
Abstract
Background:
We explored whether self-reported current cannabis use is associated with inflammatory biomarkers among people with HIV (PWH), given high rates of cannabis use and chronic immune activation among PWH.
Methods:
At seven Centers for AIDS Research Network of Integrated Clinical Systems (CNICS) cohort sites, which integrate data on participant characteristics including demographic and clinical information, and substance use behaviors, we used linear regression to estimate the average difference in biomarkers associated with cannabis use, adjusted for demographic characteristics and sampling weights. Cannabis use was considered as Never, Former, or Current (past 3-month) use. Thirteen plasma biomarkers were measured once on or after 2010 among a subset of PWH on antiretroviral therapy with HIV viral suppression within CNICS. Cannabis use was assessed within 1 year prior to biomarker collection. Biomarkers were log-transformed and scaled by standard deviation to standardize estimates.
Results:
Among 532 PWH, the average age at biomarker collection date was 47 years, 84% were male, 61% non-White, 30% reported current cannabis use, 35% former use, and 35% never using cannabis. In adjusted linear regression, current cannabis use was associated with higher soluble CD14 (sCD14) levels (β = 0.35; 95% confidence interval [CI]: 0.09, 0.61). Former cannabis use was associated with lower C-reactive protein (CRP) (β = −0.25; 95% CI: −0.47, −0.04), although current use was not (β = −0.25; 95% CI: −0.51, 0.01) compared to never use.
Conclusions:
Cannabis use may be related to lower CRP and elevated markers of microbial translocation (e.g., sCD14), which could have implications in increasing the risk of vascular events and should be investigated in a longitudinal setting.
Background
In the current era of HIV care with advanced antiretroviral therapy (ART), HIV has become a long-term, treated condition with life expectancies of people with HIV (PWH) approaching that of the general population.1,2 However, PWH are at a higher risk of comorbidities, including cardiovascular disease (CVD), diabetes, several cancers, and aging-related illnesses.3,4 The rise in comorbidities has been attributed, in part, to chronic immune activation related to ART side effects, low-level HIV viremia, and behaviors such as substance use.3,5 There is a growing awareness of the importance of inflammation among PWH, given the array of adverse consequences with focuses on identifying factors that contribute a large inflammatory impact and approaches to mitigating chronic immune activation.3,5,6
Among PWH in the United States, substance use is highly prevalent; cannabis use has been observed as the most commonly used drug (except for nicotine/cigarette use and alcohol consumption), with estimates ranging between one-quarter to one-third of PWH reporting past 3-month use.7,8 Comparatively, estimates of past-year cannabis use in the general population range from 11% to 23%.8,9 PWH report using cannabis both recreationally and as symptom management, such as for pain or anxiety.10–13 Concerns regarding cannabis use include impaired judgment or risky behavior, poorer engagement in HIV care (e.g., lower adherence to ART), and clinical impacts such as chronic bronchitis.14–17
Cannabis has repeatedly been evaluated as a factor in the inflammatory response and, notably, as a potential anti-inflammatory agent, although findings have been mixed across panels of biomarkers.13,18–23 For example, studies on cannabis and C-reactive protein (CRP), a marker of generalized inflammation, have reported null or lower levels of the marker associated with cannabis use.20–22 In addition, several biomarkers of microbial translocation, a process by which gut microbes enter the circulatory system and increase overall inflammation, have been associated with cannabis use, including lower levels of lipopolysaccharide (LPS) binding protein (LBP) and higher levels of soluble CD14 (sCD14), and one study observed fluctuations in both LPS and sCD14 over time.24–30 Ultimately, investigators continue to hypothesize the anti-inflammatory role cannabis may have, but further research remains necessary, given the majority of studies have been small, thus limited in geographic/demographic diversity, and mixed findings complicate interpretations.21,27–30 Therefore, we explored this association using a panel of inflammatory biomarkers measured among PWH engaged in care with controlled HIV across the United States.
