
Abstract
Introduction:
The endocannabinoid system (ECS) is increasingly recognized as an important regulator of many physiological systems. People who use products derived from Cannabis sativa L. are exposed to exogenous cannabinoids. The influence of this exogenous exposure on the ECS is unclear. People who use cannabis have demonstrated lower basal levels of endocannabinoids, but the dynamic response of their ECS to a controlled stimulus is unknown. Our study purpose was to compare circulating concentrations of the endocannabinoid N-arachidonoylethanolamine (anandamide, AEA) and subjective experiences between people who use cannabis and those who do not, during and following a standardized exercise stimulus.
Materials and Methods:
Twenty adults (n = 8 who regularly use cannabis [age: 21–32 years; 5/3 males/females] and n = 12 who do not use cannabis [age: 21–39 years; 7/5 males/females]) completed a 1-h treadmill run at an intensity equivalent to 65% of peak oxygen uptake. Arterialized-venous blood was collected prior to, during (including the last minute of exercise), and 15 min following exercise for determination of anandamide concentration. The subjective experiences of the participants during and after the run were assessed with responses to several questions assessed on a Likert scale.
Results:
Compared with controls, the cannabis use group had lower AEA concentrations at end-exercise (0.47 ± 0.13 vs. 0.33 ± 0.10 ng/mL; p = 0.015) and 15-min post-exercise (0.57 ± 0.17 vs. 0.38 ± 0.18 ng/mL; p = 0.001). The cannabis use group also had worse mood (3.25 ± 1.03 vs. 2.29 ± 1.34; main effect of condition p = 0.05) and higher probability of feeling pain (p < 0.001).
Conclusion:
Habitual cannabis use was associated with diminished AEA response, worse mood, and more pain during/following exercise. These pilot data might have implications for clinical outcomes associated with cannabis use, including cannabis use disorder and withdrawal, as well as potentially for exercise adherence.
Introduction
The endocannabinoid system (ECS) regulates many physiological functions, including mood, 1 pain, 2 and subjective responses to exercise (e.g., the “runner’s high”). 3 This is achieved through activation of cannabinoid receptors 1 and 2 (CB1R/CB2R) by endogenous ligands, including N-arachidonoylethanolamine (anandamide, AEA). Cannabis sativa L. (cannabis) exerts many of its effects via partial agonism of these receptors. 4 From 2013 to 2021, cannabis use has increased substantially in the United States, 5 underscoring the need for greater understanding of potential health consequences. While prior studies have explored direct effects of cannabis (e.g., on cognition, 6 psychosis risk 7 ), relatively few have explored how chronic exposure to exogenous cannabinoids alters ECS function in non-clinical samples (e.g., adults without schizophrenia 8 or cannabis use disorder 9 ) and/or the potential downstream physiological consequences of such alterations.
Notably, a recent meta-analysis found that acute physical exercise increases AEA concentrations. 10 For example, in one study, circulating AEA increased from ∼2.5 to ∼6 pmol/mL following a 30-min walk/run. 11 While other physiological stimuli such as pain 12 can also elicit endocannabinoid release, exercise offers a controllable stimulus for studying ECS dynamics. The purpose of this pilot study was to determine whether frequent cannabis use alters the endocannabinoid and associated subjective responses to a standardized physiological stimulus. We expected that use of exogenous cannabinoids would downregulate ECS function, 13 in line with observations of disrupted endogenous opioid signaling with chronic exogenous opioid use. 14 Thus, we hypothesized that people who frequently use cannabis would exhibit a blunted AEA response to exercise compared with those who do not use cannabis. Consistent with this, daily cannabis use has been linked to reduced CB1R availability in the brain 15 and increased AEA levels during abstinence among regular cannabis users. 16
Methods
Participants
This cross-sectional study comprises two groups, people who use cannabis and those who do not (henceforth referred to as the control group). Participants were recruited in Fort Collins, Colorado, between September 2022 and May 2025. Inclusion criteria were age 21–40 years, ability to run continuously for 60 min, habitual exercise (≥5 sessions/week, ≥30 min/session during the past year), and during the previous 6 months, either (a) regular cannabis use (≥3 times/week) or (b) no cannabis use. Exclusion criteria included heart and/or peripheral vascular disease, hypertension, stroke, heart murmur, sickle cell anemia, pulmonary disorders, pregnancy, breastfeeding, or contraindication to exercise identified during a 12-lead electrocardiogram (ECG) stress test. Our Institutional Review Board approved this study (Protocol 3577). Participants provided written informed consent.
