
Abstract
Background:
Cannabinoid hyperemesis syndrome (CHS) is increasingly being observed in emergency departments and is characterized by recurrent nausea and vomiting in some cannabis users. Despite its increasing prevalence, tools for early identification and intervention are lacking. This study aimed to improve our understanding of CHS by examining patterns of cannabis use and identifying symptom profiles of individuals suspected or diagnosed with CHS. By identifying the risk factors and initial warning signs, we can support earlier recognition, harm reduction, and intervention.
Materials and Methods:
An anonymous survey was distributed via social media to gather detailed, self-reported information about cannabis consumption methods, frequency of use, product sourcing, and CHS-related symptoms. Participants were recruited online through organic outreach to CHS-focused social media communities in late 2024.
Results:
A total of 1134 participants were included in the final analysis. Most respondents reported smoking cannabis flower or using vape cartridges, although the use of edibles and concentrates were also described. The overwhelming majority of respondents (96.5%) used cannabis products at least daily, with approximately half (45%) using them six or more times per day around the time they developed CHS symptoms. Most of the respondents (61.9%) sourced cannabis from licensed dispensaries. The duration of cannabis use prior to symptom onset varied widely among participants, with nearly two-thirds (65.4%) reportedly used for more than 3 years before symptom development. During the prodromal (early) phase, symptoms clustered in the morning (63.1%) and the predominant complaints were nausea and stomach pain. Women reported more frequent and prolonged symptoms than men.
Discussion:
Our findings suggest that CHS is most associated with long-term, frequent use of inhaled delta-9-tetrahydrocannabinol (Δ9-THC) dominant cannabis. The acquisition source of cannabis products did not affect the syndrome presentation. Although many different cannabis consumption methods were represented, smoking and vape cartridges were the most commonly reported. The use of vape cartridges was associated with a shorter time to the development of CHS symptoms. Increased awareness of these patterns could improve the early recognition and management of CHS.
Keywords
Introduction
Cannabinoid hyperemesis syndrome (CHS) is a poorly understood clinical condition, characterized by cyclical vomiting in the context of long-term, frequent cannabis use. This condition has recently emerged as an increasing burden to emergency departments (ED) and health care systems, alongside the increased normalization of cannabis use worldwide. 1 Following the commercialization of recreational cannabis in Nevada, ED visits for CHS more than doubled between 2013 and 2021, increasing from 1.07 to 2.22 per 100,000 people. 2 A medical records review from Ontario, Canada found a 13-fold increase in CHS-related ED visits from pre-legalization in 2014 through legalization in 2021. 3 A retrospective cohort study of electronic health records from Kaiser Permanente Northern California found that the annual prevalence of CHS increased by at least 134–175% between 2009 and 2019. 4 It is unclear whether this increasing prevalence reflects the expanded U.S. cannabis legalization since 2012 or the improved recognition of CHS following its first description in 2004. 5
Regardless, the increased recognition of this condition has resulted in the development of diagnostic criteria (ROME-IV) in 2016. 6 Most recently, in 2025, a specific International Classification of Diseases, Tenth Revision code was established for CHS, which is expected to improve capture of the epidemiological data. Despite its increasing prevalence, the underlying pathophysiology of CHS is still not well understood, and it remains unclear why some, but not all, cannabis users develop the syndrome. Additionally, insufficiently studied factors, such as underlying genetic variation or stress regulation, may play a significant role in the pathogenesis of CHS.7–9
CHS is thought to manifest primarily, although not exclusively, in individuals with a history of frequent and long-term use of delta-9-tetrahydrocannabinol (Δ9-THC) containing products.10–12 The hallmark symptom of CHS is recurrent, severe, and refractory vomiting, frequently accompanied by abdominal pain, which is often relieved with hot bathing. 13 Symptoms are typically described in three phases: prodromal, hyperemetic, and recovery. 14 The prodromal phase of CHS typically precedes hyperemetic episodes. This early warning phase is an understudied component of the syndrome and is characterized by nausea, abdominal discomfort, and restlessness, during which patients often continue cannabis use with the belief that it provides relief. The hyperemetic phase involves severe, recurrent nausea and vomiting that can persist for several days, with the potential to cause life-threatening dehydration if prolonged. The recovery phase follows cannabis cessation and is marked by gradual resolution of symptoms, though relapse into the cycle is common if cannabis use resumes. 15 Improved awareness and identification of prodromal symptoms could aid health care providers in recognizing CHS earlier, potentially reducing its severity and overall burden.
The existing literature lacks detailed data on cannabis use patterns among individuals with CHS, particularly in the period preceding the onset of symptoms. 16 Furthermore, key information such as cannabinoid content, route of administration, dosage, and frequency of use is often absent in the literature, despite their potential relevance to diagnosis and pathology. Other factors, such as minor or synthetic cannabinoids, contaminants, pesticides, or methods of consumption, may contribute to disease progression. Specific modes of consumption may be especially important to consider, including oral ingestion, smoking flower, using vape cartridges, or dabbing concentrates (i.e., flash vaporization). 17 The absence of these data leaves uncertainty regarding the role of cannabinoid use in the development of CHS.