Methods
Study setting
This study took place in the Centers for AIDS Research Network of Integrated Clinical Systems (CNICS) cohort. 31 CNICS is a nationwide cohort of adult PWH engaged in care at 10 academic clinical sites; 7 sites with relevant data (e.g., biomarkers, cannabis use) were included in this study. 31 CNICS collects data on a wide range of participant characteristics including demographic information, clinical inpatient and outpatient data, and patient-reported outcomes (PROs) including cannabis and other substance use behaviors. A centralized data repository harmonizes all CNICS data domains. Each CNICS site has local institutional review board approval, which allows for secondary analysis of deidentified data.
CNICS operates several substudies, including a case-cohort study on inflammatory biomarkers. This case-cohort study was developed to evaluate cardiovascular events among PWH in CNICS who had a stored plasma sample and attained low-level HIV viremia with a maximum cutoff of 400 copies/mL prior to the plasma sample. The case-cohort sampling procedures have been described in detail elsewhere. 32 We used this case-cohort study to consider how cannabis use may impact plasma inflammatory biomarkers.
Data collection
The panel of 13 plasma biomarkers were measured at a single timepoint on or after 2010 through 2018 among PWH in the case-cohort. Cryopreserved plasma was assessed in duplicate for the following immunoassays representing discrete and overlapping inflammation and immune activation pathways known to be abnormal in HIV and associated with morbidity. In particular, gut epithelial barrier dysfunction as well as monocyte activation, which causes monocyte tissue factor expression, activating the coagulation cascade and increasing d-dimer levels, predict early mortality and CVD in PWH. 33 Several individual markers, including sCD14, soluble tumor necrosis factor receptors 1 and 2 (sTNFR1 and sTNFR2), interleukin-6 (IL-6), CRP, soluble urokinase plasminogen activator receptor (suPAR), and kynurenine/tryptophan (KT) ratio, have been associated with mortality and non-AIDS-defining comorbid events in this population.34–39 In addition, soluble CD163 (sCD163) has been associated with noncalcified coronary plaque, and suPAR has been associated with elevated MI risk in PWH.40,41 CRP, IL-6, interferon-inducible protein 10 (IP-10 or CXCL10), sTNFR1, sTNFR2, suPAR, and intercellular adhesion molecule 1 (ICAM-1) were all assessed via MesoScale Diagnostics (Rockville, MD); and interleukin-18 (IL-18), LPS-binding protein (LBP), sCD14, sCD163, all R&D Systems (Minneapolis, MN); and anti-cytomegalovirus (CMV) IgG index (Genway, San Diego, CA). Plasma KT ratio was assessed via high-performance liquid chromatography tandem mass spectrometry. Each biomarker was log2-transformed and standard deviation-scaled for analyses to standardize estimates.
Cannabis use and use of other substances were measured using PRO data collected on or before the biomarker specimen date up to 1 year (365 days) prior to specimen collection. Cannabis use status was considered as a three-level variable: Never, Former, or Current (past 3-month) use. Tobacco smoking was considered as a four-level variable: Never, Former, Current, or Missing. Illicit drug use was dichotomized as Never or Ever use of methamphetamine, cocaine/crack, or illicit opioids. Alcohol use was categorized into three levels based on Alcohol Use Disorder Identification Test-Consumption (AUDIT-C) scores: No current use (score: 0), Current nonhazardous use (score: 1–3 for female; 1–4 for male), or Current hazardous use (score: ≥4 for female; ≥5 for male). In summary, PWH in the biomarkers case-cohort who reported on their cannabis use within 1 year prior to their biomarker specimen date were eligible for this study.
Clinical information, such as HIV RNA levels, body mass index (BMI), dyslipidemia (based on statin treatment), LDL cholesterol level, and diagnoses including hepatitis C virus (HCV; defined as any lifetime positive result from an HCV antibody, RNA, or genotype test), is available in the CNICS data repository and was used as adjustment factors in analysis.
Statistical analysis
We used linear regression models to estimate the average difference in log-transformed and standard deviation-scaled biomarkers associated with cannabis use status, adjusted for age, sex, and race/ethnicity, with sampling weights to account for the design of the biomarker case-cohort study.