Screening visit
Potential participants completed medical screening, informed consenting, pregnancy testing (if female), assessment of body composition, and a 12-lead ECG treadmill stress test. Body habitus was quantified via measures of composition, comprising dual-energy X-ray absorptiometry (Hologic, Discovery W, QDR Series), height, and mass. During the stress test peak oxygen uptake (VO2peak) was assessed using indirect calorimetry (ParvoMedics TrueOne 2400). Participants jogged/ran on a level treadmill at their self-estimated 5 km race pace. Treadmill grade was increased by 2% every 2 min until volitional fatigue.
Habituation
Participants reported to the laboratory for 1 h of treadmill exercise. The speed required to elicit a metabolic rate equivalent to 65% VO2peak was estimated using the American College of Sports Medicine equation (VO2 [mL/kg/min] = (0.2 * speed [meters per minute] + 3.5). Indirect calorimetry confirmed relative exercise intensity and speed were titrated to maintain the target workload. Treadmill gradient remained at 0%.
Data collection visit
At least 48 h following the habituation session, participants returned to our lab for the formal data collection session. Participants were asked to refrain from vigorous exercise for ≥20 h before this visit. On arrival, a cannula was placed in a dorsal hand vein, and a heated blanket was used to facilitate collection of arterialized-venous blood. Prior to (minute 0), during (minutes 15, 30, 45, 60), and 15 min after the 60-min run (minute 75), blood was collected, heart rate (HR) was measured, and four single-item questions assessing mood (−5 = very bad to + 5 = very good), pain (“how much pain are you currently feeling?”, rated from 0 to 10), 17 fatigue (“to what extent do you feel fatigue?”, rated from 0 to 4), 18 and rating of perceived exertion (RPE: “how hard are you working?”, rated from 6 to 20, Borg scale 19 ) were verbally administered by research staff. Participants responded verbally to indicate their rating on each scale. Exercise intensity was confirmed via indirect calorimetry during minutes 22–27 and 52–57.
Determination of circulating plasma AEA
Blood samples were collected into prechilled tubes coated with ethylenediaminetetraacetic acid, centrifuged to isolate plasma, and stored at −80°C until analysis. Following study completion, plasma AEA concentrations were quantified using established liquid chromatography–tandem mass spectrometry methods. 20 Samples were prepared using salting-out–assisted liquid–liquid extraction with an isotope-labeled internal standard, alongside matrix-matched calibration and quality control samples. Chromatographic separation was performed using reverse-phase liquid chromatography, and AEA was detected using positive electrospray ionization with multiple reaction monitoring. Quantification was based on linear calibration curves spanning physiologically relevant concentrations. The limit of detection was 0.025 ng/mL.
Statistical analysis
Data are presented as mean ± standard deviation. Baseline group differences were compared using Student’s t-tests. Linear mixed modeling (lme4 21 ) was used to compare AEA concentrations and subjective measures. Models had two fixed effects (group: controls vs. people who use cannabis; and time) and one random effect (subject). Parametric assumptions were checked using normal Q-Q, residuals vs. fitted plots, and the histogram of residuals. Tukey’s Honestly Significant Difference test was done when there were significant main effects or interactions using the emmeans package. 22 Pain data were zero-inflated and not normally distributed; thus, a cumulative-link mixed model was used to determine pain probabilities between groups, and three observations from a single participant were removed as outliers, resulting in better model fit. Repeated measures correlations (rmcorr 23 ) were used to correlate AEA with subjective experiences. Significance was set at α = 0.05. All analyses were conducted using R (R-Core-Team, version 2024.12.1 + 563) in RStudio (Posit; version 4.5). Figures were created using SigmaPlot 12.3 (Graffiti LLC).
