
Abstract
Objective:
To evaluate the effects of beyond cold light whitening and desensitization on shear bond strength of orthodontic metal brackets.
Materials and Methods:
Ninety-eight extracted human premolars were randomly divided into seven groups (n = 14). Group 1 was the control (no treatment). Group 2 underwent bleaching, followed by bonding after 24 h. Group 3 received desensitization, then bonding after 24 h. Group 4 combined bleaching and desensitization, with bonding after 24 h. Groups 5, 6, and 7 followed the same procedure as Group 4, but bonding occurred 1, 2, and 3 weeks later, respectively. All samples were stored in 37°C artificial saliva after treatment and bonded with 3 M light-cure composite resin using halogen light. Shear bond strength was tested with a universal testing machine (INSTRON 5848). Adhesive remnant index (ARI) scores were assessed post-debonding. Statistical analysis was conducted using Analysis of Variance (ANOVA), Tukey’s test, and chi-square tests, with significance set at p < 0.05.
Result:
The shear bond strength 24 h after bleaching (7.5 ± 1.77 MPa) was significantly lower than the control (12.24 ± 3.71 MPa, p < 0.05). Desensitization alone (11.68 ± 3.49 MPa) showed no significant difference compared with the control (p > 0.05). Shear bond strength significantly decreased 24 h after bleaching and desensitization (p < 0.05) but recovered to control levels after 1 week (p > 0.05). ARI scores showed no significant differences.
Conclusions:
(1) Brackets bonded 24 h after bleaching or combined treatment showed reduced shear bond strength but were clinically acceptable; (2) The use of nano-biomaterial desensitizers slightly reduces the shear strength of brackets, but it will repair the damage of teeth caused by bleaching; (3) The impacts of bleaching and desensitization gradually reduce and return to normal levels after 1 week.
Introduction
Everyone has an innate desire for beauty. As society evolves and economic standards rise, an increasing number of individuals are becoming more conscious of their appearance, with the neatness and beauty of their teeth being vital components of a perfect image. Consequently, cosmetic dentistry has emerged as a significant field within oral medicine in recent years. The primary goal of cosmetic dentistry is to provide patients with white, well-aligned teeth and a confident smile. This not only enhances individuals’ self-assurance in daily life and social interactions but also fosters greater interest in oral hygiene. It is widely acknowledged that tooth whitening is both the foundation and a gateway to aesthetic dentistry.
The causes of tooth discoloration can be divided into three main categories: intrinsic discoloration, extrinsic discoloration, and age-related discoloration. Tooth bleaching has increasingly gained acceptance among practitioners and patients as a conservative, safe, economical, and effective method for changing tooth color. 1 Currently, the most commonly employed bleaching methods in clinical practice include at-home bleaching and in-office bleaching. The bleaching products available vary in terms of active ingredients, concentrations, application frequency, product forms, application modes, and light activation.2,3 For instance, the active ingredients can consist of hydrogen peroxide, urea peroxide, and sodium perborate, 4 with each bleaching agent offered in several different concentrations.
Although bleaching can significantly enhance the color of teeth, numerous studies have reported potential side effects, including alterations in surface morphology, changes in chemical composition, and reduced bonding strength.5–7 Orthodontists are particularly concerned about the effects of bleaching on the bonding strength of orthodontic brackets. Several researchers have conducted extensive experiments to investigate this issue, presenting varying viewpoints. Prietsch et al. 8 found that bonding brackets 24 h after bleaching resulted in a significant reduction in bonding strength, suggesting that bracket bonding should be postponed for 1 week after bleaching. Conversely, Miles et al. 9 argued that bonding brackets 1 week post-bleaching also leads to decreased bonding strength, recommending a 2-week delay. However, some scholars have concluded through extensive experimentation that there is no change in the bonding strength of brackets after bleaching, indicating that bonding time is not restricted.10–12 Thus, the timing of bracket bonding after bleaching has become a prominent topic in recent years. This article aims to investigate the bonding strength of brackets bonded 24 h after bleaching.
One of the primary adverse reactions associated with tooth bleaching treatments, both during and after the procedure, is tooth sensitivity. Consequently, desensitization, particularly following intensive bleaching, has become a critical step in the process. Various desensitizers are currently employed in clinical practice, each with distinct mechanisms of action. To my knowledge, numerous studies have investigated the effects of desensitizers on bracket bonding strength.5,13–15 In recent years, several oral nano-biological materials have emerged on the market, including a new type of biogenic nano-material specifically designed for desensitization. This biogenic nano-material provides multiple benefits, such as desensitization, caries prevention, maintenance of gum and periodontal health, and remineralization, and is now available for clinical application. However, research on its impact on the bonding strength of orthodontic brackets remains lacking.
Thus, the aim of this study is to investigate the effects of bleaching, desensitization, and their combination on the bonding strength of orthodontic brackets.
Experimental Materials and Methods
Experimental materials
A total of 98 maxillary premolars extracted for orthodontic purposes were used in this study. The teeth were treated using the Beyond Cold Light Tooth Whitening System and whitening agents (Beyond Technologies, USA). Bio-nanomaterial desensitizer (Beijing Daqing Biotechnology Co., Ltd.) was applied to reduce sensitivity. The bonding of 3 M Mini Thin Orthodontic Metal Brackets (Maotai Medical Equipment Co., Ltd., USA) was performed using Transbond XT Light-Cured Orthodontic Adhesive (3M Unitek, USA), following surface preparation with 37% phosphoric acid (BISCO, USA).
