
Abstract
Spinal cord injury (SCI) disrupts neurological pathways controlling movement, sensation, and autonomic processes, commonly causing long-term impairments. The restoration of damaged spinal tissue continues to pose significant therapeutic challenges. The RISEUP project explores an innovative combinatorial therapy that integrates stem cell transplantation with µsPEFs delivered by an Electro-Pulsed Bio-Hybrid (EPB) device. This in silico study faithfully reproduces the in vivo experimental setup that will be applied within the project to assess EPB functionality and stimulation effects. By positioning the EPB numerical model over the thoracic vertebral region of interest in the ViZOO Neurorat anatomical rat model, and by implementing laminectomy and SCI, a virtual replica of the in vivo experiments is proposed, aiming to inform, in a prospective way, whether electric (E-)field intensities estimated by in vitro studies and microdosimetry and shown to be suitable for electroporation could be reached in vivo, in the complex and evolving environment of the injured spinal cord. To reflect the biological evolution of SCI over the stimulation time, two lesion phases were simulated. First, acute SCI represents the immediate post-injury environment, while chronic models capture the later phase characterized by altered conductivity and structural reorganization. This dual-phase approach allows for a more accurate assessment of the experiments. Finally, dosimetric assessment was computed and evaluated in terms of induced E-field distribution, and peripheral nerves response. Peak E-fields beneath the EPB ranged from 20 to 70 kV/m, sufficient for transient membrane permeabilization and stem cell activation. Field penetration improved in chronic lesions due to increased conductivity, with deeper median fields (∼2 kV/m) compared to acute models. Neurofunctional safety was evaluated by coupling the E-field output to axonal electrophysiological models of intercostal nerves. The findings demonstrate that the EPB device can deliver effective, localized stimulation with minimal off-target neural activation. Furthermore, temporal lesion evolution influences field distribution, underscoring the importance of phase-specific assessment.
Keywords
Introduction
Spinal cord injury (SCI) is a devastating clinical condition resulting in severe motor, sensory, and autonomic dysfunctions, often leading to permanent disability. The global incidence of SCI ranges from 10 to 83 cases per million people annually, with traumatic causes such as vehicular accidents, falls, and sports injuries being the most common.1–3 Nontraumatic SCI, arising from tumors, infections, or degenerative diseases, is also increasingly recognized. 4 In traumatic SCI, the initial mechanical insult causes immediate tissue damage, which is subsequently worsened by secondary injury cascades. 5 These include excitotoxicity, ischemia, oxidative stress, and inflammatory responses, ultimately leading to glial scar formation and cystic cavity development. Such pathophysiological changes create a hostile environment for axonal regeneration and severely limit the central nervous system’s intrinsic capacity for recovery.6,7
Currently, clinical treatments for patients diagnosed with SCI do not provide a cure, although various strategies, including pharmacological, surgical, and neurophysiological approaches, have been developed to promote functional recovery.8,9 To overcome these challenges, various therapeutic strategies have been investigated.6,10,11 Among them, neuromodulation has emerged as a promising approach,12,13 employing controlled electrical or magnetic stimulation to modulate neural circuit activity and facilitate motor function recovery.14–16 Notably, epidural electrical stimulation (EES) has demonstrated considerable success in enabling voluntary movement in individuals with incomplete SCI, particularly when residual descending pathways are preserved.16,17 However, EES efficacy depends on the presence of sufficient spared fibers and functional relays, limiting its application in cases of extensive damage.18,19 Complementary to neuromodulation, tissue engineering strategies aim to restore spinal cord continuity by implanting scaffolds composed of biomaterials and stem cells.20–22 These constructs are often enriched with neurotrophic factors to support cell survival, differentiation, and axonal guidance23,24 with the ultimate goal of creating a biological bridge that reconnects disrupted spinal pathways.
Within this multidisciplinary context, the European-funded project (FET Open of Horizon Europe Program 2020) “Regeneration of injured spinal cord by electro pulsed bio-hybrid approach” (RISEUP) proposes an innovative strategy combining stem cell therapy with targeted electrical stimulation through an Electro Pulsed Bio-hybrid (EPB) device. The EPB presents an applicator that delivers microsecond pulsed electric fields (µsPEFs) through an array of interdigitated electrodes embedded in a biocompatible scaffold composed of a polylactic acid (PLA) substrate and microfibers. These µsPEFs aim to promote stem cell proliferation and differentiation by modulating membrane permeability and calcium signaling, thereby facilitating bridge formation across the lesion.25–27 Although in vitro studies have demonstrated the biological effects of this stimulation,28–30 translating these findings in vivo requires careful dosimetric evaluation. Numerical modeling of E-field distributions in realistic rat anatomical models provides a crucial tool to ensure that optimal stimulation parameters are still achieved in the SCI environment, without adverse effects for the rats.
This study presents a detailed digital twin dosimetric model that enables a prospective evaluation of the electric stimulation delivered by the EPB applicator in a spinal cord-injured rat (SCI-rat). The model replicates the surgical implantation procedure and stimulation protocol that will be applied in vivo within the RISEUP project, and it allows to assess whether the E-field intensities shown in vitro28–33 to be able to manipulate cells through electroporation can be reached in vivo, within the complex and evolving environment of the injured spinal cord.