We also conducted several sensitivity analyses; each variation in adjustment was a separate analysis. We additionally adjusted for tobacco smoking status and illicit drug use, as well as for alcohol use. The case-cohort eligibility criteria included HIV viral load <400 copies/mL, so we further adjusted for viral suppression at 50 copies/mL to consider more modern cut points of viral suppression. We additionally adjusted for HCV and CMV IgG to consider the impact of other infections. We also adjusted for BMI category (<18.5, 18.5–24.9, 25.0–29.9, ≥30.0 kg/m2), and dyslipidemia. We adjusted for LDL cholesterol in an sCD14 model. Finally, we evaluated the potential impact of outliers by restricting analyses to the bottom 99% of biomarker values.
Results
Among the 532 PWH who were eligible for this study, the average age at biomarker specimen date was 47 years (median: 47, interquartile range: 39–54). Most PWH were male (84%) and non-White (61%) (Table 1). Thirty percent of PWH reported current cannabis use, whereas 35% reported former use, and 35% reported never using cannabis.
Demographic and Clinical Characteristics of People with HIV with Plasma Biomarker Specimen by Cannabis Use Status
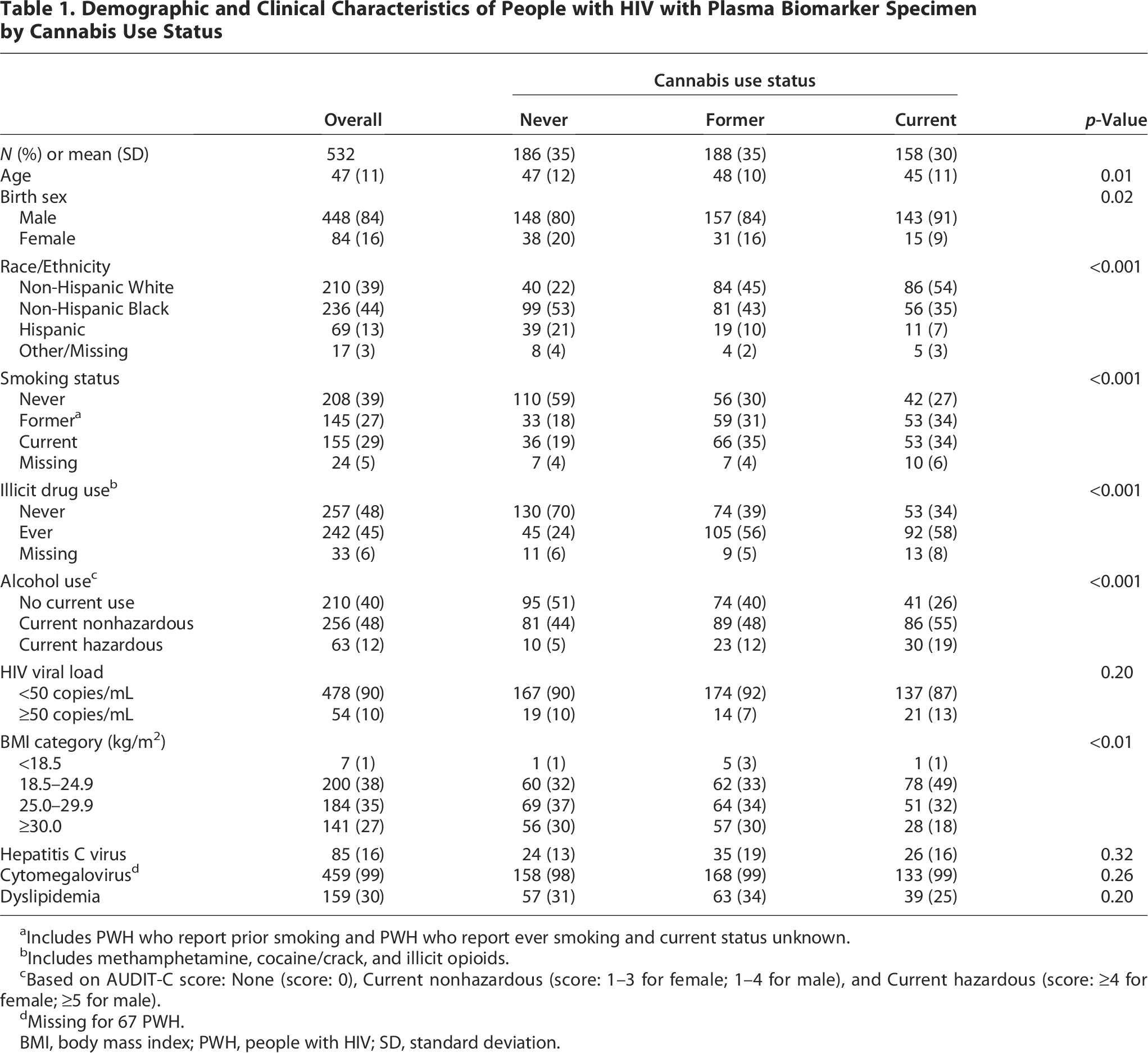
Includes PWH who report prior smoking and PWH who report ever smoking and current status unknown.
