
Abstract
Background:
Medical cannabis (MC) has emerged as a potential therapy for Parkinson’s disease (PD), targeting motor and nonmotor symptoms (NMS), such as pain, sleep disturbance, and urinary dysfunction. Cannabinoid receptors in central and peripheral systems, including the bladder, provide a mechanistic basis for symptom modulation. This study evaluated the feasibility, safety, and preliminary clinical effects of MC on NMS in PD within a real-world, regulated framework.
Methods:
In this single-center, open-label, prospective cohort, 68 patients with PD initiating MC were assessed at baseline and at 3 months using validated scales: the Non-Motor Symptoms Scale (NMSS), King’s Parkinson’s Disease Pain Scale (KPPS), PD Sleep Scale-2 (PDSS-2), PD Quality-of-Life Questionnaire-8 (PDQ-8), and International Prostate Symptom Score (IPSS), along with 2-day urinary diaries. Participants used either cannabis oil extract or inflorescence products with varying THC/CBD (Δ9-tetrahydrocannabinol/cannabidiol) ratios. Adverse events and withdrawals were recorded. Cannabinoid composition was analyzed via ultra-high-performance liquid chromatography and correlated with clinical outcomes.
Results:
Fifty participants (mean age 65.6 ± 11.0 years; 68% male) completed follow-up. MC use was associated with improvements in NMSS total (Δ 14.5, p = 0.001), PDSS-2 (Δ 5.9, p < 0.001), KPPS (Δ 8.1, p = 0.004), PDQ-8 (Δ 1.5, p = 0.040), and the NMSS urinary domain (Δ 2.1, p = 0.050). Nighttime urinary frequency decreased (median Δ 0.5, p = 0.016), while daytime parameters were unchanged. No correlations were found between cannabinoid composition or THC/CBD enrichment type and clinical response. The dropout rate was 26.5%, mainly due to loss to follow-up.
Conclusions:
Short-term, self-titrated MC was feasible and appeared generally well tolerated in this open-label setting, suggesting potential benefits for pain, sleep, and nocturnal urinary frequency in PD. These exploratory findings warrant randomized controlled trials focused on these domains and incorporating standardized dosing, pharmacokinetic monitoring, and predefined cognitive safety assessments to determine efficacy, safety, and optimal dosing.
Introduction
Nonmotor symptoms (NMS), such as pain, sleep disturbances, fatigue, mood and cognitive changes, and autonomic dysfunction, are common and often disabling in Parkinson’s disease (PD). 1 Despite their prevalence and impact, NMS remain underrecognized and undertreated. 2 Pharmacologic treatments often offer limited benefit or cause adverse effects, while nonpharmacologic approaches such as cognitive behavioral therapy, exercise, or sleep hygiene are inconsistently applied. Consequently, many patients turn to complementary or alternative therapies to better manage their complex symptom burden.
Medical cannabis (MC) represents one such approach. Preliminary studies and patient surveys suggest that cannabis may alleviate certain NMS, including pain,3,4 insomnia, and anxiety, 5 and may even reduce motor symptoms such as tremor and rigidity in some individuals.3,6 However, existing data are inconsistent and constrained by small sample sizes, heterogeneous formulations, variable dosing regimens, and reliance on self-reported outcomes. Robust, controlled evidence supporting efficacy and safety in PD is still lacking. 7
Biological plausibility for these reported effects is supported by the role of the endocannabinoid system, which modulates pain perception, sleep regulation, 8 urinary function, 9 mood, and motor control, 10 domains frequently disrupted in PD. Cannabinoids such as Δ9-tetrahydrocannabinol (THC) and cannabidiol (CBD) interact with CB1 and CB2 receptors, influencing dopaminergic, serotonergic, and neuroinflammatory pathways that are implicated in PD pathophysiology.11,12 Beyond the central nervous system, cannabinoid receptors are also expressed in peripheral organs, such as the urinary tract, where their presence in the urothelium and detrusor muscle suggests a role in modulating bladder contractility and sensation. 13
Estimates of cannabis use among people with PD vary by study and country, with surveys reporting any past or current cannabis use in roughly 6–40% of patients, depending on definitions (medical vs. nonmedical), timing, and legal context.14–16 A national survey by the Parkinson’s Foundation found that approximately one-quarter of respondents had used cannabis in the previous 6 months, 15 often without formal medical guidance. 5 Given the rising real-world use of cannabis among individuals with PD, systematic evaluation of its therapeutic potential is warranted.
We conducted a prospective study to evaluate real-world MC use among patients with PD within a regulated framework. Specifically, we aimed to (1) assess feasibility and safety, (2) measure changes in validated nonmotor and urinary outcomes, and (3) analyze cannabinoid composition to explore associations with clinical effects. This approach provides a practical basis for determining the therapeutic role of MC in managing unmet nonmotor needs in PD.
Materials and Methods
This exploratory, single-center, open-label study evaluated the feasibility, safety, and preliminary clinical effects of MC on NMS in PD. Participants self-titrated cannabis over a period of 3–6 weeks (titration protocol provided in the Supplementary Data), reflecting real-world prescribing practices in regions where MC is legally accessible. The study protocol was approved by the local Institutional Review Board (approval number 7553-20). All patients provided written informed consent prior to commencing MC treatment. The trial was registered at ClinicalTrials.gov (NCT05106504). This report adhered to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines (Supplementary Table S1).
