
Abstract
Background:
California legalized medical cannabis in 1996 and nonmedical adult use in 2016, with commercial recreational sales starting in 2018. The consequences of cannabis legalization and commercialization on medical cannabis utilization are not well understood.
Methods:
We analyzed data from 178,832 adults (aged ≥18 years) in the California Health Interview Survey (2017–2024). Past-month cannabis use and doctor-recommended use were assessed each year. We fit survey-weighted logistic regression models with year as a categorical predictor, used omnibus Wald tests to assess whether prevalence differed across years, and estimated year-to-year differences with Tukey-adjusted contrasts. All analyses accounted for survey weights, strata, and primary sampling units.
Results:
Between 2019 and 2024, about 1.6% of all respondents and 16.4% of past-month cannabis users reported doctor-recommended use. Among past-month users, doctor-recommended use fell from 18.5% (95% Confidence Interval [CI]: 16.6%–20.4%) in 2019 to 8.5% (95% CI: 7.3%–9.8%) in 2024 (p < 0.01). Overall past-month cannabis use held steady, at 16.5% (95% CI: 15.5%–17.6%) in 2019 and 15.4% (95% CI: 14.5%–16.2%) in 2024 (p = 0.22). Tukey-adjusted comparisons showed the decline was most apparent from 2021 onward. The pattern held across sex and most age and racial/ethnic groups, though differences did not reach statistical significance among young adults aged 18–25 (–7.6 percentage points; p = 0.09), Asian respondents (–2.9 percentage points; p = 0.62), or African American respondents (–8.8 percentage points; p = 0.47).
Discussion:
After adult-use legalization and commercialization, doctor-recommended use decreased by more than half among past-month cannabis users, even as overall use remained stable. The decline in doctor-recommended use suggests that legalization and commercialization in California may have altered patterns of medical utilization without reducing population-level use. Together, these findings align with broader national trends in which recreational access may be displacing formal medical oversight. This reduction in physician oversight raises the concern that individuals with complex medical conditions may increasingly rely on the recreational marketplace without the benefit of clinician guidance.
Introduction
Over the past decade, cannabis policies in the United States have undergone rapid and significant changes. As of mid-2025, 40 U.S. states, three territories (Puerto Rico, Guam, and the U.S. Virgin Islands), and the District of Columbia have implemented regulations that allow for medical use of cannabis by adults (≥21 years of age). Twenty-four states regulate cannabis for nonmedical use by adults.1–3
California first legalized cannabis for medical use in 1996, with the Compassionate Use Act (Proposition 215), allowing physician-qualified patients who met specific clinical criteria defined by the state to purchase, possess, and cultivate cannabis for therapeutic use. 4 Subsequently, California legalized nonmedical use for adults (≥21 years) in November 2016 under the Adult Use of Marijuana Act (Proposition 64), with commercial sales beginning January 1, 2018. 5 This policy shift established new incentives for formalized medical use, including exemption from state excise and local sales taxes and the ability to possess cannabis in greater quantities than recreational users. In contrast, a physician qualification is no longer required to purchase cannabis in California, thus eliminating a pre-existing incentive.
The consequences of recreational cannabis legalization and commercialization on medical cannabis utilization are not well understood. Preliminary reports from other states have documented subsequent declines in formal medical cannabis registry enrollment following recreational legalization.6,7 Using data from the California Health Interview Survey (CHIS), this report describes changes in the prevalence of doctor-recommended cannabis use in California between 2019 and 2024, contextualizing these shifts against overall past-month cannabis use trends.
Methods
Study population
The CHIS is the largest state-level health survey in the United States, conducted by the University of California, Los Angeles (UCLA) Center for Health Policy Research. 8 CHIS is a continuous, population-based survey that used computer-assisted telephone interviews with a dual-frame random-digit-dialing design prior to 2019 and since 2019 has employed an address-based sampling design with mixed web and telephone administration to achieve representation from all 58 counties in California. Within sampled households, one adult respondent is randomly selected. Annual CHIS adult response rates ranged from 2.9% in 2019 to 7.4% in 2024. Population weights are incorporated based on California Department of Finance estimates. These weights address unequal sampling probabilities and nonresponse biases inherent in complex survey designs.
