
Abstract
Purpose:
Demodex folliculorum infestation is an important contributor to meibomian gland dysfunction (MGD) and chronic ocular surface disease. This study evaluated and compared the therapeutic efficacy of intense pulsed light (IPL) and eyelid hygiene (ELH) for Demodex-associated MGD.
Methods:
In this prospective, randomized comparative trial, 50 patients (100 eyes) with Demodex-associated MGD were allocated to two arms. Group A (n = 25) received three Eyesis IPL sessions at baseline, week 2, and week 4. Group B (n = 25) performed daily eyelid hygiene with OCuSOFT Lid Scrub for 6 weeks. Ocular surface parameters, including ocular surface disease index (OSDI), tear film lipid layer thickness (TFLL), noninvasive tear film break-up time (NITBUT), meibomian gland dropout, meibum quality and expressibility, corneal fluorescein staining (CFS), Schirmer’s I, and Demodex count, were assessed from baseline to week 6. Best-corrected visual acuity (BCVA) and intraocular pressure (IOP) were recorded at each visit.
Results:
Both treatments significantly improved OSDI, NITBUT, TFLL, Schirmer’s I, and CFS over 6 weeks (all p < 0.001). Compared with ELH, IPL achieved larger and earlier reductions in symptoms, greater increases in TFLL, and superior improvements in meibum quality and expressibility from week 4 onward (between-group p ≤ 0.021). Demodex counts decreased significantly in both groups with no between-group difference at week 6. BCVA, IOP, and adverse events remained stable, indicating a favorable short-term safety profile.
Conclusion:
IPL and ELH are effective for Demodex-related MGD, but IPL provides faster and more pronounced improvements in meibomian gland function, tear film stability, and patient-reported symptoms over 6 weeks.
Introduction
Meibomian gland dysfunction (MGD) is a chronic, multifactorial condition, and the leading cause of evaporative dry eye disease (DED) worldwide, significantly affecting ocular health and quality of life. 1 It involves obstruction of gland ducts and abnormal secretion, resulting in altered meibum composition, tear film instability, ocular inflammation, and discomfort. 2 With a global prevalence of 35–70%, MGD is among the most common disorders in ophthalmic practice.3,4 Demodex infestation is a frequently overlooked contributor to MGD. 5 These ectoparasites inhabit eyelash follicles and meibomian glands (MGs), and when overpopulated, they obstruct ducts, trigger granulomatous inflammation through their exoskeleton and waste products, and may introduce bacteria such as Bacillus oleronius, whose antigenic proteins further aggravate ocular surface inflammation. 6
Managing Demodex-associated MGD is difficult because mites reside deep in follicles and are protected by a rigid exoskeleton. Standard care emphasizes eyelid hygiene (ELH) to lower mite burden. OCuSOFT Lid Scrub (OLS) contains terpinen-4-ol (T4O), the principal bioactive component of tea tree oil (Melaleuca alternifolia), which has demonstrated pediculicidal activity against head lice. 7 T4O has antimicrobial and anti-inflammatory properties; at higher concentrations, it can sting and irritate the ocular surface. Daily TTO-based lid scrubs, combined with in-office debridement, reduce mite counts and improve symptoms.8,9 Intense pulsed light (IPL) has emerged as a promising therapy for MGD. 10 First used in dermatology for rosacea and pigmentary disorders, IPL delivers noncoherent light between 500 and 1200 nm. 11 Prieto et al. observed reduced Demodex viability after IPL and proposed that mite chromophores absorb IPL energy, leading to coagulative necrosis and mite death. 12 Heat may also contribute, since Demodex does not survive temperatures above 54°C. 13 IPL liquefies inspissated meibum, facilitates gland expression, and improves the lipid layer of the tear film. 14 Outcomes depend on device type and treatment area. Growing clinical evidence shows improvements in symptoms, meibum quality, and tear film stability, along with substantial reductions in Demodex density, supporting IPL for Demodex-associated MGD. 15
Both ELH using OLS and IPL are proven treatments for Demodex-related MGD, but differ fundamentally; OLS acts as a continuous chemical acaricide, whereas IPL employs periodic photothermal energy. As randomized controlled trials have not directly compared these two approaches, this prospective study aimed to evaluate their relative efficacy. It assesses outcomes beyond mite eradication, including symptom relief, MG function, tear film stability, and patient comfort, providing evidence to guide the clinical management of Demodex-associated MGD.
Methods
Subject recruitment and ethics compliance
This prospective randomized clinical trial was conducted at the Dry Eye Clinic of the Tianjin Medical University Eye Hospital. Fifty consecutive adults (18–80 years) with Demodex-related MGD were enrolled between April 2024 and August 2025 and randomly assigned to two arms. Group A (n = 25) underwent three IPL sessions at baseline, week 2, and week 4. Group B (n = 25) underwent daily ELH with OLS for 6 weeks. Participants were examined at baseline and at weeks 2, 4, and 6. The study adhered to the Declaration of Helsinki, received approval from the Tianjin Medical University Eye Hospital Ethics Committee (2025KY-22), and was registered at https://www.chictr.org.cn/indexEN.html, ChiCTR2600117086. All participants provided written informed consent after a full explanation of the procedures and objectives.
Study criteria
Eligible participants met the following criteria: (1) age ≥18 years; (2) diagnosis of MGD-related dry eye per the 2020 Chinese Consensus on Dry Eye (examination/diagnosis criteria); (3) bilateral MGD at any stage per the International Workshop on MGD; and (4) detectable Demodex on eyelashes. Exclusion criteria were: (1) age >80 years; (2) lacrimal gland disorders, active ocular inflammation, eyelid entropion/ectropion, uveitis, or other significant ocular disease; (3) history of ocular trauma, chemical burns, ocular surgery, contact lens wear, systemic rheumatic/immune disease, Sjögren’s disease, pregnancy, or lactation; and (4) use of any ocular medication within the week before enrollment. A computer-generated sequence and an allocation method were used to allocate eligible participants to the two study groups. All subjective and objective assessments were performed by the same experienced ophthalmologist, who was not aware (blinded) of the participants’ treatment allocation.
