
Abstract
Background:
Cannabis is the most used federally controlled substance in the United States. Given the increasingly widespread use of cannabis, further examination of its health implications is needed. We evaluated the association of cannabis use and longitudinal kidney outcomes among a cohort of adults living in Baltimore, MD.
Methods:
We used data from healthy aging in neighborhoods of diversity across the life span study. Baseline cannabis use (obtained between 2004 and 2009) was categorized as never tried, tried, never used regularly (irregular use), regular use >6 months prior (former regular use), and regular use within the past 6 months (current regular use). The primary outcome was incident chronic kidney disease (CKD), defined as an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 at follow-up (2013–2017). Risk of rapid kidney function decline (decline in eGFR of >3 mL/min per 1.73 m2 per year) and incident albuminuria (albumin-to-creatinine ratio [ACR] ≥ 30 mg/g) were also assessed. Multivariable logistic regression was used to evaluate the association of cannabis use with kidney outcomes.
Results:
Among 1,521 participants, the mean age was 48 years, 58% were female, and 58% were of Black race. Participants with current regular cannabis use were more likely to be younger, male, Black, and to concurrently use cigarettes, opiates, and/or cocaine. Compared with those with no history of cannabis use, participants with current regular cannabis use were not at higher risk of incident CKD (OR: 0.79 [95% CI: 0.37–1.68]), rapid kidney function decline (OR: 0.80 [95% CI: 0.43–1.49), or incident albuminuria (OR: 0.84 [95% CI: 0.38–1.87]) after adjustment for sociodemographics, health factors, and concurrent use of cigarette, opiate, or cocaine.
Conclusion:
In this Baltimore-based cohort of adults without CKD, there was no independent association between cannabis use and adverse kidney outcomes over time.
Introduction
Cannabis (i.e., marijuana) is the most used federally controlled substance in the United States. In 2023, an estimated 62 million individuals reported using cannabis at least once in the past year. 1 The medical use of cannabis is allowed in 47 states, the District of Columbia, and three U.S. territories. 2 Notably, cannabis use is increasing among middle-aged and older adults, populations that are often impacted by chronic health conditions such as chronic kidney disease (CKD).3,4 Given the rising societal acceptance and widespread use of cannabis, further investigation into its long-term implications for kidney health is warranted.
Cannabis contains phytocannabinoids including Δ9-tetrahydrocannabinol (THC) and cannabidiol (CBD), which exert their effects primarily through G-protein coupled cannabinoid receptors type 1 (CB1) and type 2 (CB2).5,6 In the kidneys, CB1 receptors are predominantly expressed, and their activation has been implicated in the development of diabetic nephropathy, nondiabetic proteinuria, and fibrosis.7–13 It has been noted that patients with IgA nephropathy and those with acute interstitial nephritis exhibit increased CB1 receptor expression in kidney biopsy samples. 10 The role of CB2 receptor expression in the kidney is less clear, as evidence suggests both harmful 14 and protective15–17 kidney-related effects of CB2 expression.
Prior studies have demonstrated associations between substance use (including cigarettes, cocaine, opiates, and other psychotropic agents) and kidney injury.18–21 However, evidence on the long-term impact of cannabis use on kidney outcomes is limited. 6 In this study, we evaluated the association of cannabis use and longitudinal kidney outcomes among a population of adults living in Baltimore, Maryland. We hypothesized that cannabis exposure would be associated with adverse kidney outcomes.
Material and Methods
Study design and participants
We used data from the Healthy Aging in Neighborhoods of Diversity across the Life Span (HANDLS) study, a population-based cohort study aimed at evaluating health disparities by race and socioeconomic status. The HANDLS study design has been previously described in detail. 22 Briefly, 3,720 Black and White city-dwelling adults aged 30–64 years were recruited from 13 neighborhoods in Baltimore, Maryland. Of these, 1,536 participants (41%) had household incomes below 125% of the poverty level, while 2,186 (59%) had incomes above the poverty level. Participants were enrolled between August 2004 and March 2009 (baseline for the present study) with an anticipated longitudinal follow-up of 20 years and five triennial study visits.
We evaluated the association of cannabis use at study baseline and kidney outcomes at HANDLS study visit 4 (between September 2013 and September 2017). Participants were excluded from our analysis if they were missing data on creatinine, cannabis use, or if they did not attend study visit 4 (Fig. 1). Participants with an estimated glomerular filtration rate (eGFR) <60 mL/min per 1.73 m2 at baseline (study visit 1) were excluded from the analysis evaluating the risk of incident CKD at follow-up. Participants with urine albumin-to-creatinine ratio (UACR) ≥30 mg/g at baseline were excluded from the incident albuminuria analyses. Participants with an eGFR <15 mL/min per 1.73 m2 were excluded from the rapid kidney function decline analysis. Given the concern for competing risks due to death, we compared the proportion of deaths that occurred at follow-up between cannabis exposure groups. This study was performed in accordance with the Declaration of Helsinki. Study participants provided written documentation of informed consent, and the National Institute of Environmental Health Sciences, National Institutes of Health, approved the HANDLS study protocol.
