
Abstract
Background:
HYPER-H21-4 trial, a randomized, placebo-controlled, crossover trial, showed that chronic cannabidiol (CBD) supplementation reduces blood pressure (BP) in patients with primary hypertension. Given the association between the endocannabinoid (EC) system and hypertension, we aimed to determine whether changes in circulating ECs, signaling molecules of the EC system, could explain CBD-mediated cardiovascular effects.
Methods:
For this purpose, anandamide (AEA) and 2-arachidonoylglycerol (2-AG) were measured in 66 patients with hypertension. Patients were assigned to receive CBD for 5 weeks (225–300 mg/day for the first 2.5 weeks, increasing to 375–450 mg/day for the subsequent 2.5 weeks), followed by 5 weeks of placebo, or 5 weeks of placebo followed by 5 weeks of CBD.
Results:
Administration of the CBD formulation for 5 weeks resulted in a significant increase in plasma AEA levels, whereas no such increase was observed during the placebo period (Placebo: 37.0 ± 18.0 ng/mL vs. 38.9 ± 20.8 ng/mL, CBD: 36.7 ± 18.0 ng/mL vs. 47.9 ± 24.6 ng/mL, F = 3.592, p = 0.042; ΔCBDAEA 11.1 ± 3.7 ng/mL, p = 0.025). Change in AEA levels following CBD administration (ΔCBDAEA) did not correlate with change in systolic BP following CBD administration (ΔCBDSBP) (r = −0.106, p = 0.428). Multivariate analysis showed that body mass index, current antihypertensive treatment, and fasting plasma glucose at baseline emerged as significant predictors of AEA increase, while BP reduction did not demonstrate a significant association. No significant association was found between chronic CBD administration and 2-AG plasma concentrations (placebo: 28.8 ± 4.3 ng/mL vs. 38.9 ± 20.8 ng/mL; CBD: 36.7 ± 18.0 ng/mL vs. 47.9 ± 24.6 ng/mL; F = 0.513, p = 0.478).
Conclusions:
Collectively, these findings suggest that although chronic CBD administration appears to increase AEA, but not 2-AG plasma levels, this study provides no conclusive evidence that such alterations explain CBD-mediated BP reduction.
Introduction
Given the long-standing use of Cannabis sativa, extensive data have accumulated on the physiological effects of its constituents. 1 Among the more than 110 identified phytocannabinoids—chemical compounds produced by cannabis—cannabidiol (CBD) and tetrahydrocannabinol are the most studied. A key challenge in CBD research is its interaction with over 65 molecular targets, including receptors, ion channels, transporters, and enzymes. 2 Notably, CBD exhibits low affinity for cannabinoid receptors CB1 and CB23,4 but acts as a “functional antagonist” of CB1, likely via negative allosteric modulation.3,4
The discovery of the human endocannabinoid (EC) system—a complex lipid signaling network that regulates cardiovascular, immune, and central nervous functions—further complicates CBD research. 5 This system includes cannabinoid receptors, enzymes for EC synthesis and degradation, and endogenous ligands called ECs. The two major ECs, anandamide (AEA) and 2-arachidonoylglycerol (2-AG), exert effects that are tightly regulated by their on-demand synthesis and rapid enzymatic breakdown. 6 ECs have been associated with cardiometabolic disorders, including hypertension, diabetes, and heart failure, 7 with animal studies and small human investigations linking ECs to elevated blood pressure (BP).8–11 In pre-clinical studies, AEA has been shown to reduce BP by lowering cardiac contractility and peripheral vascular resistance through CB1 receptor activation. These effects are more pronounced in hypertensive animal models, possibly due to upregulation of CB1 expression in cardiovascular tissues, as discusssed later. 12
We recently completed the HYPER-H21-4 trial, a randomized, placebo-controlled, crossover study showing that 5-week CBD supplementation lowered BP in patients with primary hypertension. 13 Subsequent mechanistic sub-analyses explored the basis of this effect.14–17 Given the EC system’s association with hypertension and our trial findings, we aimed to determine whether CBD’s cardiovascular effects could be explained by changes in circulating EC levels.
Materials and Methods
Study design and ethical considerations
The present study represents a focused, exploratory, mechanistic sub-analysis of the HYPER-H21-4 trial, a randomized, triple-blind (participants, investigators, and outcomes assessor), placebo-controlled, crossover study conducted from December 2021 to April 2022. The trial took place at the Department of Integrative Physiology and Department of Pathophysiology, University of Split School of Medicine, in accordance with the Declaration of Helsinki and reviewed by the institutional Ethics Committee (15th December 2021, Class: 003-08/21-03/0003; Reg. No.: 2181-198-03-04-21-0091). Participants provided informed consent, and the study was registered on ClinicalTrials.gov (ID: NCT05346562). Full details of the protocol and capsule manufacturing are reported elsewhere. 18
Participants
The study included 70 participants in total, but for the present analysis, only patients who finished the whole course of the study were taken into account (66 participants). Inclusion criteria were as follows: Grade 1 or Grade 2 hypertension, as defined by the contemporary European Society of Cardiology guidelines; age between 40 and 70 years; and a body mass index (BMI) between 18.5 and 35 kg/m2. 19 Conversely, patients were excluded if they met any of the following conditions: any secondary form of hypertension; antihypertensive treatment not consisting of an ACE inhibitor, diuretic, or calcium channel blocker; use of CBD-containing supplements (regardless of administration route); smoking; use of cannabis-based products; or the presence of significant chronic diseases such as malignancy, heart failure, liver cirrhosis, chronic kidney disease, diabetes mellitus, or epilepsy, as well as significant psychiatric disorders.