Eligibility criteria
Inclusion criteria were as follows: (1) a diagnosis of idiopathic PD according to the UK PD Society Brain Bank clinical diagnostic criteria, confirmed by a movement disorders specialist; (2) receipt of an MC license from the Israeli Ministry of Health (MOH) for PD-related symptoms or pain but had not yet initiated use; (3) disease severity within Hoehn and Yahr (HY) stages 1–4; (4) a stable regimen of antiparkinsonian medications for at least 30 days before enrollment; (5) age between 18 and 80 years. Exclusion criteria included were as follows: (1) MC use within 30 days before recruitment; (2) suspected or confirmed atypical parkinsonian disorders; (3) severe comorbidities likely to influence outcomes (chronic pain syndrome, spinal cord injury, any malignancy); and (4) cognitive impairment precluding the ability to provide informed consent or complete study questionnaires.
Procedures
Data collection
Baseline demographics (age, sex) and disease characteristics (HY, disease duration) were recorded. NMS, quality of life (QoL), and urinary functions were assessed at baseline and after 3 months of MC use. Validated questionnaires included the Non-Motor Symptoms Scale (NMSS), 17 King’s Parkinson’s Disease Pain Scale (KPPS), 18 PD Sleep Scale-2 (PDSS-2), 19 and PD Questionnaire-8 (PDQ-8). 20 Urinary functions were assessed using the International Prostate Symptom Score (IPSS) 21 and the NMSS urinary domain. 17 Patients also completed a 2-day urinary diary documenting daytime (07:00 am–09:59 pm) and nighttime (10:00 pm–06:59 am) frequency and voided volume using a volumeter provided by the study team. At follow-up, 3 mL of MC extract or 3 g of inflorescence were collected to analyze phytocannabinoid content and explore associations with clinical outcomes.
MC titration
Patients obtained MC from licensed pharmacies and were monitored through follow-up calls. They could choose either inflorescence or oil extract formulations and select among CBD-rich, THC-rich, or balanced products. A standardized self-titration protocol used in routine clinical practice was followed. Participants began with one drop or puff nightly, increasing by one every 3 days. Upon reaching four drops or puffs, they could add a morning dose for persistent daytime NMS (e.g., pain) and, if needed, a mid-day dose for residual symptoms. Patients were instructed to report any adverse effects.
Side effects documentation and study withdrawal
Patients were instructed to contact the research coordinator regarding any side effects leading to dose reduction, discontinuation, or difficulty titrating MC. The coordinator also initiated follow-up calls during the first 3 weeks of titration to monitor tolerability. Adverse events were documented when they affected treatment continuation or dosing. Study withdrawals were recorded along with the corresponding reasons.
Extraction analysis
Extract preparation. Inflorescences were frozen at −20°C using liquid nitrogen to preserve their chemical integrity. Frozen inflorescences were ground into a fine powder using a mortar and pestle. The ground material was then transferred into 15 mL tubes. Absolute ethanol was added to each inflorescence powder sample at a sample-to-ethanol ratio of 1:4 (solids:solvent ratio). The mixture was thoroughly agitated on a shaker for 30 min to ensure efficient extraction of cannabinoids and other phytochemicals. Following extraction, the mixture was filtered through a 0.2 μm polyvinyl difluoride syringe filter to remove any solid particulate matter. The filtrate was collected into new tubes. The solvent was then evaporated under a stream of nitrogen to obtain a concentrated dry extract. The extract was weighed and resuspended in absolute methanol to achieve the desired concentration. The resuspended extract was then filtered through a 0.45 μm syringe filter to ensure a clear solution devoid of any remaining particulates.
Chemical analysis
The cannabinoid composition analysis was performed using UltiMate 3000 ultra-high-performance liquid chromatography coupled with an ultraviolet-visible diode array detector system (Thermo Scientific, Bremen, Germany). Analysis was carried out using a HALO C18 Fused-Core column (2.7 μm, 150 × 2.1 mm), with a HALO guard column (2.7 μm, 5 × 2.1 mm), and a ternary A/B/C multistep gradient (solvent A: water with 0.1% acetic acid, solvent B: acetonitrile with 0.1% acetic acid, and solvent C: methanol) at a constant flow rate of 0.3 mL/min.22,23 For each patient, cannabinoid concentrations were measured in all cannabis products they used, including oil extracts and inflorescences. Thirteen patients used two products, although for one of these only a single product was available for analysis. To generate a single representative value per patient for each cannabinoid, we calculated the arithmetic mean of that cannabinoid’s concentration across all analyzed products for that patient. This approach ensures that each patient contributes one value per cannabinoid to subsequent analyses, regardless of the number of products they used. The cannabinoids included in the analysis were tetrahydrocannabinolic acid (THCA), Δ9-tetrahydrocannabinol (THC), cannabidiolic acid (CBDA), cannabidiol (CBD), cannabigerolic acid (CBGA), cannabigerol (CBG), cannabidivarinic acid (CBDVA), cannabidivarin (CBDV), tetrahydrocannabivarin (THCV), cannabinolic acid (CBNA), cannabinol (CBN), cannabichromenic acid (CBCA), cannabichromene (CBC), cannabicyclol (CBL), Δ8-tetrahydrocannabinol (D8-THC), cannabichromevarin (CBCV), and cannabicitran (CBTC). Total THC, CBD, and CBG were calculated using the formula: total = 0.877 × acid form + neutral form (i.e., total THC = 0.877× THCA + THC, total CBD = 0.877× CBDA + CBD, total CBG = 0.877× CBGA + CBG).
