
Abstract
Background:
Exogenous cannabinoids are considered promising therapeutic candidates for inflammatory bowel disease (IBD). However, robust pre-clinical evidence supporting its efficacy remains limited. This systematic review and meta-analysis aimed to evaluate the therapeutic effects of exogenous cannabinoids in animal models of IBD.
Methods:
Controlled experimental studies involving animal models of IBD that evaluated the effects of exogenous cannabinoids compared to untreated models were included. Four databases (PubMed, Embase, Web of Science, and the Cochrane Library) were searched up to August 26, 2025. Two independent reviewers conducted study selection, data extraction, and the risk-of-bias assessment. The risk-of-bias assessment was performed using the Systematic Review Center for Laboratory Animal Experimentation tool. Meta-analyses were performed using standardized mean differences (SMDs) and random-effects models. The study was registered in INPLASY (INPLASY202540009).
Results:
Twenty-seven pre-clinical studies involving 408 animals were included. Compared with controls, exogenous cannabinoids significantly reduced disease activity index (SMD = −3.43; 95% confidence interval [CI]: −4.98 to −1.89; I2 = 83%) and histopathological score (SMD = −4.46; 95% CI: −6.37 to −2.54; I2 = 84%). It also decreased levels of myeloperoxidase (MPO), TNF-α, IL-6, and IL-1β. However, substantial heterogeneity was noted across several outcomes.
Interpretation:
Exogenous cannabinoids show beneficial effects in pre-clinical IBD models, likely through anti-inflammatory, antioxidant, and barrier-enhancing mechanisms. These findings provide a supportive foundation for future translational research. Nevertheless, the overall certainty of the evidence is limited by unclear randomization, lack of blinding, high heterogeneity, and small sample sizes. Although some clinical trials have already begun exploring its therapeutic potential, further rigorous and standardized animal studies are needed to clarify mechanisms, optimize dosing, and reinforce the translational pathway.
Introduction
Inflammatory bowel disease (IBD), comprising Crohn’s disease and ulcerative colitis, is typified by persistent inflammatory processes within the gastrointestinal tract. 1 The global burden of IBD has been steadily increasing, with notable disparities in its incidence and prevalence across different regions, countries, and age demographics. 2 While the prevalence of IBD has recently plateaued in several Western nations, it remains persistently high. 3 In contrast, newly industrialized regions in Asia and South America continue to experience rising trends in both the incidence and prevalence of the disease. 4 The burden of IBD continues to rise globally among children, adolescents, and the elderly.5,6 The core therapeutic goals in the management of IBD are to induce and sustain clinical remission, promote mucosal healing, and prevent or address disease-related complications. 7 Current pharmacological treatments for IBD include aminosalicylates, corticosteroids, immunomodulators, biologics, and antibiotics. 8 The limitations of existing therapies underscore the urgent need for alternative treatment strategies that are both effective and safe. Accordingly, there is a pressing need for innovative therapeutic strategies that are not only more efficacious but also better tolerated in the management of IBD.
With a millennium-long medicinal history, the cannabis plant has been extensively employed for therapeutic, recreational, and spiritual purposes.9,10 In gastroenterology, it is renowned for its antiemetic, appetite-stimulating, and antidiarrheal effects. 11 Exogenous cannabinoids, encompassing phytocannabinoids derived from the Cannabis sativa plant and synthetic analogs, have attracted attention due to their potential benefits in a variety of medical conditions,12,13 including IBD.14,15 Phytocannabinoids include over 100 compounds, most notably Δ9-tetrahydrocannabinol (THC), the primary psychoactive component, and cannabidiol (CBD), a nonpsychoactive molecule, alongside others such as cannabigerol (CBG), cannabinol, cannabichromene (CBC), and tetrahydrocannabivarin (THCV). 16 Synthetic cannabinoids, designed to mimic or enhance endocannabinoid effects, 17 include dronabinol (synthetic THC), nabilone (a synthetic THC analog), WIN 55,212-2 (a nonselective CB1/CB2 agonist), JWH-133 (a selective CB2 agonist), and HU-210 (a potent CB1/CB2 agonist). Pre-clinical and clinical investigations indicate that exogenous cannabinoids exert a wide range of pharmacological effects, encompassing anti-inflammatory, antioxidant, anticancer, anticonvulsant, analgesic, and neuroprotective actions.18–24 These effects are mediated by interactions with the endocannabinoid system, a complex neuromodulatory network that regulates several physiological processes, including inflammation, gastrointestinal motility, visceral feeling, and immunological responses.17,25 The endocannabinoid system’s two G-protein-coupled receptors—CB1, enriched in central and enteric neurons, and CB2, upregulated on gut immune cells—respectively dampen visceral hypersensitivity and hypermotility while suppressing pro-inflammatory cytokine release.25,26 Endogenous ligands, such as anandamide and 2-arachidonoylglycerol, bind to these receptors to maintain homeostasis. 27 THC acts as a partial agonist at both CB1 and CB2 receptors, promoting anti-inflammatory responses and modulating gut motility; CBD exhibits low affinity for CB1/CB2 but influences the system indirectly by inhibiting FAAH, activating transient receptor potential vanilloid 1, and modulating peroxisome proliferator-activated receptor gamma.28,29 CBG and CBC also engage CB2 to reduce inflammation, whereas THCV may act as a CB1 antagonist or partial agonist depending on dose.30,31 Synthetic agonists such as WIN 55,212-2 and JWH-133 primarily target CB2 to suppress cytokine production and immune cell activation in the gut.32,33 However, the outcomes of individual animal studies are frequently influenced by various factors, including the heterogeneity of IBD animal models, differences in treatment duration, and limited sample sizes. 15 Therefore, definitive conclusions about the anti-inflammatory and antioxidant effects of exogenous cannabinoids in the context of IBD treatment remain difficult to establish. Moreover, the methodological rigor and potential publication bias in animal studies are uncertain, which may overstate the efficacy of exogenous cannabinoids. 34 To provide a more objective and comprehensive assessment, the present study undertakes a systematic meta-analysis of available pre-clinical data, aiming to clarify the anti-inflammatory and antioxidant effects of exogenous cannabinoids in IBD and inform future translational and clinical research.
Systematic reviews that incorporate animal research can enhance the reliability of evidence from animal studies, facilitate the translation of animal findings to human applications, and mitigate the squandering of financial resources and redundant animal experimentation. 35 A systematic analysis of pre-clinical animal evidence can optimize trial design protocols. 36 Currently, there is a lack of comprehensive evidence from pre-clinical studies indicating that exogenous cannabinoids can treat IBD. Therefore, this study aims to perform a systematic review and meta-analysis of pre-clinical evidence regarding the use of exogenous cannabinoids on IBD models in animals, with a focus on evaluating their therapeutic efficacy and elucidating potential underlying mechanisms.
Materials and Methods
This systematic review and meta-analysis conformed to the methodological criteria set in the Cochrane Handbook for Systematic Reviews of Interventions and complied with the reporting guidelines detailed in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 37 The study has been registered with INPLASY, and its registration number is INPLASY202540009. No amendments were made to the protocol for this meta-analysis.
