
Abstract
Introduction:
Cannabis use has risen disproportionately among middle-aged and older U.S. adults, groups particularly vulnerable to adverse effects, including cannabis use disorder (CUD). Consumption patterns have diversified in recent years. The quantity of cannabis use, historically measured in limited ways (e.g., number of joints), is now considered a key risk factor for CUD. However, age-related differences in consumption patterns and their relationships with CUD remain understudied. This study investigated age-related differences in consumption patterns and examined the relationship between quantity of use—measured by milligrams of THC (mgTHC)—and self-reported CUD in individuals with regular cannabis use.
Materials and Methods:
A total of 4134 U.S. adults (ages 18+; 45.9% male, 54.1% female) who reported daily cannabis use completed an online survey assessing cannabis consumption patterns and self-reported Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition’s CUD criteria. Pearson’s chi-square tests and one-way analysis of variance examined differences in sex, reasons for use, methods of consumption, CUD severity, criteria count, and mgTHC with comparisons across three age-groups (18–49, 50–64, 65+). Regression models, adjusted for sex and reasons for use, analyzed age-specific associations between mgTHC and CUD.
Results:
Overall, over 70% reported using cannabis for both medical and recreational purposes. Middle-aged adults were more likely to report medical use than younger ones (18.1% vs. 13.7%; p < 0.001) and older adults (14.1%; p = 0.027). Older adults were more likely to report recreational-only use compared with middle-aged adults (15.8% vs. 10.5%; p = 0.002). Smoking buds was the most common consumption method across age-groups, while high-potency concentrate use declined with age. In the overall sample, daily mgTHC was associated with CUD severity, and middle-aged and older adults endorsed fewer CUD criteria than younger adults at all levels of mgTHC; however, age effects were not statistically significant.
Discussion:
Among daily cannabis consumers, middle-aged and older adults differed from younger consumers in methods of consumption and reasons for use. While both groups consumed lower quantities than their younger counterparts, no age-related differences were observed in the relationship between mgTHC consumption and CUD, contrasting with evidence suggesting that older cannabis consumers may be more vulnerable to cannabis-related negative outcomes.
Introduction
In recent decades, cannabis use has increased among U.S. adults, with the most notable relative rise among middle-aged (50–64 years) and older adults (≥65 years).1–5 Historically, concerns about cannabis-related harms focused on adolescents and young adults,6–9 leaving middle-aged and older adults among the least studied populations of cannabis consumers. However, older adults have heightened biological vulnerability to adverse cannabinoid effects due to several physiological factors—age-related reductions in brain volume, neuron count, and neurotransmitter sensitivity, which amplify drug effects. The lipophilic nature of cannabinoids increases their accumulation in older individuals because of greater adipose tissue, less lean body mass and water content, a larger volume of distribution, and age-related declines in hepatic blood flow, delaying elimination and increasing the risk of adverse effects.10–12 Accordingly, middle-aged and older adults are particularly vulnerable to cannabis-related harms, 13 including falls, 14 physical 5 and cognitive decline,15–17 and injuries leading to emergency department visits. 18 With expanding legalization, cannabis consumption patterns have become increasingly diverse, varying in quantity and frequency of use, product potency, methods of administration, product types, and reasons for use (medical vs. recreational).19–22 Understanding these patterns in middle-aged and older adults is critical for assessing age-specific risks and informing harm reduction strategies. To date, only a few studies have focused on these populations,22–25 offering an initial step toward identifying differences in motivations for use and consumption patterns between middle-aged adults, older adults, and younger age-groups. However, these studies remain limited in scope, hindering efforts to accurately assess risk and develop effective, age-tailored harm reduction approaches.
One key risk of cannabis consumption is cannabis use disorder (CUD), a condition marked by a persistent and problematic pattern of use that disrupts social and occupational functioning. 26 CUD occurs in 20–33% of individuals with cannabis use27,28 and has increased among the U.S. adult population,29,30 as well as among patients in various clinical settings, including middle-aged and older adults. Studies have identified several patterns of use that increase the risk of CUD, including the frequency and quantity of cannabis use, as well as the potency of products consumed. These risks appear to be heightened among older age-groups.31–34 However, a limitation in current research is the lack of standardized measures to capture the diverse methods of cannabis consumption and quantify use accurately. This gap in measurement may contribute to the limited understanding of cannabis use patterns among older adults and their associated risk of CUD.