Includes methamphetamine, cocaine/crack, and illicit opioids.
Based on AUDIT-C score: None (score: 0), Current nonhazardous (score: 1–3 for female; 1–4 for male), and Current hazardous (score: ≥4 for female; ≥5 for male).
Missing for 67 PWH.
BMI, body mass index; PWH, people with HIV; SD, standard deviation.
In our primary adjusted models, current cannabis use was associated with higher sCD14 levels (β = 0.35; 95% confidence interval [CI]: 0.09, 0.61, p = 0.008) compared to never using cannabis (Fig. 1). Former cannabis use was associated with lower CRP levels (β = −0.25; 95% CI: −0.47, −0.04, p = 0.020), and current cannabis use was nonsignificantly associated (β = −0.25; 95% CI: −0.51, 0.01, p = 0.058). Cannabis use was marginally (p < 0.1) associated with some other biomarkers, such as the KT ratio and sCD163, as well.
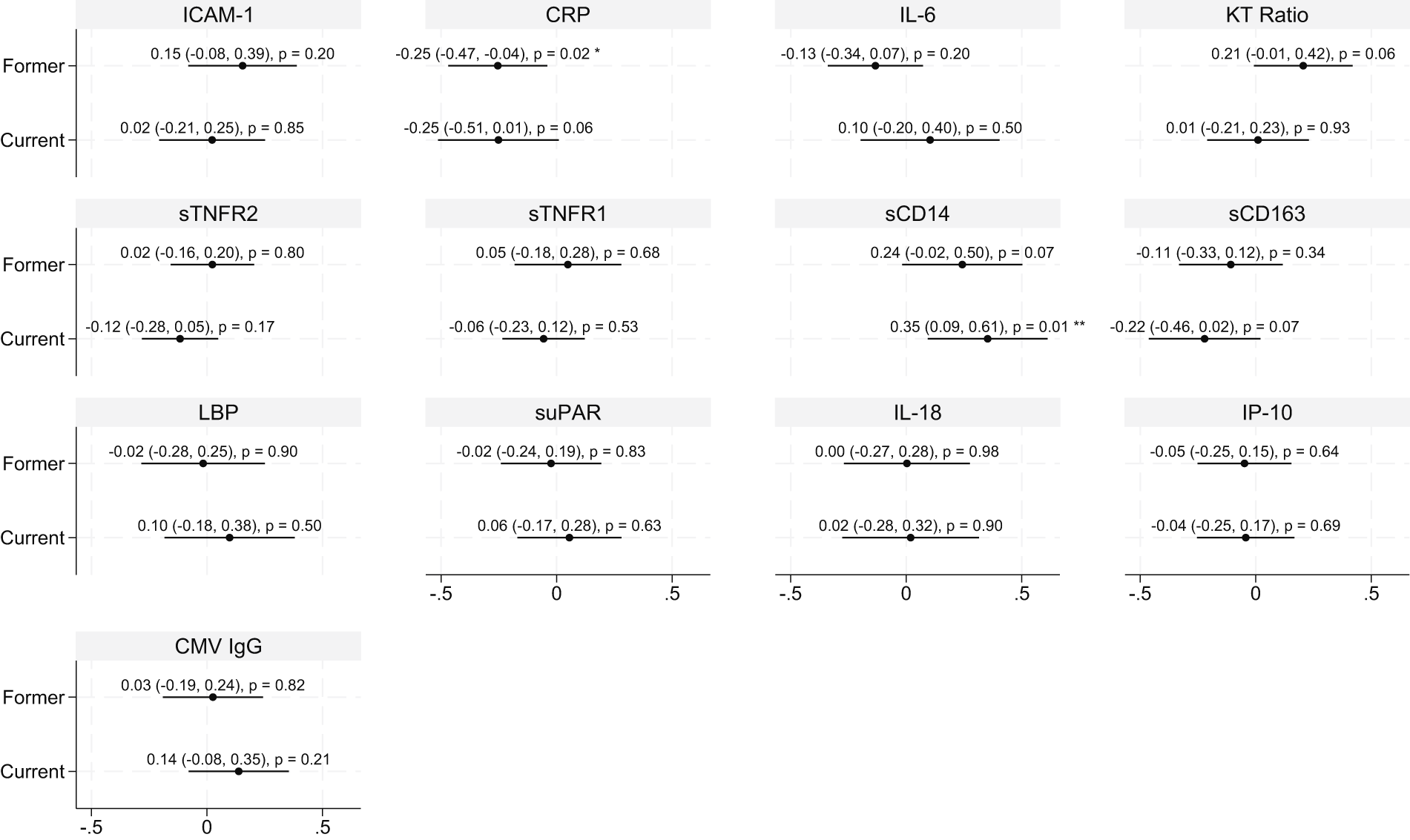
Forest plots for the association between cannabis use (reference: Never use) and standard deviation-scaled log-transformed biomarkers using linear regression adjusted for age, sex, race/ethnicity, and sampling weighted. N = 532. **p < 0.01; *p < 0.05. CRP, C-reactive protein; CMV IgG, anti-cytomegalovirus IgG index; ICAM-1, intercellular adhesion molecule 1; IL-6, interleukin-6; IL-18, interleukin-18; IP-10, interferon-inducible protein 10; KT ratio, kynurenine/tryptophan ratio; LBP, lipopolysaccharide binding protein; sTNFR2, soluble tumor necrosis factor receptor 2; sTNFR1, soluble tumor necrosis factor receptor 1; sCD14, soluble CD14; sCD163, soluble CD163; suPAR, soluble urokinase plasminogen activator receptor.
These findings were mostly consistent in sensitivity analyses. CRP and sCD14 were robust to additionally adjusting for smoking and illicit drug use, adjusting for alcohol use, adjusting for HIV viral load at <50 copies/mL, adjusting for other viruses (HCV, CMV), adjusting for BMI, adjusting for dyslipidemia, and excluding the top 1% of biomarker values (Supplementary Figures