Search strategy
A systematic and comprehensive search of the Cochrane Library, Embase, PubMed, and Web of Science databases was conducted to identify relevant studies from their inception to August 26, 2025. No language restrictions were applied in this study. Both free-text phrases and Medical Subject Headings (MeSH) terms about exogenous cannabinoids and IBD were incorporated into the search strategy to maximize the retrieval of relevant studies. The specific search terms included “cannabis,” “cannabinoids,” “cannabidiol,” “dronabinol,” “inflammatory bowel disease,” “ulcerative colitis,” “Crohn’s disease,” and other related terms. The search strategies for each database are provided (Supplementary Table S1). EndNote reference management software was used to organize and remove duplicates from the search results obtained from each database.
Inclusion and exclusion criteria
Following the Population, Intervention, Comparison, Outcome, and Study Design (PICOS) framework, 38 eligible studies were selected based on the following criteria: (1) Population: animal models of IBD, with no restrictions on age, sex, species, or method of modeling; (2) Intervention: exogenous cannabinoids as the sole therapeutic modality, with no limitations on dosage, duration, or route of administration; (3) Comparison: the control group comprised IBD models that did not receive any therapeutic intervention; (4) Outcome: the clinical outcomes included the disease activity index (DAI) score, histopathological score, macroscopic damage score (MDS), colon weight-to-length ratio and colon length. Molecular and inflammatory outcomes included myeloperoxidase (MPO) activity, the levels of interleukin-1β (IL-1β), interleukin-10 (IL-10), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α); (5) Study Design: controlled experimental studies conducted in animal models.
Studies were excluded if they (1) were in vitro experiments, commentaries, reviews, case reports, or clinical trials; (2) lacked an untreated IBD control group; (3) omitted sample size information; (4) provided unusable data; (5) were duplicate publications; or (6) had inaccessible full-text articles.
Study screening and data extraction
EndNote (version X20) was utilized to organize all the studies that were retrieved. The titles and abstracts of the remaining studies were independently reviewed by two authors after duplicate records had been deleted. The remaining potentially eligible publications were downloaded as full texts and underwent a final screening according to the predefined inclusion and exclusion criteria. Differences among reviewers regarding the inclusion of studies were resolved through consensus discussions. From each included study, the following information was extracted: (1) study features, including authors, publication year, animal species, strain, sex, and age; (2) details about the IBD model used; (3) intervention characteristics, such as type of exogenous cannabinoids, dosage, route of administration, and treatment duration; (4) control group details; (5) outcome measures, including clinical and molecular/inflammatory outcomes related to IBD severity and inflammation; (6) results for each outcome, including mean values, standard deviations, and sample sizes for both control and intervention groups. When numerical data were presented only in graphical form, values were extracted from the figures using digitization software (Engauge Digitizer).
Bias risk assessment
The included animal studies were evaluated for risk of bias using the Systematic Review Center for Laboratory Animal Experimentation (SYRCLE) assessment tool. 39 The tool was used to assess the risk of bias across key domains, including selection bias, performance bias, detection bias, attrition bias, reporting bias, and other potential sources. The assessment was independently performed by two reviewers, and disagreements were resolved by consensus after consultation with a third reviewer.
Statistical analysis
Version 5.4 of Review Manager (RevMan) was used to perform data synthesis for this meta-analysis. For continuous outcomes, SMDs with 95% confidence intervals (CIs) were calculated. The I2 statistic and chi-squared test were employed to assess statistical heterogeneity. When significant heterogeneity was identified (I2 > 50%), a random-effects model was adopted. Conversely, a fixed-effects model was applied in the face of no significant heterogeneity. A p-value < 0.05 denoted statistical significance. Forest plots were constructed to visually depict the pooled effect sizes along with their associated 95% CIs. Leave-one-out sensitivity analyses were conducted for each meta-analysis to assess the robustness of the findings. Subgroup analyses were performed only when two or more studies contributed to each stratum.
Results
Study selection
A systematic search yielded 5,362 articles from PubMed (n = 548), Embase (n = 2,426), Web of Science (n = 2,255), and the Cochrane Library (n = 133). After removing 1,360 duplicates, 4,002 studies underwent title and abstract screening, resulting in the exclusion of 3,951 articles. Subsequently, a total of 51 articles were identified as possibly relevant and chosen for full-text in-depth review. Two independent researchers thoroughly assessed these articles against predefined eligibility criteria, ultimately resulting in 27 studies for the systematic review. Figure 1 depicts the selection procedure for the study.
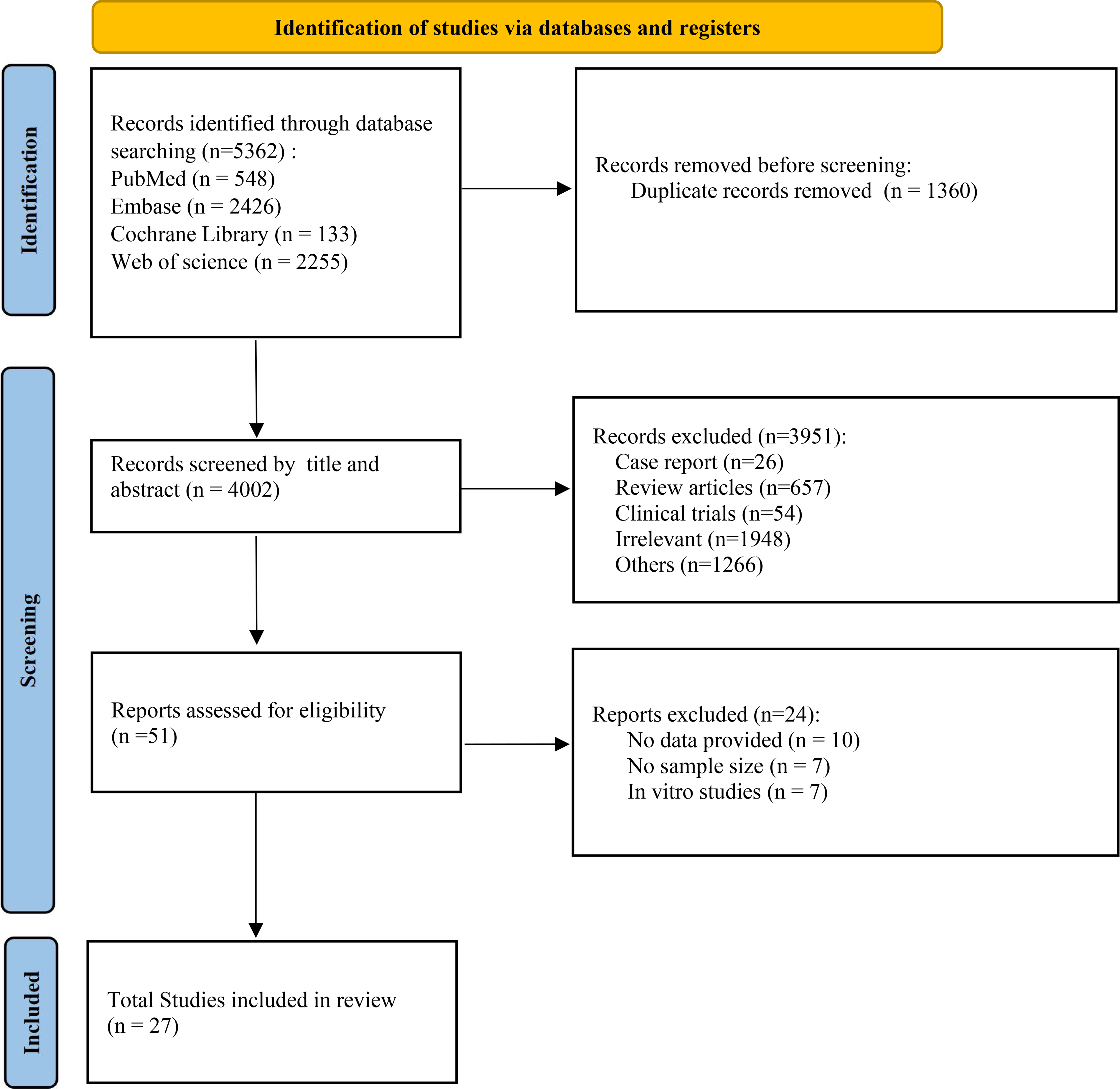
Flowchart of the literature selection process.