This survey aims to build upon the existing understanding of the clinical history, symptom presentation, and cannabis use patterns associated with CHS. By elucidating these key factors, we seek to support health care professionals with the early identification of CHS symptoms through more informed history taking and to reduce harm in individuals with CHS through early intervention.8,13,14
Methods
This was an observational, descriptive survey study that collected anonymous data from a digital questionnaire using © 2025 QuestionPro Survey Software. Following a literature review of survey methodology and consulting with stakeholders in the CHS community, a questionnaire was developed that included specific questions addressing cannabis use patterns and related symptoms.8,13 The study received an institutional review board (IRB) self-exemption through the University of California (UCI), Irvine (IRB #4558).
Participants were recruited online using a digital flyer, developed in accordance with UCI research guidelines, and distributed across social media platforms. Primary recruitment occurred within CHS-focused Facebook communities, with additional outreach through short-form educational video posts on Instagram and TikTok and author podcast interviews. All recruitment was organic, with no paid advertising. The survey remained open from September 24, 2024 to December 27, 2024. The authors are based in the United States, and the publicly accessible survey link was accessible to a global audience.
To proceed with the questionnaire, participants were required to meet three inclusion criteria: (1) age 18 years or older, (2) carry a formal diagnosis of CHS or suspect that they had CHS despite lacking a formal diagnosis, and (3) use of cannabis before the onset of their symptoms.
Raw data were analyzed using descriptive statistics in Microsoft Excel and GraphPad Prism (version 10.4.0). Subgroup analyses were conducted to examine trends across specific cohorts, including sex, method of consumption, and sourcing. Statistical significance was assessed using chi-squared tests, chi-squared tests for trend, or Fisher’s exact test, as appropriate, based on the sample size and data distribution using the GraphPad Statistics Guide. Analyses focused on identifying the associations between use patterns and CHS symptom characteristics.
Results
Study participants and demographics
A total of 1161 individuals completed this survey. Following data collection, 27 participants with a history of cyclical vomiting syndrome or hyperemesis gravidarum prior to initiating cannabis were excluded from the analysis, resulting in a final number (n) of 1134. All raw tabulated responses to Part 1 of our survey can be found in the supplemental information (Supplementary Data).
Demographics of study participants are shown in Table 1.
Demographic Characteristics of Survey Participants (n = 1134)
Summary of participants biological sex, age, cannabis use indication, race/ethnicity, geographic location, and education level. Those who selected “prefer not to answer” are not included.
Cannabis use characteristics
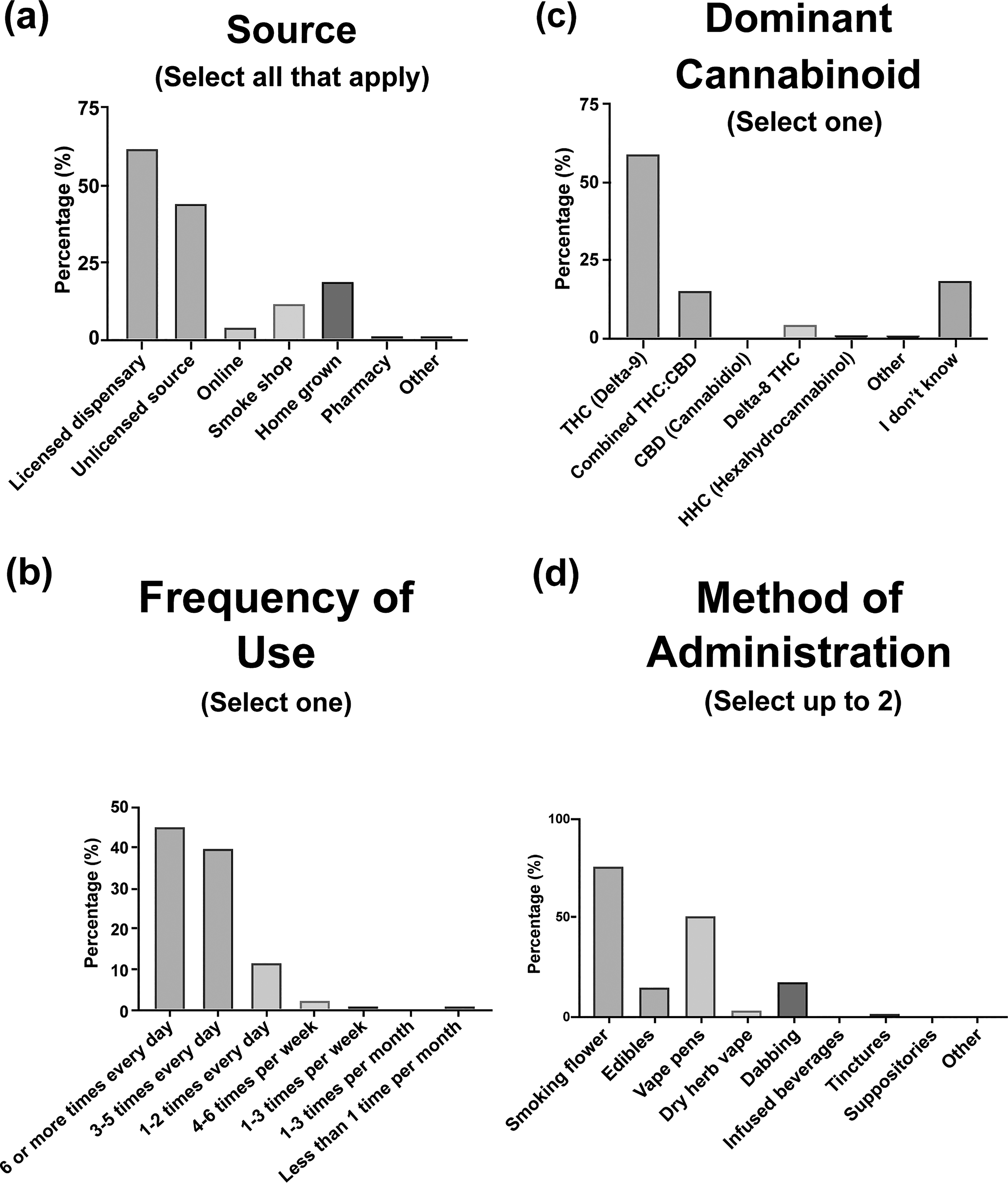
Participants answered a series of questions about their cannabis use behaviors, including acquisition sources, frequency and duration of use, cannabinoid content, and consumption methods, in the 3 months prior to developing CHS symptoms (Figs. 1 and 2).