Intervention
Subjects were randomly assigned to receive either placebo or CBD for 5 weeks, with doses adjusted based on body mass (225–300 mg/day for the first 2.5 weeks, increasing to 375–450 mg/day for the subsequent 2.5 weeks), as delineated in the study protocol. 18 The CBD dosing in the present study was selected based on prior pharmacokinetic and BP studies using similar formulations, as well as published safety data, to balance efficacy with minimization of adverse events. Following a two-week washout period, patients initially receiving CBD switched to placebo for 5 weeks, while those who had started with placebo transitioned to CBD, following the same dosing regimen. CBD was encapsulated in vegan-gel capsules, each containing 75 mg of CBD in a patented DehydraTECH™2.0 CBD formulation produced by Lexaria Bioscience Corp. The placebo capsules were filled with an organic substrate powder containing no active CBD and placed into matching vegan gel capsules for blinding purposes.
Clinical and biochemical assessment
At baseline and after each intervention, patients were scheduled to visit the lab. During each visit, a sample of venous blood from the cubital vein was taken for immediate analysis, including complete blood count, blood glucose, electrolytes, lipids, creatinine, and liver enzymes. Part of the blood was aliquoted and stored at −80°C for subsequent EC analysis. In addition, at each instance, urine samples were obtained in order to establish the concentration of CBD metabolites (7-OH-CBD and 7-COOH-CBD) in urine. Blood was drawn via venipuncture into prechilled polypropylene Vacutainer tubes containing K2-EDTA as anticoagulant (6 mL, BD Biosciences). Immediately after inversion (8–10 gentle turns), tubes were kept on ice and processed within 30 min. The choice of ethylenediaminetetraacetic acid and rapid cooling/processing was based on evidence that anticoagulant and handling conditions influence measured EC levels. Whole blood was centrifuged at 1,500×g for 10 min at 4°C. Plasma concentrations of the ECs AEA and 2-AG were measured using a competitive enzyme-linked immunosorbent assay (ELISA). Following thawing, plasma samples were kept on ice to minimize enzymatic degradation. Prior to analysis, samples were prediluted at a ratio of 1:4 for AEA and 1:5 for 2-AG using phosphate-buffered saline (phosphate-buffered saline; pH 7.2), in accordance with the manufacturer’s instructions. Quantification was performed using commercial ELISA kits (Abbexa, Cambridge, United Kingdom), and absorbance was measured on an Elisys Duo ELISA analyser (Human Diagnostics Worldwide). The limit of detection (LOD) was 0.1 ng/mL for AEA and 1 ng/mL for 2-AG, with assay ranges of 0.1–10 ng/mL and 1–100 ng/mL, respectively. The intra-assay and inter-assay coefficients of variation were <10% for AEA and <12% for 2-AG, indicating good assay precision. For the analysis of CBD and its metabolites, plasma was separated by centrifugation at 4°C at 1,370 × g for 10 min and stored at −20°C within 1 to 2 h of collection. Each sample was labeled with the study number, test session number, date, and time of collection for each participant. For each patient, two urine samples (5–10 mL) and three plasma samples (1.5–2 mL) were sent directly to the laboratory for evaluation. Standards for the qualitative and quantitative determination of CBD were sourced from Cerilliant, Sigma Aldrich (Round Rock, TX, USA), and the analysis was performed using the UHPLC-MS/MS system (Ultimate 3000RS with TSQ Quantis MS/MS detector, Thermo Fischer Scientific, Waltham, MA, USA). The quantitative analysis was conducted with external calibration curves for each analyte, which ranged from 0 ng/mL to 2,000 ng/mL. The limits of detection (LOD) and quantification (LOQ) were established using the Blank Samples method (Supplementary Table S1). Biochemists with extensive experience, blinded to the participants’ group allocation, analyzed all blood and urine samples following standard operating procedures in a certified institutional biochemical laboratory.
At the first visit, in addition to a detailed anthropometric assessment and clinical examination, advanced glycation end products (AGEs) were analyzed using AGE Reader (DiagnOptics Technologies BV, Groningen, The Netherlands), a noninvasive desktop device that uses the characteristic fluorescence of certain AGEs to calculate the level of accumulated AGEs in the skin and associated cardiovascular risk category.20,21 AGEs are a heterogeneous group of molecules formed through nonenzymatic glycation of proteins, lipids, and nucleic acids. They exert a range of biological effects, including pro-inflammatory and pro-oxidative actions. A large body of evidence indicates that excessive accumulation of AGEs is associated with increased cardiovascular risk.20,21 Finally, during each visit, patients were instrumented with a Schiller BR-102 plus PWA (Schiller AG, Baar, Switzerland), 24‐h ambulatory BP monitor system. The device was programmed to record measurements every 30 min during the day (8:00 AM to 11:00 PM) and every hour throughout the night (11:00 PM to 8:00 AM). Ambulatory BP readings were processed using a modified version of the Casadei method, and the analysis was conducted by two independent investigators who were blinded to the patients’ allocation.
