
Abstract
Introduction:
Retrospective studies and patient surveys investigating cannabis-based products for endometriosis have suggested potential benefits, highlighting the unmet need for effective therapeutic alternatives. This study evaluated the efficacy of cannabidiol in reducing pain among women with surgically treated endometriosis who experienced symptom recurrence.
Materials and Methods:
This was a single-centre, randomised, parallel, triple-blind, placebo-controlled trial. Eligible participants were women with surgically confirmed endometriosis, previously treated surgically, receiving hormonal therapy, and reporting symptom recurrence. A total of 102 participants were randomized (1:1) into two groups, with 51 allocated to oral cannabidiol-enriched oil (CBDO) and 51 allocated to placebo. The intervention lasted 10 weeks. The oil was administered twice daily with dose escalation from 10 mg/day (week 1) to 150 mg/day (week 9), followed by tapering. The study was terminated after the planned interim analysis due to a lack of difference in the primary outcome and a higher frequency of adverse events in the CBDO group. Primary outcomes were changes in pain intensity (Visual Analogue Scale) and the proportion of participants with ≥30% and ≥50% pain reduction. Participants reported their average perceived pain intensity during the preceding week at each visit. Secondary outcomes included sensory thresholds, psychiatric symptoms, functional impairment, quality of life (QoL), and adverse effects, focusing on common cannabidiol-related symptoms.
Results:
Approximately 40% of participants in both groups achieved ≥50% pain reduction, and ∼60% reported ≥30% improvement. At the end of treatment, mean pain intensity was 41.6 mm in the CBDO group and 36.8 mm in the placebo group. Although both groups showed significant within-group reductions, differences between groups were not significant. CBDO was associated with improvements in psychological symptoms and several QoL domains but also with more mild adverse events, mainly gastrointestinal symptoms and perceived weight changes. Participants in the placebo group exhibited better scores in physical QoL domains. No serious adverse events occurred.
Discussion:
Both groups showed consistent and significant pain reduction, but cannabidiol was not superior to placebo. The trial was discontinued at the interim analysis due to the absence of clinically relevant benefit and higher mild adverse-event rates with CBDO. Improvements in placebo-treated participants highlight potential placebo effects and the limited power of secondary analyses.
Introduction
Endometriosis affects approximately 5–10% of women globally,1–4 impacting an estimated 180 million, primarily of reproductive age, though it also occurs post-menopause. 5 It is characterized by endometrial-like tissue outside the uterine cavity and chronic inflammation, yet its definition excludes symptoms or physiological changes. 6 The disease may be present in asymptomatic individuals and up to 24% of those with persistent pelvic pain. 7 It is associated with dysmenorrhea, dyspareunia, dyschezia, and noncyclical pelvic pain, and, beyond physical symptoms, endometriosis reduces quality of life (QoL),8,9 and work productivity, 10 and imposes significant health care and societal costs.11,12
Current guidelines recommend initiating treatment based on a presumptive diagnosis. Hormonal therapy is commonly regarded as the first-line option, offering comparable efficacy to surgery, with lower risks and costs. 13 These therapies primarily act by inhibiting ovulation, reducing serum estradiol levels, and suppressing uterine blood flows, leading to decreased prostaglandin-mediated inflammation, inhibition of menstruation, and cyclic nociception, mechanisms that collectively limit lesion activity and attenuate menstrual-related pain. 14 However, only two-thirds of patients respond adequately, 14 with up to 60% reporting persistent significant pain after one year. 15 Critically, hormonal therapies do not improve fertility outcomes. 16 Laparoscopic excision or ablation remains the standard surgical approach. While surgery may offer temporary relief, it is not curative, 17 and its effectiveness, particularly for superficial lesions, remains debated. 18 Symptom recurrence is common post-surgery; 19 20–30% of women report no relief, 20 with recurrence in 20% by two years and up to 50% by five years. 21 Reoperation rates exceed 30% in the first year and continue to rise over time, 22 underscoring the limitations of lesion-focused and hormone-dependent strategies, especially when no visible lesions are present.
Therapeutic failure and symptom recurrence, along with increasing recognition of the central nervous system’s role in endometriosis-associated pain,23,24 have driven interest in novel treatments such as cannabinoids. 25 Cannabidiol (CBD) stands out for its favorable safety profile 26 and multimodal mechanisms. It acts on inflammatory, opioid, vanilloid, and serotonergic pathways,27,28 as well as ion channels and G-protein-coupled receptors implicated in pain modulation, 29 CBD also interacts with the endocannabinoid system, including modulation of CB1 and CB2 receptor activity and enhancement of endogenous cannabinoid signaling, 30 mechanisms relevant to both peripheral and central pain processing. Beyond these, although its anxiolytic, antidepressant, and neuroprotective effects have been described primarily in preclinical studies and have not yet been confirmed in clinical trials, such properties may still be relevant to the neuropsychiatric symptoms commonly associated with endometriosis. 31 Taken together, these features position CBD as a mechanistically distinct alternative.
From a clinical perspective, retrospective studies and patient surveys suggest potential benefits of cannabis-based products, though these observations remain largely unverified in randomized controlled trials beyond a small number of specific indications. They suggest improvements in cyclical and acyclical pain, sleep, and reduced reliance on conventional analgesics, despite methodological limitations32–37 and some adverse effects, such as tiredness, diarrhea, and changes of appetite/weight. 38 Despite these observations, ongoing confusion between recreational/nonmedical cannabis use and the therapeutic use of cannabinoid-based medicines continues to foster misinformation and stigma. Moreover, although numerous rigorously controlled trials and systematic reviews are now available, they have consistently demonstrated clear therapeutic benefit only in a few narrowly defined indications,39–41 which further limits the reliability and generalizability of the findings reported in retrospective and survey-based studies.