We recently developed a self-report method to calculate the daily milligram consumption of delta-9-tetrahydrocannabinol (mgTHC), the primary psychoactive compound in cannabis products that produces negative effects, for use in surveys.35–37 This approach uses detailed items on cannabis use patterns, including the amount and potency of cannabis products consumed, and converts this information into daily mgTHC.35,37 Recent analyses showed that greater mgTHC was associated with greater risk of self-reported CUD across all severity levels, as well as greater mean increases in CUD criteria count among daily cannabis consumers. 38 These findings support the use of mgTHC as a valid measure for quantifying cannabis use and estimating associated risks of CUD. Utilizing a precise measure such as mgTHC, which encompasses key factors related to cannabis consumption, could also offer important insights into age-related differences in vulnerability-associated risks. While preliminary findings suggested potential age-related differences in both mgTHC consumption and CUD criteria counts, interpretation was limited by categorization constraints, and age-related moderation was not incorporated in assessing the associations between mgTHC and CUD variables. 38 Consequently, there is a need for a more detailed examination of age-related differences in mgTHC consumption and its relationship with CUD.
We analyzed a subset of U.S. adults who report daily cannabis use, drawn from a larger survey of adults with cannabis use, distributed via social media, that has been used in prior studies addressing different research questions.24,35,39,40 The study had two primary objectives as follows: (1) To compare cannabis consumption patterns among middle-aged and older adults with daily cannabis use, as well as with younger adults with cannabis use; and (2) to examine age-related differences in the relationship between mgTHC consumption and self-reported CUD. We hypothesized that age-related differences in cannabis consumption patterns would reflect findings from the limited existing literature—namely, that older adults tend to use cannabis in less risky ways and more often for medical purposes. 24 Furthermore, although studies using mgTHC remain exploratory given the recent development of this metric, prior research suggests that older adults may be more vulnerable than younger individuals to developing CUD and other adverse outcomes.31–34 Accordingly, we hypothesized that middle-aged and older adults would exhibit stronger associations between mgTHC intake and self-reported CUD.
Materials and Methods
Sample
Residents of the 50 U.S. states and the District of Columbia, aged 18 years or older, were recruited between February and April 2022 for an anonymous online survey on cannabis behaviors. Recruitment used keyword-targeted advertisements on Meta, 41 with no compensation offered to minimize the risk of bot participation. 42 The study procedures received approval from the Dartmouth Committee for the Protection of Human Subjects. Individuals who clicked on the advertisement were directed to a consent page for the study. Those who consented answered eligibility questions to confirm they were at least 18 years old, reported any use within the 7 days preceding survey completion, and passed bot and attention checks before proceeding to the main survey. The survey gathered information on sociodemographic factors, cannabis use behaviors, mgTHC consumption, and CUD.
Of the 8284 adult respondents, 540 were deemed ineligible due to lack of consent (n = 20), being younger than 18 (n = 19), exiting before reaching the survey (n = 383), or failing bot or attention checks (n = 118). Specifically, participants were excluded if they failed both of two attention checks or were flagged for bot-like behavior. The attention checks included a simple multiplication question; to account for potential mis-clicks, participants who answered incorrectly were given a second attempt before being excluded. Bot detection combined automated and manual methods, including Qualtrics’ reCAPTCHA and RelevantID tools as well as manual screening for suspicious email addresses and responses to a hidden item visible only to automated scripts. Additional logic checks were applied to detect inconsistencies—for example, reporting cannabis use on more days in the past 7 days than in the past 30 days.
Measures
CUD items
CUD within the past year was evaluated using 16 yes/no items adapted from the National Survey on Drug Use and Health (NSDUH) and the Alcohol Use Disorder and Associated Disabilities Interview Schedule-5. These items assessed the 11 Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition’s (DSM-5) diagnostic criteria for CUD, which previous studies have shown to have reliable and valid measures.43–46 Two self-reported CUD outcomes were derived from the responses as follows: (1) The total count of criteria endorsed (range 0–11) and (2) DSM-5 CUD severity levels, categorized as None (0–1 criteria), Mild (2–3 criteria), Moderate (4–5 criteria), and Severe (6+ criteria).
Cannabis consumption patterns
As described previously, items to measure cannabis consumption were adapted from an established cannabis assessment.35–38 Consumption items covered use during the prior 7 days.