Independent variables
Cannabis use
Cannabis use was evaluated using CHIS data collected from 2017 to 2024. Past-month cannabis use (2017–2024) was assessed among those reporting ever using cannabis and determined by the question, “During the past 30 days, on how many days did you use marijuana, hashish, or another THC product?” Those who reported greater than 0 days were classified as past-month users and asked additional questions, including “Was any marijuana use recommended by a doctor or health care provider?,” categorized as “Yes” or “No.” For additional methods, see Supplementary Data.
Statistical methods
The analytic sample (n = 178,832) included respondents who completed cannabis-related questions, drawing from combined annual data files spanning 8 years (2017–2024). Person-level sampling weights, strata, and primary sampling units were applied to all analyses to account for the complex survey design. Descriptive statistics were reported as unweighted counts and weighted percentages. Survey-weighted logistic regression models were fitted with year included as a categorical predictor, and omnibus Wald tests were used to assess whether prevalence differed significantly across years. Subsequent analyses, which included estimation of pairwise contrasts between years using marginal means with Tukey adjustment for multiple comparisons, were conducted using the same survey-weighted framework. Models used a quasibinomial family to obtain robust variance estimates in the presence of potential overdispersion. All analyses were performed in R (Version 4.5.2).
Results
Between 2019 and 2024, approximately 1.6% (n = 3132) of all respondents and 16.4% of past-month users reported that at least some of their past-month cannabis use was recommended by a doctor (Table 1).