Characteristics of the included studies
The main characteristics of the included studies are summarized in Table 1, including (1) first author and year of publication; (2) animal species and sex; (3) animal body weight; (4) sample size per group; (5) modeling method; (6) dosage, route of administration, and treatment duration; and (7) outcome measures. Of the 27 studies included, 16 were disseminated in English and 2 in Chinese, involving 408 animals (202 experimental subjects and 206 controls). In terms of species, the studies included CD1 mice (7 studies41–47), ICR mice (6 studies40,48–52), C57BL/6 mice (3 studies53–55), C57BL/6J mice (1 study 56 ), C57BL/10J mice (1 study 57 ), BALB/c mice (1 study 58 ), and Charles River Wistar rats (1 study 59 ). Of the studies analyzed, 13 utilized male animals (n = 210), 2 employed female animals (n = 30), 2 incorporated both sexes (n = 26), and 1 study did not report sex-specific information. The methods for establishing animal models of IBD included dextran sodium sulfate (DSS; 10 studies, oral administration), dinitrobenzene sulfonic acid (DNBS; five studies, intracolonic administration), and 2,4,6-trinitrobenzenesulfonic acid (TNBS; three studies, with two using intracolonic administration and one using enema). For clinical outcomes, seven studies reported the MDS, five studies reported the DAI score, and three studies reported histopathological findings. Regarding molecular and inflammatory outcomes, 13 studies assessed MPO levels, 7 studies evaluated IL-6 levels, 7 studies measured IL-1β levels, 5 studies examined IL-10 levels, 6 studies reported colon length, 5 studies provided colon weight/length ratios, and 5 studies quantified TNF-α levels.
Characteristics of the Included Studies
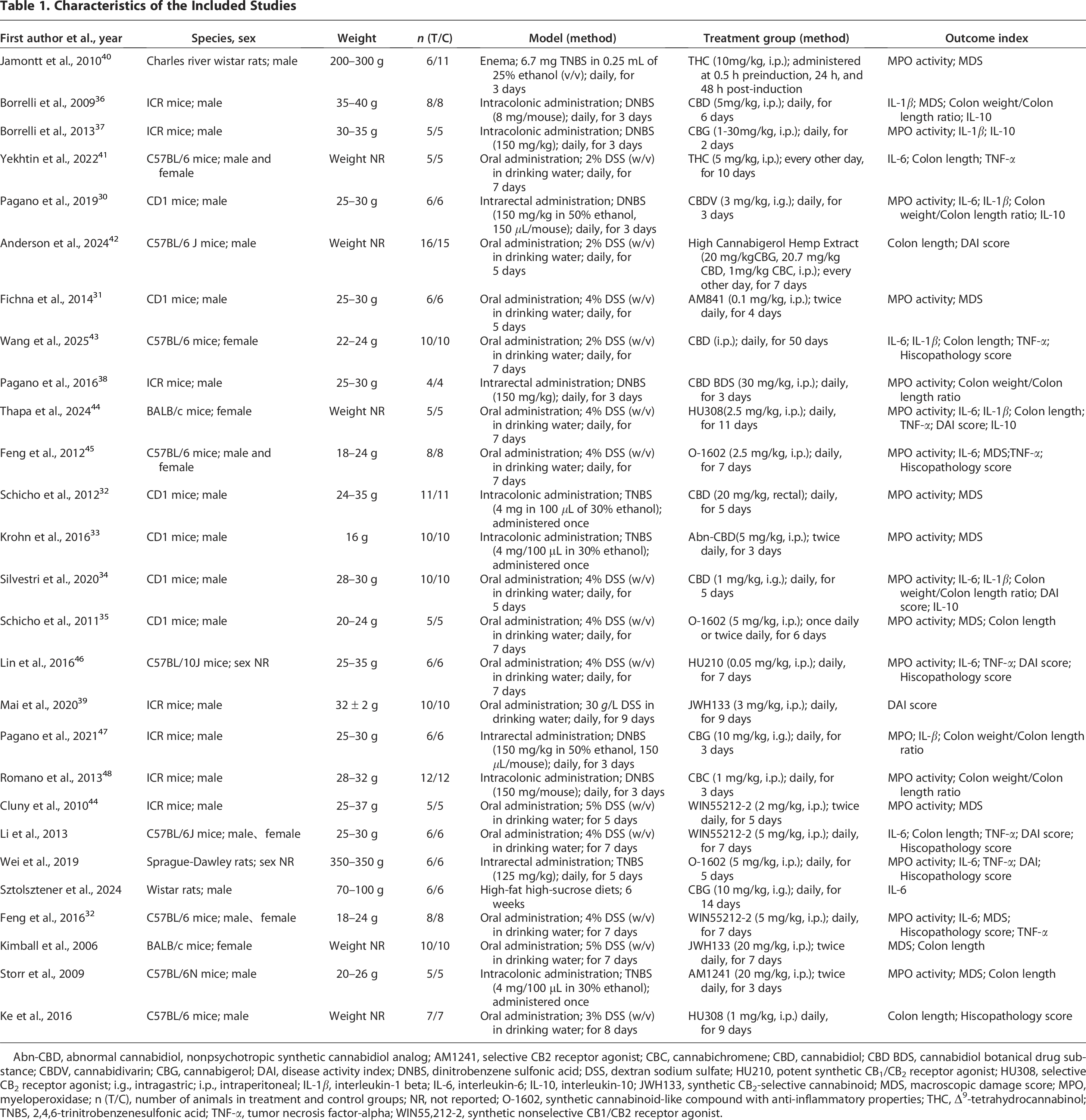
Abn-CBD, abnormal cannabidiol, nonpsychotropic synthetic cannabidiol analog; AM1241, selective CB2 receptor agonist; CBC, cannabichromene; CBD, cannabidiol; CBD BDS, cannabidiol botanical drug substance; CBDV, cannabidivarin; CBG, cannabigerol; DAI, disease activity index; DNBS, dinitrobenzene sulfonic acid; DSS, dextran sodium sulfate; HU210, potent synthetic CB1/CB2 receptor agonist; HU308, selective CB2 receptor agonist; i.g., intragastric; i.p., intraperitoneal; IL-1β, interleukin-1 beta; IL-6, interleukin-6; IL-10, interleukin-10; JWH133, synthetic CB2-selective cannabinoid; MDS, macroscopic damage score; MPO, myeloperoxidase; n (T/C), number of animals in treatment and control groups; NR, not reported; O-1602, synthetic cannabinoid-like compound with anti-inflammatory properties; THC, Δ9-tetrahydrocannabinol; TNBS, 2,4,6-trinitrobenzenesulfonic acid; TNF-α, tumor necrosis factor-alpha; WIN55,212-2, synthetic nonselective CB1/CB2 receptor agonist.
