with optical microscopy should be incorporated: potentiometric sensor tuned to local K+ and single-cell Ca2+ measurements, field-effect and organic electrochemical transistor tuned to whole-cell electrical measures and frequency-resolved impedance spectroscopy. Simultaneously, soluble ion and metabolite measurements in readily available biofluids can be used to measure systemic transport dysregulation.
Electrochemical cancer biomarker detection advances along two complementary routes: direct measurement of ions and metabolites that report dysregulated transport and membrane-potential shifts, and electrical interrogation of tumor-derived macromolecules whose expression reflects altered ion handling. Urine is a practical matrix, with examples such as zincon-based impedance sensing of Zn2+, 4 molecularly imprinted films read by voltammetry or FETs for spermine, 23 and enzyme-free redox chemistries for sarcosine; all require stringent selectivity in complex matrices and prospective clinical validation. 39 To complete the picture, macromolecular assays profile upstream expression programs that drive or respond to this ion-handling phenotype.
Macromolecular electrochemical assays encompass nucleic acids and proteins. In urine, PCA3 and miRNAs are quantified on screen-printed electrodes via hybridization or redox-tagged probes, routinely achieving picomolar limits and clinically meaningful discrimination.13,14,40 For proteins, ECL implemented on mesoporous indium tin oxide or graphene–quantum-dot architectures attains sub-pg·m−1 sensitivity with robust serum recoveries.24,26,41 Drift is mitigated through ratiometric readouts and peptide-based dual-mode designs, while microfluidic immunoarrays support multiplexed serum panel;25,27,42 for near-patient triage, rapid electrochemical immunochromatographic strips operate directly in whole blood or serum. 43 Integrating these layers supports a staged development plan that progresses from mechanism faithful discovery to validated, multiplexed panels ready for clinical use.
Taken together, the translational roadmap for electrochemical detection of bioelectric biomarkers in cancer advances through a staged yet integrated strategy that emphasizes mechanistic fidelity at the single-cell level, selective and multiplexed molecular assays in accessible fluids, and platform designs that fit seamlessly into clinical workflows. Early milestones should focus on perfused, chip-based assays that preserve ionic physiology for discovery and patient stratification; the medium term should emphasize robust urine and serum panels built on printed electrodes with embedded calibration; and long-term success will depend on harmonized performance standards, cross-site reproducibility, and regulatory-grade validation that ties assay readouts to treatment decisions. Anchoring each stage in ion-channel and transporter biology ensures that readouts are not merely correlative but inform clinical decisions in precision oncology. By deliberately linking measurement to the ion-channel and transporter dysregulation that drives malignancy, electrochemical platforms can convert bioelectric insights into practical diagnostic tools; this pathway can move bioelectric biomarkers from academic concept to operational pillar, supporting early detection, risk stratification, and real-time monitoring that complement and extend current genomic and proteomic diagnostics. The discovery-to-clinical-adoption translational pathway follows a structured format which shows how biological targets, sensing modalities and clinical objectives match between research and regulatory stages (Fig. 1).