Models and Methods
The EPB applicator design and model
The EPB applicator designed within the RISEUP project and used in this study integrates bioengineering and electrical stimulation principles to promote stem cell proliferation and differentiation. The device consists of an interdigitated array of planar gold electrodes, alternating active and ground tracks, embedded in a PLA substrate, as shown in Figure 1a. Its virtual model was implemented in Sim4Life (ZMT Zurich MedTech AG, v8.2) and presented in Figure 1b, using simple Computer-Aided Design (CAD) primitives to define the electrode layout and dimensions. A PLA microfibril layer (Fig. 1c), composed of closely packed cylindrical microfibrils, overlays the electrodes. This layer has the role of supporting cell adhesion and axonal guidance. Its presence still enables effective electric field values to be reached at the cellular level, as demonstrated in previous study. 34
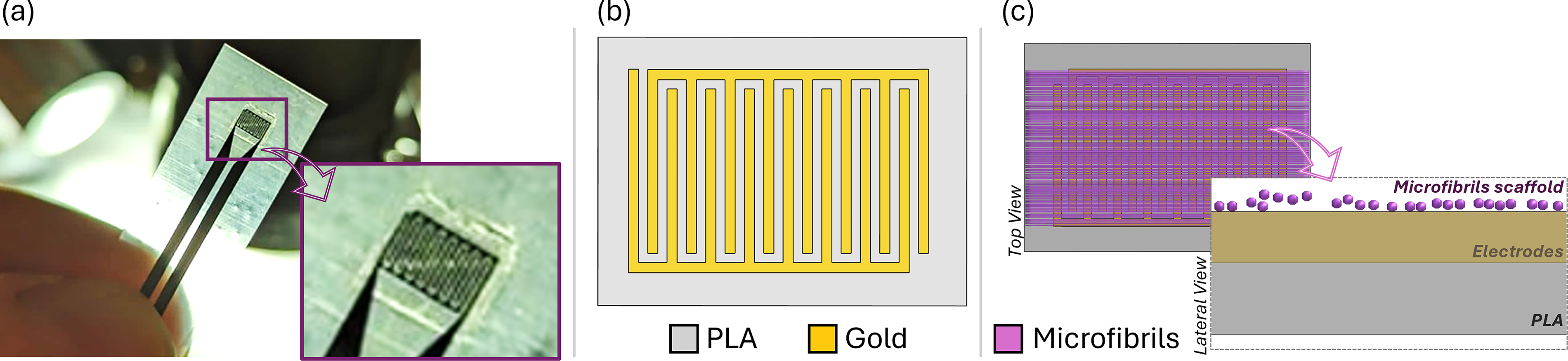
Picture of the produced EPB without connections
Numerical reproduction of the in vivo experiments
To mimic the experimental setup to be used in vivo, a 3D anatomical model of a rat was selected and modified to reflect the post-injury surgical condition.
Among the existing ViZOO models, the Neurorat (v4.0, IT’IS Foundation), in Figure 2a, with a weight of 150 g and a length without tail of 15 cm, was selected as the best representation of the Nude rats used experimentally (250 g, 20 cm). It counts 179 structures segmented from MRI and CT scans, providing high-resolution anatomical detail, 35 including nerve trajectories, necessary for the neurofunctionalized study. Since the Neurorat model represents a healthy animal, manipulations had to be applied to faithfully reproduce the surgical procedure carried out within the RISEUP in vivo experiments (i.e., T8 laminectomy, SCI induction, and EPB implantation).

Numerical reproduction of the laminectomy.
Laminectomy is a surgical technique involving the removal of the lamina, the posterior bony arch of a vertebra, to gain direct access to the spinal cord.36–38 As illustrated in Figure 2, the virtual laminectomy was digitally reproduced on the Neurorat model by removing the lamina of the targeted vertebrae (T8), using 3D editing tools applied to both cortical and cancellous bone. To preserve anatomical consistency, adjacent structures such as the dura mater and cerebrospinal fluid were also modified to reflect the post-laminectomy configuration. The final configuration, shown in Figure 2c, reveals the exposed spinal cord following virtual bone resection, mirroring the experimental surgical access used for EPB implantation. Then, to realistically reproduce the injured rat, a lesion model was developed and integrated into the 3D rat anatomy. The lesion model was generated by starting from a simplified ellipsoidal mesh (Fig. 3a), which was progressively morphed to match the shape observed in confocal microscopy images (Fig. 3b). Its dimensions were then adjusted to reflect the average lesion volume (0.89 ± 0.6 mm³) obtained from nine rats, ensuring both anatomical plausibility and volumetric consistency, and results in approximately 1.86 mm in length, 0.96 mm in width, and 0.95 mm in depth. The resulting 3D lesion, refined for topological accuracy and exported in STereoLithography (STL) format, was embedded at the T8 level in the spinal cord model, completing the SCI-rat representation (Fig. 3c).