A Constant Temperature Water Bath (SUB Aqua Plus series, UK) was used. Mechanical testing was conducted using an INSTRON 5848 Micro Fatigue Testing Machine (INSTRON, USA), while surface characterization was performed with a LEXT Olympus Laser Scanning Microscope (OLS, Japan). Artificial saliva, prepared according to a specific formula, was used in the experiment, containing 10 g of sodium carboxymethyl cellulose, 30 g of sorbitol, 1.2 g of potassium chloride, 0.9 g of sodium chloride, 0.05 g of magnesium chloride, 200 mL of 0.053% calcium phosphate, 10 mL of 0.2% sodium phosphate, 0.33 g of paraben, and 1000 mL of distilled water.
Experimental methods
Tooth selection criteria
The teeth are normally developed, free from tetracycline staining and dental fluorosis, with intact enamel, no surface cracks, and no caries. They have not been treated with chemical agents such as alcohol, formaldehyde, hydrogen peroxide, or other bleaching agents, nor have they undergone dental pulp treatment. Following the extraction of premolars for orthodontic purposes, periodontal instruments are employed to remove any residual periodontal tissue and calculus from the teeth, which are then stored in 37 degree artificial saliva.
Experimental groups
Ninety-eight maxillary premolars meeting the standards were randomly divided into seven groups, with 14 teeth in each group. Group G1 served as the control group, with no treatment applied to the teeth, and brackets were bonded directly during the experiment. Group G2 underwent cold light bleaching and were stored in 37 degree artificial saliva for 24 h before bracket bonding. Group G3 received desensitizer application and were stored in 37 degree artificial saliva for 24 h prior to bonding. Group G4 underwent cold light bleaching, followed by desensitizer application, and were then stored in 37 degree artificial saliva for 24 h before bonding. Group G5 followed the same treatment as Group G4 but were stored in 37 degree artificial saliva for 1 week before bonding. Group G6 underwent the same procedure as Group G4 but were stored in 37 degree artificial saliva for 2 weeks prior to bonding. Group G7 followed the same steps as Group G4 but were stored in 37 degree artificial saliva for 3 weeks before bonding.
Bleaching and desensitization
All buccal surfaces of the teeth were polished using a polishing paste and rubber cups for 10 sec, rinsed thoroughly with running water, and dried with oil-free compressed air. The teeth were divided into seven groups for different treatments and conditions. Group G1 served as the control group, with no treatment applied. The teeth were stored in artificial saliva at 37°C, and brackets were bonded after 24 h. Group G2 underwent tooth bleaching according to the instructions for the Beyond cold light whitening product. A uniform 1 to 2 mm layer of 35% hydrogen peroxide whitening gel was applied to the buccal enamel surfaces, illuminated for 12 min using the whitening device positioned perpendicular to and close to the tooth surface. This procedure was repeated three times, for a total illumination time of 36 min. The whitening gel was removed with strong suction, wiped with a sterile dry cotton ball, and rinsed thoroughly. The treated teeth were stored in artificial saliva at 37°C, and brackets were bonded after 24 h. Group G3 underwent desensitization with the bio-nanomaterial desensitizer, prepared by mixing 0.1 g of powder with 30 µL of saline and stirring until fully combined. The mixture was applied to the buccal surfaces until evenly distributed, left for 2 min, and excess powder was rinsed off with clean water. The teeth were then stored in artificial saliva at 37°C, and brackets were bonded after 24 h. Group G4 underwent bleaching as in Group G2, followed by desensitization as in Group G3. The teeth were stored in artificial saliva at 37°C, and brackets were bonded after 24 h. Group G5, Group G6, and Group G7 followed the same bleaching, desensitization, and storage methods as Group G4, but brackets were bonded after 1, 2, and 3 weeks, respectively.
Bracket bonding
Twelve samples from each group were selected for bracket bonding using Transbond XT light-cured orthodontic adhesive, in accordance with the manufacturer’s instructions.
The tooth surfaces were dried with a sterile cotton ball and then treated with 37% phosphoric acid for 30 sec. After rinsing the surfaces with water from a three-way syringe for 30 sec, they were dried again until a chalky white appearance was achieved. If no chalky white appearance was observed, the tooth surface was re-etched. A thin layer of Transbond XT primer was applied to the treated surface using a soft-bristled brush, and a small amount of adhesive was placed on the base of the bracket. The bracket was then positioned on the buccal surface of the tooth and carefully adjusted to ensure that its long axis aligned with that of the tooth. Excess adhesive around the bracket was removed using the tip of a sharp instrument, and finally, the curing light was applied to the mesial and distal sides of the bracket for 20 sec each.
All procedures during the bracket bonding process were performed by the same skilled operator. The samples with bonded brackets were then stored in artificial saliva and maintained in a constant temperature water bath for 24 h.
Shear bond strength testing of brackets
The roots of all bonded brackets were embedded in a circular ultra-hard gypsum base, ensuring that the bonding surfaces of the brackets and the enamel were perpendicular to the base. The shear bond strength (SBS) of the brackets was tested using the INSTRON 5848 micro fatigue testing machine. A shear blade was attached to the moving arm of the testing machine, while the sample was positioned on another moving arm. The cutting edge of the shear blade was aligned in the bracket slot, parallel to the base of the bracket and perpendicular to the slot. During the shear force test, the shear blade was applied at a constant rate of 1 mm/min until the bracket detached. The force generated during detachment was recorded by a computer connected to the testing machine (as shown in Fig. 1), measured in newtons. The formula for calculating SBS is the shear force value divided by the area of the bracket base, expressed in MPa.