Statistical analysis
Statistical analysis and graphical data representation were conducted using IBM SPSS Statistics (version 29.0, IBM, Chicago, IL, USA), Prism for Windows® (version 10.3.1, GraphPad, La Jolla, CA, USA), and R software (version 4.4.0; R Core Team, Vienna, Austria). The Shapiro–Wilk test was used to judge the normality of data distribution. Categorical variables were presented as whole numbers and percentages, and comparisons were made using the chi-squared (χ2) test. Quantitative data were expressed either as mean ± standard deviation or median and interquartile range, depending on the distribution characteristics. Spearman’s rank correlation was used to assess potential relationships between quantitative variables. To assess the dynamics of AEA, we employed a mixed model analysis of variance (ANOVA). Time points (baseline and end of the treatment period) and treatment regimen (CBD vs. placebo) were assigned as within-subject factors, while the treatment sequence (CBD followed by placebo vs. placebo followed by CBD) was treated as a between-subject factor. For each analysis, F-values reflecting the interaction between time and treatment (time*treatment) were reported, with Bonferroni post hoc tests applied to assess specific pairwise comparisons. In cases where no significant time*treatment interaction was observed, the corresponding p-values were provided. Differences in pre- and post-intervention values (ΔCBD) were reported as mean ± standard error of the mean. To determine the factors associated with changes in AEA following five weeks of CBD supplementation, we employed multiple logistic regression analysis. In the initial model, we utilized stepwise regression, incorporating independent variables such as age, sex, BMI, fasting blood glucose levels, current treatment with antihypertensive drugs (angiotensin-converting enzyme inhibitors ± CCB ± diuretics), AGEs-based risk category, BP reduction, and CBD dosage (mg/kg/day). Subsequently, significant predictors identified in the first model—namely age, blood glucose, history of treated or untreated hypertension, and