Method of administration
Methods of administration included smoking flower buds, vaping flower buds, vaping concentrates, dabbing concentrates, consuming edibles, and “other” (e.g., tinctures, capsules, or pills).
Quantity items and mgTHC calculations
Participants were initially asked if their daily cannabis consumption was consistent over the prior 7 days. Those with consistent use were routed to questions about their typical daily quantity for each product by time of day. Those with varying consumption were routed to questions about their quantity for each of the prior 7 days. Response options included various units as follows: flower in hits, grams, or joints; concentrates in hits or grams; edibles in mgTHC; capsules in number of capsules and mgTHC per capsule; and THC liquids or tinctures in drops or milliliters. Participants also estimated the THC potency for flower and concentrate products. Additional details about survey items are available in prior studies.35–40 Daily mgTHC values were calculated by summing the THC content across all cannabis products consumed using an algorithm developed in previous research.35,37
Reasons for cannabis use
Participants were asked about their primary reason for using cannabis. Responses included medical use only, recreational use only, or both.
MgTHC per day
Daily mgTHC estimates were derived by calculating the total THC consumed from all reported cannabis products, using information on quantity, potency, and route of administration. For those reporting in grams, the calculation involved multiplying the amount used by the product’s THC concentration, a unit conversion factor (1000 mg/g), and an adjustment for method of administration efficiency constant that accounts for THC loss due to the administration method. For participants reporting consumption in “hits,” an additional grams-per-hit conversion was applied. Efficiency values for each administration method were informed by prior literature.47–51 If participants did not indicate a typical daily quantity, daily averages were estimated from their total reported use over the past week. In cases where product-method responses were incomplete, missing values were imputed using the MICE package in R, incorporating data such as age, sex, race, reasons for use, and other cannabis use characteristics. To address implausibly high values, daily THC totals were capped at 1000 mg based on expert recommendations and recent evidence.36,38,52
Statistical analysis
Descriptive statistics were calculated to provide information on sex, age-groups (18–49 years, 50–64 years, 65+ years), cannabis consumption patterns, CUD severity and criteria count, and mean daily mgTHC. Pearson’s chi-square tests and one-way analysis of variance were used to conduct pairwise comparisons of frequencies and mean CUD criteria count between the three age-groups. To examine age-specific associations of mgTHC (exposure variable) with self-reported CUD criteria count (outcome variable), linear regression was fit with log-transformed mgTHC as a continuous predictor, age-group category, and the interaction of age with log mgTHC, adjusted for sex and medical/recreational cannabis use. To examine for potential nonlinear associations in the relationship between mgTHC and self-reported CUD criteria count, sensitivity analyses utilized the categorical mgTHC variable divided into bins (e.g., 10 mg or 50 mg increments). Predicted mean criteria count for self-reported CUD was plotted to visualize the findings. All analyses were conducted in R (version 4.2.2). 53 To address some unusually high daily mgTHC values that appeared biologically implausible and therefore erroneous, daily THC consumption values were winsorized at 1000 mgTHC, consistent with prior work. 38
Results
Age and sex
The mean age of the sample was 47.75 years (standard deviation [SD] = 14.5). Within the overall sample, 51.6% (n = 2135) were ages 18–49, 35.3% (n = 1461) were ages 50–64, and 13.0% (n = 538) were 65 or older. Overall, 54% of participants were female, with the proportion of women decreasing across age-groups (18–49: 58.3%; 50–64: 53.1%; 65+: 40.8%).
Methods of cannabis consumption and quantity of THC consumed
Across all age-groups, smoking flower buds was the most common method of consumption (18–49: 89.4%; 50–64: 90.1%; 65+: 87.0%), followed by vaping concentrates and consuming edibles. Concentrate use, including both vaping and dabbing, was more prevalent among younger adults and declined with increasing age-groups. The mean daily mgTHC consumption differed significantly by age. For the overall sample, the mean was 210.79 mgTHC per day (standard error [SE] = 255.01). Specifically, the mean was 239.83 mgTHC (SE = 268.17) for participants aged 18–49, 197.90 mgTHC (SE = 248.58) for those aged 50–64, and 130.51 mgTHC (SE = 190.89) for participants aged 65 or older (Table 1, Fig. 1).