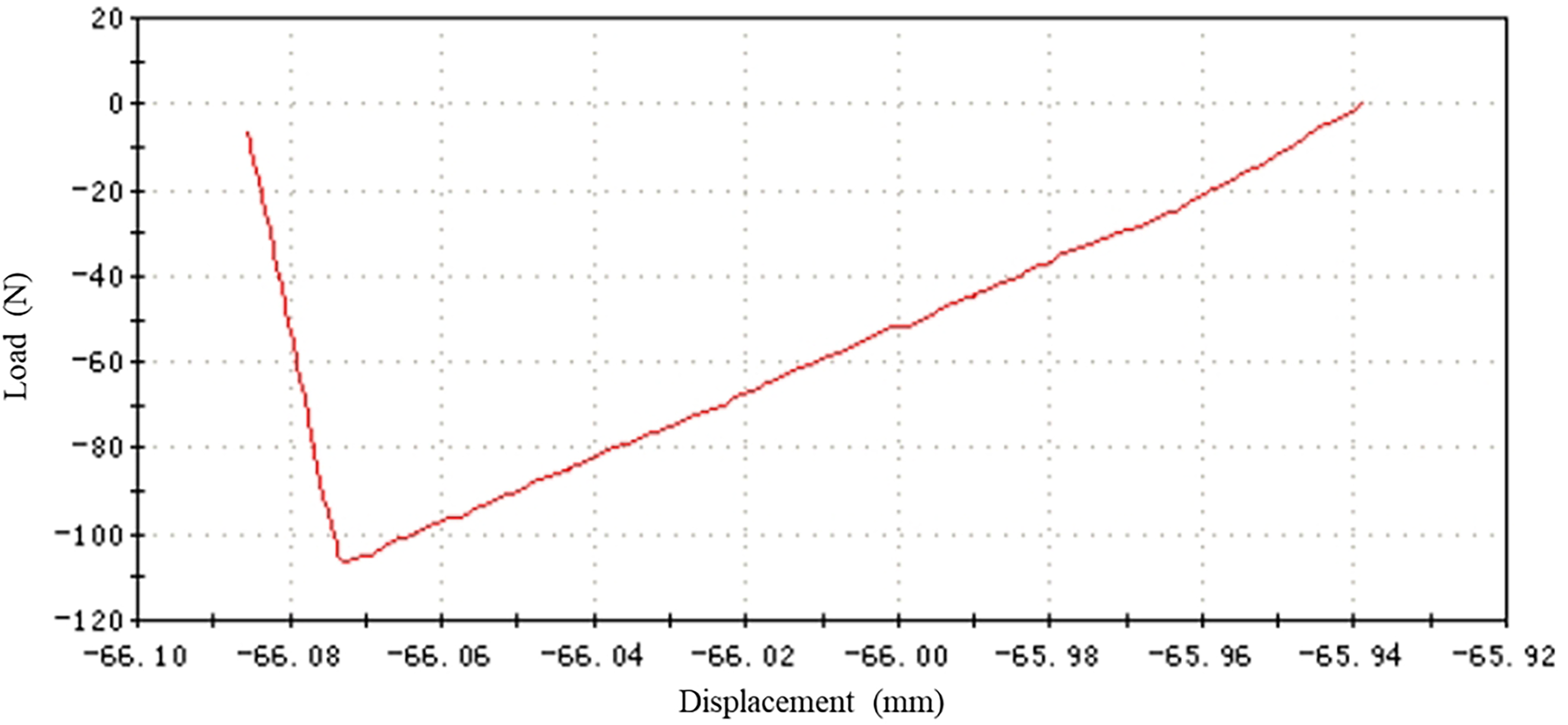
Bracket shear force curve diagram.
Statistical analysis of the adhesive remnant index
The buccal surfaces of the teeth and the bases of the brackets were examined using a 10× magnifying glass to assess the residual adhesive on all samples. Each sample was scored according to the adhesive remnant index (ARI) scoring criteria.
The ARI scoring criteria are as follows: 5 points indicate no residual adhesive on the enamel; 4 points represent less than 10% residual adhesive on the enamel; 3 points indicate more than 10% but less than 90% residual adhesive on the enamel; 2 points represent more than 90% residual adhesive on the enamel; and 1 point indicates that the adhesive completely remains on the enamel.
The ARI scoring system provides a comprehensive evaluation of the location of adhesive failure during bracket detachment.
Laser scanning microscope observation of enamel surface structure
Following bleaching, desensitization, and the combined treatment of bleaching and desensitization, two samples were randomly selected from each group. One of the samples was etched with 37% phosphoric acid for 30 sec, then rinsed with running water for 30 sec and dried using oil-free compressed air until a chalky white appearance was observed. All samples were separated at the enamel-cementum junction, and the crowns were sectioned in the mesio-distal direction, with the buccal portion of each crown chosen for scanning. Each sample underwent a gradient dehydration process with 75%, 95%, and 100% ethanol, with each concentration applied for 30 min, followed by natural air drying. The samples were fixed with clay, and the laser scanning microscope was employed to examine the flatter areas of the enamel surface, capturing one image at 2000× magnification for each sample.
Statistical analysis
All data were statistically analyzed using SPSS 19.0 software. SBS values were analyzed using one-way ANOVA and independent samples T-tests, while ARI values were assessed using the chi-squared test. A significance level of p < 0.05 was considered statistically significant.