Results
Of the 32 enrolled adults, 20 completed data collection. Nine were lost to follow-up, and three withdrew (two for unrelated reasons and one due to a compensation request exceeding the consented amount). No baseline differences were observed between groups (Table 1).
Participant Characteristics
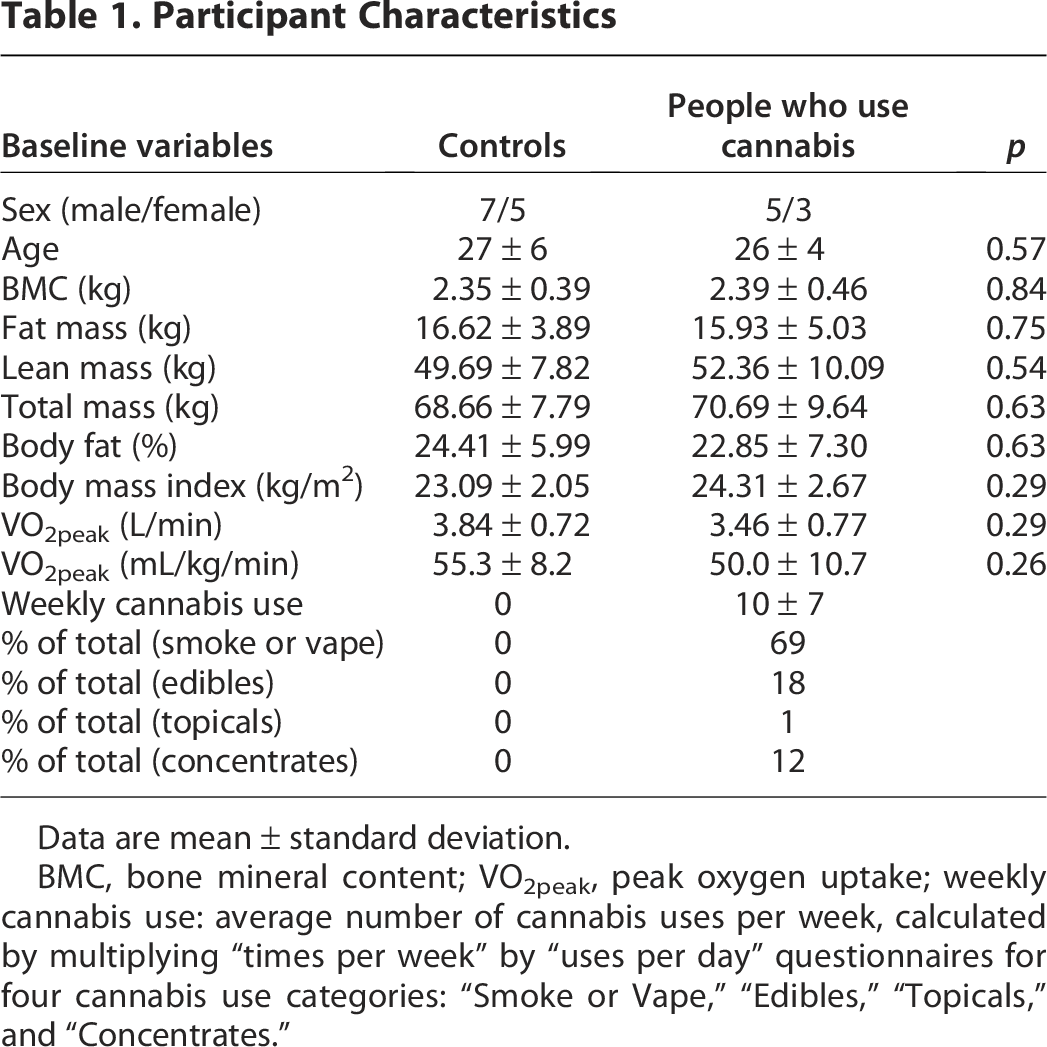
Data are mean ± standard deviation.