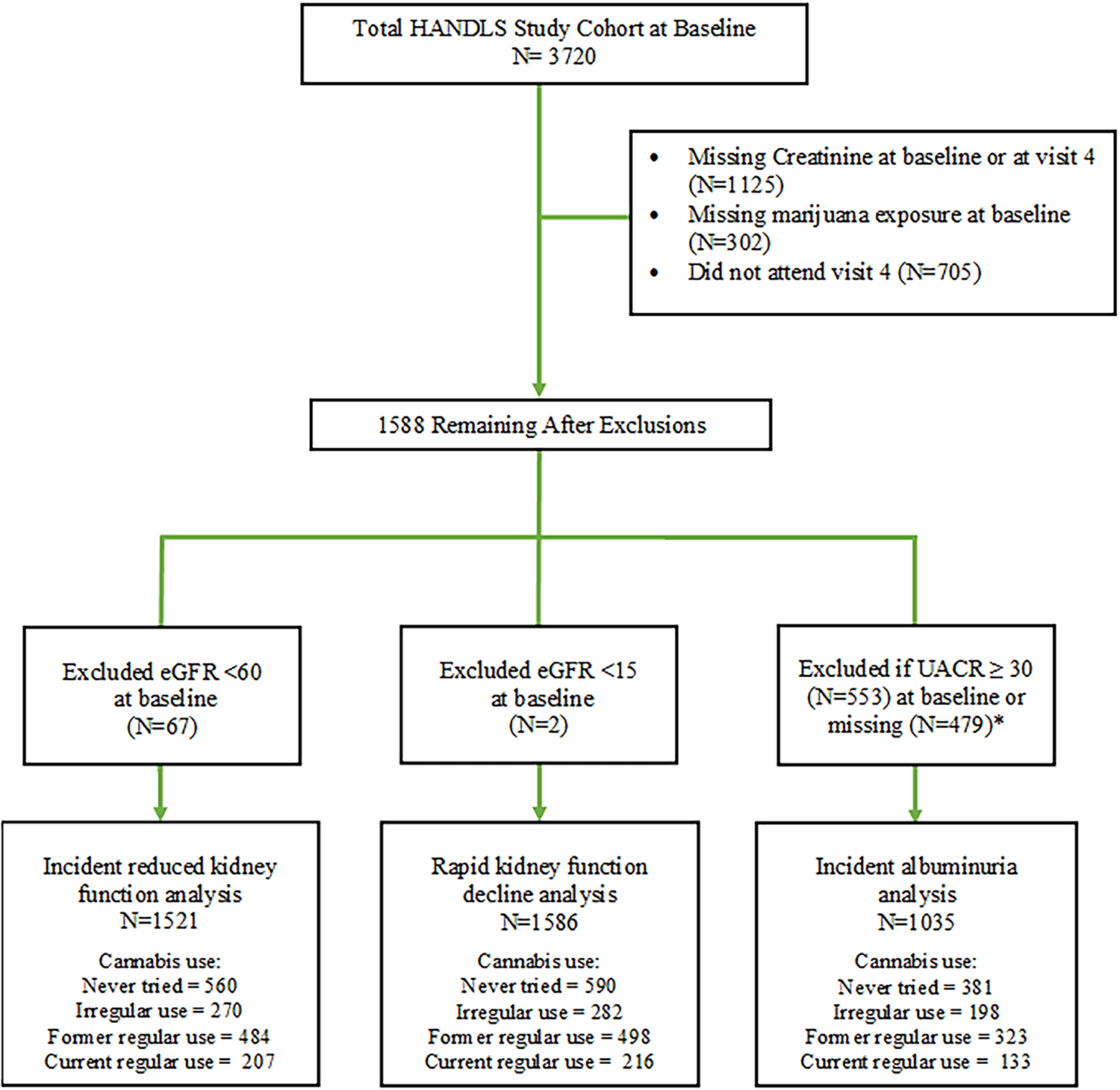
HANDLS cohort and study population. *Exclusions outlined for ACR ≥30 mg/g at baseline and missing ACR at visits 1 or 4 were not mutually exclusive. eGFR, estimated glomerular filtration rate; HANDLS, Healthy Aging in Neighborhoods of Diversity across the Life Span; UACR, urine albumin-to-creatinine ratio.
Primary exposure
The exposure of interest, cannabis use, was obtained by self-report at the baseline study visit. Cannabis use was categorized as (1) never tried, (2) tried, never used regularly, herein referred to as “irregular use” (3) regular use more than 6 months prior, herein referred to as “former regular use,” (4) regular use within the past 6 months, herein referred to as “current regular use.” The cannabis type, mode of consumption, or dosing was not available.
Outcomes
At each study visit, fasting blood and spot urine samples were obtained as part of the medical assessment. Serum creatinine of included participants was measured at Quest Diagnostics Inc. by isotope dilution mass spectrometry (Olympus America Inc., Melville, NY) and standardized to the reference laboratory at the Cleveland Clinic. UACR was evaluated at Quest Diagnostics Inc. using an immunoturbidimetric assay (Kamiya Biomedical Co., Seattle, WA). Glomerular filtration rate was estimated using the 2021 CKD-EPI Creatinine equation. 23 Incident CKD was defined as a new eGFR <60 mL/min per 1.73 m2 at visit 4. Rapid kidney function decline was defined as a reduction in eGFR ≥3 mL/min/1.73 m2 per year between baseline (visit 1) and visit 4.24–26 Incident albuminuria was defined as a new UACR ≥30 mg/g at visit 4.