Statistical analysis
Baseline characteristics were summarized using descriptive statistics. Paired pre- and post-treatment differences were analyzed across all clinical outcomes. Normality was assessed using histograms, Q–Q plots, and the Shapiro–Wilk test. For normally distributed data, paired t-tests were applied; for nonnormal or ordinal data, Wilcoxon signed-rank tests were used. Continuous variables are reported as mean ± SD or SE, and categorical variables as counts and percentages. Urinary diary measures, including daytime and nighttime frequency, voided volume, and maximum voided volume, were compared pre- and postintervention using Wilcoxon signed-rank tests, given the small sample sizes for these measures. Analyses were conducted per protocol, including only participants who completed both timepoints. Missing data were not imputed; participants with incomplete paired data for a given outcome were excluded from that specific analysis. Results are expressed as mean differences with 95% confidence intervals (CI). Statistical significance was set at two-tailed p < 0.05.
Correlations between change scores of clinical outcomes (NMSS, KPPS, PDSS-2, PDQ-8, IPSS, and urinary measures) and cannabinoid concentrations were assessed using Pearson’s r with Benjamini–Hochberg false discovery rate (FDR) correction. Heatmaps visualized correlation strength and direction. Subgroup analyses compared outcomes across cannabis types (CBD-rich, THC-rich, THC + CBD-rich) using Kruskal–Wallis or Wilcoxon rank-sum tests, with FDR correction for multiple comparisons. Analyses were performed in R (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study population
Sixty-eight patients with PD were enrolled, of whom 50 patients completed follow-up and were included in the final analysis. The mean age at baseline was 66.8 ± 10.3 years, the mean disease duration was 5.7 ± 5.5 years, and 66.2% were male. The median HY stage was 2.0 (IQR: 1.0–2.0). The mean follow-up duration was 3.0 ± 1.5 months. Baseline demographic and clinical characteristics are presented in Table 1.
Baseline Characteristics of the Full Cohort and Analyzed Cohort
Values are presented as mean ± standard deviation, median (interquartile range), or n (%), as appropriate. The “full cohort” (n = 68) includes all patients initially enrolled, while the “analyzed cohort” (n = 50) represents those included in the per-protocol analysis.
p-Values compare the analyzed cohort (n = 50) to the full cohort (n = 68), excluding missing values. Continuous variables were compared using t-tests or Mann–Whitney U tests as appropriate; categorical variables were compared using chi-square or Fisher’s exact tests.
Medication data were retrievable for 61 of 68 participants in the full cohort and 44 of 50 in the analyzed cohort; 7 and 6 patients, respectively, had inaccessible records due to reliance on external HMO systems. Proportions are calculated over retrievable denominators.
HY, Hoehn and Yahr stage; NMSS, Non-Motor Symptoms Scale; PD, Parkinson’s disease; PDSS-2, Parkinson’s Disease Sleep Scale-2; KPPS, King’s Parkinson’s Disease Pain Scale; PDQ-8, Parkinson’s Disease Questionnaire 8; IPSS, International Prostate Symptom Score; LEDD, Levodopa Equivalent Daily Dose.
Study retention
Of the 68 participants initially enrolled, 18 (26.5%) did not complete the study or discontinued MC use. Eleven (16.2%) were lost to follow-up, two (2.9%) elected not to initiate MC after enrollment, two (2.9%) discontinued because of adverse effects (depression and dizziness), one (1.5%) discontinued after a single trial dose due to perceived lack of efficacy, one (1.5%) withdrew before initiating MC following a new diagnosis of prostate cancer, and one (1.5%) was unable to continue due to administrative or licensing issues. The remaining 50 participants completed both baseline and 3-month assessments and were included in the per-protocol analysis. Participant flow and reasons for study discontinuation are detailed in Supplementary Figure S1. As shown in Table 1, baseline demographic and clinical characteristics did not differ significantly between the full cohort and the analyzed cohort (all p > 0.25). Baseline concomitant medication classes, including urologically active agents, sleep agents, pain medications, and antidepressants, were retrievable for 61 of 68 participants in the full cohort and 44 of 50 in the analyzed cohort and are detailed in Supplementary Table S2; no significant differences were observed between cohorts for any medication class (all p > 0.34).
Change in NMS
Among the analyzed cohort (n = 50), self-titrated MC was associated with improvements across multiple clinical measures representing NMS (Fig. 1, Table 2). Mean scores improved for global NMS burden (NMSS total), pain (KPPS), sleep quality (PDSS-2), and QoL (PDQ-8). A borderline change was observed in the NMSS urinary domain, with no significant change in IPSS. Data completeness ranged from 82% to 98% across questionnaires.