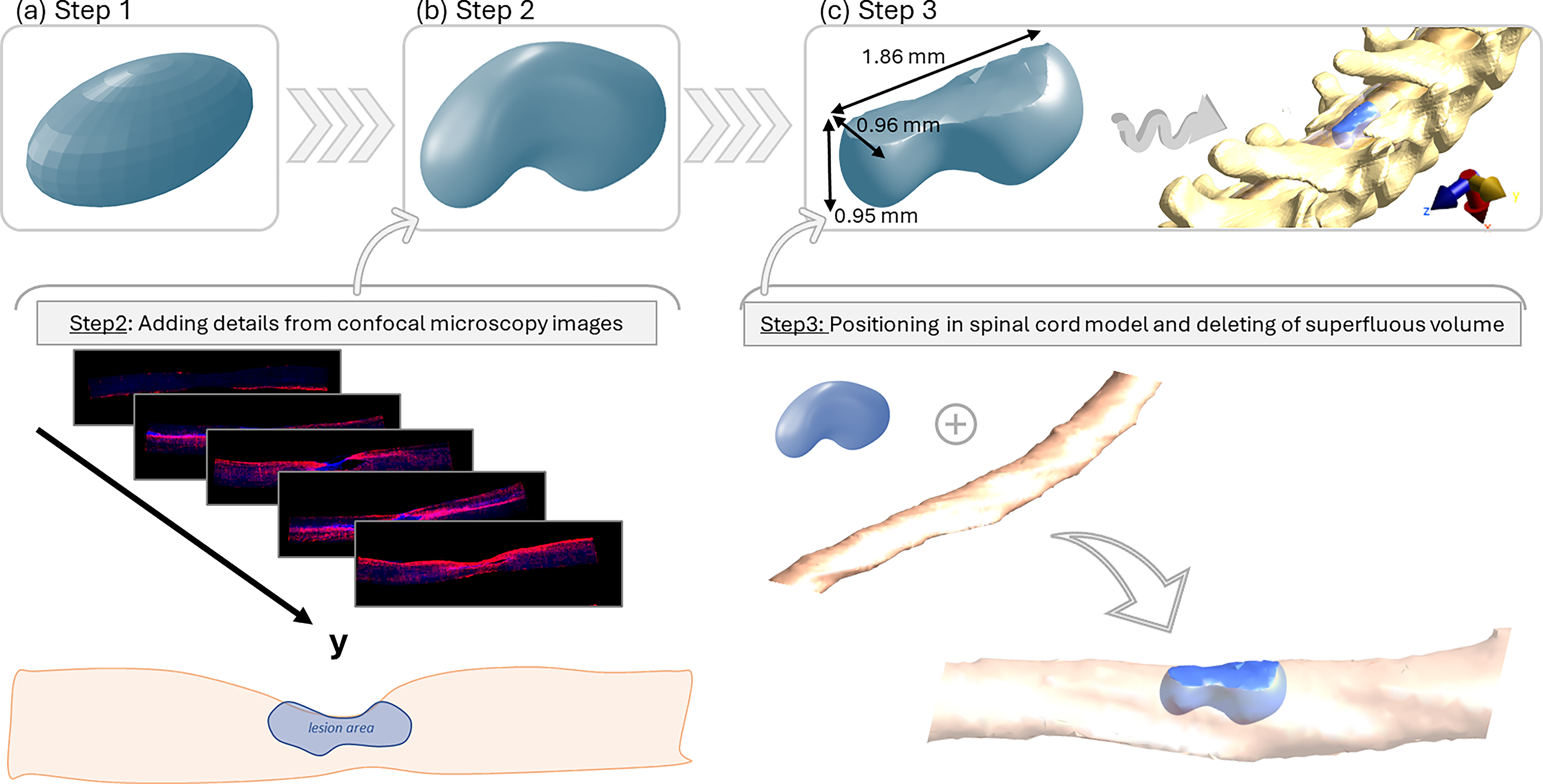
Workflow for realistic spinal cord lesion reconstruction.
Finally, the EPB applicator was placed within the completed SCI-rat model, as illustrated in Figure 4 from different perspectives, directly over the injured region, following the implantation procedure that will be used in the in vivo experiments. This configuration resulted in a complete SCI-rat model with the implanted EPB, serving as the simulation domain for the electric field evaluation.
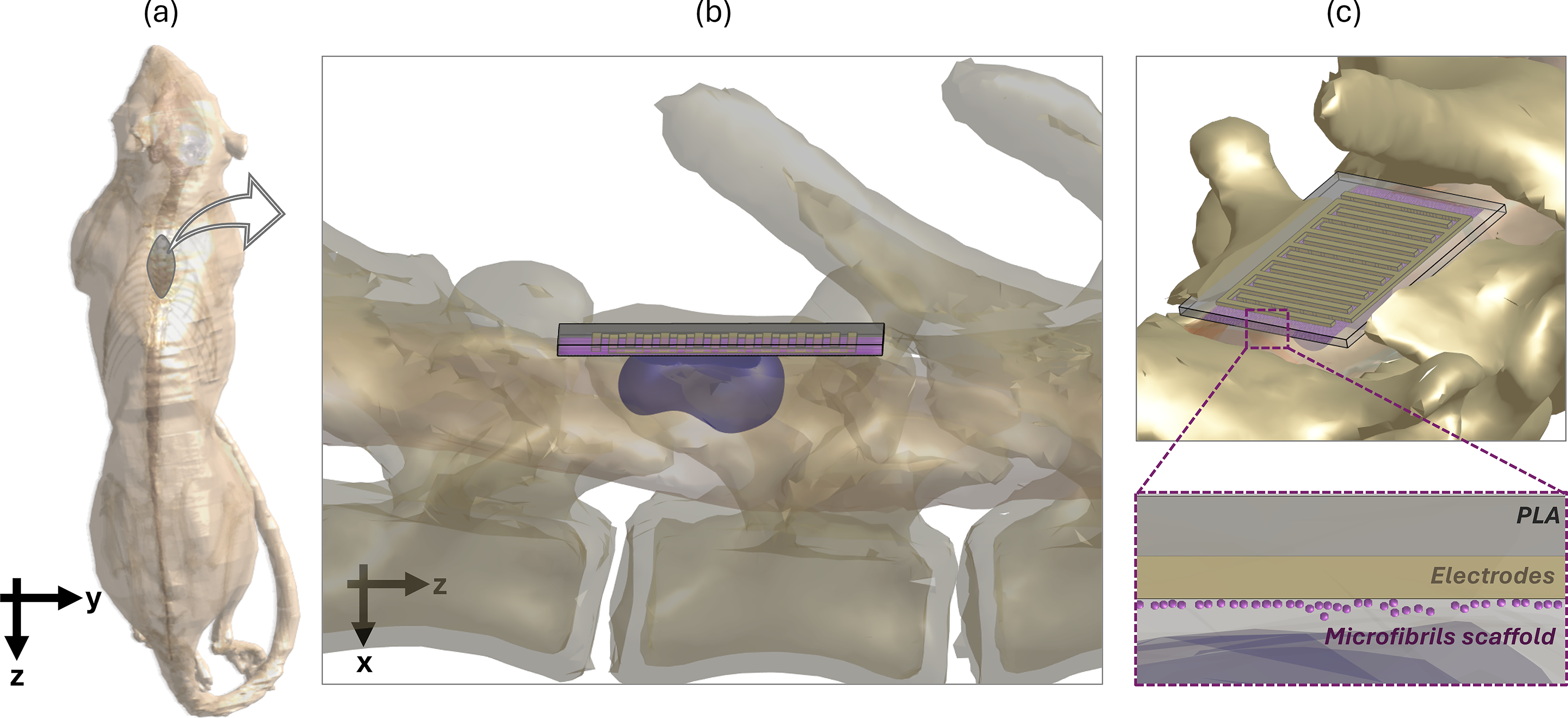
Numerical reproduction of the in vivo experiments.