BP reduction—were incorporated into a second model (standard regression) to mitigate the risk of overfitting. In both models, the dependent variable was defined as either an increase in AEA or the absence of such an increase. As 2-AG levels did not follow a normal distribution, Aligned Rank Transform (ART) ANOVA was employed. Furthermore, multiple linear regression analysis on rank-transformed data was used to determine whether 7-OH-CBD levels at the end of the CBD intervention are associated with 2-AG levels, independent of age, sex, and BMI. All analyses were performed on a per-protocol basis. p < 0.05 was considered significant in all instances.
Results
The baseline characteristics of the studied population were previously detailed in the main study. 13 Key characteristics relevant to the current analysis are presented in Table 1. The average age of the participants was 54.5 years, with males accounting for 56% of the population, and the median BMI was 28.2 kg/m2.
Baseline Characteristics of Studied Population
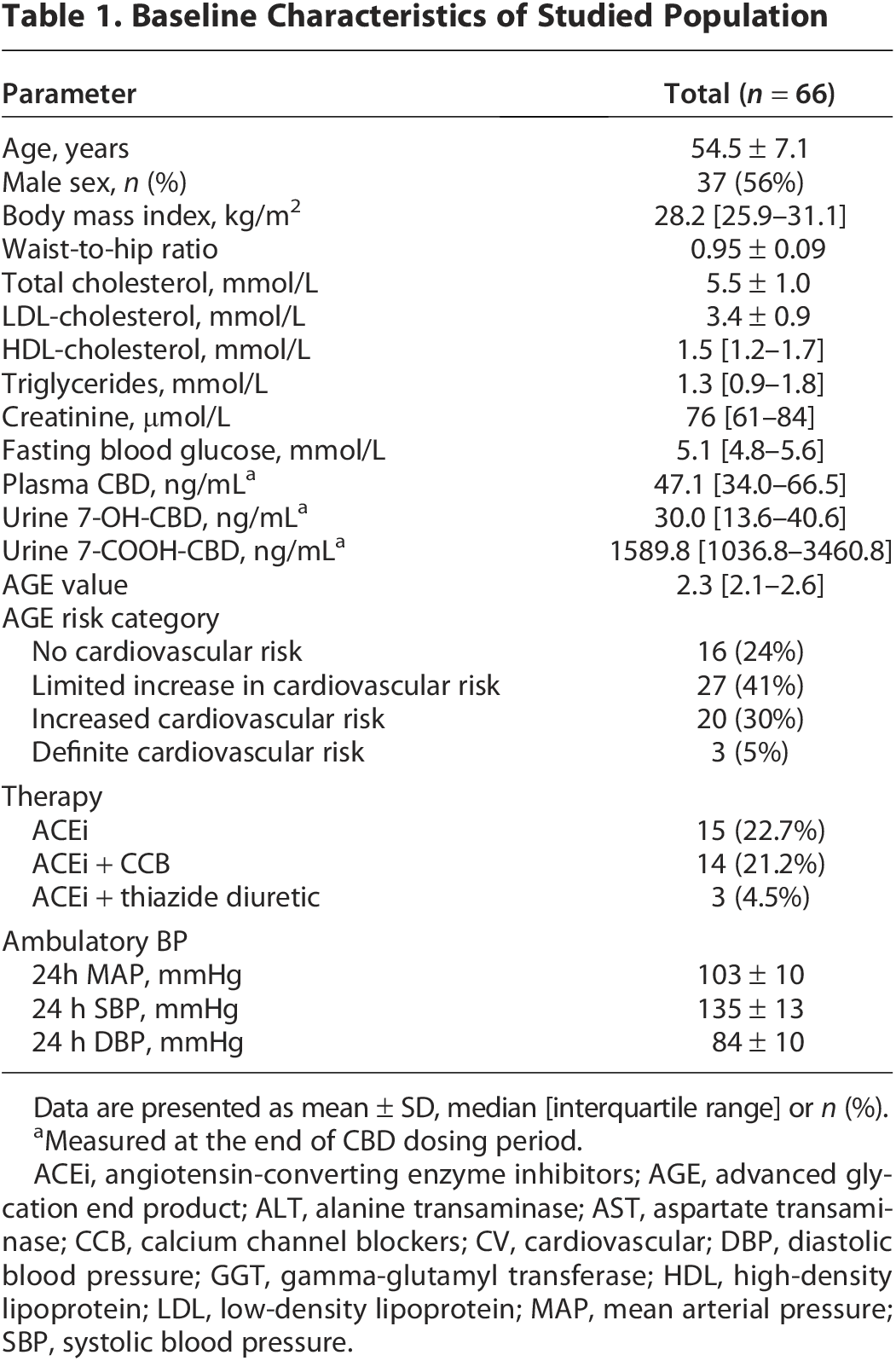
Data are presented as mean ± SD, median [interquartile range] or n (%).
Measured at the end of CBD dosing period.
ACEi, angiotensin-converting enzyme inhibitors; AGE, advanced glycation end product; ALT, alanine transaminase; AST, aspartate transaminase; CCB, calcium channel blockers; CV, cardiovascular; DBP, diastolic blood pressure; GGT, gamma-glutamyl transferase; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MAP, mean arterial pressure; SBP, systolic blood pressure.
Administration of the CBD formulation for 5 weeks resulted in a significant increase in plasma AEA levels, whereas no such increase was observed during the placebo period (placebo: 37.0 ± 18.0 ng/mL vs. 38.9 ± 20.8 ng/mL, CBD: 36.7 ± 18.0 ng/mL vs. 47.9 ± 24.6 ng/mL, F = 3.592, p = 0.042; ΔCBDAEA 11.1 ± 3.7 ng/mL, p = 0.025) (Fig. 1).
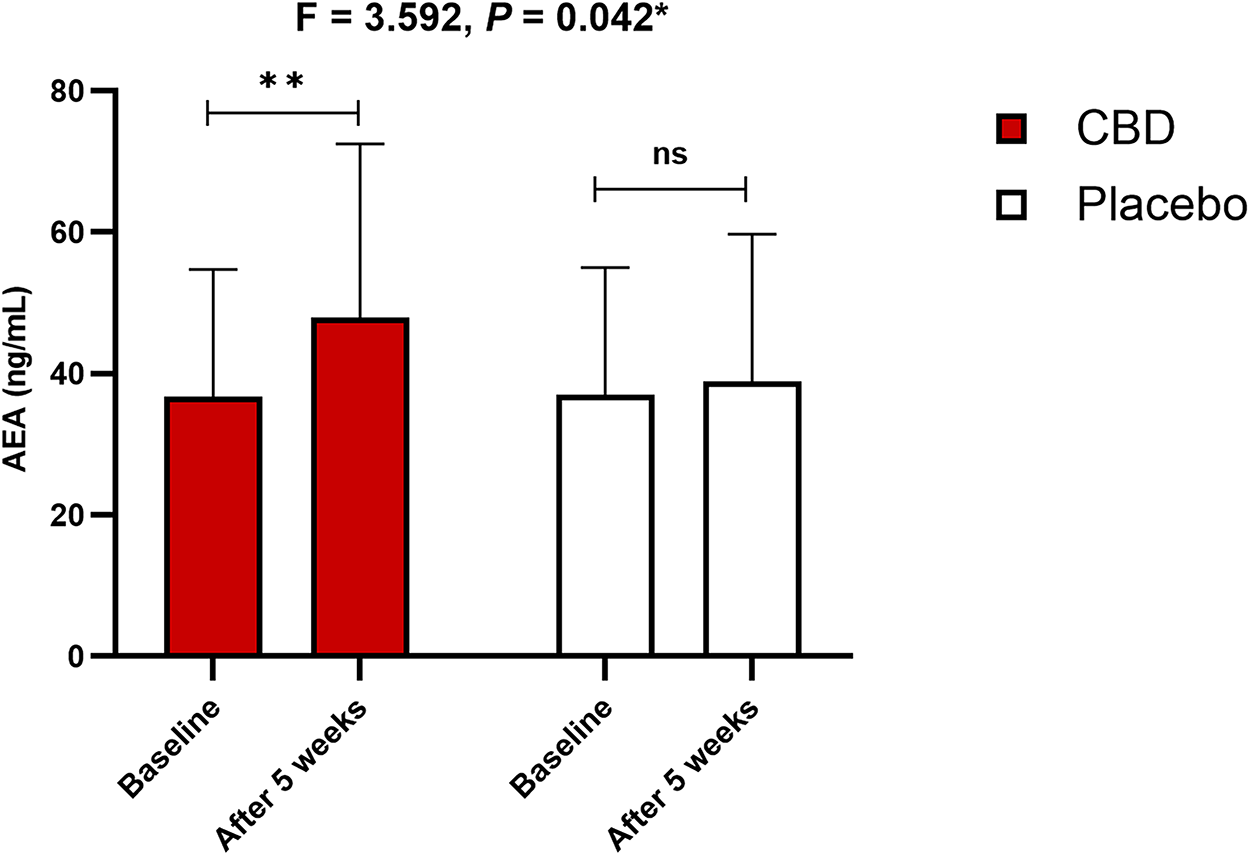
Effect of chronic CBD administration on plasma AEA concentrations. AEA, anandamide; ANOVA, analysis of variance; CBD, cannabidiol. *mixed model ANOVA with post hoc Bonferroni test **p = 0.025.