S1, S2, S3, S4, S5, S6, and S7). Current cannabis use was associated with lower CRP with statistical significance when we adjusted for HIV VL at <50 (β = −0.26; 95% CI: −0.52, −0.01, p = 0.045) and when excluding the top 1% of biomarker values (β = −0.26; 95% CI: −0.51, −0.01, p = 0.045). Some biomarkers were newly statistically significant with additional adjustment for substance use and viruses, such that current cannabis use was associated with lower sCD163 and marginally associated with lower sTNFR2 (Supplementary Figs. S1 and S3). In the model for sCD14, additionally adjusting for LDL cholesterol, estimates were stable: former (β = 0.23; 95% CI: −0.04, 0.49, p = 0.092), and current (β = 0.34; 95% CI: 0.07, 0.60, p = 0.014) cannabis use remained associated with elevated sCD14.
We did not observe statistically significant associations between cannabis use and the following biomarkers: ICAM-1, IL-6, sTNFR1, LBP, suPAR, IL-18, IP-10, or CMV IgG titer.
Discussion
We found that cannabis use was associated with a subset of plasma inflammatory biomarkers among a panel of 13, including higher sCD14 and lower CRP, in a cohort of PWH with suppressed HIV. sCD14 is a marker of innate immune activation, including from microbial translocation, and elevated sCD14, which has been previously identified in the context of cannabis use, may have implications in increasing the risk of CVD and mortality.28,29,42,43 Alternatively, our observation of lower levels of CRP, which is also consistent with prior work, highlights possible anti-inflammatory properties of cannabis.21–23 Most other biomarkers in this panel were not associated with cannabis use, although some sensitivity analyses suggested marginal associations, such as higher KT ratio and lower sTNFR2 and sCD163. This study used only a single measure for each biomarker, so further analysis incorporating longitudinal data, and particularly including repeated measures of the biomarkers, would help clarify these findings.