Stimulation protocol and electromagnetic simulation setup
Within the RISEUP project, a µsPEFs stimulation protocol was designed to target the stem cells implanted with the EPB at the site of SCI, with the aim of inducing sequential biological effects that would promote tissue regeneration, in line with previous in vitro stem cells studies.27–33 Bipolar square-wave pulses of equal amplitude (10 V) but different durations were sequentially applied over time. Specifically, within 5 days postinjury, the implanted stem cells were stimulated with short pulses (25 µs + 25 µs, one per minute for 30 min) to promote their proliferation, at this stage the lesion is at its acute phase, typically characterized by residual spinal cord tissue mixed with blood. Whereas 5–10 days post-injury, the same cells are stimulated with longer pulses (750 µs + 750 µs, single pulse) to promote their differentiation. At this stage, the lesion is in its chronic phase, marked by edema and altered tissue composition.
To estimate numerically the E-field induced inside the rat under such experimental protocol, the Ohmic Quasi-static Solver implemented in Sim4Life was employed, assigning to the healthy tissues the dielectric properties taken from the IT’IS Low-Frequency Database at 1 Hz. 39 In the lesion region, despite the underlying microscopic heterogeneity due to edema, macrophages, and other immune cells, the tissue was modeled as homogeneous and isotropic.40–45 To capture the evolving nature of SCI, two simulations were performed to represent the acute and chronic post-injury phases. 46 In the acute phase, the laminectomy site (e.g., the SCI-surrounding area) was assumed to be filled with blood, and the lesion conductivity was set to 0.45 S/m, representing an average between blood and spinal cord tissue. 39 In the chronic phase, to mimic scarred tissue resulting from edema and residual blood, both the conductivity of lesion and SCI-surrounding area were increased to 1.18 S/m.39,47 The dielectric properties of conductivity values used for each tissue in each simulation are listed in Table 1.
Summary of the Tissue Conductivity Values for the Biological Tissues Considered

A graded voxel mesh was adopted, with a minimum resolution of 5 µm in the region surrounding the EPB to ensure high spatial accuracy, and a coarser mesh (up to 0.5 mm) in peripheral areas of the rat model. This configuration produced a simulation domain comprising 113 million voxels.
This simulation setup enabled accurate dosimetry of the electric field distribution in evolving SCI environments under physiologically relevant stimulation conditions.
Beyond dosimetry, potential off-target effects from the µsPEFs stimulation on the peripheral nervous system was carried out particularly focusing on the left and right intercostal nerves from T7 to T9, as they lie directly beneath the EPB (Fig. 8a). For each nerve, a single fiber is present and was modeled using a cable model of rodents’ motor axons with explicit representation of the node of Ranvier and myelin sheath, implemented ad hoc to reproduce the behavior of the peripheral nerve fibers of rodents, as described by Raspopovic and colleagues, 48 and integrated in Sim4Life. The NEURON solver, embedded in the commercial software, was used to simulate axonal electrophysiology and calculate possible action potentials. A multiphysics coupling was established between the quasi-static electromagnetic simulation and the neuronal model: the spatial distribution of the induced electric field computed by the Quasi-static solver is integrated along the axonal trajectory to extract the potential field, which in turn is used as an external perturbation to the transmembrane potential. This enabled the evaluation of the temporal evolution of membrane potential under the applied stimulation conditions. Simulations were performed setting a fiber diameter of 10 µm48,49 and a resting membrane potential of −78 mV, at physiological temperature (37°C). An external modulating bipolar square-wave pulse is then applied on the potential field to reproduce both the µsPEFs proliferation (pulse duration: 25 μs + 25 μs) and differentiation (pulse duration: 750 μs + 750 μs) protocols and to evaluate whether the applied voltages could elicit action potentials in the considered fibers. An action potential (AP) is considered to occur if the spike characteristics match those reported in previous studies,48,49 in terms of amplitude and duration.
Results from this neurofunctional assessment served to quantify safety margins and evaluate possible activation of peripheral nerves during EPB stimulation.
Results
Electric field distribution in acute and chronic SCI phases
The spatial distribution of E-field induced by the EPB device was evaluated under both acute and chronic SCI conditions.
Figure 5 illustrates the E-field on a sagittal plane intersecting the applicator center for (a) acute and (b) chronic lesion models. Insets highlight a zoomed view around the lesion (white contour). All data are reported in dB, calculated using 30 kV/m as the reference field intensity.