We previously demonstrated that five weeks of CBD but not placebo administration led to a decrease in BP. Accordingly, we examined whether an increase in CBD-associated AEA might explain the decrease in BP. Firstly, among patients who experienced BP reduction (48 [73%]), 64.6% had an increase in AEA levels. On the other hand, change in AEA levels following CBD administration (ΔCBDAEA) did not correlate with change in systolic BP following CBD administration (ΔCBDSBP) (r = −0.106, p = 0.428). Accordingly, baseline systolic BP did not correlate with ΔCBDAEA (r = 0.004, p = 0.974). Similarly, no correlation was found between ΔCBDAEA and ΔCBDDBP (r = 0.021, p = 0.876) or baseline diastolic BP and ΔCBDAEA (r = 0.088, p = 0.505). To assess whether BP reduction predicts an increase in plasma AEA concentrations, we conducted multiple logistic regression analysis. In the final model, age, BMI, current antihypertensive treatment, and fasting plasma glucose at baseline emerged as significant predictors of AEA increase, while BP reduction did not demonstrate a significant association (Table 2). Unlike baseline glucose values, ΔCBDGlucose showed no correlation with ΔCBDAEA (r = −0.223, p = 0.087). When glucose levels were compared at the study onset and end of the study, a clear reduction was seen (5.3 ± 0.6 vs. 5.0 ± 0.5 mmol/L, p < 0.001). However, no time*treatment interaction was seen between CBD and placebo (F = 0.022, p = 0.883), even when the presence of prediabetes was taken into account (between-subject factor) (F = 0.525, p = 0.471).
Multiple Logistic Regression Analysis of Predictors for Increase in Plasma AEA Concentrations
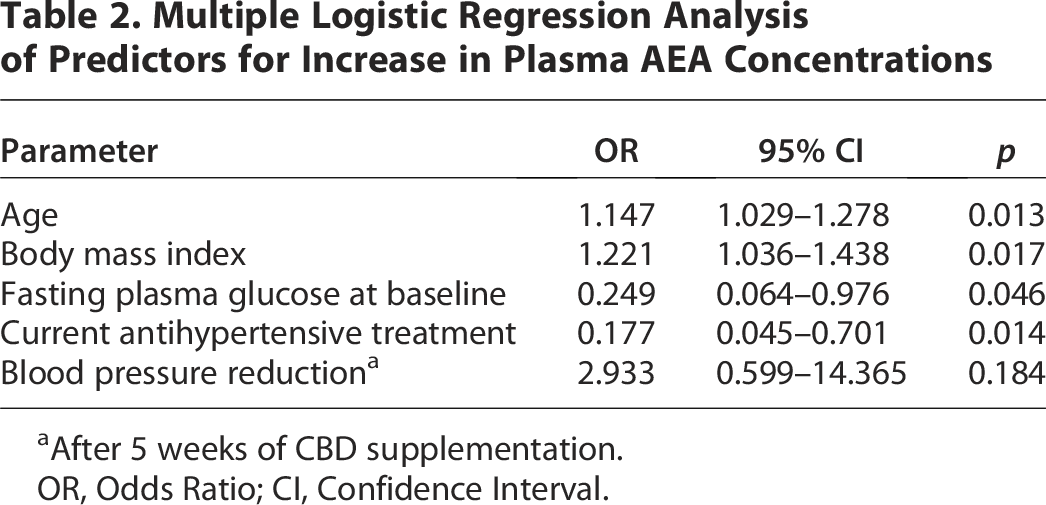
After 5 weeks of CBD supplementation.
OR, Odds Ratio; CI, Confidence Interval.