Inflammation among PWH is a continually growing area of research, with reports highlighting the link between chronic immune activation and heightened risk of many comorbidities (e.g., CVD, cancers).3,4 Microbial translocation has been a focal point of this work; disruption of the gut microbiome is well-known among PWH, and the range of related outcomes is broad, including frailty, diabetes, CVD, and mortality.26,34,37 Minimizing generalized inflammation and targeting specific pathways of inflammation (e.g., microbial translocation) could offer widespread benefit to the overall health of PWH.
Prior work on cannabis and markers of microbial translocation has reported mixed results. A pilot clinical trial on eight PWH evaluated the effect of orally administrated cannabinoid-based treatment on inflammation and found several signatures of decreased inflammation (e.g., sTNFR2) as well as several instances of fluctuations in levels during the observation period, which included periods of elevated inflammatory markers, such as for LBP and sCD14. 30 Another study among 107 PWH identified that heavy cannabis use was associated with lower levels of LBP. 27 Yet, others found elevated sCD14 associated with cannabis among PWH who also use methamphetamine and cocaine.28,29
Indeed, not all markers related to microbial translocation were consistently elevated or reduced in our analyses; higher sCD14 was a primary finding, while LBP was null, and the KT ratio was marginally elevated. However, microbial translocation, and specifically the relationship between LPS/LBP and sCD14, remains complex, as the levels of each do not always correlate (e.g., sCD14 has been associated with higher and lower levels of LPS).25,26 sCD14 can also be elevated in response to other toll-like receptor 4 (TLR4) ligands including oxidized LDL, but we observed very little attenuation of the cannabis association after LDL adjustment in our models (main model without LDL: former cannabis use: [β = 0.24; 95% CI: −0.02, 0.50, p-value: 0.067], current cannabis use: [β = 0.35; 95% CI: 0.09, 0.61, p-value: 0.008]; with LDL adjustment: former cannabis use: [β = 0.23; 95% CI: −0.04, 0.49, p-value: 0.092], current cannabis use: [β = 0.34; 95% CI: 0.07, 0.60, p-value: 0.014]). 44 Similarly, while obesity in PWH has been associated with decreased sCD14, adjustment for BMI also failed to attenuate the association between cannabis and sCD14, suggesting that the cannabis–sCD14 relationship is independent of these factors (Supplementary Fig. S4). 45
It is also important to acknowledge the possibility that the intensity of cannabis use may affect biomarker associations. Moderate cannabis use might reduce intestinal inflammation, while heavy or chronic cannabis use may instead diminish microbial diversity and richness, resulting in exacerbated intestinal and systemic inflammation.46,47 There is likely a mix of moderate and heavy cannabis use in the present sample, leading to some overlap of these two possible effects, which helps explain the inconsistent directions of associations for related markers. Several studies have converged on the hypothesis that a comprehensive investigation into the gut microbiome and dysbiosis could help clarify this complex relationship.27–30 Microbial translocation has been implicated in a greater risk of several poor health outcomes, and elevated sCD14 and KT ratio may further increase the risk of comorbidities such as CVD and diabetes.26,42,43 These risks are nontrivial, and opportunities to reduce such outcomes should be carefully considered, even if there are competing factors, such as the potential anti-inflammatory properties of cannabis.
We found lower levels of CRP associated with former, and marginally with current, cannabis use, which is consistent with much of the existing literature reporting a mix of lower levels of CRP and null associations.20–23,27 Similarly, one study that carefully measured cannabis metabolites found lower T cell activation in heavy users. 48 The theorized immunoregulatory pathway involves cannabinoid receptor 2 (CB2) in immune tissue cells interacting with cannabis metabolites, leading to lower inflammation.49,50 Although pathways are still being identified, both Δ9-tetrahydrocannabinol and cannabidiol (CBD), which are natural cannabinoids in cannabis, may induce anti-inflammatory processes by the CB2 receptor via reduction of IL-1β. 51 CBD may also operate through inhibition of the NLRP3 inflammasome and subsequent reduction of nuclear factor kappa B (NK-κB). 51 Lower CRP, which is indicative of lower generalized inflammation and related to these inflammasomes, could be a signal of this process. 52 Reducing levels of CRP could have significant clinical benefit, as elevated CRP has been associated with poor health outcomes among PWH, including myocardial infarction and frailty.32,37 It is also important to note that we do not have data on the exact timing of the most recent use of cannabis, and studies that collect that data could improve inference into relationships with biomarkers that are highly sensitive and change quickly.