Quality of the included studies
SYRCLE’s risk-of-bias tool was employed by two investigators to evaluate the quality of the included studies (Fig. 2). The findings indicated that the ratings of the included studies ranged from 3–7. Specifically, one study scored 7, three studies scored 6, nine studies scored 5, and five studies scored 3. Random sequence generation was explicitly described in only four studies, whereas information on it was lacking in the remaining 14 studies, raising concerns about potential selection bias. Conversely, baseline characteristics were consistently documented as comparable (low risk) across all studies. Allocation concealment and blinding of investigators were rarely specified, resulting in unclear risk for most studies, with one exception noting a lack of blinding (high risk). This may lead to selection bias and performance bias, which could compromise the reliability of the findings. Eight of the 18 studies reported that animals were kept in identical settings, whereas the remaining 10 studies did not provide specifics on the conditions. There was no indication of selective reporting in any of the included studies, and all data were provided completely. Other biases were classified as low risk in 12 studies, unclear in five, and high risk in one study. Upon comprehensive quality assessment, the included studies are deemed appropriate for meta-analysis.
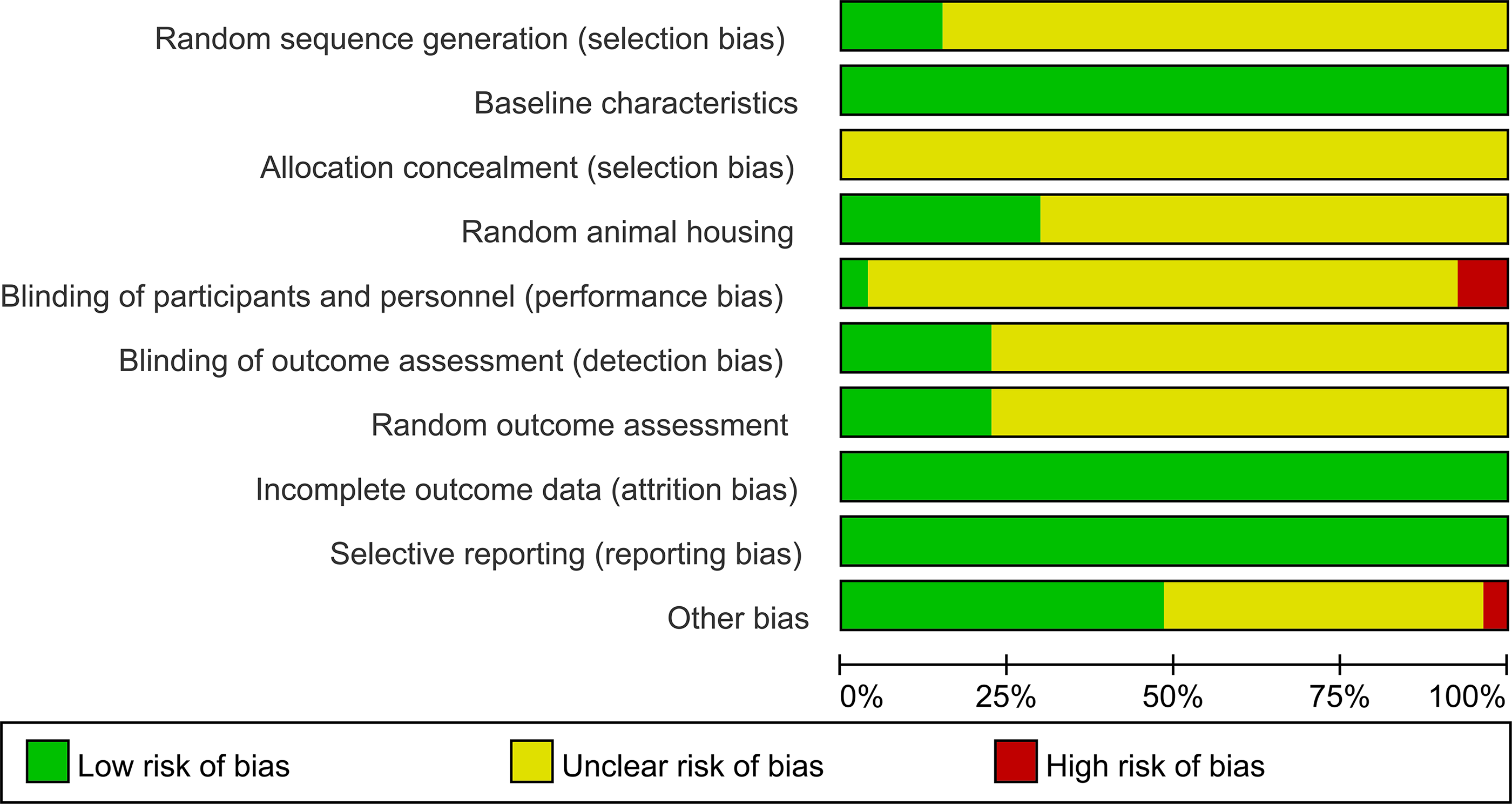
Risk-of-bias assessment of the included animal studies based on the SYRCLE risk-of-bias tool. The graph summarizes the proportion of studies rated as low, unclear, or high risk across each domain. Green indicates low risk of bias, yellow indicates unclear risk of bias, and red indicates high risk of bias.
Effects of exogenous cannabinoids on IBD
Clinical outcomes, including DAI score, histopathological score, MDS, colon weight-to-length ratio, and colon length, were identified as key indicators reflecting intestinal damage and disease severity in pre-clinical models of IBD. Molecular and inflammatory outcomes, including MPO activity and concentrations of IL-6, IL-10, IL-1β, and TNF-α, were used to characterize inflammatory activity and mucosal injury. To account for model-specific immune signatures, analyses were stratified by induction models (DSS, TNBS, DNBS, and diet-induced colitis), and results were reported separately for clinical and molecular/inflammatory outcomes in each model (Supplementary Table S2). An evidence map summarizing outcome availability and eligibility for quantitative pooling is provided (Supplementary Fig. S1).
DSS-Induced Models of IBD
Clinical outcomes
DAI score
This meta-analysis included six studies of DSS-induced murine colitis that evaluated the effect of exogenous cannabinoids on the DAI. Using a random-effects model, exogenous cannabinoids significantly reduced DAI compared with the untreated group (SMD = −2.99; 95% CI: −4.51 to −1.47; p = 0.0001; I2 = 82%; Fig. 3A). Leave-one-out analyses supported the robustness of the findings.