Results
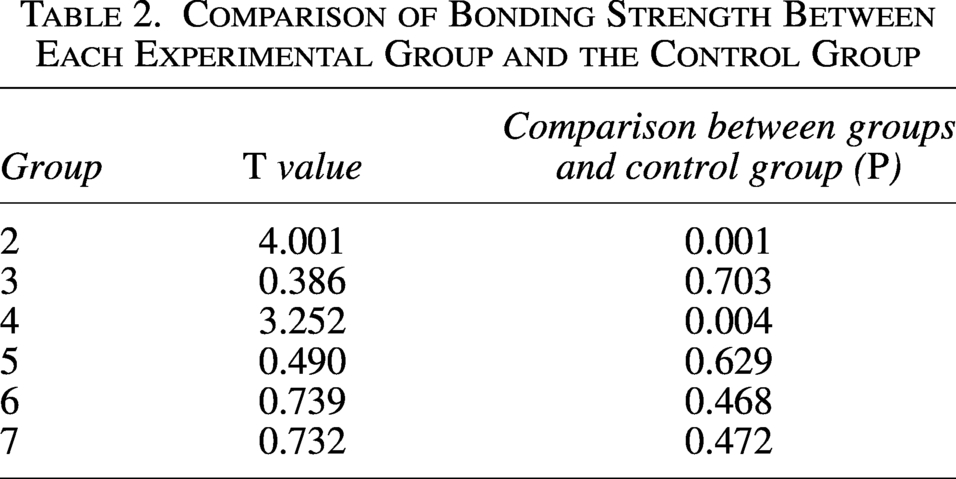
The statistical descriptions of SBS for each group are presented in Table 1. One-way ANOVA indicated significant differences among the seven groups (p < 0.01). Pairwise comparisons between each experimental group and the control group were performed using independent samples T-tests, with results displayed in Table 2. The SBS of brackets bonded 24 h after bleaching (7.50 ± 1.77 MPa) was significantly lower than that of the control group (12.24 ± 3.71 MPa; p < 0.05). For brackets bonded 24 h after desensitization, the SBS (11.68 ± 3.49 MPa) showed a slight decrease compared with the control group, but this difference was not statistically significant (p > 0.05). Brackets bonded 24 h after combined bleaching and desensitization exhibited a SBS of 8.29 ± 2.01 MPa, which was significantly lower than that of the control group (p < 0.05). However, the SBS of brackets bonded 1 week after combined bleaching and desensitization (12.95 ± 3.35 MPa) demonstrated a slight increase compared with the control group, with no statistically significant difference (p > 0.05). The SBSs of brackets bonded 2 weeks (11.24 ± 2.92 MPa) and 3 weeks (11.27 ± 2.73 MPa) after combined bleaching and desensitization gradually recovered, approaching those of the control group, with both showing no statistical differences compared with the control group (p > 0.05).
Statistical Descriptions of Shear Bond Strength (MPa) and Results of One-Way ANOVA for Each Group
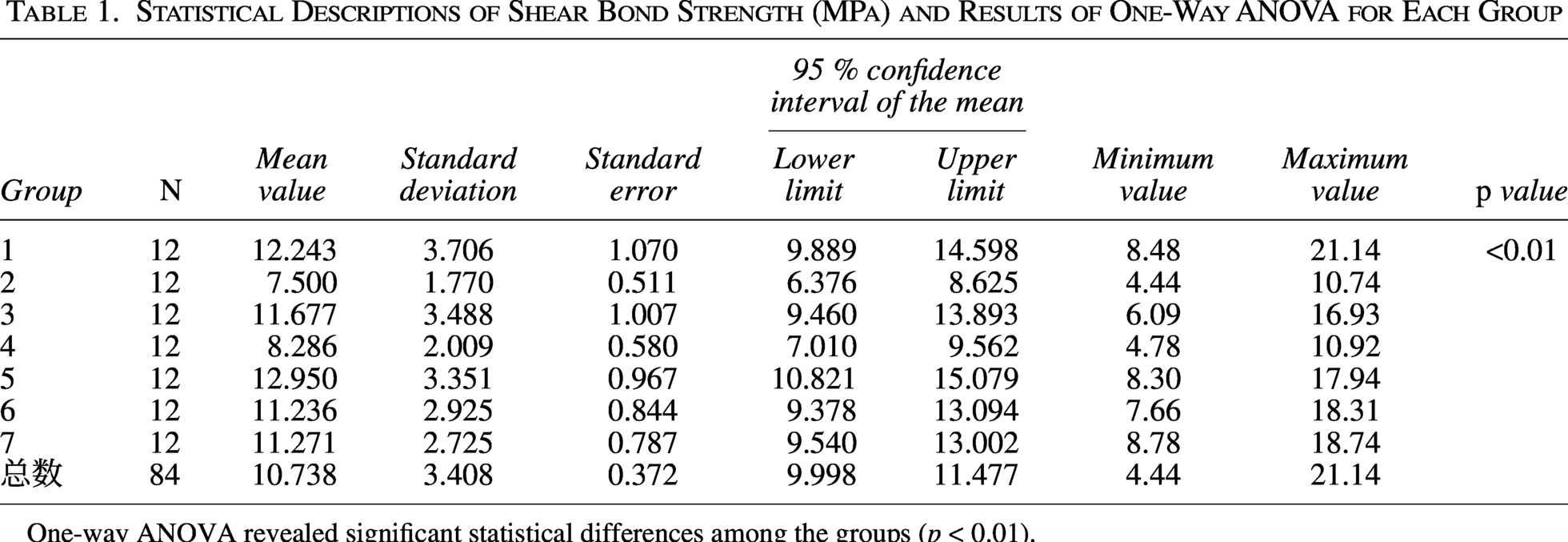
One-way ANOVA revealed significant statistical differences among the groups (p < 0.01).
Comparison of Bonding Strength Between Each Experimental Group and the Control Group
The ARI values for all samples were evaluated, with the scoring results presented in Table 3. Chi-squared analysis indicated no significant differences among the seven groups (p > 0.05). The bar chart in Figure 2 clearly illustrates that scores of 3, 4, and 5 were more frequent across the groups.

ARI distribution bar chart.