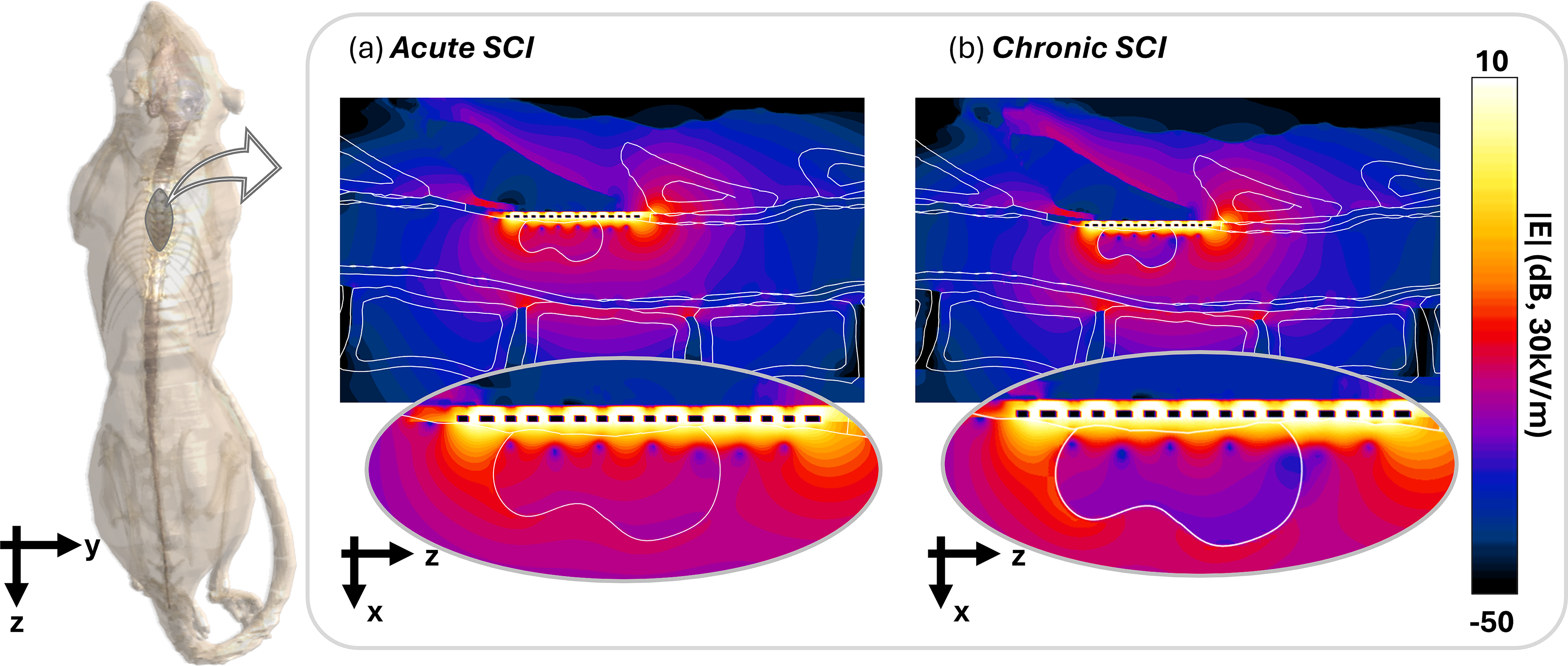
E-field distribution on sagittal views for simulative treatment of spinal cord lesion in
Under both conditions, the E-field is primarily concentrated close to the electrodes, with peak intensities reaching tens of kV/m, and decays toward surrounding tissues, reaching up to −15.6 dB (∼5 kV/m) in the spinal cord. Overall, the presence of the microfibril scaffold alters the field distribution, especially just beneath the EPB in line with previous study. 34 In acute phase (Fig. 5a), tissue discontinuities influence both the shape and intensity of the field. Focusing on the lesion, elevated values (up to 3.5 dB, corresponding to 45 kV/m) are observed near the EPB, gradually decreasing toward deeper regions, where the field drops to around −29.5 dB (1 kV/m), indicating limited penetration into the lesion. In contrast, chronic phase (Fig. 5b) shows a more homogeneous E-field distribution across the lesion. The lesion tissue experiences overall smaller electric field magnitudes compared with the acute case. Although peak values near the EPB are similar, deeper regions reach up to −23.5 dB (2 kV/m), suggesting that increased conductivity due to structural remodeling may enhance field penetration within the lesion.
Moreover, multiple axial planes at increasing depths were analyzed for the acute model (Fig. 6). These planes correspond to three key regions (Fig. 6a):
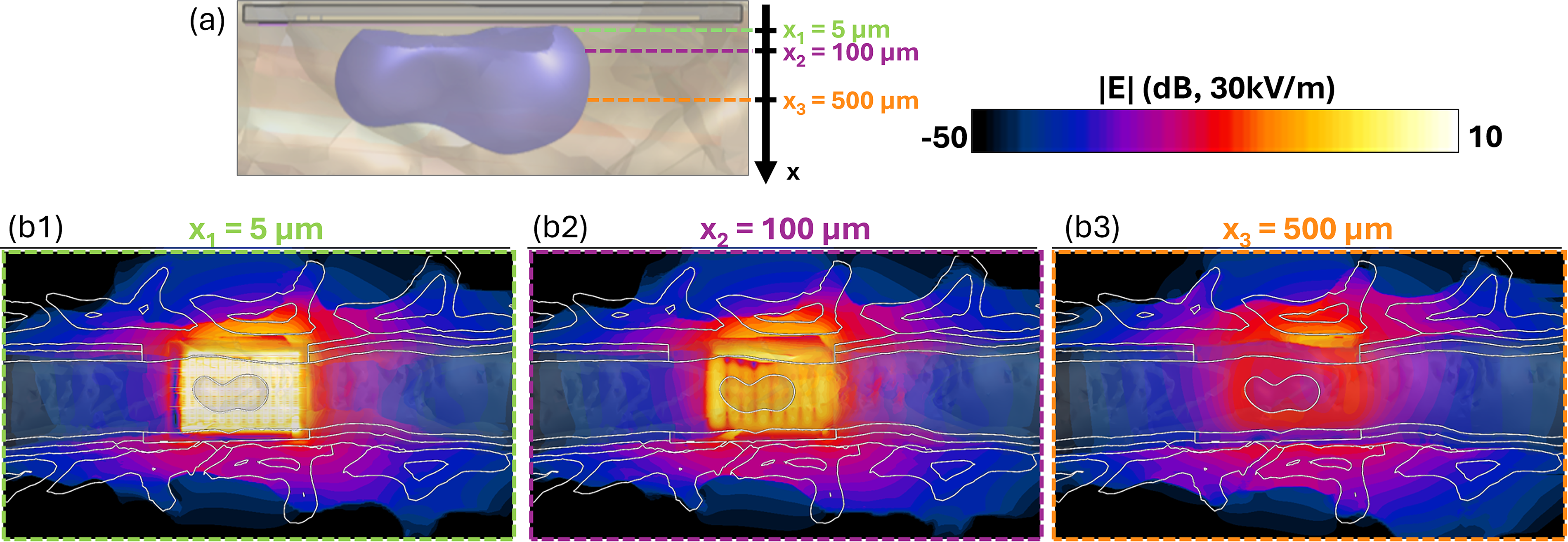
E-field distribution on axial planes views for simulative treatment of spinal cord lesion in acute phase at different quotes (
x1 = 5 µm, directly above the electrodes and representing the site of cells deposition;
x2 = 100 µm, within the first layers of the lesion, where cells may migrates;
x3 = 500 µm, deeper within the injured spinal cord, where cavity is formed.