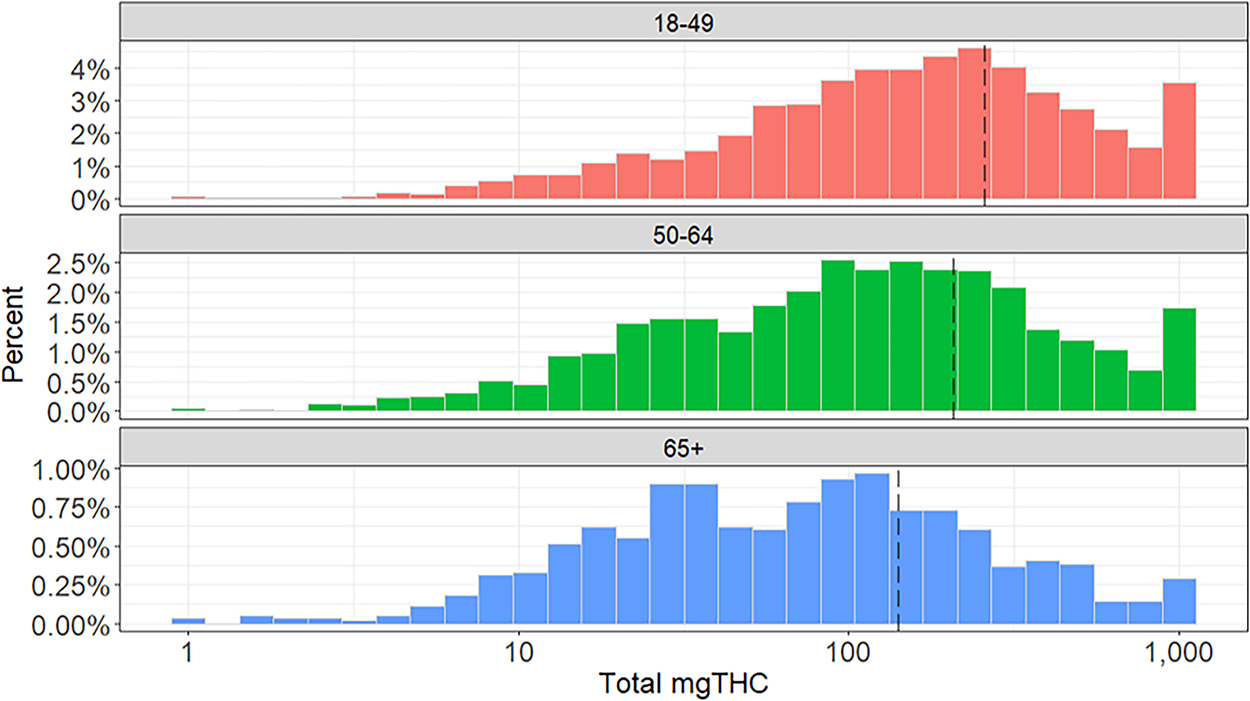
Distribution of estimated total mgTHC consumption among daily users, by age-group. mgTHC, milligram of delta-9-tetrahydrocannabinol.
Sample Demographics, Self-Reported Cannabis Consumption Patterns, mgTHC, and Cannabis Use Disorder, Overall and by Age-Groups
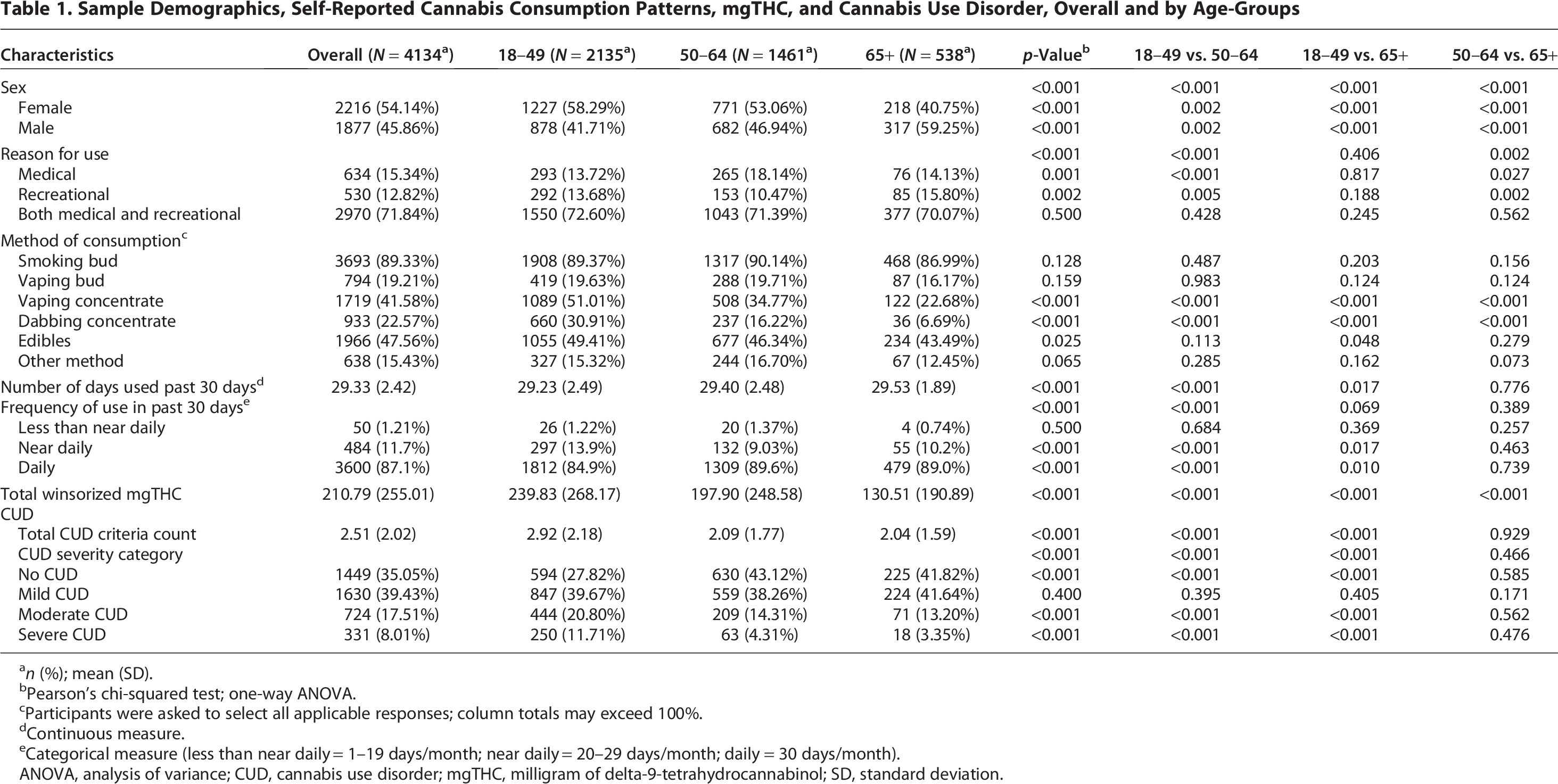
n (%); mean (SD).
Pearson’s chi-squared test; one-way ANOVA.
Participants were asked to select all applicable responses; column totals may exceed 100%.
Continuous measure.
Categorical measure (less than near daily = 1–19 days/month; near daily = 20–29 days/month; daily = 30 days/month).
ANOVA, analysis of variance; CUD, cannabis use disorder; mgTHC, milligram of delta-9-tetrahydrocannabinol; SD, standard deviation.
Cannabis use disorder
Approximately 65% of participants in the sample met the diagnostic criteria for CUD, reporting an average of 2.51 (SD = 2.02) CUD criteria. The total number of CUD criteria decreased with increasing age-groups: 18–49 years (2.92, SD = 2.18), 50–64 years (2.09, SD = 1.77), and 65+ years (2.04, SD = 1.59; p < 0.001). In the overall sample, approximately 35% did not meet the criteria for CUD (0–1 criteria), while 39.4% had mild CUD (2–3 criteria), 17.5% had moderate CUD (4–5 criteria), and 8% had severe CUD (6+ criteria). Middle-aged and older adults were less likely than younger adults to meet the criteria for moderate CUD (18–49: 20.8%; 50–64: 14.3%; 65+: 13.2%; p < 0.001) or severe CUD (18–49: 11.7%; 50–64: 4.3%; 65+: 3.4%; p < 0.001). No significant differences were observed in CUD diagnosis (across severity levels) or total CUD count between middle-aged and older adults.
Reasons for cannabis use
In the overall sample and within each age-group, most participants reported using cannabis for both medical and recreational purposes (overall: 71.8%; 18–49: 72.6%; 50–64: 71.4%; 65+: 70.1%; p = 0.5). Middle-aged adults were significantly more likely to report using cannabis for medical-only purposes compared with other age-groups. Adults from younger age-groups were significantly more likely to report using cannabis for recreational-only purposes compared with middle-aged adults; however, differences were relatively minor. Approximately 16% of older adults reported recreational-only use, which was significantly higher than the rate among middle-aged adults (10.5%) but not significantly different from that of younger age-groups.