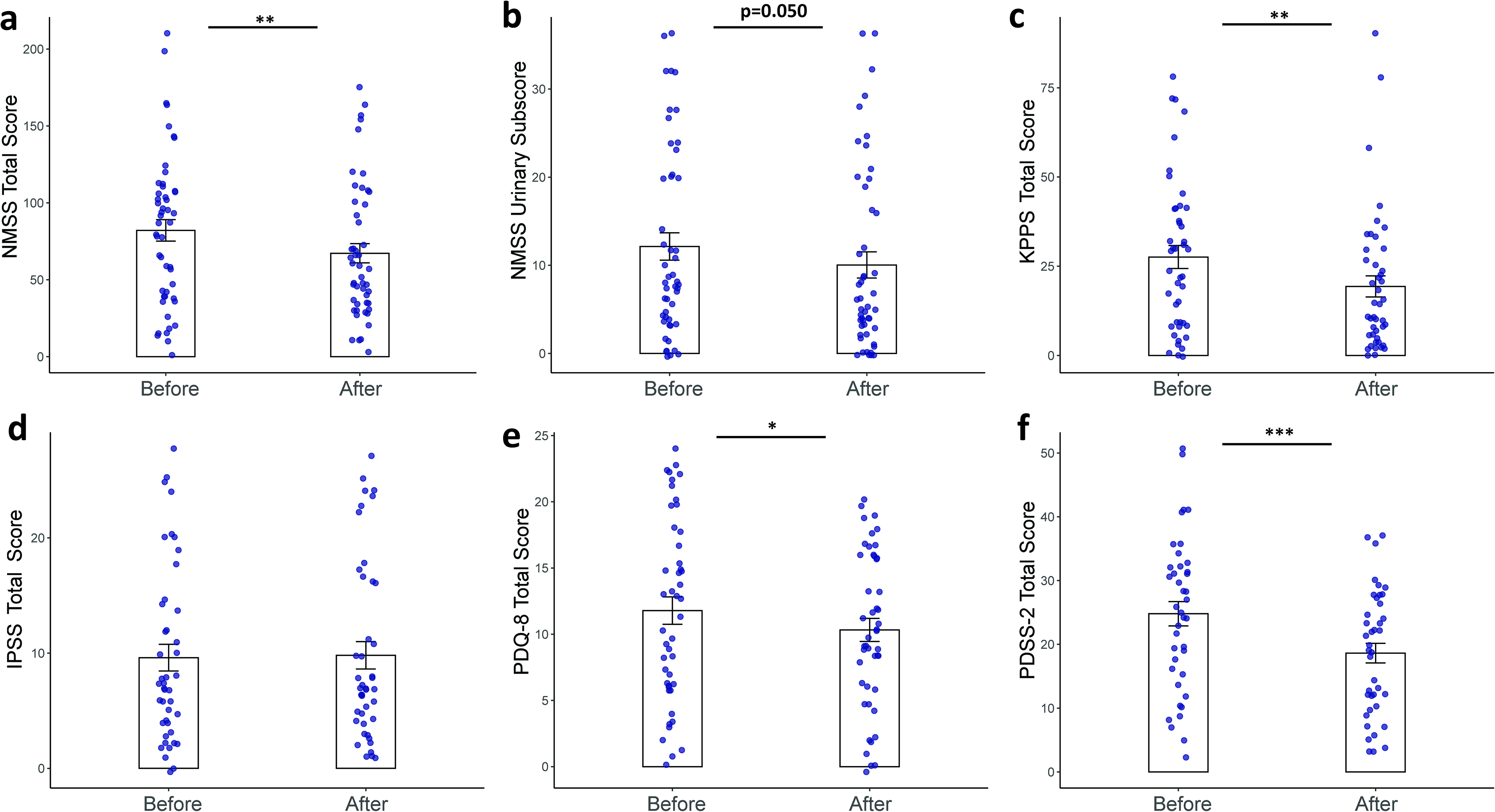
Changes in nonmotor symptom and quality-of-life measures before and after self-titrated medical cannabis in the analyzed cohort (n = 50). Panels show changes in
Changes in Clinical Outcome Measures Following Self-Titrated Medical Cannabis in the Analyzed Cohort (n = 50)
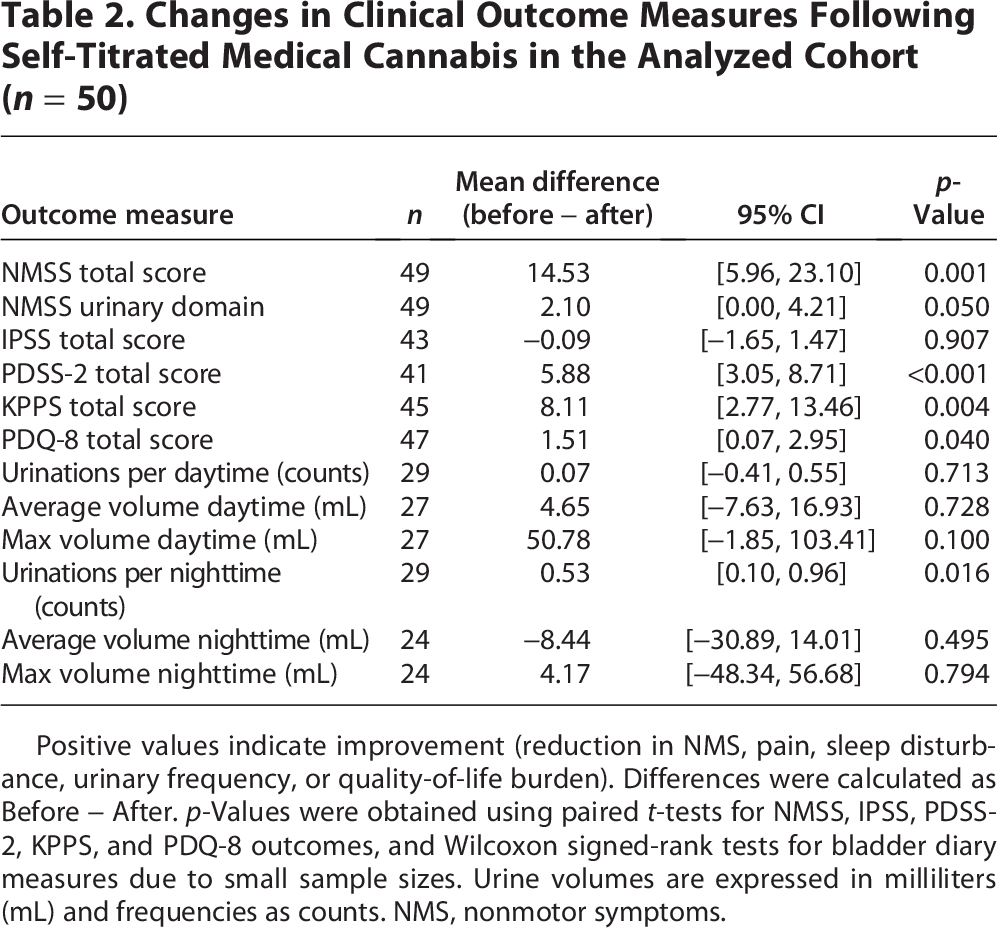
Positive values indicate improvement (reduction in NMS, pain, sleep disturbance, urinary frequency, or quality-of-life burden). Differences were calculated as Before − After. p-Values were obtained using paired t-tests for NMSS, IPSS, PDSS-2, KPPS, and PDQ-8 outcomes, and Wilcoxon signed-rank tests for bladder diary measures due to small sample sizes. Urine volumes are expressed in milliliters (mL) and frequencies as counts. NMS, nonmotor symptoms.
Bladder diaries
Analysis of 2-day urinary diaries showed a significant reduction in nighttime urinary frequency after 3 months of MC use (Fig. 2, Table 2). Daytime frequency and both daytime and nighttime urinary volumes did not change significantly. Diary data were available for approximately half of the participants, limited mainly by incomplete entries or missing volume recordings.
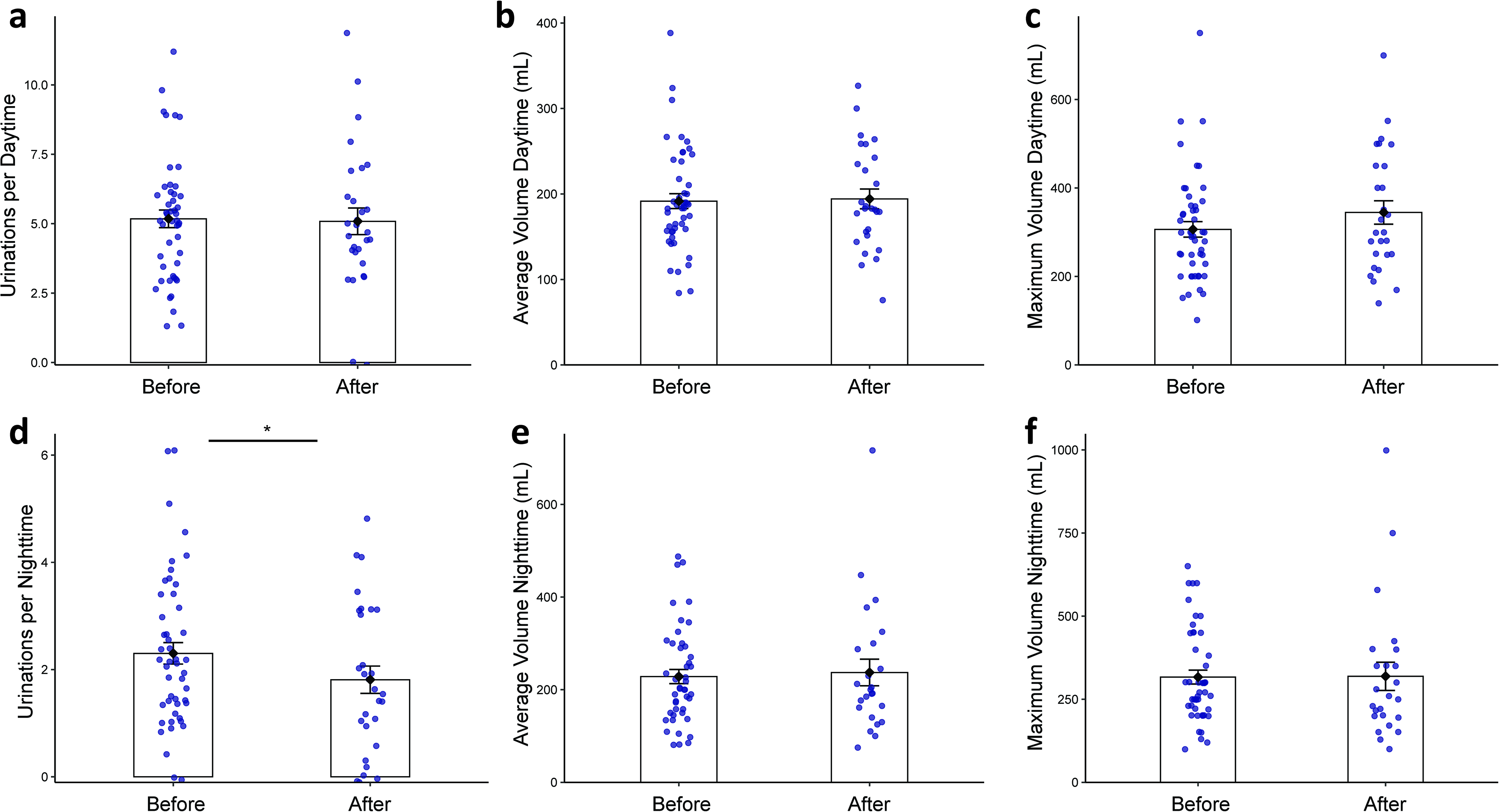
Changes in bladder diary measures before and after self-titrated MC in the analyzed cohort. Panels show
Cannabis extract composition and clinical outcomes