BMC, bone mineral content; VO2peak, peak oxygen uptake; weekly cannabis use: average number of cannabis uses per week, calculated by multiplying “times per week” by “uses per day” questionnaires for four cannabis use categories: “Smoke or Vape,” “Edibles,” “Topicals,” and “Concentrates.”
Exercise intensity markers
Between-group differences in exercise stimulus were assessed using HR and relative intensity. Except for baseline (T0) HR, there were no group differences in any outcome (all p > 0.11; Table 2).
Group Differences in Exercise Outcomes and Subjective Measures
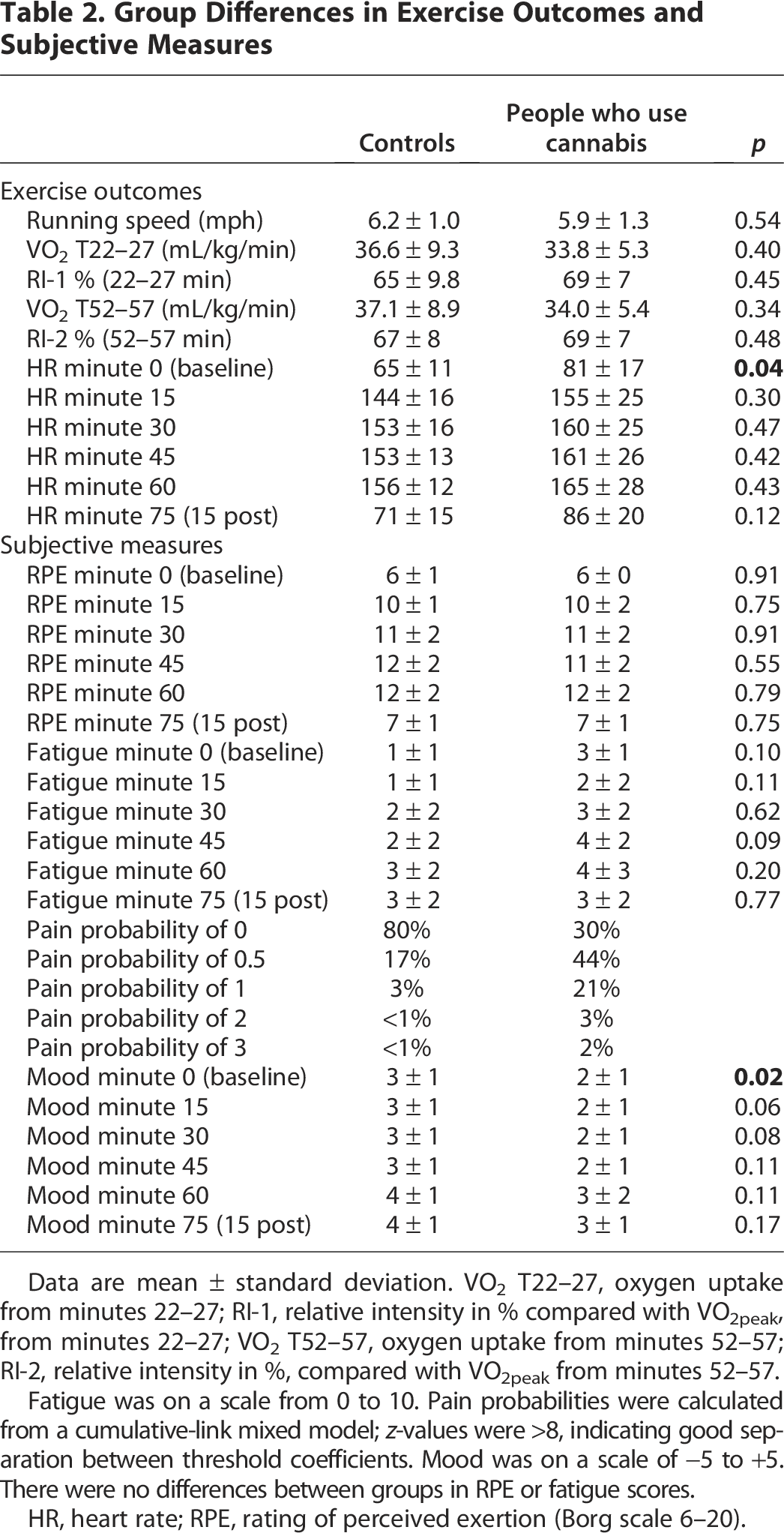
Data are mean ± standard deviation. VO2 T22–27, oxygen uptake from minutes 22–27; RI-1, relative intensity in % compared with VO2peak, from minutes 22–27; VO2 T52–57, oxygen uptake from minutes 52–57; RI-2, relative intensity in %, compared with VO2peak from minutes 52–57.
Fatigue was on a scale from 0 to 10. Pain probabilities were calculated from a cumulative-link mixed model; z-values were >8, indicating good separation between threshold coefficients. Mood was on a scale of −5 to +5. There were no differences between groups in RPE or fatigue scores.
HR, heart rate; RPE, rating of perceived exertion (Borg scale 6–20).
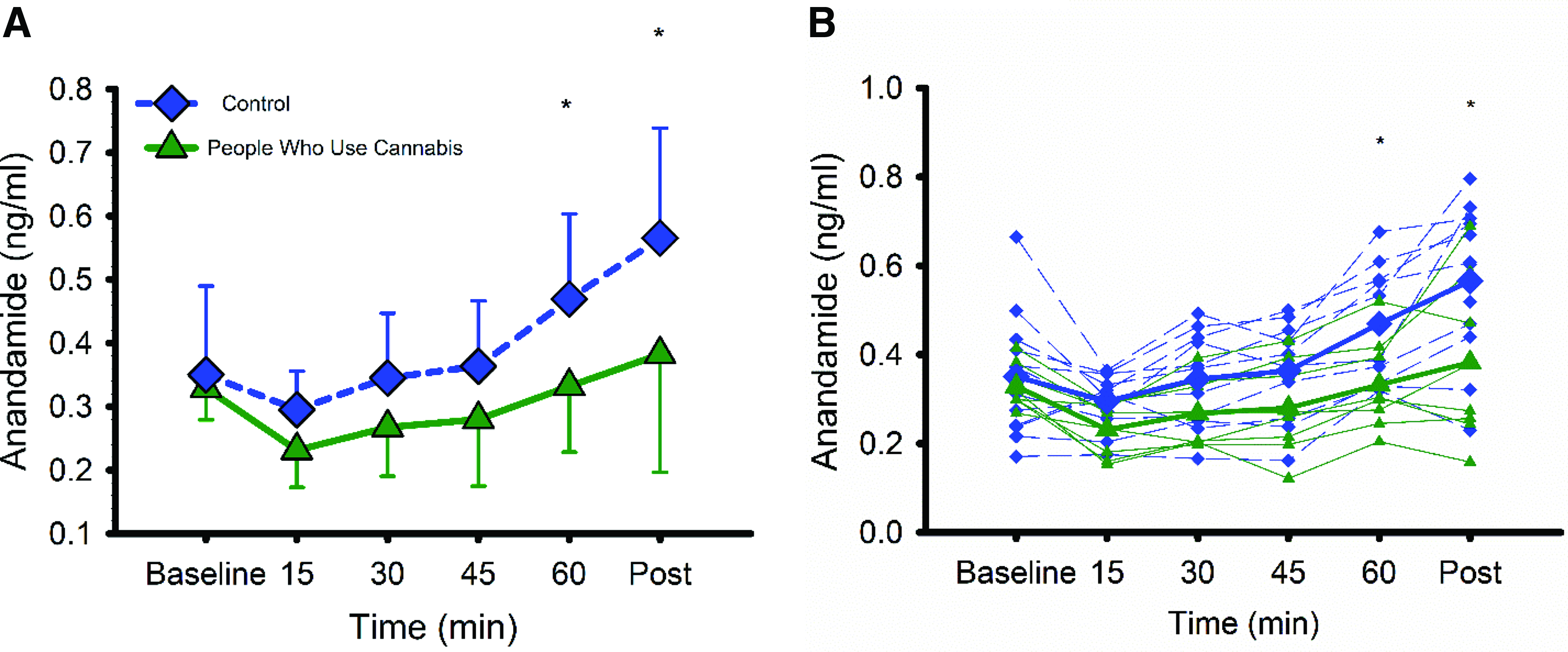
Circulating plasma AEA concentrations