In this context, the primary aim of this study was to evaluate the efficacy of an oral cannabidiol-enriched oil (CBDO), formulated from a full-spectrum hemp extract containing less than 0.3% THC, in reducing pain among women with surgically treated endometriosis who, despite hormonal therapy, experienced symptom recurrence. Secondary objectives include assessing CBDO’s effects on peripheral pain thresholds, psychological symptoms, central sensitization, catastrophizing, QoL, and the occurrence of adverse events.
Materials and Methods
This was a single-center, randomized, parallel, triple-blind, placebo-controlled trial, approved by the Research Ethics Committee of the Ribeirão Preto Medical School Hospital, University of São Paulo (process number 5.868.049). It was registered with the national ethics system (CAAE: 47489321.0.0000.5440), which includes both the local Research Ethics Committee (CEP) and the Brazilian National Research Ethics Commission (CONEP), as well as on ClinicalTrials.gov (NCT 05670353). All participants provided written informed consent. The trial followed established clinical pain research guidelines 42 and adhered to CONSORT standards, 43 including its extension for pain intervention trials. 44
Eligible participants were women aged 18 years or older with a diagnosis of chronic pelvic pain (CPP), defined according to the International Association for the Study of Pain (IASP) [https://www.iasp-pain.org/publications/free-ebooks/classification-of-chronic-pain-second-edition-revised/] and the ReVITALize [https://www.acog.org/practice-management/health-it-and-clinical-informatics/revitalize-gynecology-data-definitions] initiative led by the Royal College of Obstetricians and Gynaecologists. All had surgically confirmed endometriosis and prior surgical therapy, followed by continuous hormonal treatment.
Recurrent pain was required ≥6 months after surgery (following initial symptom relief), with a mean pain score ≥4 on the numerical rating scale (NRS), 45 and a cumulative pain score ≥24 across the six days preceding randomization. Recent transvaginal ultrasound findings (within one month prior to recruitment) were reported and not used for participant eligibility. Previous diagnosis was based on visual criteria for typical lesions 46 and histopathology for atypical lesions, and women were included regardless of disease stage, given the lack of correlation with symptom severity. 47 Additional eligibility criteria were complete removal/destruction of all endometriotic lesions in a single surgical procedure and agreement to randomization, exclusive study participation (i.e., not being concurrently enrolled in any other clinical study), daily phone access, and written informed consent.
Exclusion criteria encompassed use of CBD-interacting medications (e.g., chloroquine, clobazam, warfarin, valproic acid), prior cannabinoid intolerance, inability to take oral medication, pregnancy or breastfeeding, cannabis use in the past three months, lifetime cannabis dependence, substance abuse, or severe chronic conditions. Specifically excluded were insulin-dependent diabetes, uncontrolled hypertension, respiratory diseases, hematological, hepatic, and renal (grades 3–5) and metabolic disorders, and immunosuppression.
Setting
Participants were recruited from the Pelvic Pain Outpatient Clinic at HCFMRP-USP, a tertiary care center within Brazil’s Unified Health System (SUS).
Intervention
Participants were randomized (1:1) to receive a CBDO solution (33 mg of CBD per milliliter in an oily medium-chain triglyceride [MCT] vehicle) or a matching placebo (MCT oil without cannabinoids). The CBDO consisted of a purified preparation derived from a full-spectrum hemp extract, containing CBD as the major cannabinoid and less than 0.3% THC, with only trace amounts of other naturally occurring cannabinoids. Both groups self-administered the oil twice daily for 9 weeks, following an identical titration schedule.
In the CBDO group, dosing began at 10 mg/day (week 1) and increased weekly to 20 mg (week 2), 30 mg (week 3), 40 mg (week 4), 50 mg (week 5), 100 mg (weeks 6 to 7), and 150 mg/day (weeks 8 to 9). The initial 10 mg dose corresponded to approximately three drops of the CBDO solution, delivered via a dropper bottle to facilitate accurate administration. This conservative starting dose followed the commonly adopted “start slow, go slow” titration approach used in clinical cannabinoid therapy to optimize tolerability. 48 Participants could stabilize their dose if clinical improvement was sustained. In week 10, the dose was tapered by 10–50 mg every two days. The placebo group underwent a simulated dose escalation mirroring this schedule.
Dosage was determined by local/international expert consensus. 49 Participants took the investigational product/placebo with meals, continued hormonal therapy, and were permitted nonsteroidal anti-inflammatory drugs for adjunct symptom relief. We selected the oral route because it offers practical advantages for adherence, safety, and dosing consistency in outpatient chronic pain trials, despite its known pharmacokinetic limitations. Participants were instructed to take the study medication with meals to minimize variability in CBD absorption. Because of CBD’s lipophilicity and the known enhancement of absorption with dietary fat, participants were instructed to take the investigational product together with a small fatty snack (e.g., yogurt) to optimize consistency in absorption. Adherence was calculated by pre- and posttrial bottle weight measurements, recorded in a dispensation form.