Scoring Table for ARI Values and Results of the Chi-Squared Test
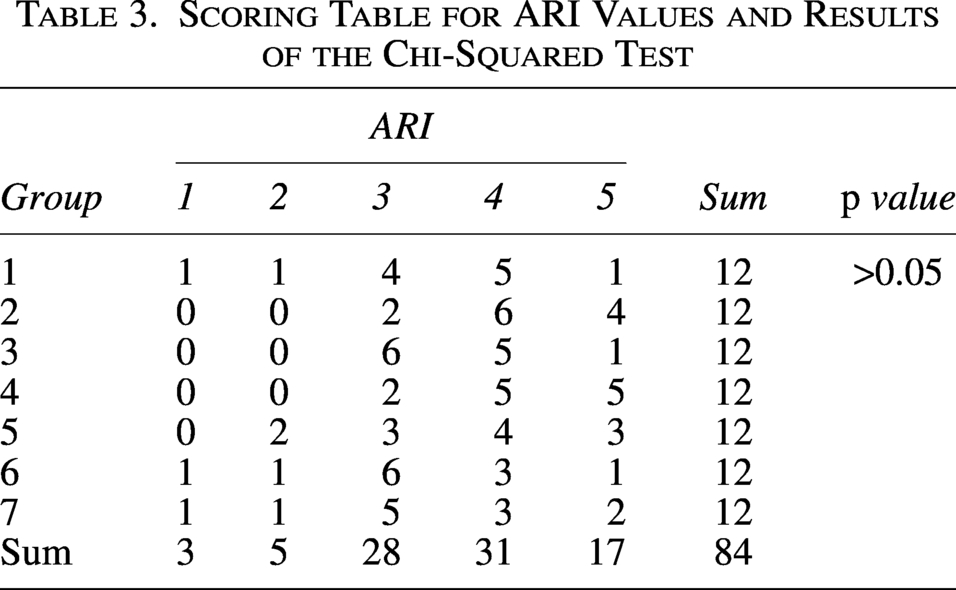
The chi-squared test revealed no significant differences among the groups (p > 0.05).
The laser scanning microscope at 2000× magnification revealed that the enamel surface in the control group was uniformly smooth and even, exhibiting scattered pits and a few scratches (as shown in Figs. 3A and Figs. 4A). After etching with phosphoric acid for 30 sec, the enamel surface demonstrated demineralization of inorganic material, resulting in a typical fish-scale appearance (as shown in Figs. 3H and 4H). Following 24 h of bleaching with 35% hydrogen peroxide, signs of demineralization emerged on the enamel surface, characterized by the loss of normal structure and the development of numerous micropores (as shown in Figs. 3B and 4B). After the nano-bioactive desensitizer, the enamel surface appeared uneven and gully-like, resembling a layer of mineralized material covering it (as shown in Figs. 3C and 4C). Laser scanning microscopy of the combined bleaching and desensitization group indicated a significant reduction in micropores on the enamel surface compared with the bleaching-only group, and it lacked the gully-like appearance observed in the desensitization-only group (as shown in Figs. 3D and 4D). Over time, the enamel surface gradually restored, approaching a normal smooth and even appearance (as shown in Figs. 3E, 4E, 3F, 4F, 3G, and 4G). All experimental groups exhibited disrupted normal enamel structure after etching with 37% phosphoric acid, with irregular demineralization evident around the enamel rods. Some regions displayed dense porosity, while others appeared rough and weathered, with some even showing signs of flaking (as shown in Figs. 3I, 4I, 3J, 4J, 3K, 4K, 3L, 4L, 3M, 4M, 3N, and 4N).
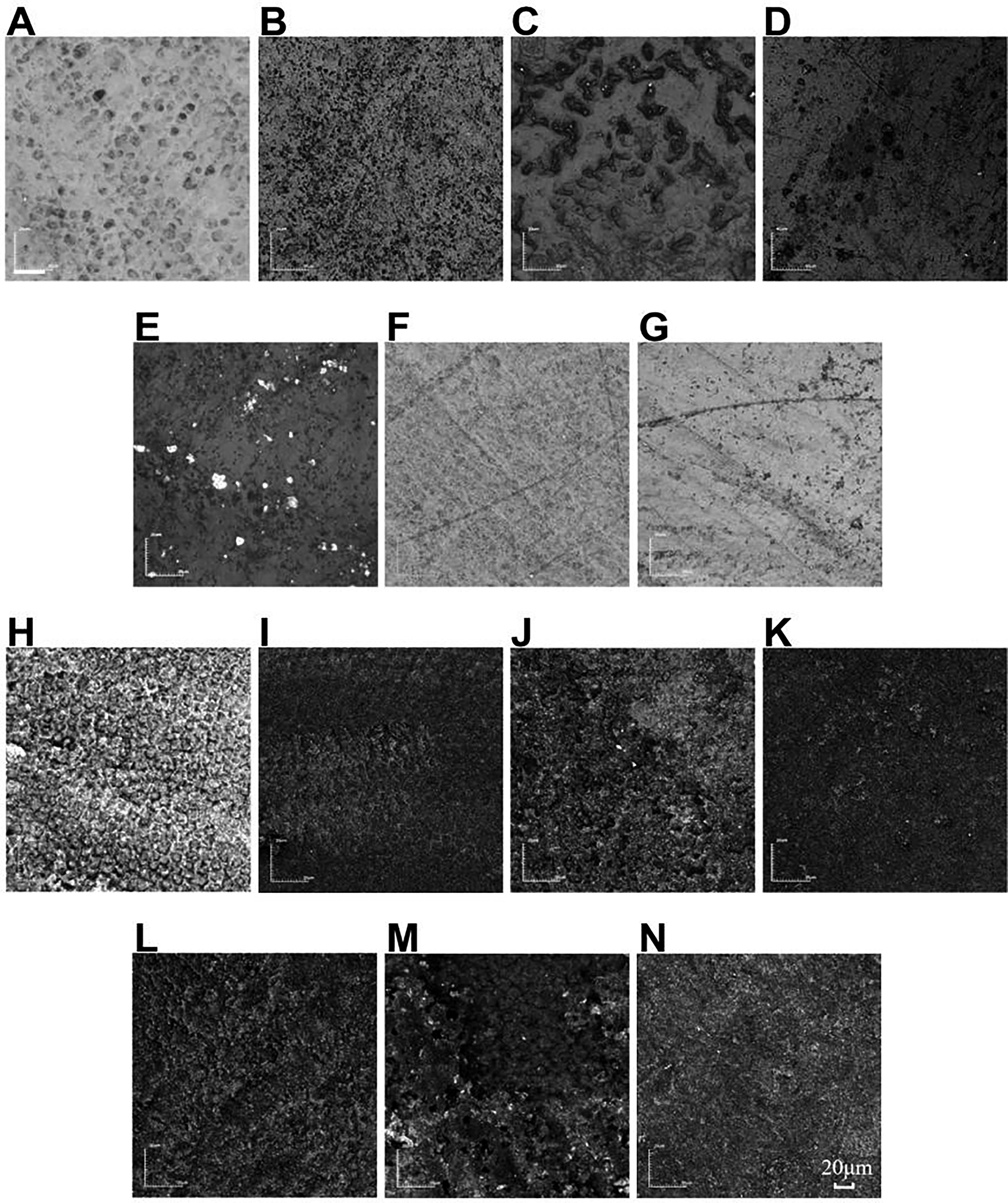
The gray image of enamel structure under laser confocal microscopy was magnified by 2000 times.