Samples of MC products were collected from 44 patients, totaling 56 products (50 oil extracts [89%] and 6 inflorescences [11%]); 13 patients (30%) used two different products, typically for nighttime use, although for one patient only a single product was available for analysis. The detailed cannabinoid composition of all products is provided in Supplementary Table S3. No significant correlations were observed between concentrations of individual cannabinoids and changes in clinical or urinary outcomes (NMSS, KPPS, PDSS-2, PDQ-8, IPSS, and diary-derived measures; Supplementary Figs. S2 and S3).
Patients were categorized into CBD-rich, THC-rich, and balanced THC/CBD subgroups for exploratory comparison (Fig. 3). In both three-group (Kruskal–Wallis) and two-group (Wilcoxon rank-sum) analyses, no outcomes reached statistical significance after false discovery rate (FDR) adjustment (Supplementary Table S4). Only nominal trends were observed for NMSS (p = 0.034, p_adj = 0.37) and maximum daytime voided volume (p = 0.079, p_adj = 0.65), indicating that the overall clinical response was not dependent on extract composition or enrichment type.
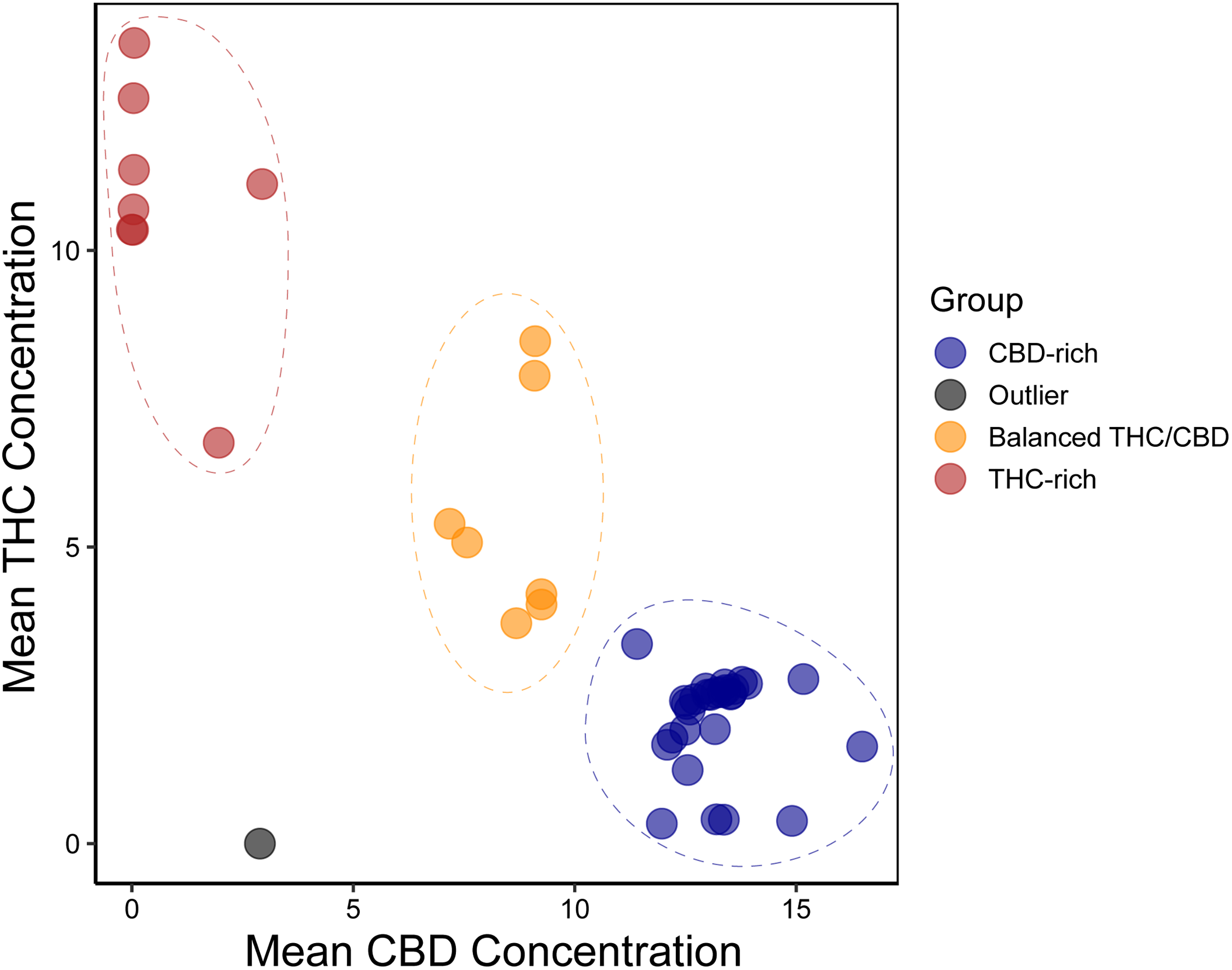
Distribution of mean THC and CBD concentrations by cannabinoid composition group. Each point represents an individual patient, plotted according to mean THC and mean CBD concentrations across the study period. Colors denote cannabinoid composition groups (CBD-rich, balanced THC/CBD, THC-rich), defined empirically based on relative cannabinoid exposure. Dashed ellipses illustrate the approximate distribution of each group. A single outlier with negligible cannabinoid exposure is shown in gray. CBD, cannabidiol; THC, Δ9-tetrahydrocannabinol.