Outcomes
Primary outcomes included changes in pain intensity, assessed via the Visual Analogue Scale (VAS, 0–100 mm), and the proportion of participants reporting ≥30% or ≥50% pain reduction, thresholds recommended by the IMMPACT group 50 for clinically meaningful improvement in chronic pain trials and still endorsed in contemporary guidance. 51 After randomization, participants rated their average perceived pain intensity during the preceding week at each weekly visit. Participant ratings of overall improvement were assessed by the Patient Global Impression of Change scale and classified as having “improved” if they reported very much, much, or minimal improvement.
Secondary outcomes comprised thermal pain thresholds (heat and cold), psychological symptoms using the Generalized Anxiety Disorder 7-item scale (GAD-7) 52 the Patient Health Questionnaire (PHQ-9), 53 pain catastrophizing symptoms using the Pain Catastrophizing Scale (PCS), 54 central sensitization assessed with the Central Sensitization Inventory, 55 and QoL measured using the WHOQOL-BREF instrument [https://www.who.int/tools/whoqol/whoqol-bref/docs/default-source/publishing-policies/whoqol-bref/portuguese-brazil-whoqol-bref]. Thermal thresholds were measured using the DFNS protocol developed by the German Research Network on Neuropathic Pain with the TSA-II Neurosensory Analyzer (MEDOC®, 2005), applying the method of limits. Participants indicated when warmth or cold was first perceived and when it became painful. This method has demonstrated strong reliability and reproducibility across centers. 56
Adverse effects were assessed systematically using the UKU Side Effect Rating Scale 57 and the CBD-specific CARE Scale. 58 Laboratory evaluations (bilirubin, ALP, gamma-glutamyl transferase, aspartate aminotransferase, aspartate aminotransferase) were performed at baseline, week 5, and week 9. Plasma CBD/THC levels were measured at baseline and weeks 2, 6, and 10.
Baseline cohort characterization included body mass index (BMI), heart rate, blood pressure, stress symptoms measured using the Impact of Event Scale, 59 posttraumatic stress disorder assessed with the Posttraumatic Stress Disorder Checklist, 60 history of childhood trauma evaluated using the Childhood Trauma Questionnaire, 61 and self-reported comorbidities (migraine, anxiety, depression, irritable bowel syndrome, hypersensitivity, temporomandibular dysfunction, fibromyalgia, cervicalgia, restless leg syndrome, and chronic fatigue).
Sample size estimation
The sample size calculation was based on VAS pain scores. For the primary pain outcome (two-sample t-test), 51 participants per group were required to detect an effect size of 0.5 with 80% power and a one-sided α = 0.05. For the ≥30% and ≥50% pain relief outcome, 33 participants per group were required, assuming a placebo response ≤30% and a treatment response ≥50% (α = 0.05). This yielded an initially planned total sample size of 102 participants.
Randomization and blinding
Participants were allocated via dynamic adaptive randomization based on sample minimization, 62 stratified by disease stage to ensure balanced group distribution (1:1 ratio), using R software and the Minirand package. Allocation concealment was strictly maintained, with irreversible randomization post-assignment. Each participant received a unique study ID and two-digit code for pharmacy-controlled dispensation. Blinding was enforced for participants, clinicians, nursing/laboratory staff, researchers, and data analysts. Only the unblinded pharmacist prepared treatments, safeguarding study integrity while ensuring accurate dispensation.
Statistical analysis
Data were collected and managed via REDCap, adhering to international standards, and securely stored until anonymized posttrial export. Clinical and demographic variables were compared using t-tests (normally distributed continuous), Mann-Whitney U (non-normal), and chi-square (categorical). Spearman’s correlation assessed pain-thermal threshold relationships.
Analyses followed a modified intention-to-treat principle. Two participants were excluded immediately after randomization due to dispensing error, before receiving any effective exposure or providing outcome data. All remaining randomized participants completed follow-up. Minor variations in visit timing (1–3 days) were handled within the mixed-effects framework.
Pain intensity (VAS, mm) was analyzed via linear mixed-effects models (lme4 package), with treatment group and follow-up week (fixed effects) and participant-specific random intercepts. Adjusted marginal means (emmeans package) estimated weekly pain reduction (baseline vs. follow-up), with Cohen’s d effect sizes.
Proportional pain reduction (≥30% and ≥50%) was modeled via generalized linear mixed-effects (glmer, logit link), incorporating group-week interactions and random intercepts. Predicted probabilities (inverse logit) were compared as prevalence ratios (relative risks) for binary outcomes; continuous outcomes reported mean differences (95% CIs). Analyses used R software, with maximum likelihood estimation.
Results
A prespecified interim analysis (O’Brien-Fleming method,63,64 α = 0.025) was conducted after 50 participants (25 per group), revealing no clinically meaningful superiority of the intervention over placebo for primary outcomes and higher adverse event rates. The external supervisory board, research team, and local ethics committee collaboratively terminated the trial early, following prespecified stopping criteria in the approved protocol, to avoid unnecessary exposure to potential adverse effects without clear therapeutic benefit.
Patient characterization
Baseline characteristics are detailed in Table 1, with both groups showing comparable profiles. Treatment adherence was high, confirmed by the return of empty bottles, except for one participant in the CBDO group (73.8%) and two in the placebo group (97.2% and 97.8%). All participants had undetectable baseline plasma CBD levels. CBD concentrations increased significantly at weeks 2, 6, and 10 (t = 3.135, p = 0.004), with median (IQR) values of 2.00 (0.68), 4.69 (2.99), and 5.98 (2.65) ng/mL, respectively. THC remained undetectable throughout the study.