Covariates
Several sociodemographic variables (age, sex at birth, self-identified Black or White race, household income above or below 125% of the federal poverty level, 27 and level of educational attainment measured in years) were ascertained at baseline. Clinical and behavioral measures such as systolic blood pressure (SBP), body mass index (BMI), hypertension (HTN), diabetes mellitus (DM), current smoking, cocaine, and opioid use were also assessed at baseline. Each participant underwent sitting and standing blood pressure measurements on each arm using the brachial artery auscultation method with an appropriately sized inflatable cuff. HTN at baseline was defined based on self-report of HTN, prescription of antihypertensive medications, or having an average seated SBP ≥140 mm Hg, or an average seated diastolic blood pressure ≥90 mmHg (following the diagnostic guidelines in existence at the time of study enrollment). DM status was defined based on self-report of DM, a fasting glucose level ≥126 mg/dL, or prescription for glucose-lowering medication. Self-report (yes/no) of current cigarette smoking, opioid, or cocaine use was assessed.
Statistical analysis
Baseline participant characteristics, stratified by cannabis use status, were compared using analysis of variance or chi-square tests for continuous or categorical variables, respectively. Multivariable logistic regression was used to evaluate the odds of incident CKD, rapid eGFR decline, and albuminuria at follow-up, respectively, by cannabis use status. Participants who reported never trying cannabis served as the reference group. Multivariable models were built a-priori based on prior literature and adjusted for continuous variables (age, baseline eGFR, and educational attainment in years) and dichotomized variables (sex, poverty status, DM, HTN, concurrent cigarette smoking, opioid, or cocaine use). All kidney outcomes were analyzed as dichotomous measures. A p value <0.05 was considered statistically significant. We performed sensitivity analyses to