No significant association was found between chronic CBD administration and 2-AG plasma concentrations (placebo: 28.8 ± 4.3 ng/mL vs. 38.9 ± 20.8 ng/mL; CBD: 36.7 ± 18.0 ng/mL vs. 47.9 ± 24.6 ng/mL; F = 0.513, p = 0.478) (Fig. 2). Finally, no significant correlations were found between concentrations of CBD or its metabolites and 2-AG or AEA, except for correlation between 2-AG and 7-OH-CBD at the end of CBD dosing period (r = 0.365, p = 0.011) (Table 3). However, the association was not retained when age, sex, and BMI were considered (p = 0.160). Similarly, no correlation was established between ΔCBD2-AG and ΔCBDSBP (r = −0.148, p = 0.326), ΔCBD2-AG and ΔCBDDBP (r = −0.229, p = 0.126), or ΔCBD2-AG and baseline systolic or diastolic BP (r = −0.230, p = 0.116 and r = 0.146, p = 0.328, respectively).
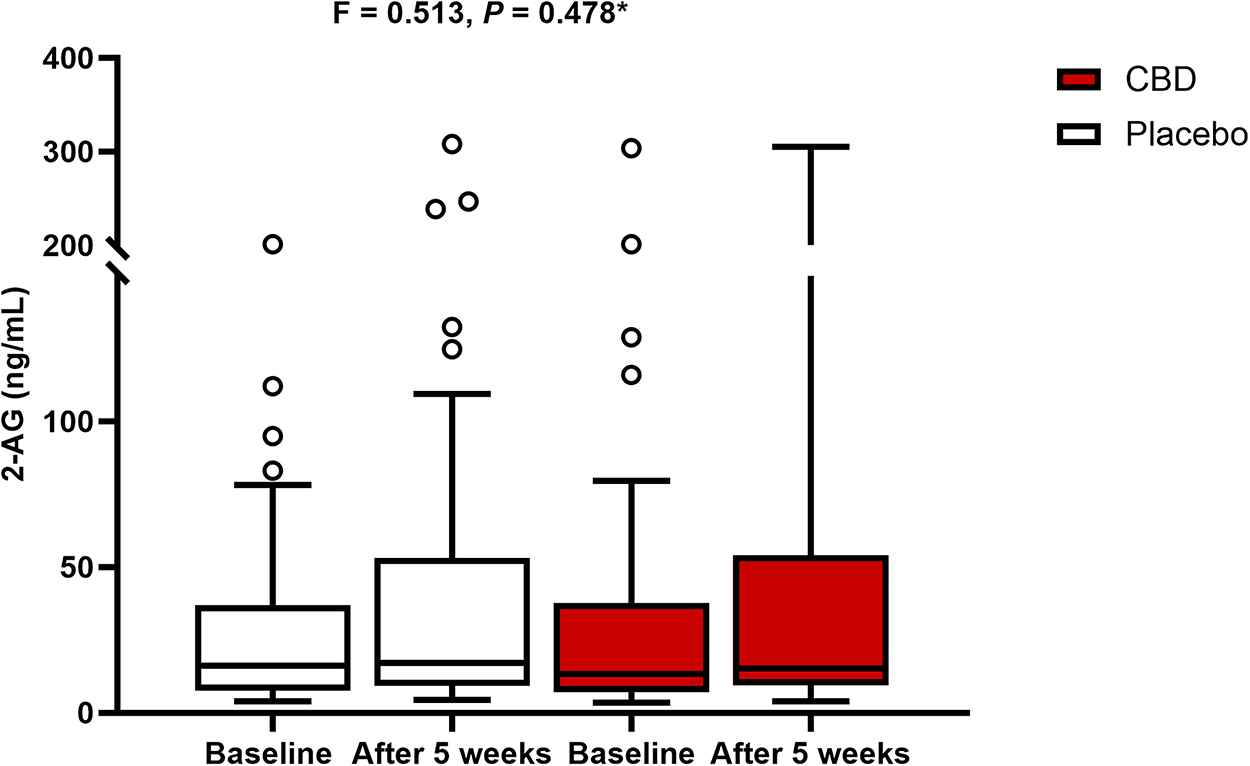
Effect of chronic CBD administration on plasma 2-AG concentrations. 2-AG, 2-arachidonoylglycerol; ANOVA, analysis of variance; CBD, cannabidiol. *Aligned Rank Transform ANOVA.