Baseline AEA was not different between groups (t(34.4) = 0.4, p = 0.69). During exercise, AEA increased in both groups (F(5,88) = 22.8, p < 0.001), with a significant group × time interaction (F(5,88) = 3.31, p = 0.008; see Figure 1). Post hoc analysis showed 42% higher AEA concentrations at T60 (0.47 ± 0.13 vs. 0.33 ± 0.10 ng/mL; t(34.4) = 2.5, p = 0.015) and 50% greater AEA concentration postexercise (0.57 ± 0.17 vs. 0.38 ± 0.18 ng/mL; t(34.4) = 3.5, p = 0.001) in the control group.
Subjective experience measures
Fatigue and RPE did not differ between groups (F(1,18) = 2.4, p = 0.13; F(1,18) = 0.002, p = 0.96). Controls had higher overall mood than people who use cannabis (3 ± 1 vs. 2 ± 1; F(1,18) = 4.4, p = 0.05). Pain was more likely among people who use cannabis: probability of no pain was 0.30 vs. 0.80 in controls, and probability of a 0.5–1 pain rating was 0.65 vs. 0.20 (p < 0.001).
Correlations between AEA and subjective experiences
AEA concentrations were positively correlated with fatigue (r = 0.26, p = 0.046) in controls but not in people who use cannabis (p = 0.598). When participants from both groups were pooled, AEA correlated with mood (r = 0.46, p < 0.001) and RPE (r = −0.33, p < 0.001).
Discussion
In our pilot study, individuals who frequently use cannabis showed a blunted endocannabinoid response to exercise, lower mood, and a higher likelihood of experiencing pain. In the full sample, circulating AEA correlated with subjective experiences. While prior work has shown altered endocannabinoid levels at rest, 24 our findings appear to be the first evidence that people who use cannabis show a blunted AEA response to a physiological stimulus. This is consistent with positron emission tomography observations of reduced CB1R availability in this population, 25 implying a global (rather than ligand- or receptor-only) downregulation of the ECS.
Exercise increases AEA after as little as 15 min. 26 In our study, the diminished AEA response in cannabis users became evident only after 60 min of exercise. The concentrations of blood chemicals are determined by the rates of appearance and disappearance. Our study was not designed to measure either; however, in light of repeated observations of increased rates of appearance of other circulating factors during exercise (e.g., the pleotropic myokine interleukin-6, 27 catecholamines, 28 growth hormone 29 ), we speculate that increased AEA may also be attributed to increased appearance and therefore decreased production in cannabis users.
Our mood and pain data align with evidence that endocannabinoids impact psychological outcomes. 30 Because pain elicits an endocannabinoid response, the higher pain ratings in the cannabis group may reflect reduced circulating AEA, which normally dampens pain perception.