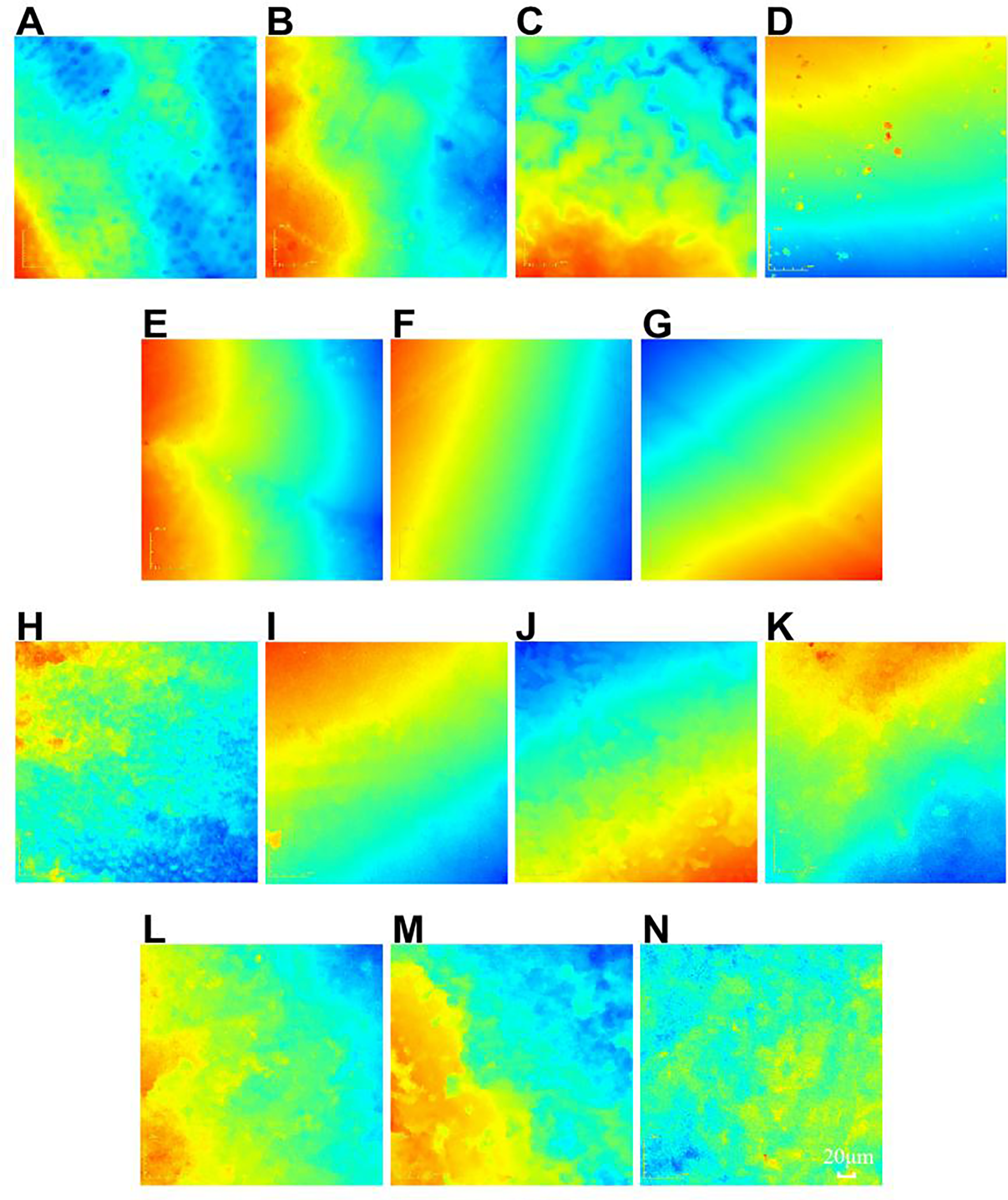
The color image of enamel structure under laser confocal microscope was magnified by 2000 times.
Discussion
The impact of bleaching on bond strength of orthodontic brackets
As the number of adult orthodontic patients continues to rise, orthodontists increasingly encounter individuals who are dissatisfied not only with the alignment of their teeth but also seek teeth whitening. Teeth bleaching is widely utilized in clinical practice due to its numerous advantages; however, its drawbacks remain a subject of debate. The mechanisms underlying teeth whitening are not fully understood, but the prevailing theory suggests that peroxides can penetrate hard tissues, generating reactive oxygen radicals that break double bonds and oxidize organic pigments, particularly reducing the coloration in dentin. 16 While the effectiveness of this treatment is well-established, concerns persist regarding its negative impacts on enamel.