Discussion
Clinical interpretation
In this exploratory prospective study, self-titrated MC use over 3 months was associated with improvements across multiple NMS domains in PD. Significant gains were observed in global NMS burden, pain, sleep quality, nocturnal urinary frequency, and QoL. Notably, the most specific and internally consistent signal emerged in nocturnal urinary frequency. The magnitude of improvement in NMSS (Δ14.5), PDSS-2 (Δ 5.9), and KPPS (Δ 8.1) scores met or exceeded published minimal clinically important differences (MCIDs) of approximately 13.91, 24 3.44, 25 and 3–9 points, 26 respectively, suggesting potentially meaningful benefits in global NMS, sleep, and pain.
These findings align with growing evidence that cannabinoids such as CBD and THC may modulate sleep architecture and pain processing in PD and other neurological disorders. 27 In an open-label study, Lotan et al. reported reductions in pain and sleep disturbance following cannabis use, alongside improvement in motor function. 6 Similarly, in a randomized, placebo-controlled trial, Peball et al. found that treatment with nabilone, a synthetic THC analogue, alleviated NMS, primarily through improvements in sleep-related disturbances and anxiety. 28 A meta-analysis by Urbi et al. further supported these effects across multiple studies. 29
In contrast, change in PDQ-8 (Δ1.5), although statistically significant, was below thresholds for clinical relevance (six points for PDQ-8 30 ), suggesting limited impact on QoL domain. These magnitudes are comparable to placebo responses observed in PD trials, emphasizing the need for cautious interpretation. Nonetheless, a modest but significant reduction in nocturia frequency was noted, aligning with evidence that endocannabinoid signaling may influence detrusor contractility and bladder sensory pathways.31–34 Cannabinoid receptor (CB1 and CB2) expression within the bladder and their activation have been shown to alter afferent signaling and detrusor tone. 35 Among patients with multiple sclerosis, a combination of THC–CBD has been reported to reduce bladder overactivity symptoms. 36 The lack of significant changes in daytime urinary measures may reflect both the predominantly evening use of MC and the limited completeness of urinary diaries (∼50%), which may have reduced analytic power. Given the predominantly evening use of MC, the nocturnal signal may reflect a time-linked cannabinoid effect on bladder sensory or detrusor pathways, although indirect effects through improved sleep continuity or pain reduction cannot be excluded. Future studies using objective voiding monitors or wearable sensors could clarify circadian dynamics and disentangle direct bladder effects from sleep-mediated improvements.