There are additional limitations to this study as well. Our biomarker samples were only collected at a single timepoint; therefore, we could not evaluate changes over time, which remains important to understand trajectories and long-term impacts. 30 Future work could also consider whether biomarkers fluctuate after cessation of cannabis use. We did not have access to biologically measured cannabis use; however, we used self-reported information taken from a widely accepted tablet-based platform with good properties for accurate collection (i.e., minimal concern of social desirability bias impacting reporting). 53 We also did not have complete information regarding severity/intensity of use, potency of cannabis, or route of use (e.g., orally ingested, smoked, vaped); however, we assume that most PWH smoke cannabis. 54
Several unique and novel aspects of this study contribute to our understanding of the relationship between cannabis use and inflammation among PWH. Strengths of this study include the geographic and demographic diversity (e.g., 16% female) of the cohort, including seven clinical sites across the United States and a representation across race/ethnicity groups. The richness of CNICS data aided in our depth of analysis; we were able to consider the use of other substances as well (tobacco cigarette smoking, illicit drug use, alcohol use) beyond the main cannabis exposure as well as several clinical factors (coinfections, BMI) that may influence inflammation. Finally, we were able to specify the temporality of cannabis use prior to measurement of plasma biomarkers and restricted collection of cannabis report to within 1 year of biomarker specimen date to minimize measurement error while maintaining a reasonable sample size (N > 500).
Legalization of cannabis continues to occur across the United States; currently, recreational cannabis use is legal in 24 states. Prior work has found negligible changes in prevalence or severity of use following legalization among adult PWH, although cannabis use remains common in this population.7,8,55 Indeed, the plethora of potential benefits (e.g., anxiety and pain reduction, appetite stimulant) from cannabis use among PWH should not be ignored; however, the potential increases in inflammation could be detrimental and also must be considered as factors in the utility of cannabis as a therapeutic resource. 56 Moderate cannabis use may offer beneficial anti-inflammatory properties and protection to microbial integrity; however, chronic or problematic use may induce the opposite, pro-inflammatory impacts.46,47 This is an important distinction in the setting of HIV, as this population reports high substance use and often at problematic levels, such as dependence. 8 These findings offer additional evidence in this complex relationship, in that they support potential anti-inflammatory properties of cannabis, as well as the role of microbial translocation, indicated by elevated sCD14, as an important area of focus in considerations for care.
Conclusion
We observed both higher and lower inflammatory biomarkers associated with cannabis use among PWH, suggesting a combination of mechanisms that impact various inflammatory pathways. Cannabis use may be related to lower generalized inflammation, characterized by CRP. In addition, cannabis may be linked with increased microbial translocation, indicated by sCD14. Both relationships could have further downstream impacts on the overall health of PWH. These findings should be further investigated in a longitudinal setting.
Authors' Contributions
S.A.R.: Conceptualization, Methodology, Writing, Formal analysis; J.A.C.D.: Conceptualization, Methodology, Writing—R&E, Funding acquisition; K.A.C.: Writing—R&E, Funding acquisition; E.F.A.: Writing—R&E; B.M.W.: Writing—R&E, Data curation; S.N.: Writing—R&E, Data curation; L.B.: Writing—R&E, Data curation; M.S.S.: Writing—R&E, Data curation, Funding acquisition; R.D.M.: Writing—R&E, Data curation; K.H.M.: Writing—R&E, Data curation; I.P.: Writing—R&E; A.D.: Writing—R&E; C.G.: Writing—R&E; F.F.: Writing—R&E; M.M.K.: Writing—R&E, Data curation, Funding acquisition; H.M.C.: Writing—R&E, Data curation, Funding acquisition; P.W.H.: Writing—R&E, Conceptualization, Data curation, Funding acquisition.
Author Disclosure Statement
The authors report no potential conflicts of interest, including relevant financial interests, activities, relationships, and affiliations.
Footnotes
Funding Information
This work was supported by the National Institutes of Health:
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.