The effects of bleaching on the bond strength of orthodontic brackets have become a significant area of research in recent years. Numerous scholars, both nationally and internationally, have conducted extensive experiments on this topic. Bishara et al. 10 proposed that bleaching agents with varying compositions and concentrations do not influence bracket bond strength. Similarly, Homewood et al. 11 and Uysal et al. 12 concluded in their studies that there is no change in bond strength. In contrast, some researchers15,17–19 argue that using 35% hydrogen peroxide for in-office bleaching significantly reduces bracket bond strength, whereas 10% carbamide peroxide does not have a significant impact. The findings of this study are consistent with those of these researchers, indicating that the use of 35% hydrogen peroxide for in-office cold light bleaching significantly lowers the bond strength of brackets, with a statistically significant difference (p < 0.05) observed between groups G1 and G2. In addition, several scholars2,8,12,18–25 have noted significant variations in the bond strength of brackets after bleaching, with effects ranging from immediate to 4 weeks post-treatment. Further, Matta et al.26–28 found that using 10% carbamide peroxide for bleaching significantly increases bracket bond strength, with no restrictions on the timing for bonding brackets afterward.
Reynolds 29 determined that the minimum bond strength required in orthodontic practice is 6–8 MPa, as this level can withstand chewing and orthodontic forces. In this study, the average SBS values for all experimental groups exceeded the minimum clinical requirement. Therefore, following Beyond cold light bleaching, brackets can be bonded 24 h later, regardless of whether a desensitizer is used.
The impact of bleaching on the surface structure of teeth
Enamel is the only acellular structure in the body and the hardest tissue, primarily composed of crystals formed by ions such as calcium and phosphate, with organic materials and water constituting only a small fraction. Approximately 86% of its total volume is made up of inorganic materials. This study observed varying degrees of demineralization and dissolution on the enamel surface after bleaching with 35% hydrogen peroxide, revealing a significant number of micropores (as shown in Fig. 3B), a phenomenon documented in several studies.16,30,31 Moreover, the loss of minerals in the enamel extends beyond the visible surface, potentially affecting the subsurface enamel as well. 32
Scherer et al. 33 found that bleaching does not cause significant changes to the surface structure of enamel, nor does it lead to over-etching. Conversely, Rotestei et al. 34 and Perdigão et al. 35 reported that bleaching can decrease the calcium-to-phosphate ratio in enamel, altering its chemical composition and crystal arrangement, which may lead to reduced enamel thickness. Other researchers have reached similar conclusions, indicating that significant changes in tooth structure occur after bleaching over periods ranging from 24 h to 4 weeks. Consequently, they recommend delaying bracket bonding to allow for the recovery of bonding performance before the bleaching process. Jose et al. 36 discovered that bleaching disrupts the enamel surface structure, thereby affecting the bond strength between enamel and composite resin. Observations using optical microscopy indicated that bleaching results in a loss of enamel minerals, which is particularly pronounced at 24 h post-bleaching and persists even after 12 weeks in artificial saliva. Enhanced magnification with scanning electron microscopy allows for clear observation of specific changes in enamel surface structure after bleaching. In this experiment, scanning light microscopy revealed that acid etching post-bleaching causes a loss of prism shape and exhibits signs of over-etching (as shown in Fig. 3I). Further, the loss of calcium ions, reduction in enamel microhardness, and alterations in organic materials can all contribute to decreased bond strength of brackets.
The impact of residual bleaching agents on bond strength
After tooth bleaching, etching with 37% phosphoric acid for 30 sec, as observed through laser scanning microscopy, reveals significant acid erosion on the enamel surface. This erosion can greatly increase the surface area available for bonding, suggesting that the bond strength of the brackets should theoretically increase. However, the results of this study indicate that the SBS 24 h post-bleaching (7.50 ± 1.77 MPa) is significantly lower compared with the control group (12.24 ± 3.71 MPa; p < 0.05). This suggests that bleaching substantially reduces bracket bond strength, and the decrease in bond strength after bleaching is related not only to the surface structure of the enamel but also to additional factors. Numerous scholars have demonstrated through in vitro and in vivo experiments that the reduction in bond strength following bleaching is also associated with residual bleaching agents.
The most commonly used bleaching agents in-office are 35–50% hydrogen peroxide, which is 7–16 times stronger than those used at home. 17 In-office bleaching employs higher concentrations of peroxide, often combined with light, to accelerate the reaction and produce immediate effects; however, this may also lead to a substantial increase in the concentration of residual peroxide on the tooth surface. The presence of these residual bleaching agents can adversely affect the bonding process, as they rapidly decompose and release oxygen into the pores of the tooth surface, thus impacting the curing of the bonding system.37–39 Compared with non-bleached enamel, bleached enamel surfaces exhibit a higher number of short resin tags, resulting in decreased bond strength.5,13–15 Over time, as residual oxygen is eliminated, the bond strength of the enamel surface may increase. 38 Some researchers recommend using pumice before bonding to reduce residual hydrogen peroxide and mitigate the impact of residual bleaching agents on bracket bond strength. They also suggest delaying bracket bonding for a period ranging from 24 h to 4 weeks post-bleaching to allow for the complete consumption of residual bleaching agents. In addition, Bulut et al.3,23,37 recommend using 10% sodium perborate (an antioxidant) for bleaching to counteract the reduction in bond strength associated with immediate bonding after bleaching. Sun et al. 40 suggest using bonding agents containing ethanol after bleaching to mitigate or eliminate the effects of residual oxygen on bond strength. All these findings are noteworthy and warrant further investigation.