evaluate the association of cannabis use and kidney outcomes among HANDLS participants who returned for visit 5, a more recent follow-up visit of participants (September 2017 to March 2020), but one in which recruitment ended early due to the COVID-19 pandemic. All analyses were conducted using Stata Version 16.0 (StataCorp, College Station, TX).
Results
Among 1,521 study participants, the mean age was 48 years; 893 (58%) were female, and 889 (58%) were of Black race (Table 1). Thirty-eight percent (n = 574) had an annual income less than 125% of the federal poverty level, 663 (44%) had HTN, and 690 (46%) were concurrently using cigarettes. Concurrent cocaine and opiate use were low, reported by 99 (6.5%) and 51 (3.5%) participants, respectively. For cannabis use, 560 (37%) reported never trying; 270 (18%) reported irregular use; 484 (32%) reported former regular use; 207 (14%) reported current regular use (Table 1). Participants with current regular use were more likely to be younger, male, of Black race, have an annual income <125% federal poverty level, and concurrently use cigarettes, opiates, or cocaine; but they were less likely to have HTN or DM.
Baseline Characteristics according to Cannabis Use Status
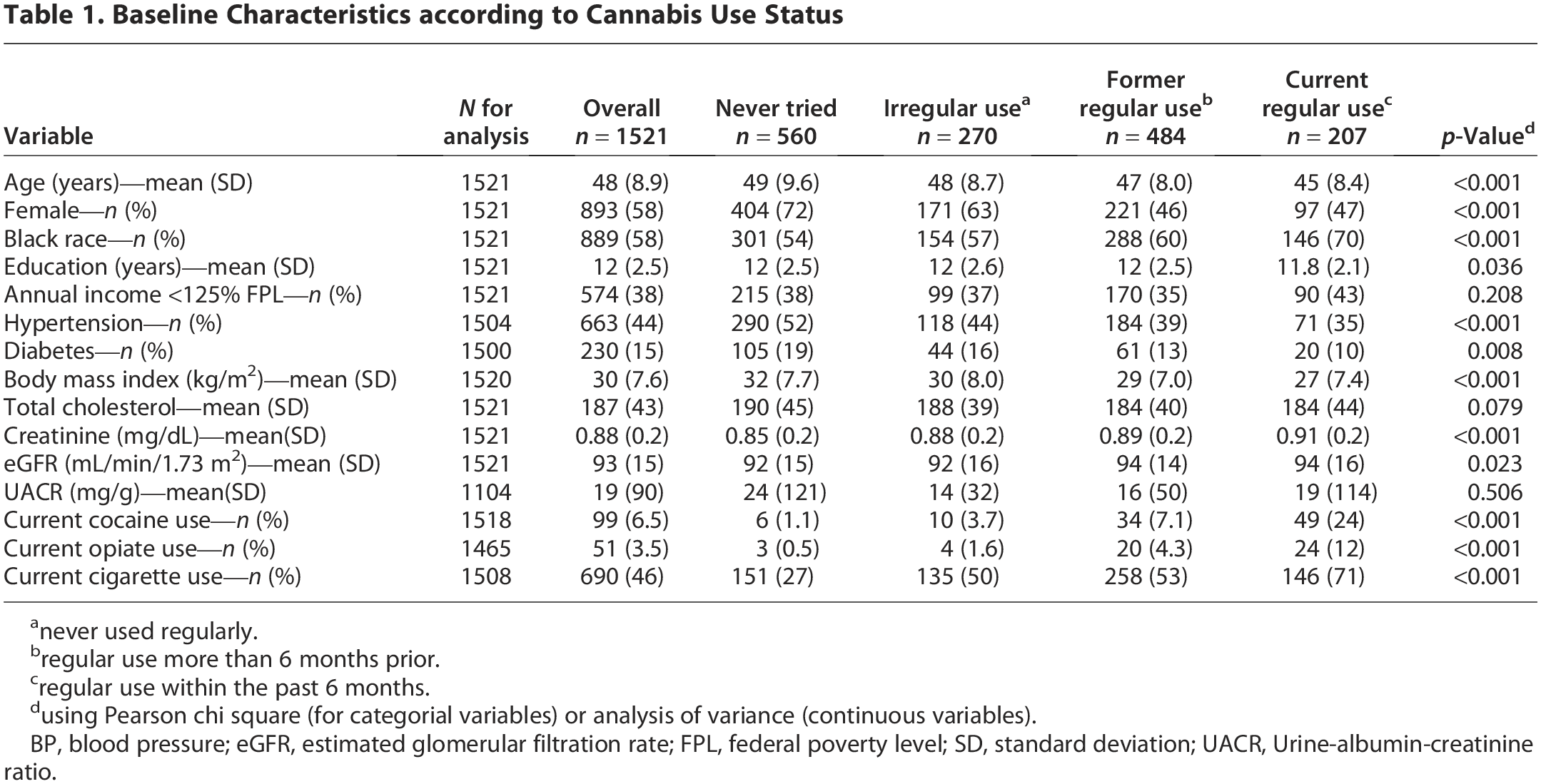
never used regularly.
regular use more than 6 months prior.
regular use within the past 6 months.
using Pearson chi square (for categorial variables) or analysis of variance (continuous variables).
BP, blood pressure; eGFR, estimated glomerular filtration rate; FPL, federal poverty level; SD, standard deviation; UACR, Urine-albumin-creatinine ratio.
The average follow-up time between baseline and visit 4 was 8.6 years, ranging from 4.8 to 12.5 years. A total of 52 (3%) deaths occurred in this sample, but there was no statistically significant difference in deaths between cannabis exposure groups (Pearson χ2, p = 0.821) (Supplementary Table S1). Among 1521 participants with an eGFR of ≥60 mL/min per 1.73 m2 at visit 1, 121 (8%) developed incident CKD at follow-up. After