Daily mgTHC and associations with CUD
In the overall sample, daily mgTHC was positively associated with the mean self-reported CUD criteria count (β = 0.21, 95% confidence interval [0.15, 0.28], p < 0.001) (Table 2). On average, participants aged 50–64 and ≥65 endorsed fewer CUD criteria at all levels of daily mgTHC consumption compared with those aged 18–49. However, these differences were not statistically significant (Table 2, Fig. 2). Sensitivity analysis exploring the nonlinear relationship between mgTHC and CUD criteria count did not find any additional differences between age-groups 50–64 and 65+ (Supplementary Fig. S1).
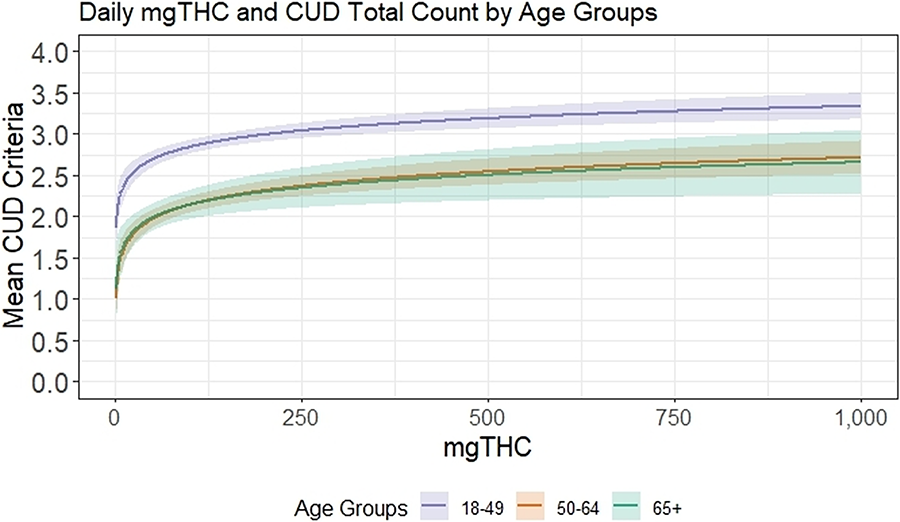
Relationship between daily mgTHC and mean CUD criteria count, by age-groups. CUD, cannabis use disorder.
Association Between mgTHC and Self-Reported Cannabis Use Disorder Count with Age-Group Interaction
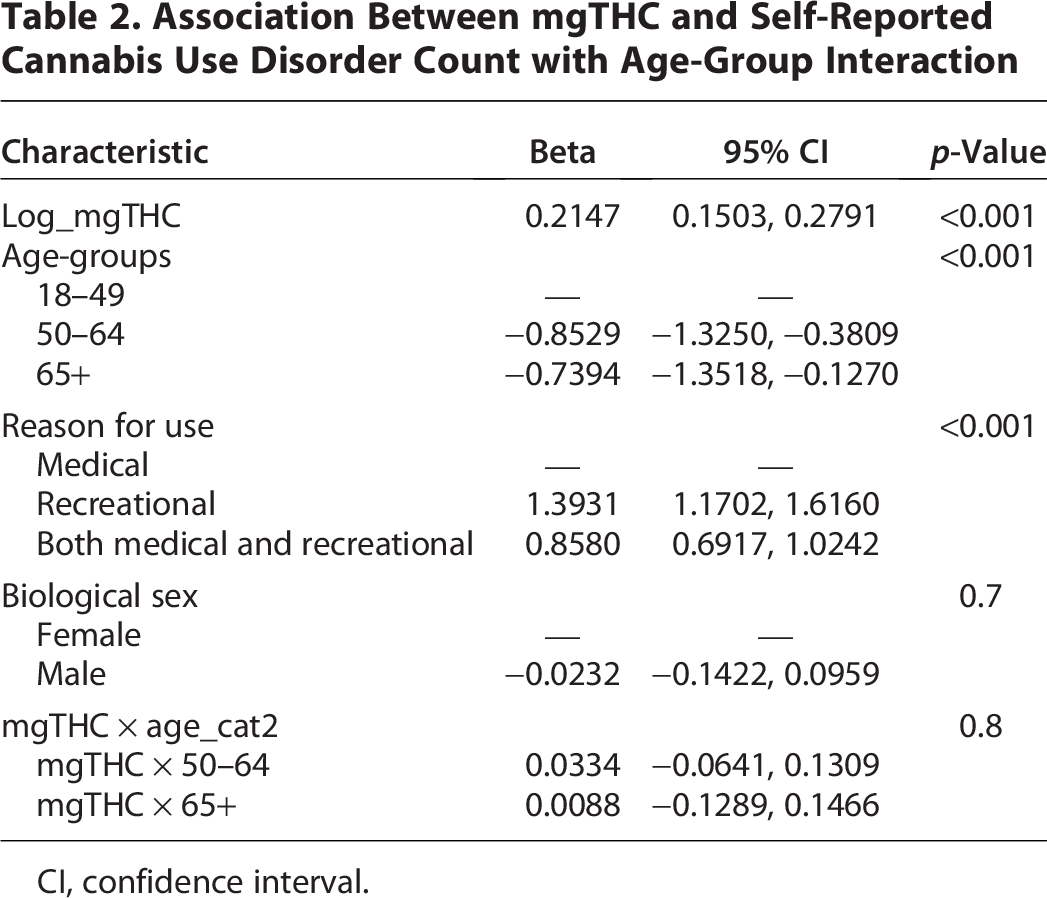
CI, confidence interval.
Discussion
In an online sample of adults with daily cannabis use, middle-aged and older adults differed from younger adults—and from each other—in several consumption patterns. Their daily mgTHC intake was generally lower than that of younger users, yet no significant age differences were observed in the relationship between mgTHC consumption and CUD outcomes. These findings contribute to the limited literature on age-related differences in cannabis use patterns and represent an important first step in evaluating the applicability of our recently developed mgTHC measurement procedure35,37,38 across demographic subgroups. While the lack of observed age effects on the mgTHC-CUD relationship may stem from methodological limitations, such as a ceiling effect from restricting the analysis to individuals with daily use, 38 it challenges existing hypotheses and warrants further investigation.
Although studies have explored reasons for cannabis use, including medical use,54–61 there are limited data on how these reasons vary across the adult lifespan. 62 Medical cannabis use has risen in recent years, driven by increasing beliefs in its therapeutic potential.63,64 Prior studies suggest that middle-aged and older adults are more inclined to use cannabis for medical purposes, such as managing pain, insomnia, or other conditions,23,65 rather than for recreational reasons such as enjoyment or social activities, which were more commonly reported by younger individuals. 