The impact of desensitizers on tooth surface
Tooth sensitivity is one of the most common side effects of tooth bleaching. 15 Bleaching agents can penetrate enamel and dentin, promoting the release of inflammatory mediators within the dental pulp and damaging pulp cells.4,41 Various measures have been implemented to prevent tooth sensitivity during the bleaching process, including taking analgesics prior to bleaching, reducing the concentration of bleaching agents, shortening the duration of bleaching, and applying desensitizers.42–44 Some studies recommend incorporating desensitizing agents like potassium nitrate and fluoride into bleaching formulations to mitigate sensitivity during the process. Research indicates that desensitizing with potassium nitrate and sodium fluoride before bleaching does not alter the incidence of tooth sensitivity among patients, but it does reduce its intensity. 45 Meng Deng et al. 46 reported that the application of 45S5 bioactive glass before and during bleaching does not compromise the whitening effect and can aid in remineralization, thereby preserving the integrity of the tooth surface.
The desensitizer utilized in this study is primarily composed of bioactive mineral materials and represents China’s first nano-sized bioactive desensitizer for teeth. The powder particles of this desensitizer range in diameter from 200 to 800 nm, providing a large specific surface area that facilitates rapid penetration into smaller pores in the teeth. This process releases silicon ions, calcium ions, and phosphorus ions—active components that promote mineralization. Initially, a silica-rich layer forms, followed by the absorption of calcium and phosphorus ions to create a calcium phosphate layer, which subsequently crystallizes into carbonate apatite, completing the remineralization process and effectively sealing the pores for desensitization. In addition, upon contact with saliva, the powder releases sodium ions, raising the local pH to 8–8.5. This alkaline environment not only neutralizes the acidity of the hydrogen peroxide in the bleaching agent but also enhances the formation of hydroxyapatite. When this desensitizer is applied alone to the enamel surface, it can form a layer of carbonate apatite. Following phosphoric acid etching, the normal structure of the enamel surface is compromised, exhibiting severe demineralization and a rough, weathered, rock-like appearance. Although the SBS of brackets bonded 24 h after desensitization (11.68 ± 3.49 MPa) shows a slight decrease compared with the control group, the difference is not statistically significant (p > 0.05), indicating that the desensitizer does not significantly affect the SBS of brackets. These findings contrast with those of Tukkahraman et al., 15 who observed a significant decrease in bond strength when employing potassium nitrate and oxalate desensitizers on enamel. Clinical observations suggest that the desensitizing effect of this product is favorable when used post-bleaching. Experimental studies on SBS reveal significant statistical differences between G1 and G4 (p < 0.05), while G1 shows no statistical differences compared with G5, G6, and G7 (p > 0.05). The enamel surface, when compared with Figure 3B, appears relatively smooth with significantly reduced porosity, demonstrating the immediate effectiveness of sealing and remineralization provided by the desensitizer. Although the SBS significantly decreases when brackets are bonded 24 h after bleaching with desensitization, it shows slight enhancement compared with the group that did not use a desensitizer post-bleaching. Moreover, this desensitizer is fluoride-free, making it suitable for use by pregnant women and children, thus deserving clinical promotion.
ARI value
Following bracket detachment, adhesive residue remains on both the enamel surface and the base of the bracket. The location of bond failure during detachment varies, leading to differences in the amount of adhesive left on the enamel and the bracket base. The residual adhesive was examined using a 10× magnifying glass, and the ARI values of each sample were recorded according to the ARI scoring criteria, which effectively reflect the characteristics of bond failure. The ARI values for the samples in this study are presented in Table 3 and Figure 2. Statistical analysis in Table 3 reveals no significant differences between groups (p > 0.05). Figure 2 illustrates that groups 3, 4, and 5 exhibit higher frequencies, suggesting that bond failures primarily occur at the resin-enamel interface (G2, G4) or within the resin itself (G1, G3, G5, G6, G7). When bond failure occurs within the resin, the integrity of the enamel surface can be preserved. Conversely, failure at the enamel-resin interface can facilitate the removal of residual adhesive from the enamel surface and minimize damage during this process. However, bracket detachment can still cause enamel damage. Similar conclusions have been reached by other researchers.18,46 While ensuring the clinical requirement for SBS, efforts should focus on preserving enamel integrity during bracket detachment.
Limitations and outlook of this study
The teeth utilized in this experiment were extracted specimens with necrotic dental pulp that lacked nutritional supply. In addition, the environment in which the teeth were placed did not fully replicate the human oral cavity; rather, it aimed to simulate oral conditions as closely as possible under the given circumstances. Achieving an environment that completely matches intraoral conditions is not feasible. The oral environment is highly complex, continuously undergoing dynamic changes in temperature, pressure, humidity, pH, biological enzymes, and dental plaque. It is crucial to recognize that there are notable differences between in vitro and in vivo testing; the forces applied during testing between the bracket and adhesive differ from the compressive forces experienced during natural chewing, which can result in significant damage to the enamel.5,13–15
With the ongoing development and advancement of various new materials and technologies, the SBS of brackets remains a focal point in orthodontics. The detachment of brackets can influence treatment efficacy, increase the need for follow-up visits, and elevate costs for patients. Therefore, further research is warranted to explore the effects of bleaching, desensitization, and the combination of these treatments on the SBS of brackets.
Conclusions
Both bleaching and the combination of bleaching with desensitization significantly reduce the SBS of brackets 24 h after bonding; however, the measured values still meet clinical requirements, indicating that bonding can be performed after this period. The application of a nano-sized bioactive desensitizer results in a slight decrease in the SBS of brackets but aids in repairing the damage caused by bleaching. Over time, the effects of bleaching and desensitization on SBS diminish, returning to normal levels after 1 week.
Authors’ Contributions
L.W.: Conceptualization, investigation, methodology, data curation, visualization, validation, formal analysis, writing original draft, and writing—review and editing; L.L.: Formal analysis, visualization, and writing—review and editing; J.S. and S.X.: Conceptualization, supervision, visualization, resources, writing—review and editing, and project administration. All authors read and approved the final article.
Footnotes
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
This study was funded by the National Natural Science Foundation of China [12202274] and supported by the Interdisciplinary Program of Shanghai Jiao Tong University (Project No. YG2022QN049).
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.