Demographic and Clinical Characteristics of the Participants Included in the Study
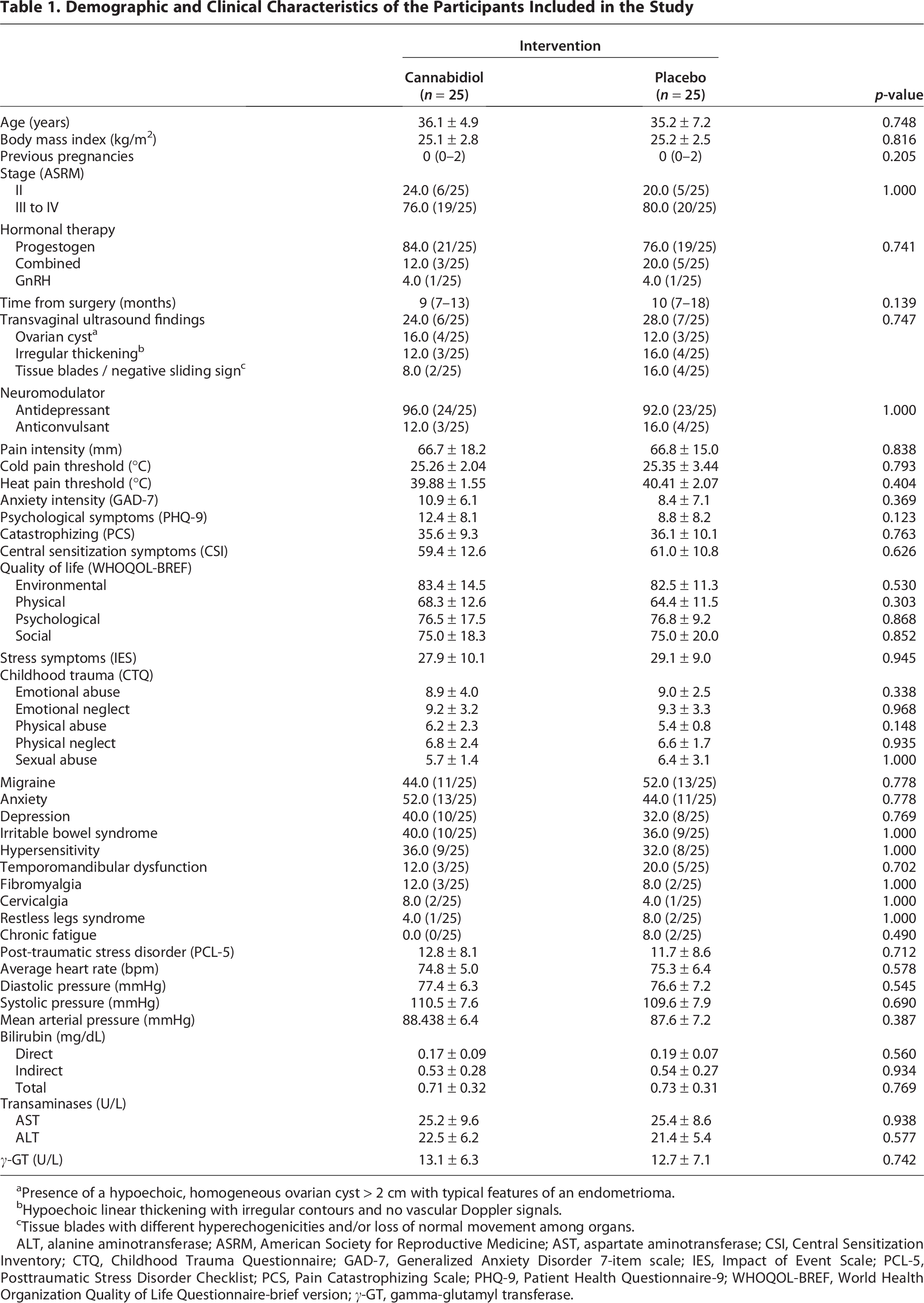
aPresence of a hypoechoic, homogeneous ovarian cyst > 2 cm with typical features of an endometrioma.
bHypoechoic linear thickening with irregular contours and no vascular Doppler signals.
cTissue blades with different hyperechogenicities and/or loss of normal movement among organs.
ALT, alanine aminotransferase; ASRM, American Society for Reproductive Medicine; AST, aspartate aminotransferase; CSI, Central Sensitization Inventory; CTQ, Childhood Trauma Questionnaire; GAD-7, Generalized Anxiety Disorder 7-item scale; IES, Impact of Event Scale; PCL-5, Posttraumatic Stress Disorder Checklist; PCS, Pain Catastrophizing Scale; PHQ-9, Patient Health Questionnaire-9; WHOQOL-BREF, World Health Organization Quality of Life Questionnaire-brief version; γ-GT, gamma-glutamyl transferase.
Participant flow
A CONSORT diagram summarizing screening, exclusions, randomization, follow-up, and analysis is presented in Figure 1.