multivariable adjustment, participants with irregular use (odds ratio [OR]: 0.68 [95% confidence interval (CI), 0.37 to 1.25]), and those with former regular use (OR: 0.75 [95% CI, 0.43 to 1.31]), had a similar risk of developing incident CKD compared with those who had never tried cannabis. Participants with current regular use also had a similar risk of developing incident CKD at follow-up, compared to those who never tried cannabis (OR: 0.79 [95% CI, 0.37 to 1.68]) (Table 2).
Odds Ratio for Incident Chronic Kidney Disease at Follow-Up (i.e., New eGFR < 60 mL/Min/1.73 m2)
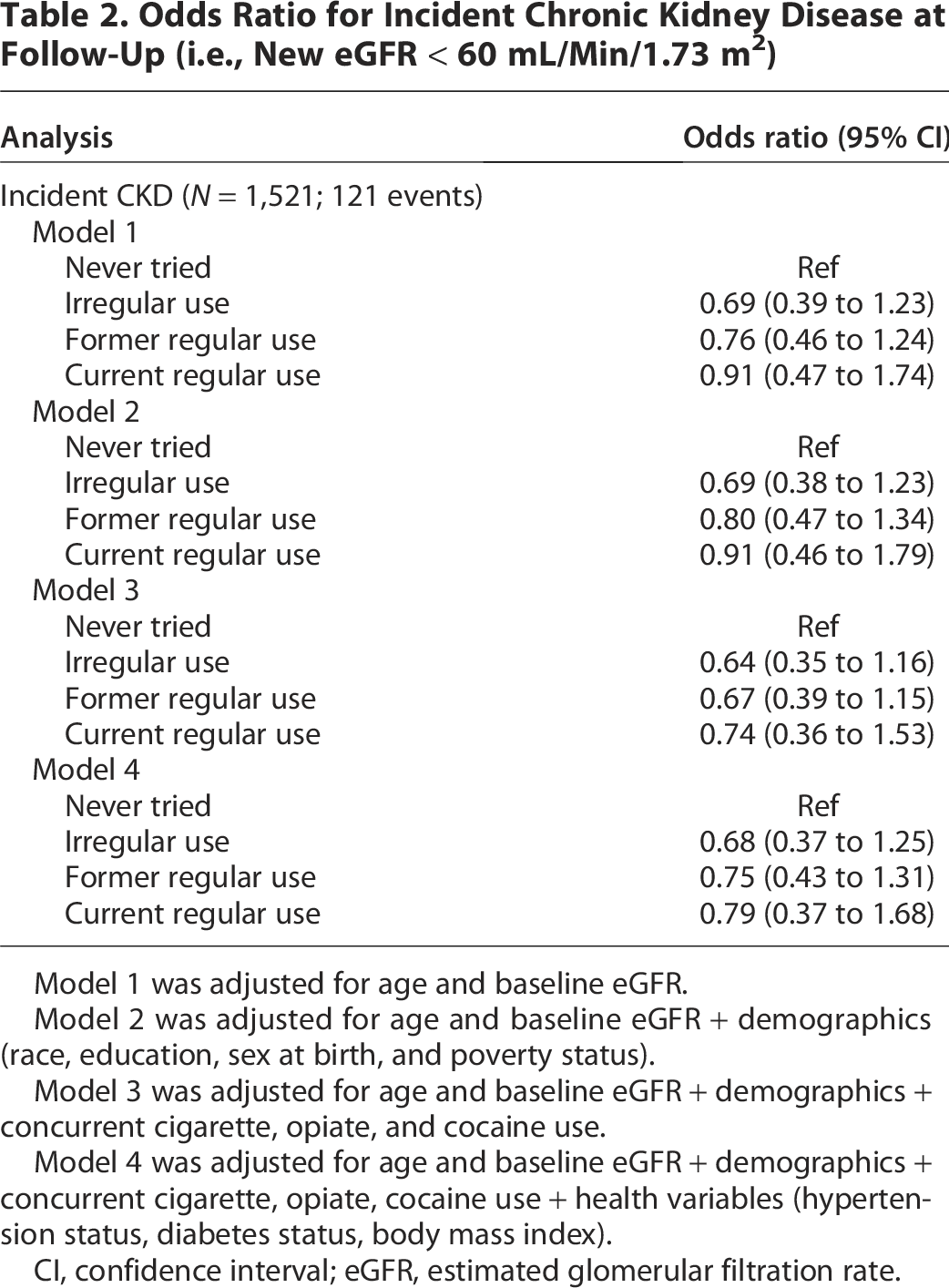
Model 1 was adjusted for age and baseline eGFR.
Model 2 was adjusted for age and baseline eGFR + demographics (race, education, sex at birth, and poverty status).
Model 3 was adjusted for age and baseline eGFR + demographics + concurrent cigarette, opiate, and cocaine use.
Model 4 was adjusted for age and baseline eGFR + demographics + concurrent cigarette, opiate, cocaine use + health variables (hypertension status, diabetes status, body mass index).
CI, confidence interval; eGFR, estimated glomerular filtration rate.
Among 1586 participants, 173 (11%) developed rapid kidney function decline. The median (interquartile range) changes in eGFR between study visits 1 and 4 was −5.6 (−14.3 to 1.3) mL/min per 1.73 m2. Compared with participants who never tried cannabis, the risk of developing rapid eGFR decline was similar for participants with irregular use (OR: 0.92 [95% CI, 0.56 to 1.50]), those with former regular use (OR: 0.82 [95% CI, 0.53 to 1.28]), and those with current regular use (OR: 0.80 [95% CI, 0.43 to 1.49). (Table 3). Lastly, among 1,035 participants with available UACR data at visits 1 and 4, 109 (10%) developed incident albuminuria. Compared with those who never tried cannabis, participants with former regular use (OR: 0.89 [95% CI, 0.50 to 1.59] or current regular use (OR: 0.84 [95% CI, 0.38 to 1.87]) had a similar risk of developing incident albuminuria at follow-up (Table 4).