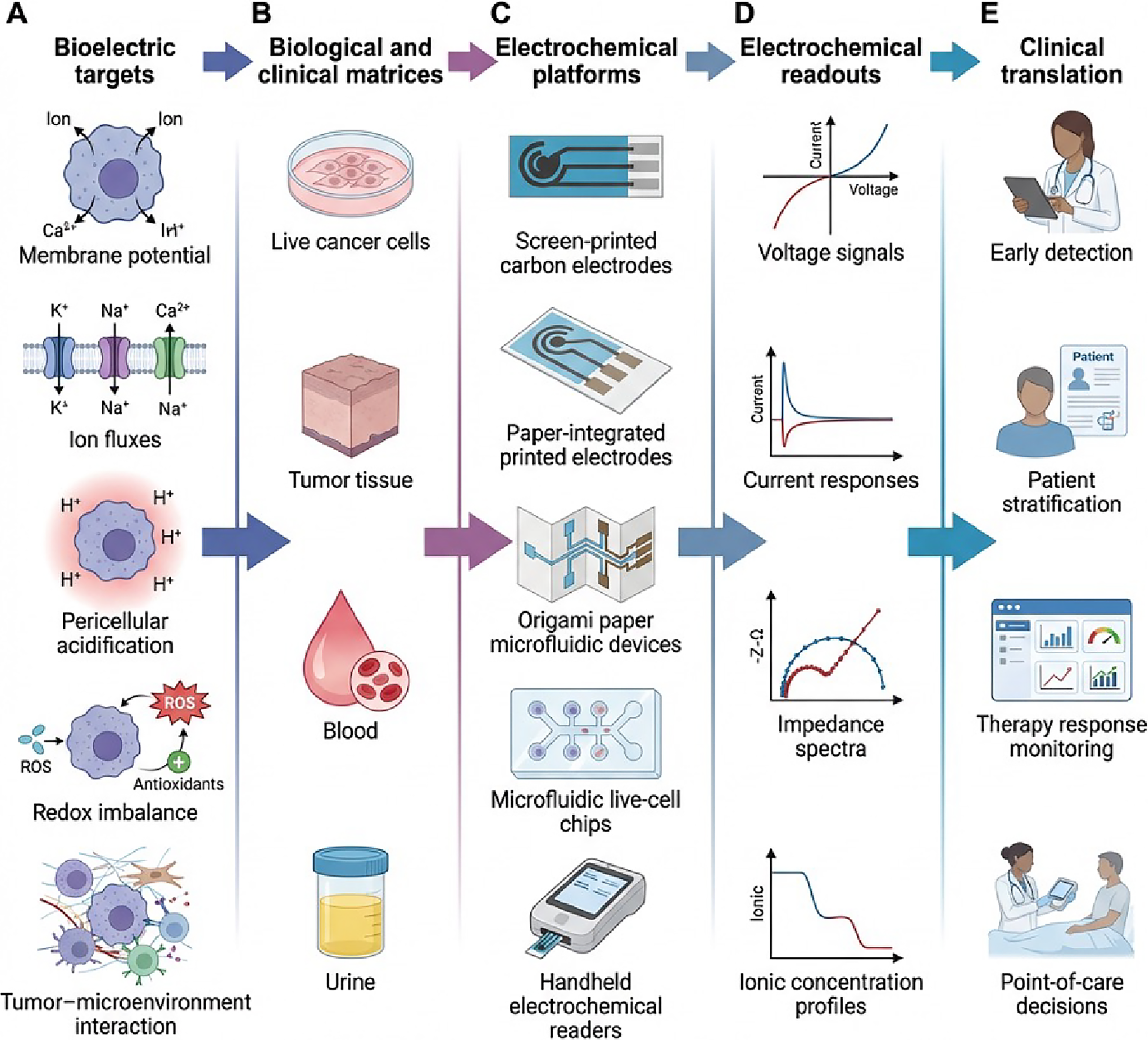
Translational roadmap of bioelectric electrochemical sensing in cancer: from targets to clinical decisions.
Challenges, Limitations, and Future Perspectives
In spite of these rapid advances, electrochemical translations of electrochemical biomarkers in cancer are hindered by a series of interdependent barriers. The heterogeneity of tumors among patients and even within tumors renders universal diagnostic thresholds because the ion channel dysregulation and membrane potential is different by type of cancer and even by microregion. Bioelectric dynamics are influenced by hypoxia, extracellular pH, and stromal interactions, compromising reproducibility. The absence of stringent patient stratification and strict biological context also means that measurements will tend to be descriptive, as opposed to actionable, and they will need the parallel evolution of biosignature models between detected signals and clinical outcomes of defined subpopulations.