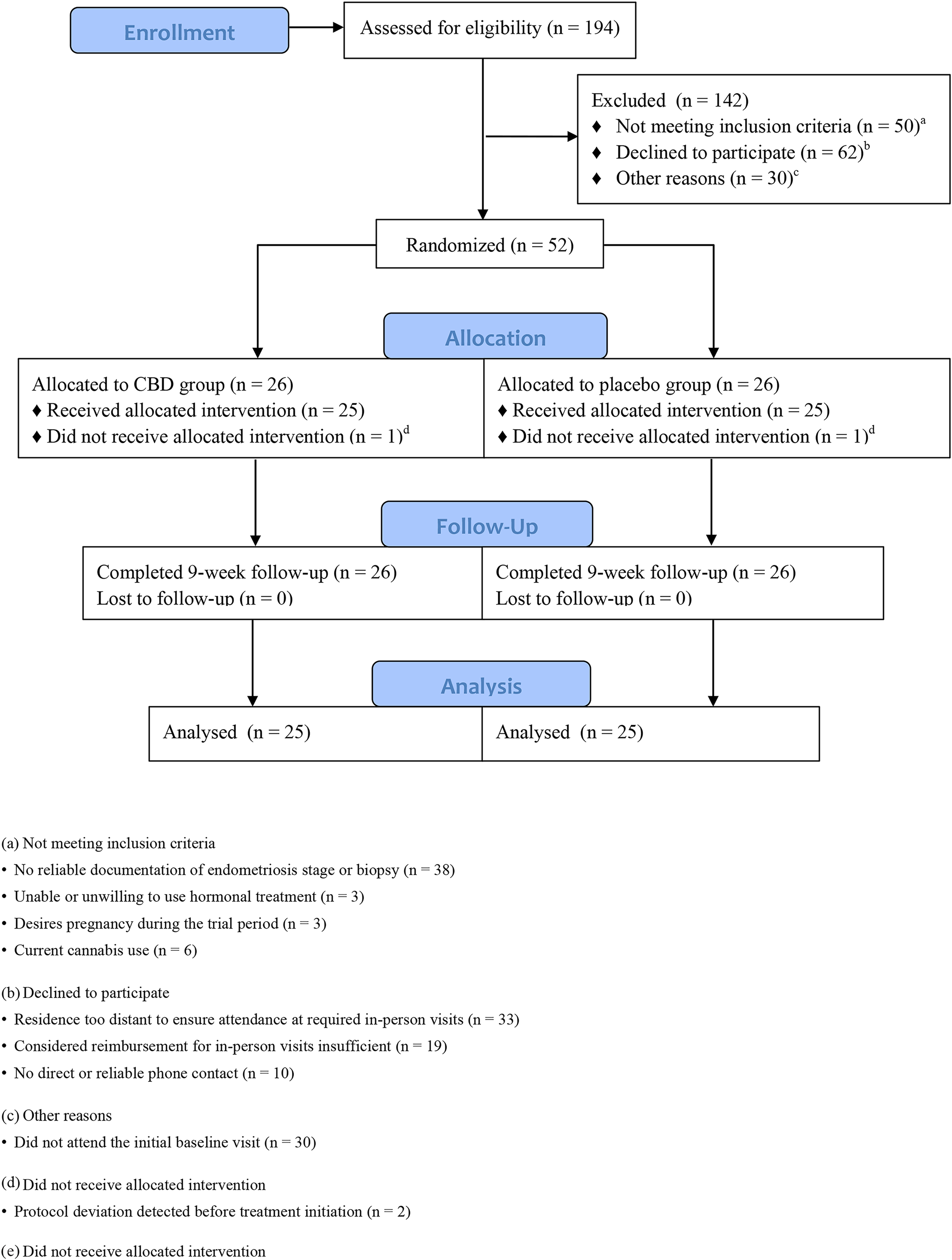
CONSORT flow diagram of participant screening, randomization, follow-up, and analysis.
Pain intensity
Clinical improvement was reported in both groups by the end of the treatment. In the CBDO group, 60% (15/25) of participants reported a meaningful improvement, while in the placebo group, this number was 72% (18/25). The difference between the groups was not statistically significant (p = 0.370). Mean final pain intensity was 41.6 mm in the CBDO group and 36.8 mm in the placebo group (Fig. 2A). A ≥30% pain reduction was observed in 68% (17/25) of CBDO-treated participants and 64% (16/25) of those receiving placebo (Fig. 2B), while 40% in each group achieved ≥50% reduction (Fig. 2C). As shown in Figure 2, both CBDO and placebo groups exhibited statistically significant within-group reductions in pain across all weeks. However, no significant between-group differences were observed at any time point.

Pain intensity variation over time according to intervention.
Thermal pain thresholds
In the placebo group, the mean threshold difference for cold stimuli between the pre-intervention period and the tenth week of treatment was −1.1°C (95% CI: −3.1–1.0; p = 0.291). In the CBDO-treated group, the mean difference was 0.2°C (95% CI: −1.5–1.8; p = 0.849). For heat stimuli, the CBDO-treated group showed a mean threshold difference of 0.9°C (95% CI: −0.4–2.3; p = 0.166). In contrast, the placebo group demonstrated a slight increase in the threshold, with a mean difference of 1.3°C (95% CI: 0.2–2.5; p = 0.028). No significant correlation was observed between the reduction in pain intensity and pain thresholds for heat stimuli (placebo group: ρ = −0.02, p = 0.925; CBDO group: ρ = 0.02, p = 0.923) or cold stimuli (placebo group: ρ = −0.05, p = 0.824; CBD group: ρ = 0.12, p = 0.562).