Cannabis use characteristics reported by participants in the 3 months before developing CHS symptoms.

Weekly cannabis consumption in the 3 months before developing CHS symptoms.
The three primary sources where respondents reported acquiring cannabis were licensed dispensaries (61.9%), the unlicensed market (44%), and homegrown cannabis (19%) (Fig. 1a). Most participants with CHS reported consuming cannabis six or more times daily (45%), followed by three to five times daily (39.9%). Only 3.5% of respondents reported using cannabis less than once per day (Fig. 1b).
The dominant cannabinoid in the products used was △9-THC (59.5%), followed by a combination of △9-THC and CBD (15.6%). Three respondents (0.3%) reported CBD as the primary cannabinoid and nearly one in five (18.3%) responded that they did not know. Additionally, two synthetically produced cannabinoids, △8-THC (4.8%) and hexahydrocannabinol (HHC) (0.6%), were infrequently reported (Fig. 1c).
When asked about their two primary methods of consumption, inhalation methods were overwhelmingly the predominant route of cannabis consumption, including smoking flower (75.8%), using vape cartridges (51.2%), dabbing concentrates (16.9%), and dry herb vaporization (2.8%). Overall, oral formulation consumption was less common with 15.5% of respondents using edibles. Substantially fewer participants reported the use of infused oils (1.1%) and infused beverages (0.6%) (Fig. 1d). Note: Participants were allowed to select two primary consumption methods, and there was a significant overlap among the categories.
Mean weekly oral cannabis consumption, measured in milligrams (mg) of THC, was 192.6 mg for edible products, 145.8 mg for infused oils, and 122.5 mg for infused beverages (Fig. 2a). The predominant method of use was smoking flower, and the mean amount inhaled, measured in grams (g) of cannabis flower, was 10.3 g per week. The mean amount of inhaled concentrates (i.e., “dabbing”), measured in grams (g) of cannabis concentrate, averaged 3.15 g per week, and vape cartridge users reported using an average of two 1-gram cartridges per week (Fig. 2b).
Duration of cannabis use
The duration of cannabis use prior to CHS symptom onset varied substantially among the participants (Fig. 3). The largest proportion (26.5%) reported use for 3–5 years, while a nearly equivalent proportion (26.2%) documented use for more than 10 years. Only 3.9% reported cannabis use for less than 6 months. Overall, most participants reported at least 1 year of use prior to symptom development.