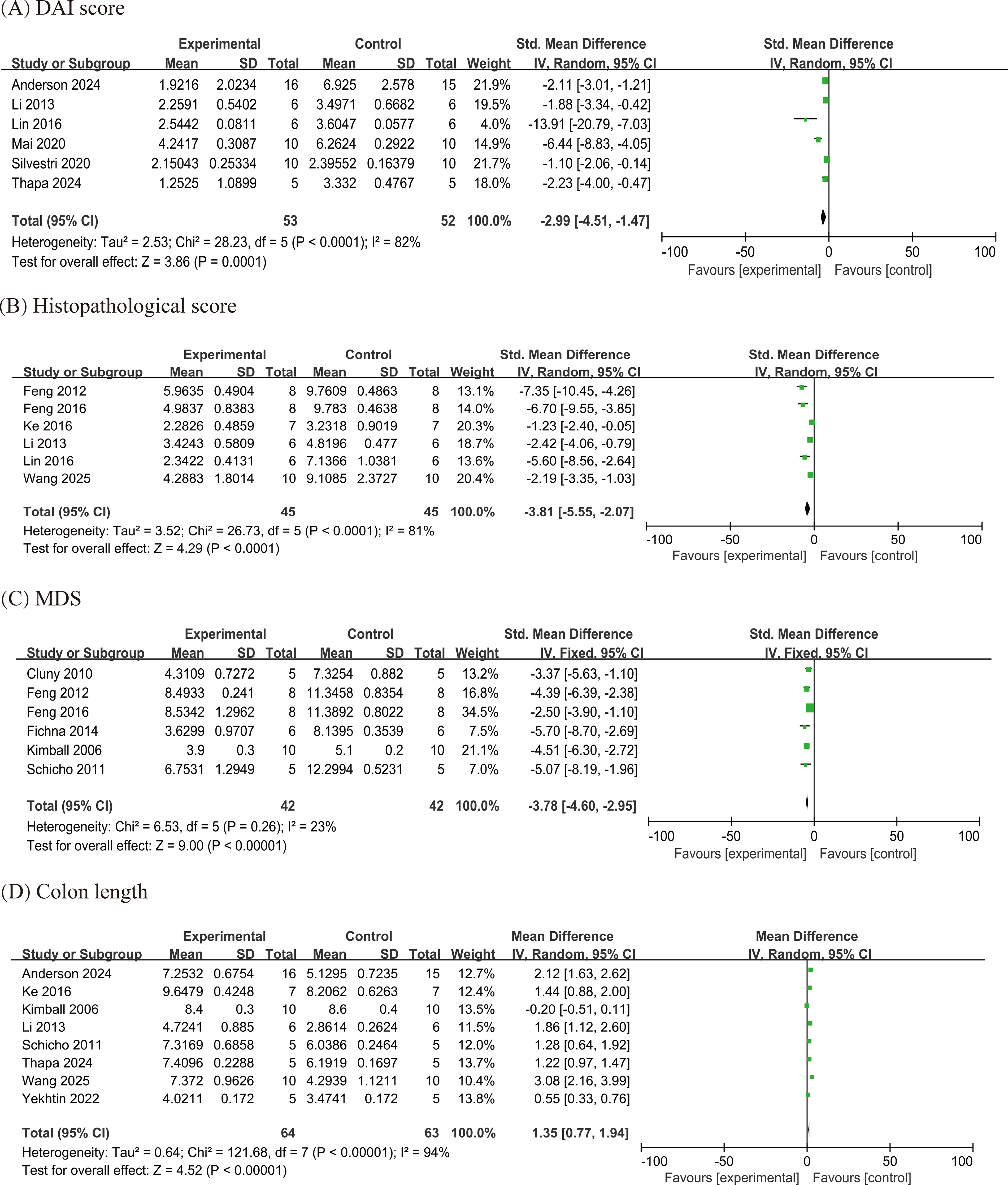
Forest plots of clinical outcomes in DSS-induced IBD models:
Histopathological score
Six studies evaluated the effect of exogenous cannabinoids on histopathological score in animal models of IBD induced by DSS. The results revealed a significant reduction in histopathological scores in animals receiving exogenous cannabinoids (SMD = −3.81; 95% CI: −5.55 to −2.07; p < 0.0001; I2 = 81%; Fig. 3B).
MDS
Six studies evaluated the effect of exogenous cannabinoids on the MDS in DSS-induced colitis. Given low heterogeneity (p = 0.26; I2 = 23%), a fixed-effect model was applied. The results demonstrated that exogenous cannabinoids significantly reduced MDS compared to control groups (SMD = −3.78; 95% CI: −4.60 to −2.95; p < 0.00001; Fig. 3C). A subgroup analysis by induction strength showed comparable effects at 4% DSS (SMD = −3.62; 95% CI: −4.64 to −2.61; I2 = 47%) and 5% DSS (SMD = −4.07; 95% CI: −5.47 to −2.67; I2 = 0%) (Supplementary Fig. S2). The magnitude of benefit did not materially differ by DSS concentration; however, power was limited for the 5% DSS subgroup.
Colon length
Eight studies evaluated colon length in DSS-induced colitis. Exogenous cannabinoids significantly increased colon length compared with controls (mean difference [MD] = 1.35 cm; 95% CI: 0.77–1.94; p < 0.00001; I2 = 94%; Fig. 3D). Leave-one-out analyses supported the robustness of this effect. Given variability in DSS concentrations across studies, we prespecified subgroups of 2%/3% versus 4%/5% DSS to reflect lower and higher induction intensities. When stratified by induction intensity (Supplementary Fig. S3), exogenous cannabinoids increased colon length in both subgroups: 2%/3% DSS (k = 4; MD = 1.74 cm; 95% CI: 0.69–2.80) and 4%/5% DSS (k = 4; MD = 1.01 cm; 95% CI: 0.09–1.93), with heterogeneity remaining high within subgroups (I2 = 95%). The between-subgroup difference was not significant (p = 0.30; I2 = 6%), indicating no evidence that DSS concentration materially accounts for the observed variability.
Colon weight-to-length ratio
In the DSS model, only one study 42 reported the colon weight-to-length ratio. Under 4% DSS, treatment of exogenous cannabinoids reduced the ratio compared with DSS controls (mean ± SD: 55.49 ± 1.38 vs. 59.02 ± 1.32; MD = −3.53; 95% CI: −4.71 to −2.35).
Molecular/inflammatory outcomes
MPO activity
Eight studies assessed MPO activity in DSS-induced colitis. Exogenous cannabinoids markedly reduced MPO activity compared with the DSS model group (SMD = −4.55; 95% CI: −6.73 to −2.37; p < 0.0001; I2 = 94%; Fig. 4A).