Odds Ratio for Rapid eGFR Decline (i.e., >3 mL/Min/1.73 m2 per Year)
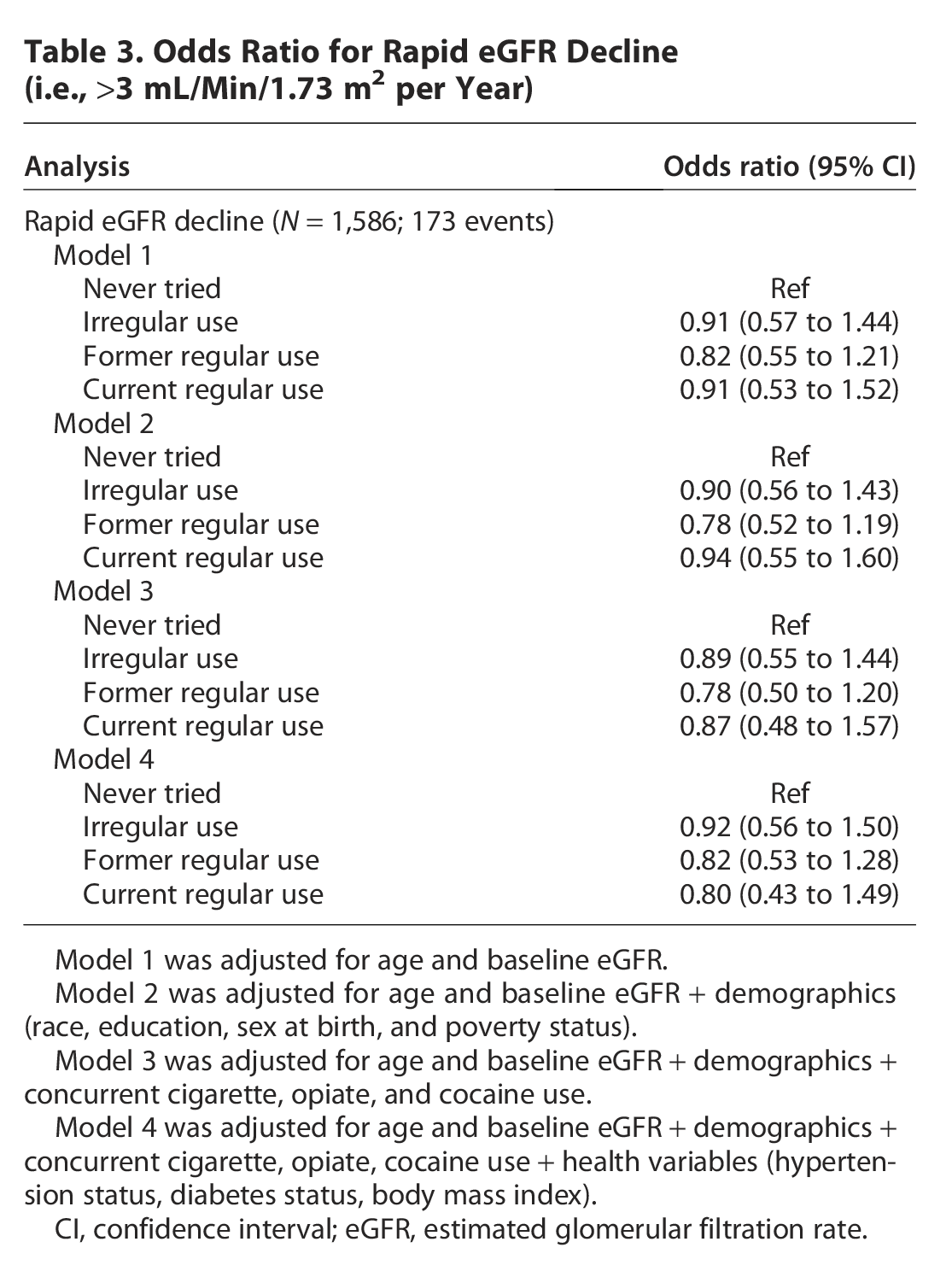
Model 1 was adjusted for age and baseline eGFR.
Model 2 was adjusted for age and baseline eGFR + demographics (race, education, sex at birth, and poverty status).
Model 3 was adjusted for age and baseline eGFR + demographics + concurrent cigarette, opiate, and cocaine use.
Model 4 was adjusted for age and baseline eGFR + demographics + concurrent cigarette, opiate, cocaine use + health variables (hypertension status, diabetes status, body mass index).
CI, confidence interval; eGFR, estimated glomerular filtration rate.
Odds Ratio for Incident Albuminuria at Follow-Up (i.e., New UACR ≥30 mg/g)
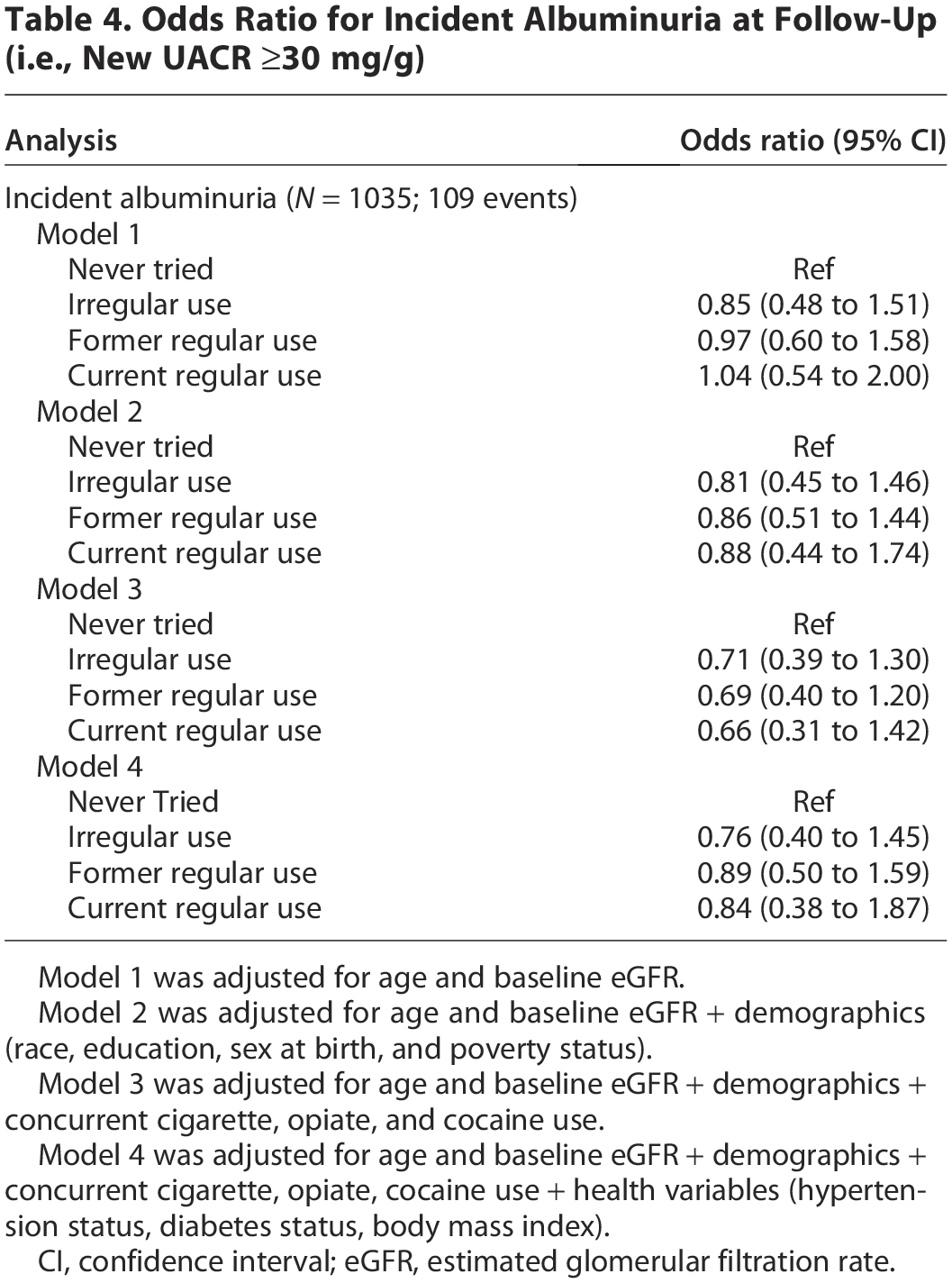
Model 1 was adjusted for age and baseline eGFR.
Model 2 was adjusted for age and baseline eGFR + demographics (race, education, sex at birth, and poverty status).
Model 3 was adjusted for age and baseline eGFR + demographics + concurrent cigarette, opiate, and cocaine use.
Model 4 was adjusted for age and baseline eGFR + demographics + concurrent cigarette, opiate, cocaine use + health variables (hypertension status, diabetes status, body mass index).
CI, confidence interval; eGFR, estimated glomerular filtration rate.
In sensitivity analyses of 820 participants returning for visit 5 follow-up (mean [range] follow-up time of 11.9 [8.9–15.2] years), former regular use was associated with a reduced risk of incident CKD after multivariable adjustment (OR: 0.45; 95% CI: 0.22–0.94). However, no significant association was observed for participants with current regular use (OR: 0.40; 95% CI: 0.14–1.11). Among participants who returned for visit 5, only 80 (9.7%) developed incident CKD. After multivariable adjustment, participants with former and current regular use had a similar risk of developing rapid kidney function decline or incident albuminuria by visit 5 compared with those who had never tried cannabis (Supplementary Tables S2, S3, and S4).
Discussion
In this prospective cohort study of middle-aged adults living in Baltimore, Maryland, who were free of CKD at baseline, 14% reported regular cannabis use within the past 6 months, similar to the 15% of U.S. adults in 2022 who reported use within the past 30 days. Consistent with previous studies, we found that individuals who used cannabis were less likely to have HTN or DM, and they also had lower BMIs.28,29 Regular cannabis use was associated with a similar risk of incident CKD compared with participants who never tried cannabis, over a mean follow-up time of 8.6 years. In addition, neither former nor current regular cannabis use was associated with rapid kidney function decline or incident albuminuria at follow-up.