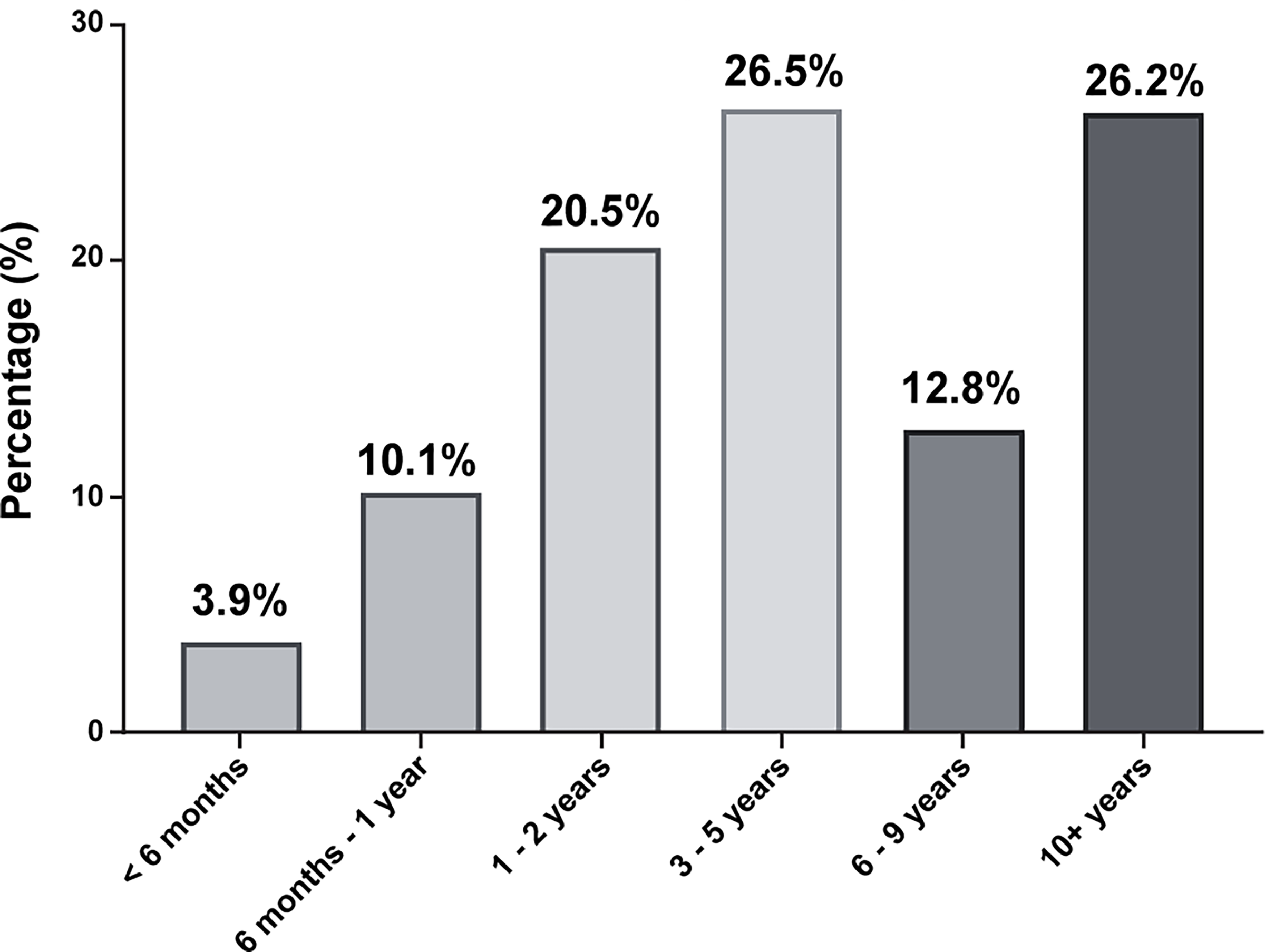
Duration of cannabis use prior to developing CHS symptoms. Duration of cannabis use before the initial onset of CHS symptoms, grouped by length of use.
Prodromal and hyperemetic phases of CHS
A wide range of symptoms and times of occurrence were described in both the prodromal and hyperemetic phases, although there were distinctions between phases (Fig. 4).
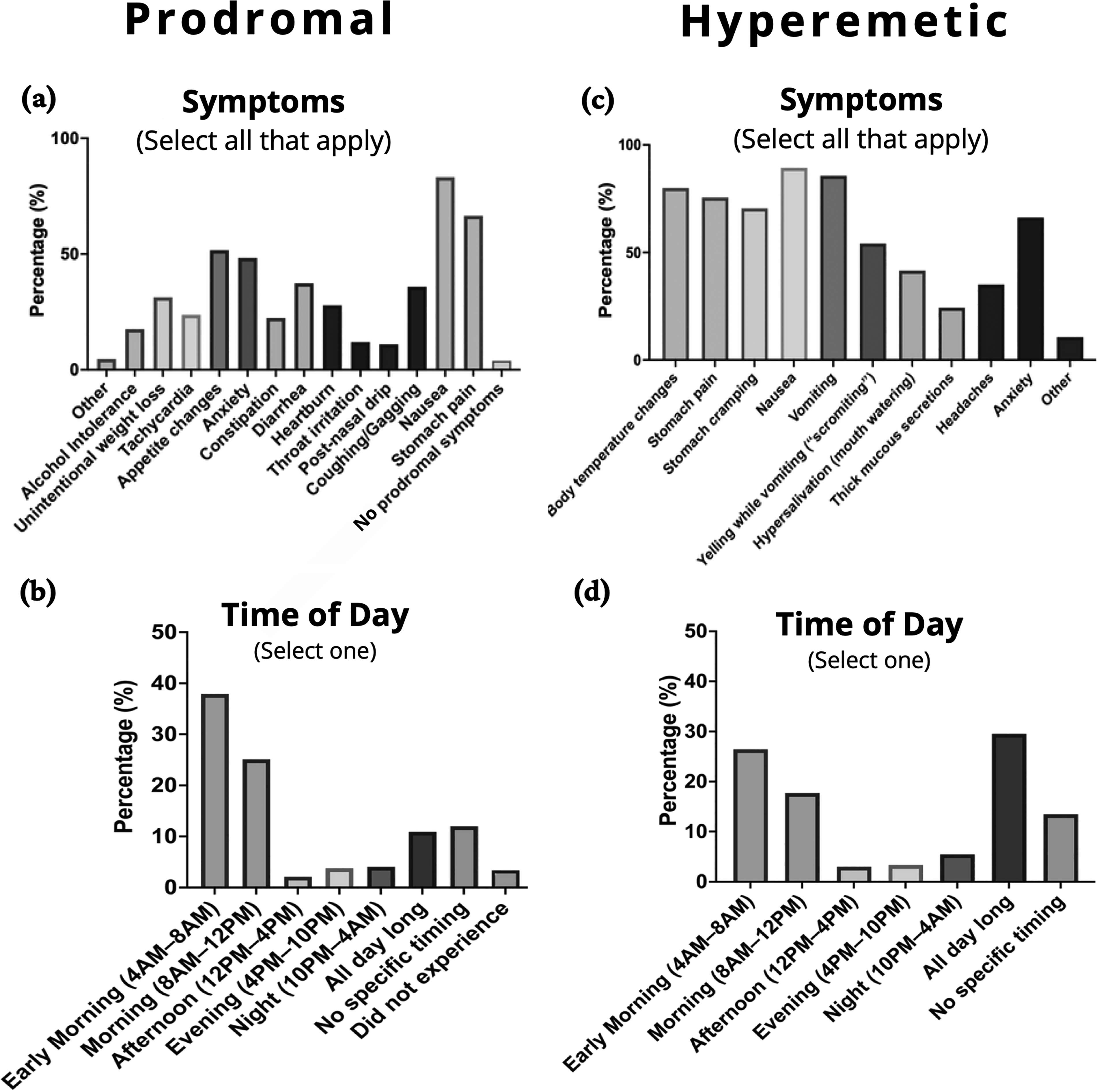
Self-reported symptoms and timing during the prodromal and hyperemetic phases of CHS.
In the prodromal phase, the predominant symptoms described were nausea (83.2%) and stomach pain (66.5%), and to a lesser extent, appetite changes (51.7%) and anxiety (48.3%). In contrast, the hyperemetic phase was characterized by a wider array of symptoms, including nausea (89.3%), vomiting (85.7%), body temperature changes (80%), and anxiety (66.2%) (Fig. 4a,c).
Morning hours were the most commonly reported time for prodromal symptoms, with the highest frequency between 4
Sex-based differences in CHS symptomatology
Females reported a higher symptom burden than males for both the prodromal and hyperemetic phases, with varying levels of statistical significance (Fig. 5a,b). When asked about hyperemetic episode duration, males were more likely to report hyperemetic episodes lasting less than one day (p < 0.0001), while females were significantly more likely to report episodes lasting 3–5 days (p < 0.01), 6–9 days (p < 0.001), and 10+ days (p < 0.001). A chi-squared test for trend revealed sex-based differences in the duration of hyperemetic episodes (p < 0.0001) (Fig. 5c). Symptom severity among women appeared to fluctuate relative to the menstrual cycle (Fig. 5d), with female respondents noting worsening (37.8%), uncertainty about worsening (34.4%), and no worsening (12.5%) during menses.
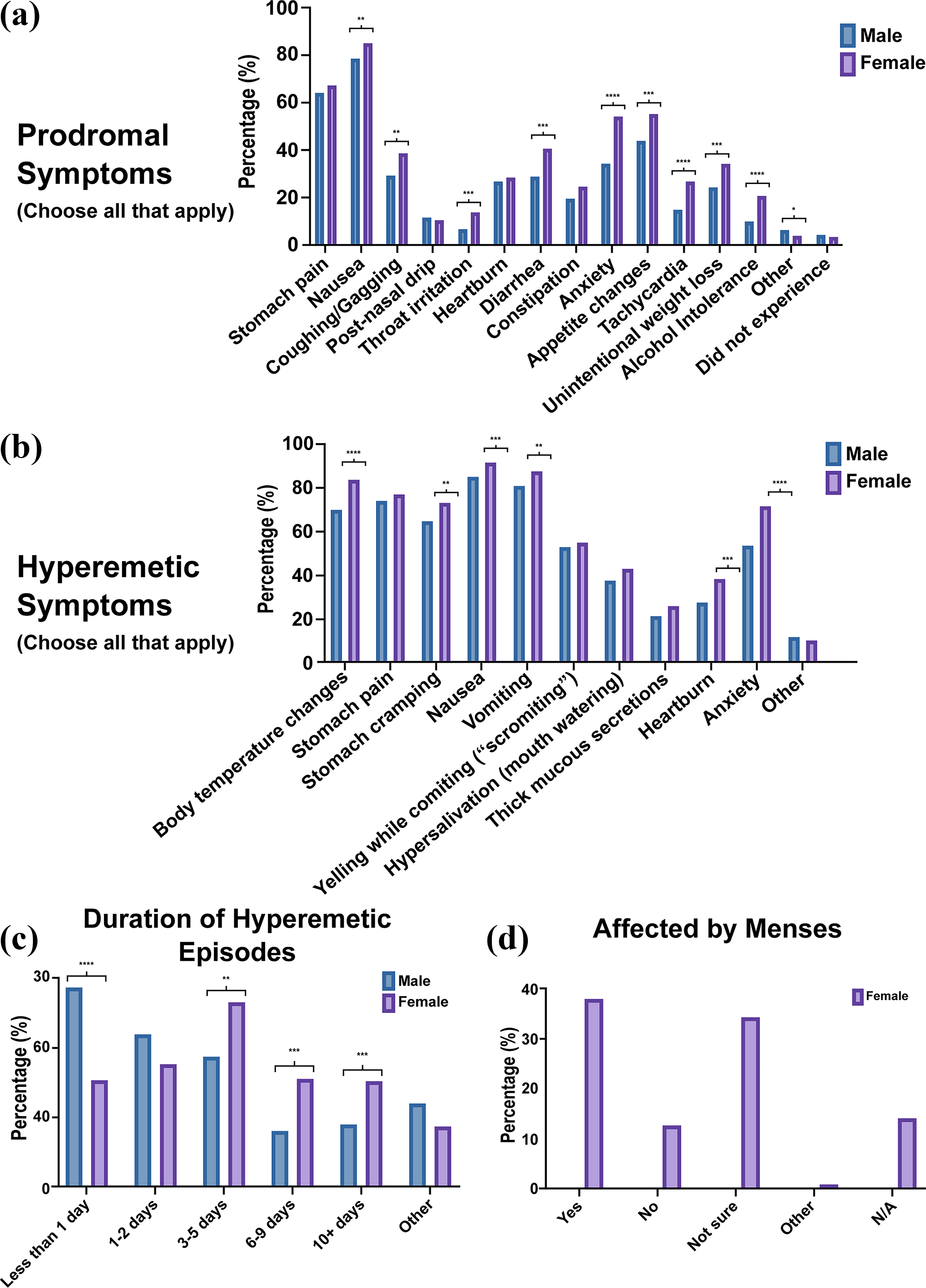
Sex-based differences in symptom reporting, episode duration, and hormonal influences in participants with CHS.