Correlation Analysis Between Endocannabinoids and CBD and Its Metabolites
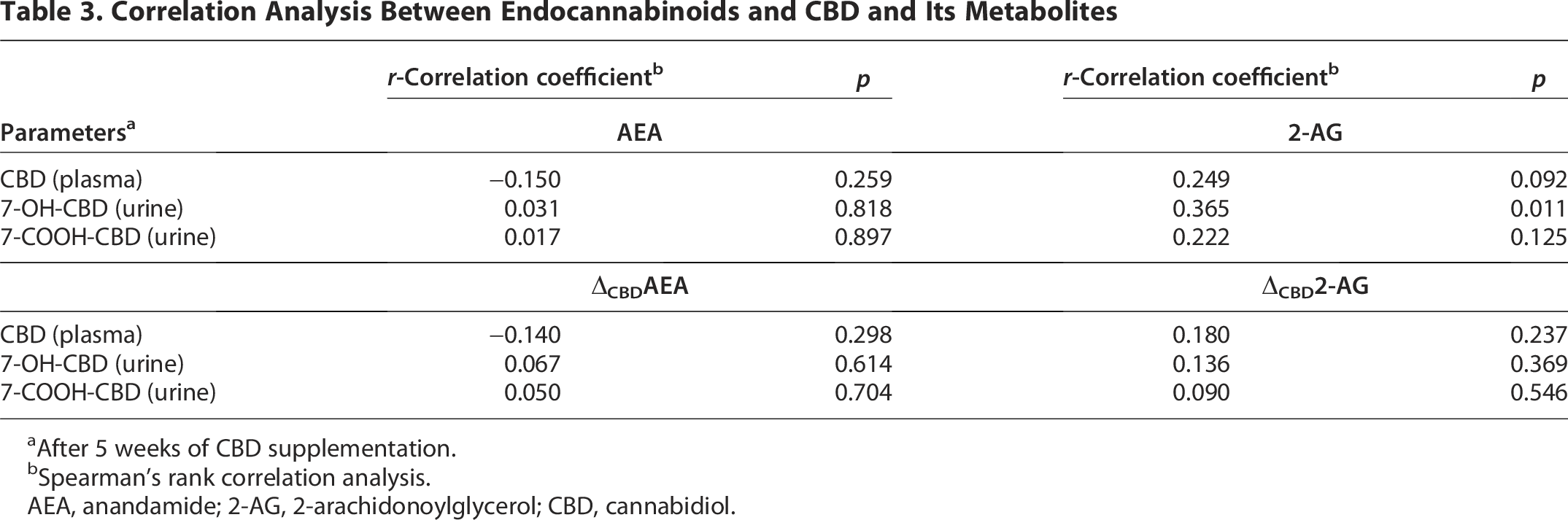
After 5 weeks of CBD supplementation.
Spearman’s rank correlation analysis.
AEA, anandamide; 2-AG, 2-arachidonoylglycerol; CBD, cannabidiol.
Discussion
This study demonstrates that short-term administration of a CBD formulation leads to a significant increase in circulating AEA levels, an effect not observed during the placebo period. Although previous findings from the same cohort indicated that CBD reduces BP, the present analysis suggests that this reduction is not directly mediated by changes in AEA levels. While a majority of participants who experienced a BP reduction also showed increased AEA levels, no direct correlation between changes in AEA and systolic BP was found. In addition, multivariable analysis identified factors such as age, BMI, baseline glucose, and antihypertensive treatment as significant predictors of AEA response, whereas BP changes were not. CBD administration was also associated with a modest reduction in fasting glucose; however, this effect was not significantly different from that observed with placebo and did not interact with glycemic status. Regarding 2-AG, no consistent effect of CBD on plasma levels was detected. Moreover, CBD and its metabolites did not generally correlate with AEA or 2-AG concentrations, apart from a modest association between 2-AG and 7-OH-CBD that was not sustained after adjustment for covariates. To the best of our knowledge, this constitutes the first report on plasma EC dynamics following chronic CBD dosing in patients with hypertension.
The main results of the HYPER-H21-4 trial demonstrated that CBD (up to 450 mg/day) successfully reduced BP after 5 weeks of administration.14,16 However, the pleiotropic nature of CBD and its molecular targets complicates our understanding of the mechanisms underlying the observed reduction, which, in this case, is reflected in the fact that BP reduction could not be explained by the daily dosage of CBD. Focused sub-analyses so far showed that CBD-mediated BP reduction is accompanied by a reduction in serum catestatin, a sympathoinhibitory peptide, and urotensin-II, a potent vasoconstrictor.14,16 In addition, CBD was shown to reduce interleukin (IL)-8, IL-10, and IL-18, but not IL-1β, IL-6, plasminogen activator inhibitor-1, TNF-α, or lectin-like oxidized LDL receptor-1 serum levels, thus implying an immunomodulatory effect of chronic CBD dosing. 17 On the contrary, 4D flow magnetic resonance imaging showed no significant changes in mean flow or pulsatility index for the internal carotid artery upon chronic dosing, despite positive changes in multiple psychological outcomes.22,23
The present results indicate an increase in AEA, but not 2-AG, following CBD supplementation. However, this increase does not appear to be associated with BP reduction, nor with CBD concentrations or its urine metabolites. Specifically, although two-thirds of the patients who experienced a reduction in BP following the intervention also showed an increase in AEA, multivariate analysis revealed that the BP reduction was not independently associated with AEA increase. In animal models and in vitro studies, AEA administration has been shown to reduce BP in a dose-dependent manner, affecting both cardiac contractility and total peripheral resistance.24–29 This CB1 receptor-mediated effect appears more prominent and longer-lasting in hypertensive rats compared with normotensive ones, which aligns with human data, including our observations, where cannabinoid-mediated hypotensive effects were more pronounced in hypertensive individuals.30–35 In this context, a meta-analysis of studies involving healthy humans demonstrated no significant effect of CBD on BP; however, it is important to note that only a few small-scale human studies were included. 36 More recent studies in individuals without cardiovascular disorders suggest that CBD attenuates the BP response during cold pressor tests, improves flow-mediated dilation, and reduces arterial stiffness with repeated dosing, though the BP-lowering effect appears to diminish with continued dosing. It should be noted that these studies focused on acute, rather than chronic, CBD effects.30–35 Nevertheless, it is worth mentioning that a recent study showed that Dahl SS rats chronically treated with AEA exhibited a significant increase in BP, accompanied by increased renal interstitial fibrosis and glomerular damage, raising doubt that prolonged cannabinoid exposure may result in aggravation of hypertension and kidney damage. 37