Cannabinoid composition and response
Despite substantial variability in THC/CBD ratios and absolute concentrations, no significant correlations emerged between individual cannabinoid levels and changes in clinical outcomes. However, because product formats (oil extract drops vs. inflorescence puffs) differ in concentration, delivery efficiency, and patient technique, dose normalization across individuals was not feasible. Analyses thus compared relative cannabinoid proportions rather than total cannabinoid exposure, which may have obscured potential dose–response relationships. Furthermore, product cannabinoid concentrations reflect nominal rather than systemic exposure, which varies substantially across individuals due to first-pass hepatic metabolism, route-dependent bioavailability, 37 and interindividual differences in cannabinoid receptor expression. 38 In a self-titration paradigm, dose adjustment to perceived effect may further compress the effective exposure range at the group level, paradoxically weakening any dose–response signal. In addition, minor cannabinoids and terpenes, which were not individually modeled, may modulate the activity of THC and CBD and contribute independently to clinical response. 39 The predominance of oil extract formulations (89%) further reflects patient preference for noninhaled routes, consistent with evolving prescribing trends and safety priorities in PD.
MC treatment adherence
Approximately one-quarter of participants discontinued the study or cannabis use. Reasons included loss to follow-up, personal decision, lack of efficacy, adverse effects, and administrative factors. These factors represent potential challenges in patient adherence and engagement in MC studies and real-life treatment.
Safety and feasibility
MC appeared generally well-tolerated within the limits of this open-label, self-reported design. Adverse effects were infrequent and mild, primarily transient dizziness or mood changes, and few patients discontinued therapy for tolerability reasons. The self-titration protocol, standardized in Israeli clinical practice, proved feasible and supported individualized dosing within a structured framework. The results suggest that MC can be safely used in PD when supported by patient education and careful clinical monitoring, in line with our prior publication. 40 Future trials should incorporate systematic adverse event reporting and cognitive assessments to ensure long-term neuropsychiatric safety, particularly in older adults with PD.
Limitations
Several limitations merit consideration. The open-label, single-center design without a control group introduces potential expectancy and observer bias. This caveat applies to all reported outcomes, including those meeting MCID thresholds, as placebo responses for subjective domains such as pain, sleep, and QoL can be substantial in open-label PD trials. The sample size was modest, and the 3-month follow-up limits inference regarding the durability of benefit or late-onset effects. Missing urinary diary data (∼50%, potential selection bias) and the absence of quantitative dosing information further restrict interpretation, as the total cannabinoid exposure could not be standardized across patients. In addition, the stability of non-antiparkinsonian medications was not formally required or verified, and we cannot exclude that changes in concomitant urologically or sleep-active agents contributed to improvements in individual patients. No cognitive or psychomotor testing was included, leaving the cognitive safety and potential neurobehavioral effects of MC unaddressed. Despite these limitations, the study’s strengths include its prospective design, use of validated patient-centered measures, and laboratory-confirmed cannabinoid profiling, providing one of the most comprehensive real-world characterizations of MC use in PD to date.
Conclusions
This prospective exploratory study provides real-world evidence that self-titrated MC may alleviate select NMS in PD, particularly pain, sleep disturbances, and nocturnal urinary frequency. While the observed improvements were modest and partly within the expected placebo range, they nonetheless identify domains where cannabinoid-based interventions may hold therapeutic promise. These hypothesis-generating findings support the rationale for conducting randomized, placebo-controlled trials specifically targeting sleep quality, pain modulation, and nocturnal urinary symptoms in PD. Future studies should include standardized dosing protocols, pharmacokinetic monitoring, and longer follow-up to define dose–response relationships and durability of benefit. In addition, systematic assessment of cognitive function, an important but unmeasured outcome in this study, will be critical to establish both therapeutic potential and neurocognitive safety of MC in this population.
Ethical Compliance Statement
The study protocol was approved by the Institutional Review Board of Sheba Medical Center (approval number 7553-20). Written informed consent was obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki. The authors confirm that they have read the journal’s position on issues of ethical publication and affirm that this work is consistent with those guidelines. ClinicalTrials.gov Identifier: NCT05106504.
Authors’ Contributions
O.A.: Conceptualization, methodology, data curation, formal analysis, writing—original draft, and visualization. S.L.: Investigation, data collection, and writing—review and editing. T.G.: Investigation, data collection, and writing—review and editing. A.S.: Project administration, study coordination, data collection, and writing—review and editing. D.M.: Methodology, formal analysis (cannabinoid profiling), validation, and writing—review and editing. A.S.: Formal analysis (cannabinoid profiling), validation, and writing—review and editing. T.F.-K.: Investigation, patient recruitment, and writing—review and editing. L.E.: Investigation, patient recruitment, and writing—review and editing. S.H.-B.: Supervision, resources, and writing—review and editing. S.A.: Conceptualization, methodology, formal analysis, data curation, writing—original draft, writing—review and editing, and supervision.
Footnotes
Consent to Participate
Written informed consent was obtained from all participants prior to study participation.
Data Availability Statement
Deidentified participant-level data that support the findings of this study contain potentially identifiable clinical information and, therefore, are not publicly available. Data may be made available from the corresponding author upon reasonable request and with approval from the relevant institutional review board and data governance bodies and execution of an appropriate data use agreement.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
No specific funding was received for this work.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.