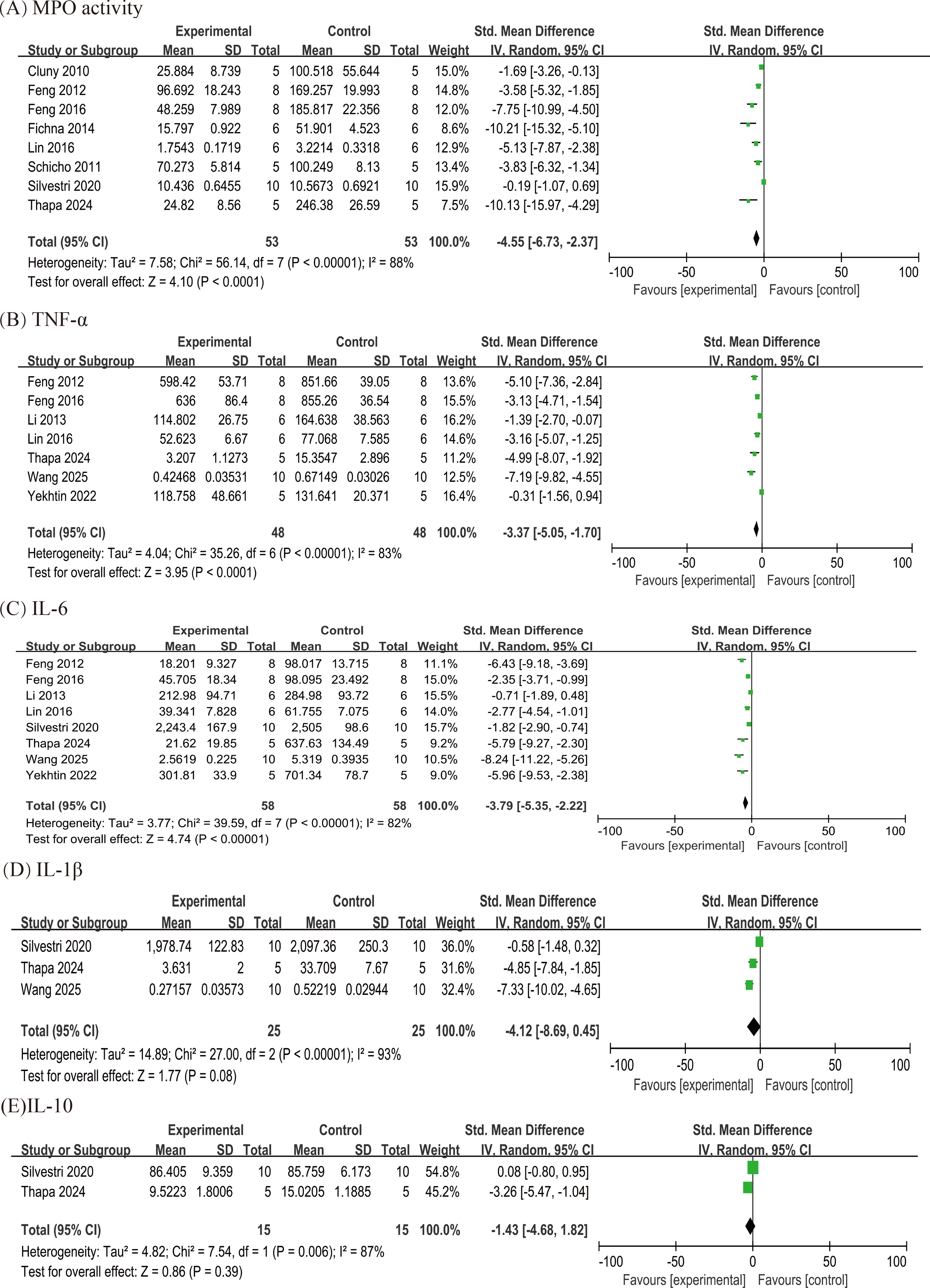
Forest plots of molecular/inflammatory outcomes in DSS-Induced IBD Models
TNF-α
Seven studies reported TNF-α levels in DSS-induced colitis. Treatment with exogenous cannabinoids significantly reduced TNF-α compared with controls (SMD = −3.37; 95% CI: −5.05 to −1.70; p < 0.0001; I2 = 83%; Fig. 4B). DSS concentration varied across studies, with five using 4% and two using 2%. A subgroup analysis based on DSS concentration showed no significant difference between subgroups (p = 0.91; I2 = 0%; Supplementary Fig. S4), indicating that DSS concentration did not explain the observed heterogeneity.
IL-6
Eight studies quantified IL-6 levels in DSS-induced colitis. In a random-effects meta-analysis, exogenous cannabinoids significantly reduced IL-6 relative to controls (SMD = −3.79; 95% CI: −5.35 to −2.22; I2 = 82%; p < 0.00001; Fig. 4C). DSS concentration varied across studies (six at 4% and two at 2%). Stratification by DSS concentration indicated a larger reduction at lower induction intensity: 2% DSS (k = 2; SMD = −7.30; 95% CI: −9.59 to −5.01; I2 = 0%) versus 4% DSS (k = 6; SMD = −2.79; 95% CI: −4.14 to −1.44; I2 = 75%; Supplementary Fig. S5). The test for subgroup differences was significant (p = 0.009); however, this result is exploratory given the small 2% subgroup (k = 2) and residual heterogeneity within the 4% subgroup (I2 = 75%).
IL-1β
Three studies evaluated IL-1β levels in DSS-induced colitis. In the primary random-effects meta-analysis, cannabinoid treatment was associated with a large reduction in IL-1β that did not reach statistical significance (SMD = −4.12; 95% CI: −8.69–0.45; p = 0.08; I2 = 93%; Fig. 4D). Leave-one-out sensitivity analysis identified Silvestri et al. 42 as the most influential study, the exclusion of which reduced heterogeneity to 32% and rendered the pooled effect significant (SMD = −6.23; 95% CI: −8.23 to −4.23; p < 0.00001; Supplementary Fig. S6).
IL-10
Two studies assessed IL-10 levels in DSS-induced colitis. In the random-effects meta-analysis, exogenous cannabinoids did not significantly affect IL-10 (SMD = 1.43; 95% CI:
DNBS-Induced Models of IBD
Clinical outcomes
Colon weight-to-length ratio
Five studies evaluated the colon weight-to-length ratio in DNBS-induced colitis. Pooled analysis indicated that exogenous cannabinoids significantly reduced this ratio compared with controls (SMD = −2.66; 95% CI: −4.32 to −1.00; p = 0.002; I2 = 82%; Fig. 5A). Leave-one-out sensitivity analysis identified Pagano et al. 52 as the most influential study; excluding it reduced heterogeneity from I2 = 82% (p = 0.002) to I2 = 39% (p = 0.18), while the direction of the pooled effect remained unchanged.

Forest plots of clinical and molecular/inflammatory outcomes in DNBS-induced IBD models:
MPO activity
Five studies evaluated the MPO activity in DNBS-induced colitis. Pooled analysis indicated that exogenous cannabinoids significantly reduced this ratio compared with controls (SMD = −6.12; 95% CI: −9.99 to −2.26; p = 0.002; I2 = 83%; Fig. 5B). Leave-one-out sensitivity analysis identified Pagano et al. 52 as the most influential study, the exclusion of which reduced heterogeneity to 27% and rendered the pooled effect significant (SMD = −7.00; 95% CI: −9.16 to −4.84; p < 0.00001; Supplementary Fig. S7).