Characteristics of Adults in California by Cannabis Use Status
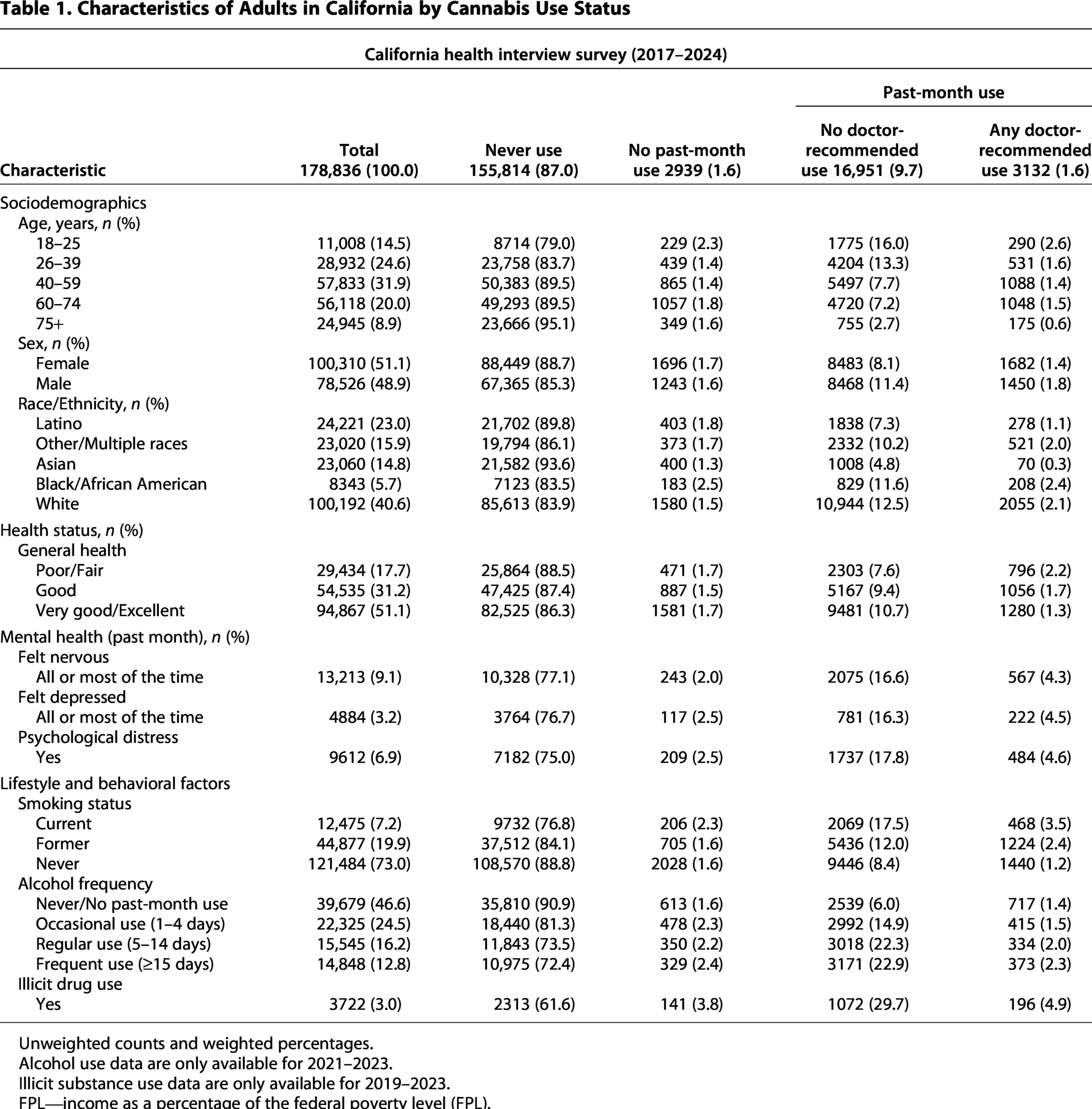
Unweighted counts and weighted percentages.
Alcohol use data are only available for 2021–2023.
Illicit substance use data are only available for 2019–2023.
FPL—income as a percentage of the federal poverty level (FPL).
Trends in doctor-recommended use
The weighted prevalence of doctor-recommended cannabis use in the past month declined sharply from 18.5% (95% CI: 16.6%−20.4%) in 2019 to 8.5% (95% CI: 7.3%−9.8%) in 2024 (p < 0.01; Fig. 1). This decline occurred despite the overall prevalence of past-month cannabis use remaining essentially stable during this period, ranging from 16.5% in 2019 (95% CI: 15.5–17.6) to 15.4% in 2024 (95% CI: 14.5–16.2; p = 0.22). Pairwise Tukey-adjusted comparisons confirmed a sustained, significant downward trend in doctor-recommended use every year, beginning in 2021 (all p ≤ 0.01 for all subsequent years).
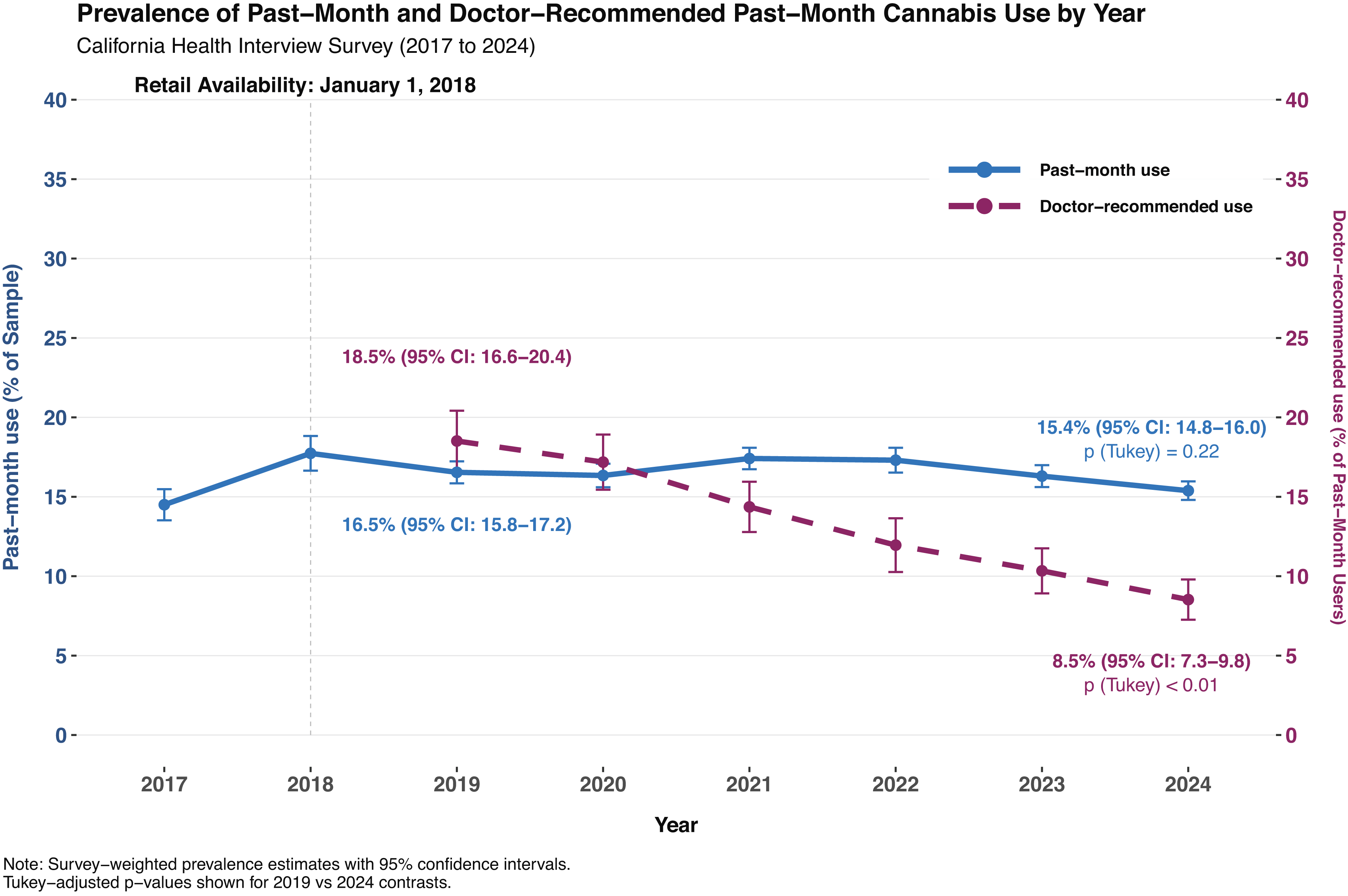
Weighted prevalence of past-month and doctor-recommended past-month cannabis use by year.
The overall decline in doctor-recommended cannabis use was consistent across sex and most age and racial/ethnic groups. However, the reduction was not statistically significant among young adults (18–25 years; –7.6%; 95% CI: –15.9–0.6; p = 0.09) nor among Asian (–2.9%; 95% CI: –8.0–2.3; p = 0.62) or African American respondents (–8.8%; 95% CI: –22.6–5.1; p = 0.47). See Supplementary Data.
Discussion