Regarding our mood findings, given the bidirectional links between ECS dysfunction and depression, 31 our results may provide early insight, albeit speculative, into subclinical mood alterations associated with regular cannabis use.
Fatigue and RPE did not appear to differ between groups, suggesting we successfully matched the physical and psychological effort put forth during the exercise bout, representing a standardized ECS stimulus. People who use cannabis may appreciate being made aware of the risk for decreased ability to produce endocannabinoids in response to physical stressors. This may also have implications for the people using cannabis to treat pain. 32 That is, it is plausible that with cannabis use, the ECS contribution to pain tolerance may be diminished. This topic would benefit from future research.
Finally, our data suggest that circulating AEA is correlated positively with fatigue (in controls only) and mood but negatively with RPE. One possible implication is that AEA might be produced as a homeostatic mediator of fatigue, but cannabis use might impair this function. This may have implications for exercise adherence, which is typically higher when participants find exercise enjoyable. 33 Given that cannabis use was associated with more pain, worse mood, and lower AEA during exercise, people who use cannabis could be encouraged to prioritize enjoyable forms of exercise, or lower-intensity exercise, to promote adherence.
Limitations and future directions
Our pilot study has several limitations. We only included a relatively small sample of young participants who exercised regularly; thus, results may not generalize to a broader population of less fit or older adults, and low statistical power may have contributed to the absence of group differences for some variables, including HR and relative exercise intensity. To promote recruitment and maintain ecological validity, we did not enforce a cannabis abstention period prior to data collection. Acute cannabis use raises AEA concentrations, 34 thus no enforced abstinence may have confounded our findings. However, in our study people who use cannabis showed lower AEA concentrations, suggesting a blunted endogenous response. We also did not standardize food intake, caffeine use, sleep, hydration status, or timing of recent cannabis use, all of which may influence AEA concentrations and affective responses to exercise. For example, plasma AEA concentrations undergo a marked change following food intake, 35 and the mood-enhancing effects of caffeine are well described. 36 We only measured one endocannabinoid (AEA) and did not confirm cannabis use or abstention via blood or urine tests. Exercise appears to have a greater impact on AEA production than 2-arachidonoylglycerol, 37 thus AEA was considered most appropriate for our research question.
Future studies could evaluate the extent to which ECS function recovers following cessation of cannabis use. Data indicate that CB1Rs are restored following a month of cannabis abstinence. 25 This work could be extended to incorporate more precise timing of cannabis cessation and stimulus/response tests, such as the exercise bout used in our study. In light of our data demonstrating that people who use cannabis have a diminished endocannabinoid response to a physiological stimulus, investigating whether normalization of endocannabinoid function during abstinence enhances stress resilience could be informative for managing cannabis use disorder and withdrawal. Perhaps one reason it is difficult for some individuals to abstain from cannabis is reduced resilience to stressors.
Conclusion
Our pilot study, although not without limitations, may have some potentially important implications. Our findings point to ECS downregulation among people who use cannabis regularly, which may also underlie differences in mood and pain during exercise. Results may have potential relevance for cannabis use disorder, mood, pain, and exercise adherence.
Authors’ Contributions
T.R.E.: Data curation, formal analysis, investigation, methodology, project administration, visualization, and writing—original draft; M.C.B.: Investigation and writing—review and editing; K.E.G.: Investigation and writing—review and editing; V.T.S.: Methodology and writing—review and editing; G.P.D.: Resources, data curation, and writing—review and editing; C.B.: Resources, supervision, conceptualization, methodology, and writing—review and editing; H.C.K.: Resources, supervision, conceptualization, methodology, and writing—review and editing. All authors reviewed and approved the final submitted article.
Footnotes
Acknowledgments
Due to the word and reference limits associated with the Brief Report format, the authors regret being unable to acknowledge some of the fine work completed by our colleagues and peers.
Author Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
The Department of Psychology and the Department of Health and Exercise Science at Colorado State University provided support for this study. H.C.K. is supported by the National Institutes of Health K23AA028238.