Molecular/Inflammatory outcomes
IL-1β levels
Three studies reporting IL-1β in DNBS-induced colitis were pooled with a random-effects model (I2 = 89%). Exogenous cannabinoids were associated with a reduction in IL-1β, but the overall effect did not reach statistical significance (SMD = −4.11; 95% CI: −8.31–0.09; p = 0.06; Fig. 5C). Leave-one-out analysis identified Pagano et al. 52 as the principal source of heterogeneity; its exclusion eliminated heterogeneity (I2 = 0%) and yielded a larger, more precise, and statistically significant effect (SMD = −6.14; 95% CI: −8.28 to −3.99; p < 0.00001; Supplementary Fig. S8).
IL-10 levels
Two studies that evaluated IL-10 levels in DSS-induced colitis were pooled using a fixed-effects model, given low-to-moderate heterogeneity (I2 = 40%; p = 0.20). The results indicated that exogenous cannabis significantly increased IL-10 relative to controls (SMD = 6.28; 95% CI: 4.04–8.52; p < 0.00001; Fig. 5D).
MDS
Evidence for MDS in the DNBS model is limited to a single study, 40 in which exogenous cannabinoids significantly reduced MDS compared with DNBS controls (mean ± SD: 2.11 ± 0.29 vs. 4.23 ± 0.27; MD = −2.12; 95% CI: −2.40 to −1.85).
TNBS-Induced Models of IBD
Clinical outcomes
MDS
Four studies assessing MDS in TNBS-induced colitis were synthesized using a random-effects model (I2 = 94%). Exogenous cannabinoids were associated with lower MDS, but the pooled effect was not statistically significant (SMD = −2.05; 95% CI: −4.23–0.13; p = 0.06; Fig. 6A).
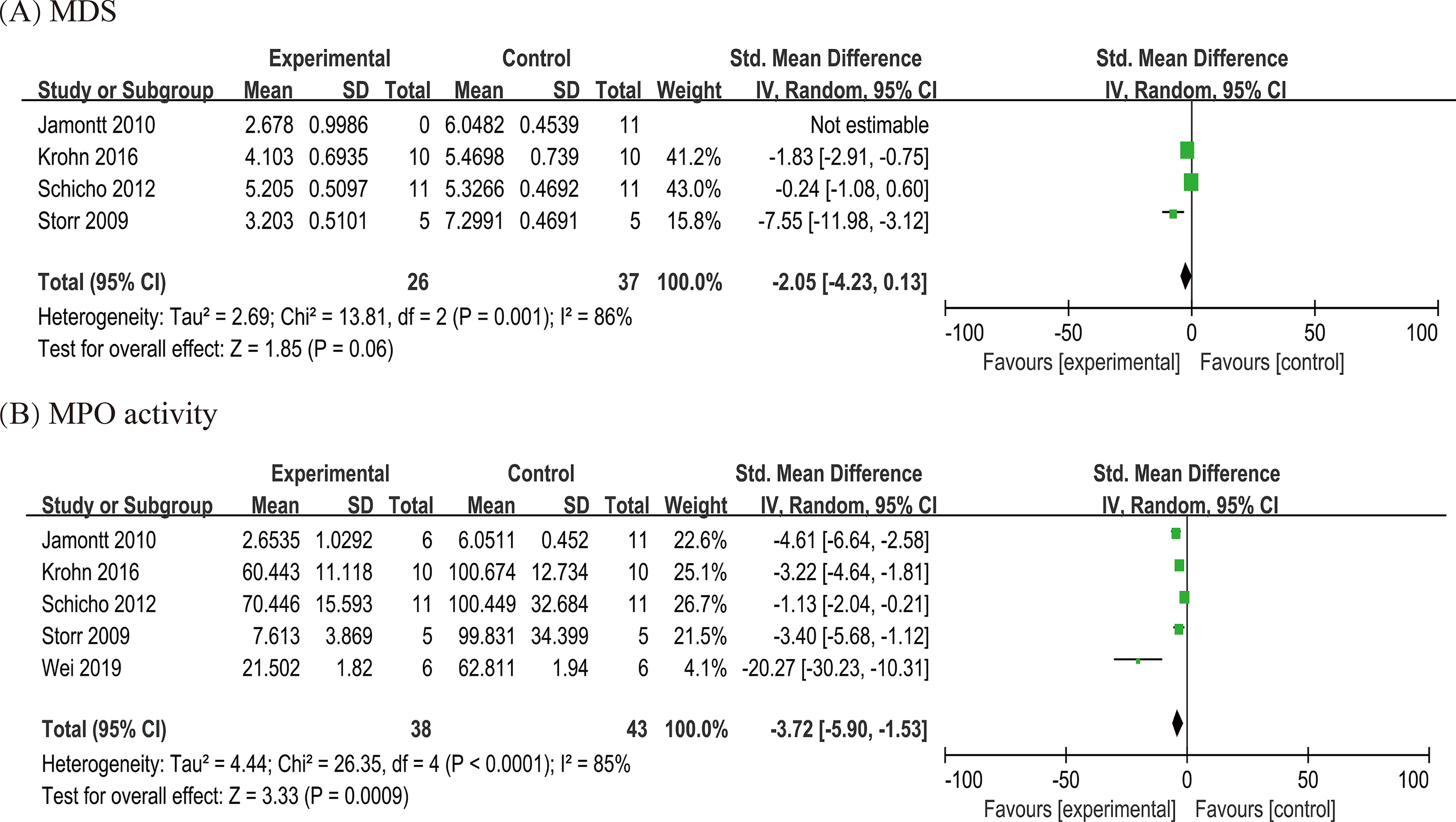
Forest plots of clinical and molecular/inflammatory outcomes in TNBS-induced IBD models:
Molecular/inflammatory outcomes
MPO activity
Five studies assessed MPO activity in TNBS-induced colitis. The results indicated a significant reduction in MPO activity following exogenous cannabinoid intervention (SMD = −3.72; 95% CI: −5.90 to −1.53; p = 0.0009; I2 = 85%; Fig. 6B).
Diet-Induced Models of IBD
Only one study reported the colon weight-to-length ratio. Under 4% DSS, treatment of exogenous cannabinoids reduced the ratio compared with DSS controls (mean ± SD: 55.49 ± 1.38 vs. 59.02 ± 1.32; MD = −3.53; 95% CI: −4.71 to −2.35).
Discussion
Summary of evidence
This meta-analysis synthesized 27 pre-clinical studies involving 408 animals to evaluate the therapeutic potential of exogenous cannabinoids in animal models of IBD. Pooled estimates showed significant reductions in DAI, histopathological and macroscopic damage scores, MPO activity, TNF-α, IL-6, IL-1β, and the colon weight-to-length ratio. By contrast, no consistent effect was observed for IL-10 or colon length. Methodological quality by SYRCLE’s risk-of-bias tool ranged from moderate to excellent, but interpretation is tempered by heterogeneity, small sample sizes, and incomplete reporting of randomization and blinding. Overall, the evidence supports anti-inflammatory and tissue-protective actions of exogenous cannabinoids in animal IBD and provides a biologically plausible rationale for more standardized, adequately powered pre-clinical studies and carefully designed early-phase clinical trials.