Single cannabis acquisition source sub-analysis
Participants included in this sub-analysis reported obtaining cannabis from a single primary source, including licensed dispensaries, the unlicensed market, homegrown cannabis, and hemp-derived products purchased online or in smoke shops (Fig. 6a). No statistically significant differences were identified in prodromal or hyperemetic symptoms based on source (Fig. 6b,c).

Symptom patterns stratified by primary cannabis product source.
Single method of consumption sub-analysis
To evaluate the influence of consumption methods on CHS development, a sub-analysis was conducted to include only participants who reported a single method of cannabis administration (Fig. 7). Due to limited responses, the edible-only (n = 17) and dabbing-only (n = 17) groups were excluded resulting in a comparison between those who exclusively reported smoking cannabis flower and those who exclusively reported using vape cartridges (Fig. 7a).
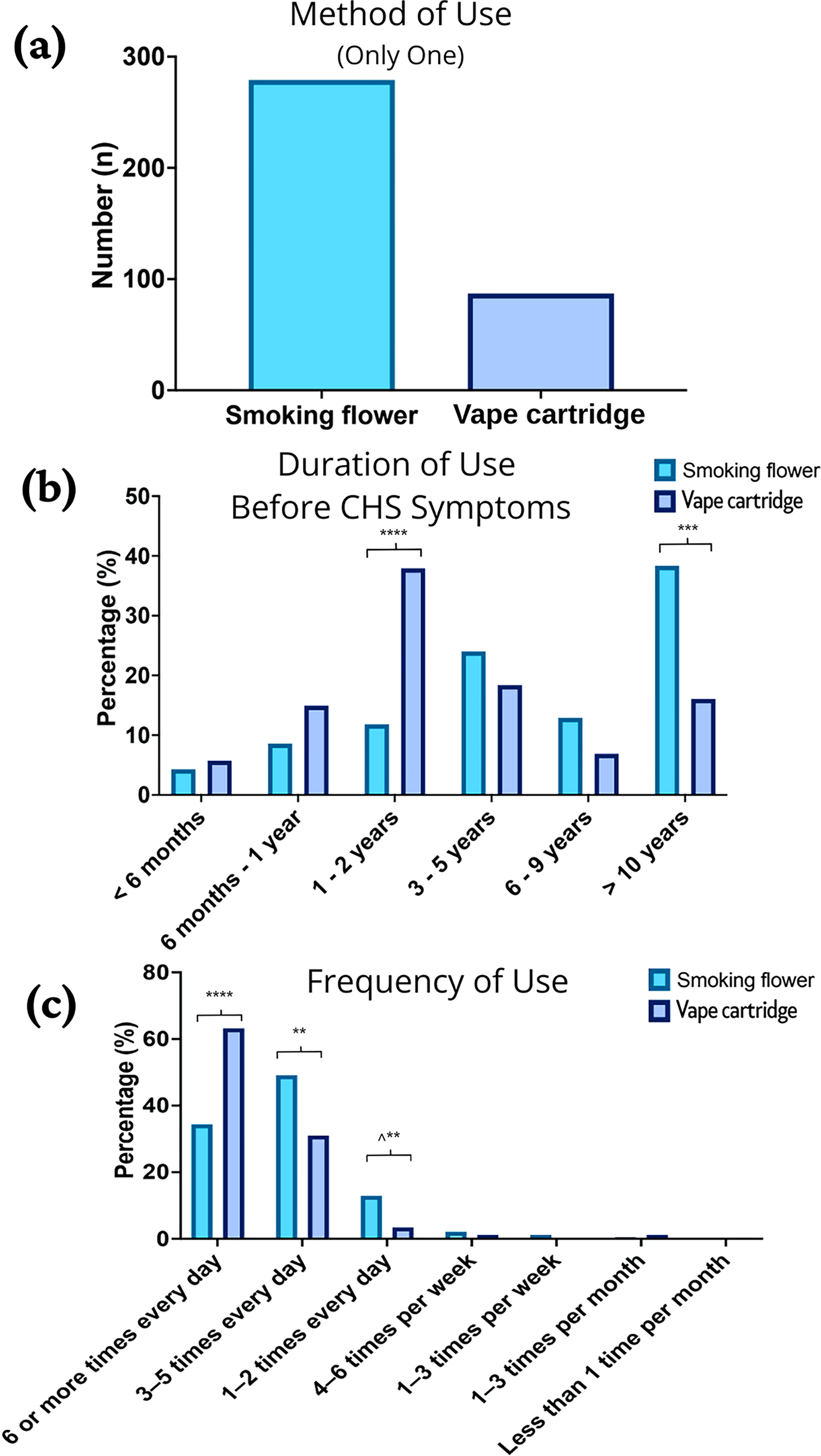
Cannabis use patterns among participants using a single administration method before CHS symptom onset.
Individuals who exclusively used vape cartridges reported developing CHS symptoms sooner than those who exclusively smoked flower. A chi-squared test for trend confirmed a statistically significant difference between the trends in these groups (p < 0.0001), suggesting that exclusive use of vape cartridges was more likely to be associated with a shorter onset of CHS symptoms than exclusive smoking (Fig. 7b). In addition, exclusive vape cartridge users tended to use cannabis more frequently than individuals who smoked flower (Fig. 7c).
Discussion
Our data highlight variable symptom onset, a wide range of cannabinoid consumption methods, frequency and dosage, as well as diverse participant experiences within the same condition. Despite this variability, several consistent themes emerged, including daily cannabis use, a predominance of inhaled △9-THC containing products, and the presence of morning-time prodromal symptoms in the majority of participants.