Our findings are consistent with several studies evaluating the association of cannabis exposure and CKD. In a smaller prospective cohort study of 647 middle-aged male veterans with HTN, followed from 1977 to 1999, cannabis use was not associated with an increased risk of mild kidney function decline (defined as an increase in serum creatinine level of 0.6 mg/dL or greater). 30 Similarly, a cross-sectional study among 13,995 U.S. adults aged 18 to 59 years examining U.S. adults from the National Health and Nutrition Examination Survey from 2007 to 2014, showed that participants with past and current cannabis use had a trend towards higher serum creatinine and lower mean eGFR. However, in multivariable-adjusted analyses, cannabis use did not have a significant association with either outcome. 31 In a retrospective analysis of 1,559 patients enrolled in the Assessment, Serial Evaluation, and Subsequent Sequelae in Acute Kidney Injury (ASSESS-AKI) study—a parallel matched cohort study that enrolled individually matched hospitalized adults with and without acute kidney injury between 2009 and 2015, cannabis use was not associated with incident CKD. 29 Moreover, a cross-sectional analysis of 3,765 young adults with preserved eGFR enrolled in the Coronary Artery Risk Development in Young Adults (CARDIA) Study showed that cannabis use was associated with lower eGFR measured by cystatin C (eGFRcys) in cross-sectional analyses. 32 However, investigators did not detect an association between cannabis use and subsequent change in eGFRcys in longitudinal analyses; this discrepancy is likely due to the greater susceptibility of cross-sectional analyses to confounding. Lastly, in the largest observational study evaluating cannabis use and kidney function (n = 223,354) that included individuals enrolled in the All of Us Research Program, lifetime cannabis use was not associated with prevalent CKD after multivariable adjustment. However, daily and weekly cannabis consumption in the preceding 3 months was significantly associated with prevalent CKD (n = 58,660). Incident CKD was not evaluated. 28
In the present study, cannabis use was not associated with rapid kidney function decline (reduction in eGFR ≥3 mL/min/1.73 m2 per year), while previous studies have found mixed results. In an analysis using CARDIA data (study start: 1995–1996, follow-up of 10 years), cannabis use was not associated with a rapid decline (≥3%/year) in eGFR measured by eGFRcys. 32 Similarly, in the Chronic Renal Insufficiency Cohort Study, which included 3,939 participants with CKD enrolled between 2003 and 2008, cumulative cannabis use was not linked to CKD progression. 33 Conversely, in the retrospective analysis of ASSESS-AKI participants, cannabis consumption was associated with faster annual decline in eGFR among participants with CKD (but not among those free of CKD at baseline). However, cannabis consumption was not associated with progressive CKD (defined as ≥50% reduction in eGFR compared with the 3-month post-hospitalization eGFR, reaching CKD stage 5, or receiving kidney replacement therapy) regardless of baseline kidney function. 29
Our study had limitations. Cannabis use was assessed only at baseline, and we did not capture the route of consumption nor quantify frequency of regular use (e.g., daily, weekly, or monthly). This is particularly important given that participants’ cannabis use may have increased during the follow-up period, coinciding with a national rise in cannabis use. 34 We lacked complete data on some covariates of interest. The low event rate for incident CKD, rapid kidney function decline, and albuminuria in our sample likely influenced our statistical power to detect differences across cannabis use groups. Given the inherent limitations of observational data, we are unable to establish causality, and our results may be subject to residual confounding that could influence the observed associations. Furthermore, our results may not be generalizable to older adults who are more often affected by CKD, and a group with increasing rates of cannabis use.35,36 Future studies should include important subpopulations, such as older adults, and further investigate the impact of cannabis use on pre-existing CKD and proteinuria. Prospective studies should aim to collect information on cannabis route of consumption and dosage, exclude individuals with concomitant use of other substances to minimize confounding, and follow individuals over longer periods to capture outcomes such as kidney failure. In addition, research should account for rising cannabis use and evolving legislation that may influence consumption patterns. For example, in Maryland, House Bill 881 (passed in 2014) established a regulatory framework for medical cannabis, but the program did not become operational until 2017, 37 coinciding with the start of HANDLS visit 5 (2017–2020), while visit 4 occurred between 2013 and 2017. Finally, while regulatory barriers pose challenges, clinical trial data in this population would be invaluable for addressing questions that are difficult to resolve using real-world observational data.
Despite these limitations, our study has several strengths. It includes a large, contemporary cohort of participants residing in Baltimore, MD, a state that ranked fifth in the nation for cannabis possession arrests in 2010. 37 Furthermore, we were able to evaluate the association between cannabis use and longitudinal kidney outcomes over a mean follow-up period of 8.6 years.
In conclusion, among a cohort of adults without CKD, we found that cannabis use was not associated with incident reduced kidney function, incident albuminuria, or rapid kidney function decline. Future studies should examine the potential kidney health impacts of various routes of cannabis consumption and dosage, particularly given that the variety of cannabis products has expanded in recent years.
Authors’ Contributions
F.A.: Conceptualization (lead), data curation (supporting), formal analysis (lead), writing—original draft (supporting), writing—review and editing (equal), and project administration (lead). D.H.: Conceptualization (supporting), data curation (supporting), formal analysis (supporting), writing—original draft (supporting), and writing—review and editing (equal). A.B.Z.: Conceptualization (supporting), data curation (supporting), writing—original draft (supporting), writing—review and editing (equal), resources (equal), and supervision (supporting). M.K.E.: Conceptualization (supporting), data curation (supporting), writing—original draft (supporting), writing—review and editing (equal), resources (equal), and supervision (supporting). D.C.C.: Conceptualization (supporting), data curation (supporting), formal analysis (supporting), writing—original draft (supporting), writing—review and editing (equal), resources (equal), supervision (lead), and project administration (supporting).
Footnotes
Acknowledgment
The authors would like to thank the participants of the HANDLS study.
Funding Information
This work was supported by the Intramural Research Program of the National Institute on Aging, National Institutes of Health (NIH). F.A. was supported, in part, by grant 2T32DK007732-26 from the NIH/National Institute of Diabetes and Digestive and Kidney Diseases.
Author Disclosure Statements
The authors have no conflicts of interest to disclose.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.