The prevalence of doctor-recommended cannabis use in California declined significantly between 2019 and 2024, while overall past-month cannabis use remained stable. This pattern indicates a shift in the number and proportion of individuals engaging in medical cannabis use under clinical guidance during the period following implementation of Proposition 64. These findings suggest that legalization and commercialization may have altered patterns of medical utilization without reducing population-level use.
This decline aligns with and extends findings from prior state- and national-level reports. Prevalence estimates reported from other population surveys, such as the International Cannabis Policy Study, 9 have generally been higher because they measure medical use more broadly, as doctor-recommended use represents only a subset of medically motivated cannabis use.
More importantly, multiple analyses of U.S. medical cannabis registries have demonstrated declining enrollment following recreational legalization. For example, a longitudinal, multistate review of medical cannabis registry data from 2009 to 2017 suggested that the total number of cardholders decreased in four states (Alaska, Colorado, Nevada, and Oregon) that had recently legalized recreational cannabis. 10 A similar study (2016–2020) reported reduced participation in five of seven states that implemented recreational programs. 6 A separate multistate analysis covering 2013–2020 found that recreational legalization was independently associated with a small decrease in medical cannabis cardholder enrollment across 23 states. 7 Together, these findings suggest that the observed reductions in doctor-recommended use in California are consistent with a broader national pattern of declining medical cannabis program participation during the period following recreational legalization.