Psychological symptoms
Participants treated with CBDO demonstrated significant posttreatment improvements in psychiatric symptom scores, as measured by the PHQ-9 (12.4 ± 8.1 vs 4.4 ± 8.1, p < 0.001) and GAD-7 (10.3 ± 6.1 vs 3.7 ± 6.1, p < 0.001). These findings were not observed in the placebo-treated group, where no significant changes were detected (PHQ-9: 8.8 ± 8.2 vs 7.8 ± 8.2, p = 0.627; GAD-7: 8.4 ± 7.1 vs 7.2 ± 7.1, p = 0.430).
Central sensitization
Both groups demonstrated significant reductions in central sensitization scores (CBDO: 59.4 ± 12.6 vs 41.0 ± 12.6, p < 0.001; placebo: 61.0 ± 10.8 vs 47.0 ± 10.8, p < 0.001). However, the scores between the groups remained comparable (p = 0.076).
Catastrophizing
Both groups showed significant reductions in pain catastrophizing scores (CBDO: 35.6 ± 9.3–24.8 ± 9.3; placebo: 36.2 ± 10.1–26.5 ± 10.1; p < 0.001 for both). Final scores did not differ significantly between groups (p = 0.508).
Quality of life
Within-group analyses showed that participants in the placebo group experienced a significant improvement only in the QoL physical domain (64.4 ± 11.5 vs. 75.0 ± 11.5, p < 0.001), with no meaningful changes in the psychological (76.8 ± 9.3 vs. 79.8 ± 9.3, p = 0.169), social (75.0 ± 20.0 vs. 85.0 ± 20.0, p = 0.045), or environmental domains (82.5 ± 11.3 vs. 84.9 ± 11.3, p = 0.234). In contrast, the CBDO group demonstrated significant improvements in the physical (68.3 ± 12.6 vs. 80.3 ± 12.6, p < 0.001), psychological (76.5 ± 17.5 vs. 83.3 ± 17.5, p = 0.017), and social domains (75.0 ± 18.3 vs. 88.0 ± 18.3, p < 0.001) but not in the environmental domain (83.4 ± 14.5 vs. 85.3 ± 14.5, p = 0.420).
Side effects
Cannabidiol-enriched treatment was significantly more frequently associated with vomiting (8.0% vs. 0.4%, p = 0.001), weight gain (10.0% vs. 2.0%, p = 0.023), and reduced taste (3.2% vs. 0.4%, p = 0.009). In addition, trends towards higher rates of nausea (20.4% vs. 9.6%, p = 0.029) and decreased appetite (10.0% vs. 4.0%, p = 0.048) were observed, although these did not reach the predefined threshold for statistical significance in interim analysis.
Between weeks 3 and 6, when there was a greater apparent effect size of the placebo treatment, we observed a tendency for a direct and inverse correlation between the intensity of side effects and perceived pain intensity in participants treated with placebo (ρ = −0.454, p = 0.034). No such trend was observed in the CBDO group (ρ = –0.09, p = 0.686).
Because the trial was terminated early, the reduced sample size limits the statistical power of the secondary analyses. These findings should therefore be interpreted as exploratory.
Discussion
Our study reveals a significant reduction in pain intensity across all follow-up weeks of treatment, irrespective of treatment condition. Most reduction occurred in week two by both the CBDO and placebo groups. By study end, nearly 40% of participants maintained ≥50% reduction in symptoms, and 60% maintained ≥30% improvement. No significant disparity in efficacy developed across groups to mark an overall disparity in efficacy over time and independently of intervention. Interestingly, subjects treated with CBDO showed improvement in psychological symptoms and multiple QoL domains. However, those in the placebo group also showed better scores in the physical QoL domain, which underlines the importance of non-pharmacologic variables in influencing patient-reported data. Such an event may be attributed to alterations in expectation-related symptoms, whereas CBDO was associated with broader but mild QoL improvements. These results together suggest the importance of placebo responses in endometriosis-related pain trials, as well as secondary outcomes in this prematurely stopped study.
The results emphasize the significant role of the placebo response, an already established variable in randomized trials in connection to pain.65,66 At least part of the improvement probably mirrors non-specific effects through virtue of expectation, classical conditioning, regression to the mean, the Hawthorne effect, and response bias. 67 The expectancy associated with CBD may influence subjective as well as physiological outcomes, particularly among individuals anticipating benefit. 68 Although a recent systematic review found only sparse and low-certainty evidence suggesting potential anxiolytic or antidepressant effects of cannabinoids compared with placebo, 69 these psychological benefits did not translate into enhanced analgesia in our investigation.
Conversely, the lessebo effect, defined by a reduced therapeutic response by virtue of awareness of possible assignment to placebo, may have further reduced the differences detected between groups. 70 Expectations may likewise have contributed to short-term improvement, previously observed and now confirmed in investigations of stress modulation by CBD. 71 This effect will probably be enhanced by the myriad reports in the media on cannabinoids, 72 and frequent contact with research staff may have enhanced feelings of support and treatment believability. Together, these factors are consistent with the expectancy model proposed by Rief and Petrie. 73 However, while these mechanisms may help contextualize participants’ subjective experiences, the principal finding of this trial is that CBDO did not demonstrate superiority over placebo for pain reduction.
Although a numerical difference in baseline PHQ-9 scores was observed, it did not reach statistical significance because of large within-group variance. This heterogeneity reduces the likelihood that depressive symptoms substantially confounded treatment effects, yet it does not entirely preclude the possibility that subtle residual mood differences—combined with limited power to detect such small effects—could have contributed to the slightly greater improvements observed in the CBDO group. Any such explanatory framework should therefore be interpreted cautiously and considered secondary.