Possible mechanism
Anti-Inflammatory Effects
Our research indicates that exogenous cannabinoids may reduce levels of the pro-inflammatory cytokines IL-6, IL-1β, and TNF-α, suggesting their potential anti-inflammatory properties. The significant improvements in the DAI, histopathological score, MDS, and colon weight/length ratio further support its anti-inflammatory properties. Fichna et al. 43 revealed that cannabinoid receptor type 1 and cannabinoid receptor type 2 signaling pathways are both involved in the anti-inflammatory effects of cannabis. Upon exposure to various stimuli, nuclear factor kappa B (NF-κB) is activated and subsequently promotes the transcription of several pro-inflammatory cytokines. 60 Initially upregulated by NF-κB activation, IL-1β and TNF-α can further stimulate the NF-κB signaling pathway, thereby establishing a self-amplifying feedback loop that intensifies the inflammatory response. 61 Exogenous cannabinoids appear to suppress the classical NF-κB signaling cascade by modulating NF-κB p65 and phosphorylated IκB-α levels, which in turn downregulate pro-inflammatory mediator expression and mitigate colonic inflammation. 53 Neutrophils, key components of the inflammatory response, significantly contribute to the advancement of IBD. 62 Upon migrating in large numbers to the site of gastrointestinal inflammation, neutrophils secrete pro-inflammatory cytokines, which attract and activate other immune cells, further exacerbating local inflammation. 63 Neutrophils also contribute to intestinal injury by releasing proteases and reactive oxygen species (ROS), which impair epithelial barrier integrity and inflict direct tissue damage. 64 By increasing intestinal permeability, this disruption makes it easier for bacteria and other dangerous substances to enter the tissue, which strengthens the immune response. 65 In vivo studies by Fichna et al. 43 revealed that a synthetic cannabinoid attenuates neutrophil migration by suppressing chemotactic responsiveness. Similarly, Krohn et al. 45 observed that a synthetic cannabinoid significantly interferes with the inflammatory recruitment of neutrophils. Translational studies are needed to confirm these observations in clinical contexts and elucidate their mechanistic basis.42,52
Antioxidative Stress
MPO is a critical enzyme involved in ROS-mediated tissue injury, primarily by catalyzing the production of ROS. 66 Its activity serves as a biomarker of neutrophil infiltration and oxidative stress severity in inflammatory conditions. 67 Our findings demonstrate that exogenous cannabinoids effectively inhibit MPO activity, suggesting their potential to mitigate intestinal oxidative stress. Excessive ROS production drives oxidative stress, contributing to IBD pathogenesis by damaging cellular components, activating pro-inflammatory signaling cascades, and compromising the intestinal epithelial barrier. 68 It has been shown that phytocannabinoids can directly suppress ROS generation,40,49 thereby alleviating oxidative stress and its associated inflammatory and barrier-disrupting consequences. The transcription factor Nrf2 and its downstream target HO-1 are pivotal in counteracting oxidative stress in IBD. 69 Wang et al. 53 identified a correlation between the antioxidant efficacy of phytocannabinoids and the stimulation of the Nrf2 pathway, as evidenced by elevated Nrf2 expression and the regulation of HO-1 gene transcription.
Barrier Protection
Our research suggests that exogenous cannabinoids can improve histopathological score, indicating their potential to enhance intestinal barrier function. The integrity of the intestinal barrier is crucial in the etiology and progression of IBD. 70 In a study by Borrelli et al., 49 FITC-conjugated dextran was used to evaluate the protective effect of phytocannabinoids on intestinal permeability. They found that phytocannabinoids alleviated the increase in intestinal permeability induced by colitis and helped restore the integrity of the intestinal epithelium. Transient receptor potential ankyrin 1 (TRPA1) confers protection against intestinal inflammation. 71 Phytocannabinoids may help restore intestinal barrier integrity under inflammatory conditions by downregulating TRPA1 expression. This impact is correlated with reduced levels of pro-inflammatory cytokines, such as IL-1β and IL-6, as well as the chemokine MCP-1. 47 In addition, phytocannabinoids may help restore intestinal barrier integrity by indirectly modulating microbial dysbiosis. 47 Interestingly, the effect of synthetic cannabinoids on improving the intestinal barrier does not appear to involve the TLR4 pathway. 57
Implications for clinical trial
This study provides preliminary evidence supporting the therapeutic potential of exogenous cannabinoids for IBD, owing to their capacity to attenuate mucosal injury and modulate pro-inflammatory cytokine responses in pre-clinical models. However, translating pre-clinical findings to clinical applications remains a challenge, as it is difficult to predict the effectiveness of treatments in human trials based solely on animal models.72,73 Key factors such as differences in drug doses, administration schedules, and the physiological variations between humans and animals contribute to the challenges of translating research from the bench to the bedside. 74 Given these disparities, methodologically robust randomized controlled trials involving exogenous cannabinoids for IBD are essential to confirm their efficacy in patients.
Strengths and limitations of the current study
This meta-analysis is the first to systematically synthesize and evaluate pre-clinical evidence regarding the efficacy of exogenous cannabinoids in experimental models of IBD. Systematic reviews, such as this one, are essential for enhancing the design of pre-clinical studies and ensuring the clinical relevance of findings. In addition, they facilitate the refinement of experimental protocols, minimizing unnecessary studies and optimizing the exploration of exogenous cannabinoids’ potential therapeutic value for IBD. All relevant studies that meet the inclusion criteria have been incorporated into this review.
Several potential limitations of this meta-analysis merit consideration. First, while a systematic approach was employed in preparing this review, it is possible that some relevant studies were not included, leading to a potential limitation in the comprehensiveness of the data. Second, data extraction software was used to extract information rather than raw data, which may introduce a degree of error. Third, the quality of the included studies varied significantly, with most studies lacking detailed explanations of randomization methods and the implementation of blinding during the experimental process. Finally, heterogeneity was observed in the outcome measures, which may affect the overall reliability of the findings. Moreover, clinical and pre-clinical evidence regarding genetic background-related IBD animal models is relatively scarce in the literature included in this study, which results in the findings being somewhat more dependent on chemically induced models. These constraints may limit the extrapolation of the conclusions to genetically susceptible populations or specific molecular mechanisms.
Conclusions
Our meta-analysis demonstrated that exogenous cannabinoids significantly reduced DAI score, histopathological score, TNF-α, MPO activity, IL-6, IL-1β, MDS, and the colon weight-to-length ratio. The potential protective mechanisms identified in animal model studies include anti-inflammatory and antioxidant effects. In conclusion, pre-clinical findings support the therapeutic promise of exogenous cannabinoids in the management of IBD. However, given the limitations in animal experimental design and the quality of the available evidence, the current findings may not fully translate to clinical contexts. Future research, characterized by more rigorous experimental design and comprehensive investigation, is necessary to confirm its clinical efficacy and to elucidate the molecular pathways through which it mediates therapeutic effects in IBD.
Authors’ Contributions
S.W. and X.L. conducted the literature search, study selection, and risk-of-bias assessment. Any discrepancies regarding the risk of bias were resolved in consultation with L.G., F.L., and C.W., who contributed to data extraction and interpretation. Y.L. was responsible for figure preparation and data visualization. S.W. prepared the initial article draft. L.G. supervised the entire project and reviewed the article for intellectual content. The final text version was read and approved by all authors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No external funding was provided for this study.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.