In Figure 6b1, the highest E-field intensities were observed, ranging between 7.4 dB and −3.5 dB (respectively, 70 kV/m and 20 kV/m), indicating strong localization of the applied field near the EPB. As the depth increases, the field intensity drops significantly, falling below −9.5 dB (10 kV/m) at x2 (Fig. 6b2), and below −29.5 dB (1 kV/m) at x3 (Fig. 6b3). These results highlight the strong spatial confinement of the field. In the chronic lesion model, the field penetration was slightly enhanced, likely due to increased tissue conductivity resulting from chronic remodeling and edema.
To further assess the E-field induced within the lesion, a descriptive comparison of statistical parameters between the two conditions was conducted. The lesion was computationally subdivided into four depth-stratified sub-volumes, depicted in Figure 7a: (i) Cell Volume (0–30 µm, green), (ii) Lesion Volume #1 (30–60 µm, purple), (iii) Lesion Volume #2 (60–100 µm, orange), and (iv) Lesion Volume #3 (100–500 µm, cyan). Electric field values were extracted and postelaborated in Matlab within each sub-volume to generate the boxplots presented in Figure 7b, with median and interquartile range values collected in Table 2. A progressive attenuation of the field is observed across increasing depths. In the Cell Volume, the median |E| exceeds 30 kV/m under acute conditions, while it is slightly lower in the chronic case, though with similar dispersion. Proceeding deeper into the lesion, in sub-volumes #1 and #2, the field magnitude decreases accordingly, showing lower medians and narrower interquartile ranges, with a ∼15% difference in the Cell Volume and ∼12% in the two subsequent layers. In contrast, in sub-volume #3, the deepest region analyzed, the median E-field is higher in the chronic case, resulting in around −36% relative difference. Despite overall low values (<5 kV/m), this inversion highlights increased penetration in chronic conditions.
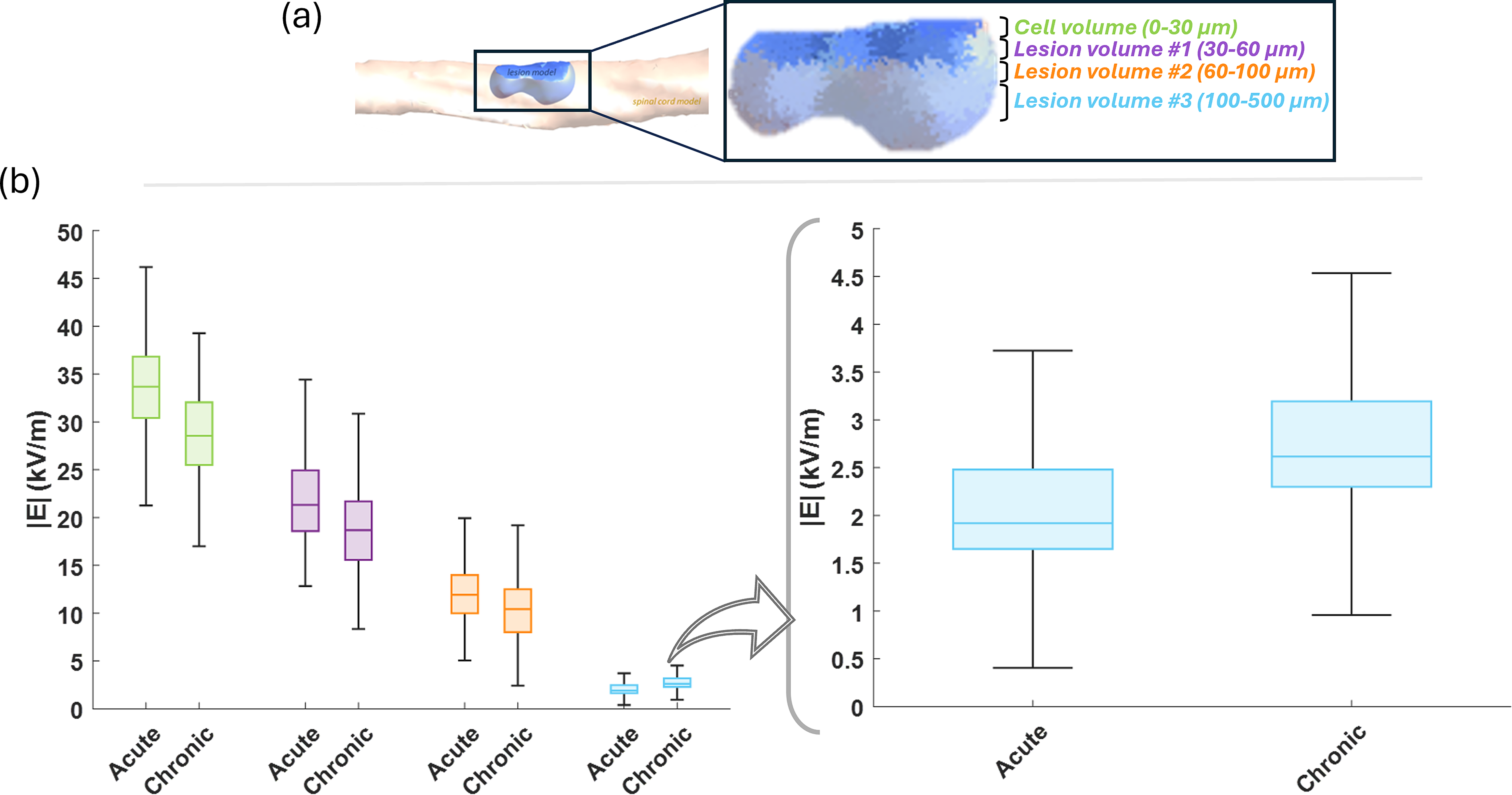
E-field distribution within SCI sub-volumes of increasing height.