23 However, our findings showed that across all age-groups, over 70% of respondents reported using cannabis for both medical and recreational purposes. Furthermore, while middle-aged adults were slightly more likely than younger adults to report medical use, no significant differences were observed between older adults and younger age-groups, in contrast to previous research. Notably, although differences in recreational-only cannabis use across age-groups were small, older adults were more likely to report it compared with middle-aged adults. However, given that the sample consisted of individuals with daily use recruited online, they may not fully represent the broader population of older cannabis consumers. Additional inquiry is needed into the interaction effects between reasons for cannabis use and other consumption patterns among middle-aged and older adults to better characterize their use.
While age differences were observed in only some cannabis consumption patterns, it is noteworthy that smoking and consuming edible products were the most common methods of cannabis use among middle-aged and older adults in this sample. This aligns with previous studies,22,23,25 including a recent study with similarly recruited samples. 24 Unlike prior research, however, this sample included adults with heavy cannabis use, with all participants reporting daily cannabis use and over 60% reporting CUD. Notably, the similarity in consumption patterns between heavy and less heavy users from previous reports suggests that middle-aged and older adults primarily consume cannabis through smoking or edibles, regardless of the intensity of their use. This may reflect the tendency of middle-aged and older adults to maintain long-standing cannabis use habits established earlier in life. Middle-aged and older adults were significantly less likely than younger adults to use vaping or dabbing as methods of cannabis consumption. However, vaping concentrates were still relatively common among adults aged 50–64 (34.7%) and those aged 65 and older (22.7%), aligning with findings from our previous research, 24 and exceeding the rates reported in several earlier studies.66–68 Given that concentrates are among the fastest growing categories of cannabis products and are known for their high potency and rapid effects, their use could pose particular risks for older adults, as such strong and immediate effects may have potentially harmful consequences in this population.