Several factors may be relevant to the decline in doctor-recommended use. Proposition 64 preserved and extended incentives for formalized medical use, including exemptions from state use and local sales taxes and higher purchase limits than recreational use. At the same time, it eliminated the practical necessity of a medical recommendation for adults 21 and older. For some, obtaining a recommendation may have largely functioned as a workaround to the prohibition of recreational use. Moreover, although formalized medical use had previously conferred certain legal protections and legitimacy, these factors became less meaningful once recreational use was legalized. Collectively, these shifts may have reduced the perceived value of maintaining a formal medical designation.
The finding that doctor-recommended use among young adults did not significantly decline is notable in the context of the minimum age requirement (≥21 years) for recreational sales, which prohibits access for a subset of these individuals. Likewise, nonsignificant results for African American and Asian respondents may reflect limited statistical power and lower baseline prevalence, respectively.
The decline in doctor-recommended cannabis use raises important clinical and public-health considerations. Clinicians continue to face substantial gaps in evidence-based guidance on dosage, methods of administration, contraindications, adverse events, prescription drug interactions, and other important aspects of cannabis-oriented clinical care. 11 Calls for medical cannabis-specific educational training within health care programs remain unresolved. 12 In the context of these gaps, the observed decline in physician oversight raises the concern that individuals with complex medical conditions may obtain cannabis products through the adult-use market without adequate medical supervision.
This study has limitations. Doctor-recommended use does not capture the broader category of self-directed medical use. Therefore, declining prevalence of doctor-recommended does not necessarily reflect reduced medical use overall. Additional factors may also contribute to the observed decline, including the establishment of the state-governed Medical Marijuana Identification Card program, which requires an in-person appointment, annual fee, registration in a state database, and medical supervision documentation from a licensed physician (requiring a separate fee), which may deter participation. All measures were self-reported and subject to underreporting. The serial cross-sectional design precludes causal inference. A key strength is the use of CHIS, which employs rigorous statewide sampling to generate a representative sample across all 58 counties.
Conclusions
Doctor-recommended cannabis use in California has declined sharply between 2019 and 2024, a period following legalization and commercialization of recreational use by adults, while overall cannabis use remained stable. Together, these findings align with broader national trends of declining medical cannabis program participation during the post-legalization period.
As legalization/commercialization continues to expand, attention to improving clinical infrastructure for medical cannabis remains important. Expanding training for health care providers, lowering barriers to medical registry programs, and promoting routine clinical inquiry about cannabis use may help maintain appropriate oversight, especially for patients with complex conditions. Absent these measures, medically motivated users may increasingly rely on the recreational marketplace without clinician guidance.
Ethical Statement
The CHIS is a population-based survey conducted by the UCLA Center for Health Policy Research and approved by the University of California, Los Angeles Institutional Review Board. This study used publicly available, fully de-identified CHIS data and was determined to be exempt from human subjects review by the University of California, San Diego. All analyses were conducted in accordance with applicable ethical standards and the principles of the Declaration of Helsinki.
Informed Consent/Patient Consent Statement
Respondents in the CHIS provided informed consent at the time of data collection. The present study involved secondary analysis of publicly available, de-identified data; no direct respondent contact occurred, and no additional consent was required.
Footnotes
Author Disclosure Statement
Dr. Corroon is a compensated member of the Board of Directors of CV Sciences, Inc., a manufacturer of hemp-derived cannabidiol (CBD) products. CV Sciences, Inc. had no role in, and no knowledge of, any aspect of this study, including its design and conduct, data analysis, article preparation, or the decision to publish.
Funding Information
This study was supported by the Center for Medicinal Cannabis Research at the University of California, San Diego (State of California award no. 6440-520–3314).
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.