Summary of the Effective Electric Field Values (E [kV/m]) Induced by μPEFs Stimulation in Different Volumes of SCI in Acute and Chronic Conditions, Reported as Median, 25th, and 75th Percentiles

Neurofunctional response
Figure 8b displays the electrophysiological responses of the three nerve fiber types to which an AP is elicited by 25 μs + 25 μs proliferation protocol (i.e., T7-left, T7-right, T8-left).
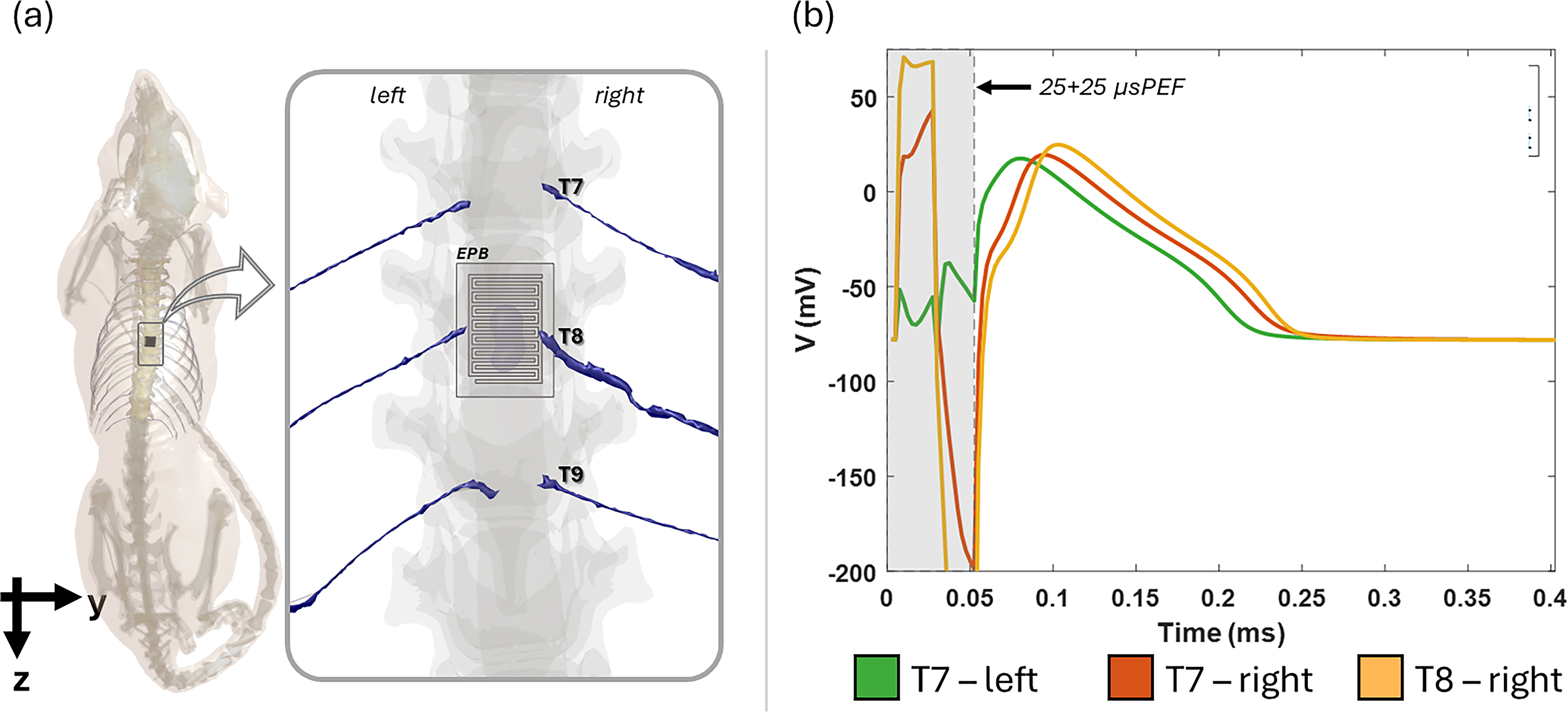
Neuronal response to stimulation.
The data reveal distinct electrophysiological behavior for responding nerve fibers and the elicited response follows the AP shape characteristic of the model.48,49 The AP occurs after stimulation, it has a duration of about 200 μs and reaches an amplitude of 20 mV from the −78 mV at resting state, in line with the 100 mV amplitude observed in previous studies.48,49 When stimulating with the 750 μs + 750 μs pulse, two out of the six fibers showed an action potential peak; however, occurring at the onset of the positive waveform (data not shown).