Furthermore, CBDO in our study did not present a significant change in thermal pain thresholds. This result is in agreement with recent academic literature, which, despite mixed results, usually correlates CBDO with mild increases in pain thresholds and tolerance and reduced pain unpleasantness but lacks to show uniform decreases in pain intensity. 74
The apparent inconsistency with the clinically reported improvement by in natura cannabis consumers32–37 may be owing to THC-CBD interactions: inhaled cannabis containing THC increases pressure pain thresholds, whereas CBD may attenuate THC’s analgesic efficacy in chronic pain populations such as in the case of fibromyalgia. 75
Other than the above-mentioned pharmacodynamic considerations, there are other pharmacokinetic considerations that could result in the conflicting results. Oral bioavailability of CBD may be low due to the first-pass effects on the liver with sluggish onset of action, whereas higher peak levels may be reached more rapidly with inhalation or oromucosal preparations. This could result in potentially poor analgesic effects with the principal method of administration used by persons using cannabis for recreation or medicinal purposes. 48
While no adverse event was serious, CBDO had higher-rate side effects, particularly gastrointestinal symptoms and self-reported weight change compared to placebo. Comparable but less severe effects in the placebo arm could be attributable to the common MCT oil vehicle or to an amplification by nocebo effect of anticipated side effects. 76 A theoretical pharmacokinetic interaction between CBD and coadministration of hormone therapies because of shared pathways in the cytochrome P450 enzyme system cannot be ruled out; 77 a clinical trial is currently investigating this possibility for oral contraceptives (NCT04396730). 78 Nevertheless, at standard oral dosing levels for CBD, meaningful interactions have not been established at this point in time, while the profile of side effects established is supportive of its safety profile. 38 The reciprocal relationship between side effect severity and pain perception in the placebo arm again highlights expectancy and treatment environment as determinants, as has been recorded in other investigations. 79
The inability to show superiority to placebo of CBDO has clinical implications, as cannabis-based products are in general use without robust evidence. Caution is required in the endorsement of CBD and especially in CPP, in whose therapy benefits may be smaller than adverse effects. The higher incidence of adverse effects, even if mild, is an issue in long-term use, backed by a Danish cohort study associating cardiac arrhythmias and medicinal cannabis. 80
Our trial joins the expanding literature on CBDO in CPP in endometriosis in emphasizing the interrelation of treatment outcomes and expectation effects. Its limitations include early termination, interim analysis, and the absence of formal expectation measurement, factors that are particularly relevant given the possibility that high expectation may obscure true differences. 81 Although no formal tool was employed, participants provided retrospective considerations of their pain experiences at trial end and spontaneous comments possibly related to overarching constructs such as hope. 82 Future studies should incorporate explicit expectation measures to better clarify their influence on outcomes.
A further limitation is that of reduced statistical power due to early study termination. While some of the secondary results indicated possible trends of interest, it is clear that the actual sample size achieved is much smaller than what was planned, so that any conclusions drawn from them, including this report, remain speculative at best. Future studies of adequate size will be needed to determine whether what is observed here reflects genuine therapeutic effects as opposed to merely study size-related artifacts.
An additional limitation is that meals were not formally standardized. Given the lipophilicity of CBD and the influence of dietary fat on its bioavailability, variability in participants’ food intake may have contributed to heterogeneity in systemic exposure despite our instruction to take the product with a small fatty snack.
Regulatory variability around products derived from cannabis is equally applicable. 83 In Brazil, even with recent advances, CBD is very controlled, requiring prescription by a doctor, clinical rationalization, and expensive importation by virtue of the nonexistence of local production. 84 These constraints shaped our study design, limiting eligibility to individuals with prior surgical and hormonal treatment to manage endometriosis-associated pain.
CBDO at tested doses did not surpass placebo at pain but enhanced psychological symptoms and QoL, highlighting the multifaceted burden of CPP. These secondary benefits imply cannabinoids as adjuncts to psychosocial features of endometriosis even in the absence of direct pain attenuation. This apparent paradox reinforces widening trial endpoints to pain intensity plus functional and psychological parameters. Future investigations should consider dose escalation and CBD:THC ratios, as THC may complement CBD in endometriosis-related pain through its partial agonism of CB1 receptors, which directly reduces nociceptive transmission, whereas CBD primarily modulates inflammatory pathways, TRPV1 activity, and serotoninergic signaling. 85 These complementary mechanisms support examining balanced CBD:THC ratios in future trials and undertaking multimodal strategies combining cannabinoids with evidence-based therapies while addressing ethical, economical, and regulatory impediments to safe and equitable translation.
Conclusion
In conclusion, though CBDO did not show superiority over placebo in pain alleviation from recurrent pain, its relationship with psychological well-being and quality-of-life enhancement reveals a complex therapeutic potential. For the present, until robust evidence clarifies these benefits, we recommend restricting cannabis-based therapies to regulated scientific environments within specialist centers. Application in the clinic, if considered, should follow exhaustive conventional options and occur within ethically guided, multidisciplinary care frameworks emphasizing patient safety, transparency, and whole support. Further investigation into optimized formulations and multimodal therapy is essential in fostering equitable, evidence-based management of this profoundly complex disorder.