In line with pre-clinical studies, prior research has shown an increase in AEA following cannabinoid administration in certain populations, 11 though this was not observed in patients with type 2 diabetes mellitus, where a small study reported no significant change in circulating AEA or 2-AG levels after a 13-week dosing regimen. 38 Furthermore, patients already on antihypertensive medications were less likely to exhibit a CBD-mediated increase in AEA, suggesting that prior treatment status may influence the EC response to CBD. The mechanisms by which CBD may elevate AEA levels involve inhibition of intracellular AEA degradation, catalyzed by fatty acid amide hydrolase, and competition for intracellular lipid catabolism.39–41 In addition, in vitro evidence suggests that CBD enhances AEA activity, inhibiting reuptake via the AEA membrane transporter, although this finding remains controversial and requires further in vivo validation. 41 While the role of EC in the pathophysiology of arterial hypertension is not fully understood, evidence suggests that responses to cannabinoid agonists are amplified in hypertension due to increased target-organ sensitivity. 25 Specifically, an upregulation of CB1 receptors has been observed in both the myocardium and the aortic endothelium of hypertensive rats. 25
The observation that fasting plasma glucose levels were reduced when comparing baseline with the end of the study warrants attention. However, as there is no evidence linking these changes to CBD, it is possible that the reduction represents a general treatment effect rather than a CBD-mediated hypoglycemic effect. In addition, we found that patients with elevated fasting plasma glucose were less likely to exhibit a CBD-mediated increase in AEA, independent of age, BMI, use of antihypertensive drugs, or BP reduction. However, the 95% confidence interval is wide, and the significance is marginal, limiting the inference about potential mechanisms. Nevertheless, it is noteworthy that a human trial has demonstrated that Δ9-tetrahydrocannabivarin, but not CBD, may influence glycemic control in patients with type 2 diabetes mellitus. 38 Patients with higher BMI were more likely to show a CBD-mediated increase in AEA, which aligns with evidence suggesting overactivation of the EC system in obesity.42,43 Likewise, older patients were more prone to an increase in AEA, which contrasts with existing data suggesting an age-related decline in EC signaling, particularly in the hippocampal region.44–46 It should be noted, however, that no patients older than 65 were included in our study, so the effect of aging should be interpreted with caution.
Several factors may limit the inferences drawn from the present study. First, the study was conducted in a single center and included only patients of Caucasian descent, which may affect the generalizability of the findings. In addition, the use of a different CBD formulation could potentially have yielded different outcomes. Patients with severe hypertension (SBP ≥ 180 mmHg) and hypertension-mediated organ damage were excluded from the study. Finally, EC levels were measured in blood samples, which may not accurately reflect their concentrations in peripheral tissues, particularly in adrenergic synapses, where their concentrations could be substantially higher.
In summary, our findings indicate that CBD supplementation increased circulating AEA levels, although this increase was not associated with reductions in BP nor with CBD plasma concentrations or its urine metabolites. Notably, patients already treated with antihypertensives, as well as those with higher age and BMI, are more likely to exhibit a CBD-mediated increase in AEA. Regarding 2-AG, no significant changes were observed in circulating 2-AG following CBD administration, although a positive correlation was found between 2-AG and urine 7-OH-CBD levels. Collectively, these findings suggest that although chronic CBD administration appears to affect the EC system, this study provides no conclusive evidence that such alterations explain CBD-mediated BP reduction.
Authors’ Contributions
M.K. participated in conceptualization, methodology, investigation, formal analysis, and original draft preparation. G.D. participated in visualization, investigation, formal analysis, and original draft preparation. J.V. participated in visualization, investigation, formal analysis, and original draft preparation. D.S.D. participated in visualization, investigation, formal analysis, and original draft preparation. Z.D. participated in conceptualization, funding acquisition, resources, project administration, and reviewing and editing of the article. J.B. participated in conceptualization, funding acquisition, resources, project administration, and reviewing and editing of the article.
Footnotes
Ethics Approval and Consent to Participate
Ethics Committee of the University of Split School of Medicine approved this study (15th December 2021, Class: 003-08/21-03/0003; Reg. No.: 2181-198-03-04-21-0091).
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
Lexaria Bioscience Corp. sponsored the study. All authors have full access to all the data and take responsibility for its integrity, as well as the accuracy of the analyses.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.