The results suggest that while total weekly or daily cannabis consumption fluctuates widely between individuals, regular and frequent use remains a defining characteristic. This is supported by existing literature indicating that CHS may result from a combination of high-frequency use and personal susceptibility, with potential mechanisms involving cannabinoid accumulation and impaired homeostatic balance.18–20
Heavy cannabis use, often defined as near-daily use, has historically been identified as a key contributor to CHS development; our findings support this concept.7,19–21 Frequency of use appears to be associated with the development of CHS, with a strong trend toward consumption frequency of multiple times per day.
The average weekly amount of inhaled cannabis reported in our study—10.3 g of smoked flower, 3.2 g of dabbed concentrates, and 2 g of vape cartridges—are consistent with what is considered moderate-to-heavy cannabis use; however, there was substantial variability in the amounts reported. Most participants consumed △9-THC dominant products, although the THC concentrations of the products used were not quantified.
While the predominant cannabinoid consumed was △9-THC, other cannabinoids such as △8-THC and HHC were also reported, though much less frequently (Fig. 1c). These three cannabinoids share similar pharmacological activities, specifically as partial agonists of cannabinoid receptor 1 (CB1), reinforcing the hypothesis that repeated CB1 receptor agonism may be a key contributor to CHS.10,11 CBD was only reported as the predominant cannabinoid by 0.3% of respondents and does not share the same pharmacology as △9-THC.