Our analysis of age-related differences in mgTHC intake and its association with CUD builds on our efforts to develop an algorithm that integrates various cannabis use components into a single indicator of THC quantity consumed per day of use. This approach addresses limitations of prior research, which primarily relied on the number of joints as a proxy for cannabis quantity. We found that cannabis mgTHC intake among middle-aged and older adults was consistently lower than in younger age-groups, with a steady decline with increasing age. However, the lack of an observed age effect on the associations between mgTHC and CUD contrasts with prior findings that suggest greater vulnerability to cannabis-related harms with advancing age.13,16,69,70 Notably, those studies focused on other negative outcomes rather than CUD, making this, to our knowledge, the first study to compare age-based associations between cannabis quantity and CUD in adults with heavy use. While there is a biological basis for the increased susceptibility of older age-groups to developing CUD—alongside societal and psychological factors such as social exclusion, isolation, deteriorating physical and mental health, and accumulating negative life events 71 —this relationship requires further investigation. Future studies should address the limitations of the current study, particularly its focus on individuals with heavy cannabis use, among whom age-related effects on the associations examined may be less pronounced. The current study did not include direct comparisons between associations of mgTHC and CUD versus those based on commonly used proxies of cannabis use (e.g., number of joints), limiting the ability to evaluate the added utility of more comprehensive dose-based metrics over conventional measures. Our ongoing research is examining how different exposure metrics relate to clinical outcomes to address this important question.
The study has limitations. Data were drawn from an online convenience sample of cannabis consumers, limiting generalizability. Self-reported survey data may be subject to measurement errors, such as recall bias, which could affect the accuracy of mgTHC calculations. This limitation is especially relevant given the considerable variability in actual THC doses, even among products with similar labels. Measurement errors may also impact the reporting of other cannabis use patterns (e.g., methods of consumption). While assessing recent use (past 7 days) is likely less vulnerable to recall bias than longer reporting periods, this shorter time frame may not fully capture participants’ typical use patterns, which might be better reflected in longer intervals (e.g., past 30 days). However, in our prior investigations, we found that for daily users, past-week cannabis use is highly likely to reflect their typical pattern over longer periods. 35 CUD symptoms in this study were self-reported, which may introduce bias—particularly among older adults who primarily reported medical use and may not perceive their cannabis use as problematic. Although prior research has shown strong agreement between self-reported and clinician-assessed CUD, 72 and although we used well-validated items from the NSDUH, the reliance on self-report remains a limitation and should be considered when interpreting the findings. The current study primarily included White participants and daily cannabis consumers, limiting the ability to generalize findings to individuals with less frequent use or individuals from more diverse backgrounds. In addition, the study did not inquire about specific health conditions for which respondents used cannabis or assess health correlates. Finally, although the grouping of participants aged 18–49 aligns with prior research,24,73,74 it may mask important heterogeneity in cannabis use patterns and related outcomes. Future studies may benefit from using narrower age bands to more precisely capture age-related differences, particularly among emerging adults.
Conclusions
Using data from an online sample of U.S. adults who frequently consume cannabis, this study contributes to the existing literature by examining differences in cannabis use patterns between younger adults and middle-aged and older adults. These differences primarily involve methods of consumption and reasons for use, areas with limited prior research. The relatively high proportion of middle-aged and older adults reporting cannabis use for recreational purposes and engaging in potentially risky practices, such as the use of concentrates, underscores the need for greater awareness of age-specific health risks. In addition, this study marks an initial effort to apply a newly introduced method for quantifying cannabis use—comprehensively measuring THC intake in milligrams—to evaluate age differences in the risk of CUD.
Authors’ Contributions
O.L.: Conceptualization, methodology, and writing—original draft. J.B.: Data curation, methodology, and writing—review and editing. A.J.B.: Funding acquisition, resources, writing—review and editing, and supervision. C.G.W.: Project administration and writing—review and editing. M.I.H.: Software, validation, and writing—review and editing. C.A.S.: Data curation and writing—review and editing. L.C.: Formal analysis, software, validation, and writing. J.L.: Formal analysis, software, and validation. M.W.: Formal analysis, software, validation, and writing—review and editing. E.A.: Writing—review and editing. D.S.H.: Conceptualization, funding acquisition, writing—reviewing and editing, and supervision.
Footnotes
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.