The implementation across the measurement pipeline is limited due to technical problems. Electrode contamination, biomolecule deposition, and signal drift in complex media like serum and urine are commonly seen, and despite some improvement in variability by ratiometric processing, the stability of such systems over time has not been demonstrated to be reliable enough to be used in practice. Small, multiplexed, ion transport-compatible chips are challenging to design, and selectivity is impaired by a small isoform selectivity and off-target cross-reactivity. Lack of calibration standards and interlaboratory standards is a drawback of analytical rigor. Most of the studies are in one center with controlled pre-analytical conditions, where variability does not represent the routine variability of the sample collection, handling, and storage. There is limited multicenter validation, and small-scale or retrospective data restrict the ability of the validity of statistical power and generalization.
Regulatory translation entails proving usefulness in clinical use other than analytical usefulness. It will be necessary to demonstrate that bioelectric readouts have a significant impact on treatment decisions and patient outcomes, and the current regulatory frameworks are largely designed to address molecular diagnostics, with little precedent to bioelectric assays and confusion regarding how agencies set the limit of detection, dynamic range, and the reproducibility standards. Limited cost-effectiveness analyses make adoption impractical in the daily oncology practice, and in low-resource environments, these two factors are key obstacles to adoption.
The integration of single-cell ion-selective measurements with either impedance-based or transistor readouts on perfused microfluidic platforms could provide mechanistic insight in the near term. Medium-term objectives should focus on multiplexed urine and serum panels placed on the printed electrodes using ratiometric calibration and inbuilt machine learning algorithms to boost robustness and classification stability. For long-term translation, international performances standards must be put in place, multi-site reproducibility research, and prospective clinical trials in which bioelectric signatures are conclusively determined to have a direct relationship to therapeutic determination. New breakthroughs in organic electrochemical transistors, nanoscale potentiometry, and microfluidic immunoarrays will increase sensitivity and throughput, and integration of these devices with artificial intelligence may provide an opportunity to track dynamic ionic signatures and mechanical response tracking dynamics, and ultimately translate bioelectric biomarkers to clinical action.
In particular, it has been demonstrated that machine-learning-assisted identification of electrochemical signatures has the potential to combine multimodal data-impedance spectra, voltammetric signals, and ion-selective electrode reading to provide better diagnostic accuracy at a higher level than simple single-parameter thresholds. Pattern recognition algorithms used to the multiplexed impedance and ion-flux data can detect the complex bioelectric fingerprint that differentiates between the subtypes of cancer, predicts whether it will metastasize or not, and real-time therapeutic response. Early treatment resistance can be detected using deep learning methods on biometric temporal bioelectric data because small changes in patterns before clinical outbreaks can be predictable.
Convolutional neural networks trained on electrical chemistries in electrochemical impedance spectroscopy have also been shown to distinguish cell phenotypes with high accuracy, whereas recurrent neural networks can track cell evolution of ionic signatures in the process of drug exposure. 44 Additionally, it could be connected to patient-specific digital twins computational models and predict treatment responses, and optimize specific therapies after individual-tumor electrophysiology with measured bioelectric parameters. These digital twins that are constantly refreshed with the electrochemical readings could enable clinicians to model the outcome of ion channel-targeted therapies or chemotherapeutic agents prior to administration, which could be used in the approach of precision medicine in oncology. 45 Electrochemical bioelectric biomarkers may be used to amplify both genomic and proteomic diagnostic with bridging the mechanistic fidelity and clinical applicability, able to be used in oncology early diagnosis, risk stratification, and precision monitoring.
Authors’ Contributions
S.S. and A.R. contributed to the study design, writing, and revision of the article. A.Gl. and G.I. provided critical feedback and assisted in refining the written content. S.C., S.G., A.D.L., A.Gi., and M.D.L. supervised the work, contributed to the final revisions, and approved the submitted version. All the authors reviewed and approved the article prior to submission.
Footnotes
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
The research leading to these results received funding from AIRC under MFAG 2022-ID. 27586 project-P.I. S.C. This project has received funding from the European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie grant agreement No. 101110684 SMART-S.S.