Discussion
This work presents a comprehensive and biologically grounded dosimetric model developed to estimate the EPB-induced E-field in a SCI-rat. By mirroring the surgical configuration and stimulation parameters that will be employed in the RISEUP in vivo experiments, the model serves as a predictive tool to determine whether electric field strengths previously identified in vitro, and shown to be sufficient to trigger electroporation and influence stem cell dynamics,26–33 can also be achieved in the altered biophysical context such as that of the injured spinal cord. Indeed, the obtained results confirmed that the E-field intensities induced beneath the EPB, where neural stem cells are expected to reside, fall within the range of 20–70 kV/m, matching the values previously demonstrated to be sufficient for transient membrane permeabilization and to promote proliferation and differentiation in vitro.28–30,33 To enhance faithfulness of the model, the temporal evolution of the lesion’s dielectric properties were also taken into account, assessing possible influences in the induced E-field, which consequently would affect stimulation efficacy. As a matter of fact, following SCI, tissue composition changes dynamically due to inflammation, edema, and extracellular matrix remodeling.7,43–45,47 By comparing models representative of the acute and chronic phases of injury, we observed that increased tissue conductivity in the chronic stage results in deeper E-field penetration. While superficial field intensities remain largely unchanged, the elevated conductivity leads to a broader spatial distribution of effective field values within the lesion core, particularly beyond 100 µm from the EPB surface. These findings suggest that the timing of µsPEFs delivery may affect therapeutic outcomes, with chronic conditions potentially enabling more homogeneous stimulation without requiring higher voltage levels.28–30,33,50
Furthermore, to evaluate the spatial selectivity of the EPB stimulation and the potential for off-target neural activation, which is a known side effect in electroporation treatments,51–55 we coupled the dosimetric analysis with neurofunctional modeling of adjacent intercostal nerves. This combined approach enabled us to assess whether the electric fields generated by the EPB could unintentionally excite nearby peripheral fibers. The results showed an incomplete activation, with a limited response of some of the fibers nearby the EPB. It is important to point out that the model used in this study is based on conduction properties of one single representative healthy nerve fiber, nevertheless, under injured conditions not all the fibers may be recruitable, and that SCI may alter the conduction behavior, potentially leading to a reduced sensitivity of affected fibers. 56 This indicates that, overall, the exposure to the EPB can be considered to remain safe. This focality of stimulation is directly attributable to the EPB design, which integrates microfibril-based scaffolds that not only support cell engraftment but also enhance the electric field locally within the superficial lesion layers. 34 By concentrating the field in the target region, the EPB effectively limits unintended spread, ensuring that stimulation is delivered precisely where needed while preserving surrounding healthy tissue. Computational dosimetry has always been considered a fundamental supportive tool during biological experiments, however, it has often been applied in an investigative manner, supported by state-of-the-art experimental results, 57 or retrospectively, after the experiments have been conducted,58,59 to assess exposure conditions. The latter studies have the advantage of immediate validation, as the experimental outcomes are already available, but they often require extensive sensitivity analyses to address uncontrolled variables. In contrast, the dosimetric study presented here was carried out prospectively, prior to the experiment, with the specific goal of informing experimental design and guiding the selection of stimulation parameters. This approach allowed the in vivo study to be conducted in a more controlled and informed manner. This strategy aligns with the concept of digital twins,60–62 rather than digital models, as it provides a subject-specific, biologically grounded virtual replica of the experimental setup that supports predictive planning through a bidirectional exchange between the physical and virtual domains. The forthcoming experimental results will thus be interpreted with the support of a robust dosimetric estimate, providing prior knowledge of the induced E-field levels. This allows the observed biological effects, whether cellular or neurofunctional, to serve not only as a validation of the computational model, but also as a valuable indicator for refining the experimental setup. In particular, discrepancies between predicted field levels and biological outcomes may inform improvements in stimulation delivery and technological assessment. This aspect becomes particularly relevant when considering the potential translation of the EPB to clinical applications in humans, where spinal cord lesions are significantly larger than those modeled in rodents. In such scenarios, the flexibility of the EPB design could offer promising avenues for adaptation, either through geometric enlargement of a single unit or the modular deployment of multiple devices to achieve adequate lesion coverage. Similarly, the same modeling strategy employed here could be extended to human digital twins, offering a useful framework to explore and optimize key design parameters such as electrode geometry and stimulation levels in anatomically realistic conditions.
Conclusion
Lying on the digital twin approach, which integrates anatomically realistic and multiphysics modeling with a faithful replica of experimental in vivo implantation conditions, the present study has enabled a predictive dosimetric analysis of the EPB device. This approach demonstrates that the induced electric field intensities in the spinal cord lesion are sufficient to trigger electroporation and promote neural stem cell activity. The simulations clearly show that effective E-field values are well confined to the lesion area, ensuring both targeted stimulation and minimal off-target effects. Moreover, the results underscore the importance of timing in stimulation protocols and confirm the safety of the proposed stimulation approach. The modeling approach adopted in this study offers a powerful and versatile framework for optimizing stimulation protocols and supporting future translational development of RISEUP technology.
Footnotes
Acknowledgments
The authors thank ZMT Zurich MedTech, AG, for providing licenses for simulation software Sim4Life.
Authors’ Contributions
N.D.: Writing—original draft, data curation and visualization. N.D., M.C., L.M., V.M.M., F.A. and M.L.: Methodology and software. N.D., M.C., P.M., A.P., L.C., S.F., F.A. and M.L.: Formal snalysis. N.D., M.C., V.M.M., F.A. and M.L.: Conceptualization. N.D., M.C., F.A., M.L.: Investigation. M.C., P.M., A.P., L.C., S.F., L.M., V.M.M., C.C., F.A. and M.L.: Writing—review & editing. C.C.: Project administration.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This work has been developed in the framework of and supported by the FET-OPEN RISEUP project funded by the European Union’s Horizon 2020 research and innovation program (grant agreement No. 964562).