In our survey, participants reported similar CHS symptoms regardless of being sourced from licensed dispensaries, the unlicensed market, hemp retailers, or homegrown cultivation. Symptom consistency across these varied sourcing categories (Fig. 6) suggests that a single contaminant or pesticide is unlikely to be the cause. Most pesticides have distinct toxicological profiles, and it is improbable that all market segments would converge on a common exposure capable of producing an identical syndrome. 22 However, it should be noted that these data are based on self-reported primary sources of cannabis, rather than direct product analysis. Without laboratory testing of the cannabis products used by the participants, contaminants as a contributing factor to CHS cannot be definitively ruled out.
Our single-method subanalysis suggests that using vape cartridges may be associated with a more rapid onset of CHS compared with smoking flower. The mechanism underlying this difference remains unclear and warrants further investigation. One possibility is that this finding simply reflects the relatively recent rise in the popularity of vape cartridges, which were far less common a decade ago. However, given the difference in pharmacokinetics, the potential influence of vape cartridge additives or contaminants, and the potentially higher THC concentrations, this connection merits closer examination. Vaporized products typically contain higher THC percentages and produce pharmacokinetic profiles characterized by higher peak plasma concentrations and faster time to peak effect (Tmax) than smoked flower, which may accelerate CB1 receptor internalization and contribute to downstream endocannabinoid system dysregulation.9,23 Notably, exclusive vape cartridge users also reported more frequent consumption, suggesting that both pharmacologic factors and ease of use or habitual dosing patterns may contribute to accelerated symptom development. In addition, cartridge formulations often include added terpenes, solvents, or other constituents that could plausibly influence symptom onset, although this remains speculative.