Authors’ Contributions
G.B.A.: Conceptualization (lead); methodology (lead); investigation (lead); writing—original draft (lead); writing—review and editing (equal). R.R.: Investigation (lead); data curation (supporting); project administration (supporting); and writing—review and editing (equal). I.G.C.O.: Methodology (lead); validation (supporting); and writing—review and editing (equal). I.D.S.: Methodology (supporting); validation (lead); and writing—review and editing (equal). J.A.S.C.: Conceptualization (supporting); methodology (supporting); project administration (lead); formal analysis (supporting); writing—original draft (supporting); and writing—review and editing (equal). J.E.C.H.: Conceptualization (supporting); methodology (supporting); project administration (lead); formal analysis (supporting); writing—original draft (supporting); and writing—review and editing (equal). M.E.Q.N.: Investigation (supporting); data curation (supporting); and writing—review and editing (equal). A.A.N.: Formal analysis (supporting); visualization (supporting); and writing—review and editing (equal). A.W.Z.: Formal analysis (supporting); visualization (supporting); and writing—review and editing (equal). W.M.J.: Investigation (supporting); resources (supporting); and writing—review and editing (equal). J.C.R.S.: Investigation (supporting); resources (supporting); and writing—review and editing (equal). O.B.P.-N.: Conceptualization (lead); methodology (lead); formal analysis (lead); project administration (lead); writing—original draft (supporting); writing—review and editing (equal); and supervision (lead).
Footnotes
Acknowledgments
The authors gratefully acknowledge the University of São Paulo for their academic support. In addition, the authors also thank: the Coordination for the Improvement of Higher Education Personnel-Brazil (CAPES) for their support of our Postgraduate Program; The Clinical Research Unit at Hospital das Clínicas of the Ribeirão Preto Medical School of the University of São Paulo (HCFMRP-USP), the Cannabinoid Research Center of the Ribeirão Preto Medical School of the University of São Paulo (FMRP-USP), the Laboratory of Electroneuromyography at HCFMRP-USP, and the Laboratory of Analytical Instrumentation and Chromatographic Techniques and Mass Spectrometry from the Department of Chemistry of the Faculty of Philosophy, Sciences and Letters at Ribeirão Preto, University of São Paulo for infrastructure support; finally, the authors especially thank Mr. Oswaldo Mazini Junior for his kindness in measuring pain perception thresholds and acknowledge all participants of the DREAMLAND trial and all professionals involved for their excellent work in building and maintaining the database.
Author Disclosure Statement
O.B.P.N. and J.C.R.S. serve as a non-remunerated board member of the Brazilian Society of Endometriosis and Minimally Invasive Gynaecology (SBE). J.A.S.C. and J.E.C.H. are the coinventors of the patent “Fluorinated CBD compounds, compositions, and uses thereof, Pub. No.: WO/2014/108899, International Application No.: PCT/IL2014/050023”, Def. U.S. number Reg. 62193296; 29 July 2015; INPI on 19 August 2015 (BR1120150164927; Mechoulam R, Zuardi AW, Kapczinski F, Hallak JEC, Guimarães FS, Crippa JAS, Breuer A). Universidade de São Paulo (USP) has licensed this patent to Phytecs Pharm (USP Resolution No. 15.1.130002.1.1). It has an agreement with Prati-Donaduzzi to “develop a pharmaceutical product containing synthetic CBD and prove its safety and therapeutic efficacy in the treatment of epilepsy, schizophrenia, Parkinson’s disease, and anxiety disorders”. J.A.S.C., and J.E.C.H. are the coinventors of the patent “Cannabinoid-containing oral pharmaceutical composition, method for preparing and using the same”, INPI on 16 September 2016 (BR 112018005423-2). J.A.S.C. was a consultant and/or has received speaker fees and/or sits on the advisory board and/or receives research funding and/or receives speaker fees from Janssen-Cilag, Torrent Pharm, Ease Labs Pharm, Prati-Donaduzzi, Mantecorp, ArtMed, PurMed Global, EaseLabs Pharm, FQM-Pharm, BioBrains, and BSPG Pharm over the past 5 years. J.A.S.C. is a member of the International Advisory Board of the Australian Center for Cannabinoid Clinical and Research Excellence (ACRE)-National Health and Medical Research Council (NHMRC). The remaining authors have no competing interests to declare for this study. The authors received no financial support for the authorship.
Funding Information
This study was supported by the University of São Paulo (USP); the Coordination for the Improvement of Higher Education Personnel—Brazil (CAPES); the Foundation for Support to Teaching, Research, and Assistance of the Hospital das Clínicas, Ribeirão Preto Medical School, University of São Paulo (FAEPA); and the São Paulo Research Foundation (FAPESP; grant no. 2021/10765-0). Additional support was provided through a grant from the National Institute of Science and Technology—Translational Medicine (INCT-TM), research fellowships from the National Council for Scientific and Technological Development (CNPq; Drs Crippa and Hallak), and in-kind donations of cannabidiol from GreenCare Pharm (São Paulo, Brazil).
Ethics Approval and Consent to Participate
The study was approved by the Research Ethics Committee of the Hospital das Clínicas of the Ribeirão Preto Medical School (process number 5.868.049), and registered on the National Research Ethics Committee (CAAE: 47489321.0.0000.5440).
Attestation Statement
The subjects in this trial have not concomitantly been involved in other randomized trials, data regarding any of the subjects in the study has not been previously published and data will be made available to the editors of the journal for review or query upon request.
Data Sharing Statement
The data that support the findings of this study are available from the coordinator, [OBPN], upon reasonable request.