The prodromal phase offers an important time frame for CHS intervention. Only 3.8% of participants denied experiencing this phase. Prodrome is characterized by low-level symptoms without intractable vomiting. It remains unclear if and for how long patients experience prodromal symptoms before their first hyperemetic episode. Most of the participants reported morning nausea during the prodromal phase. Although this has been generally recognized in the literature since 2004, our survey aimed to better understand prodromal experiences more precisely. 10 To our knowledge, this is the first study to evaluate prodromal-specific timing and symptoms. Increased awareness of this phase among consumers and clinicians may lead to earlier intervention, potentially reducing escalation to hyperemetic episodes in some patients with CHS.
Our data suggest that women and men experience CHS similarly in terms of symptom onset, consumption patterns, and overall timing of symptoms. However, notable differences were observed in symptom severity and duration. Females reported more CHS symptoms overall and experienced longer hyperemetic episodes and worsening symptoms around menstruation, suggesting a potential hormonal or sex-based influence. The reason for the longer duration of hyperemetic episodes in women remains unclear but could potentially be due to sex-based metabolic differences or greater adiposity, potentiating prolonged storage and delayed clearance of cannabinoid metabolites.10,24
Our study has several limitations. First, the survey was based on self-reported data from participants recruited via online platforms without independent verification of the CHS diagnosis, which may introduce sampling, recall, and response bias. In addition, cannabinoid potency data (e.g., %THC) were not collected for inhaled products such as flower or concentrates, as these values are frequently unavailable, unreliable and inconsistent; consequently, we could not evaluate the potential influence of product strength on CHS risk or symptom severity. The participants were predominantly female and white, which may reflect recruitment bias, variations in health care-seeking behavior, differences in survey participation willingness, or potentially meaningful epidemiological trends in CHS that warrant further investigation.
Conclusion
Our survey indicates that CHS is most strongly associated with long-term, frequent exposure to inhaled △9-THC-dominant products, with smoking flower and using vape cartridges being the predominate routes; notably, the use of vape cartridges was associated with a shorter time to symptom development. Women experienced more symptoms and longer episodes than men. While morning-clustered prodromal symptoms were common, the syndrome remains clinically heterogeneous across individuals. A heightened awareness of these usage patterns and symptom profiles can help facilitate earlier recognition and improve management in the acute care setting. The development of standardized questionnaires that assess cannabis use and characteristic symptomatology alongside the adoption of unified diagnostic criteria are needed to advance our scientific understanding of CHS.
Authors’ Contributions
C.P., M.M., and K.N. conceived and designed the study. C.P., M.M., K.N., J.H., J.S., and R.K. contributed to methodology development. C.P. and R.L. managed data organization and technical tools used for data collection and processing. C.P., J.H., J.S., K.N., R.K., and M.M. conducted the investigation. C.P., J.H., J.S., R.K., and M.M. contributed to formal data analysis. K.N. provided personal financial support for participant incentives. J.S. and M.M. drafted the original article. C.P., J.H., J.S., and M.M. critically reviewed and edited the article. R.L. and C.P. created visualizations. A.N. and C.P. supervised the project. C.P. managed project administration and served as the corresponding author. All authors read and approved the final article.
Footnotes
Acknowledgments
The authors would like to thank the administrators of Cannabinoid Hyperemesis Syndrome (CHS): A Safe Place to Recover and Learn, a private Facebook support group, for their support and assistance. The authors especially thank “Tessa420” (Tessa Datillo) for her efforts in recruiting participants through social media. Most importantly, the authors extend their gratitude to all individuals who participated in the survey and shared their experiences to advance understanding of CHS.
Author Disclosure Statement
C.P., J.S., M.M., R.K., R.L., and A.N. declare no conflicts of interest. J.H. reports providing targeted lectures and consultative services for health care professionals through Plant Amplified Wellness. K.N. is the administrator and owner of Cannabinoid Hyperemesis Syndrome (CHS): A Safe Place to Recover and Learn, a private Facebook support group.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. All participants, regardless of meeting inclusion criteria, had the option to enter into a drawing. Three winners each received $100 gift cards after the end of the study period, funded by a generous personal donation from author K.N.
Use of Artificial Intelligence Tools
Large language models were used intermittently by some authors to assist with grammar and language refinement during article preparation. These tools did not contribute to the conception of ideas, methods, analysis of data, or interpretation of results. The authors take full responsibility for the content of this work.
Data Access Statement
Aggregated numerical results from the survey are provided in the Supporting Information files. Individual-level data and free-text responses are not publicly shared in order to protect participant privacy. These materials are available from the corresponding author upon reasonable request and documentation of IRB-compliant data use.
Ethics Statement
This study was submitted to the University of California, Irvine Institutional Review Board and was determined to be self-exempt, as it involved an anonymous, voluntary online survey with no collection of personally identifiable information.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.