Participants attended the Tianjin Medical University Eye Hospital Dry Eye Clinic for four visits: baseline, week 2, week 4, and week 6. At each visit, the ocular surface parameters were assessed to track treatment-related changes over time. Examinations were performed in a standardized sequence, from the least to the most invasive, to minimize test interference and ensure consistency across visits (Fig. 1). Ocular surface characteristics were measured using the assessments in the following order of least invasive to most invasive: OSDI questionnaire, tear film lipid layer thickness (TFLL), non-invasive tear film break-up time (NITBUT), MG dropout, meibum expression, meibum quality, corneal fluorescein staining (CFS), Schirmer’s I, and Demodex count.
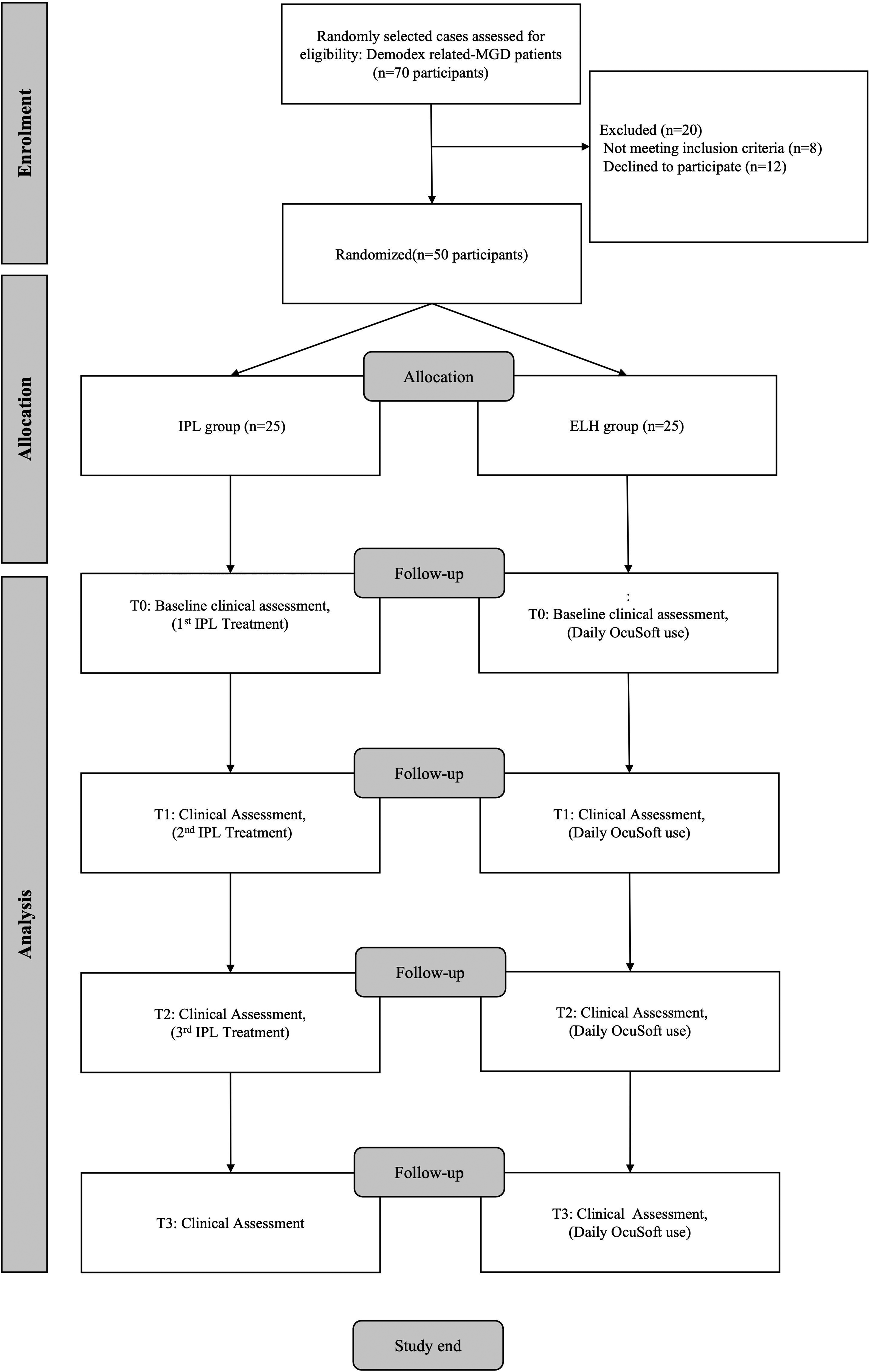
Study design.
Diagnosis of ocular demodex infestation
Three eyelashes from each eyelid, along the nasal, center, and temporal sides, were epilated under a slit-lamp microscope. A total of 12 eyelashes, specially selected with cylindrical dandruff (CD), were removed and placed on glass slides. A coverslip was placed on the lashes, and two drops of normal saline solution were slowly pipetted at the edge of the coverslip. Demodex mites were examined under a microscope at 10 × and 40 × magnification after 20 min. The total number of mites was calculated for both eyes. If the number of Demodex was ≥1, it was recorded as infected; if <1, it was recorded as no infection. 16
Objective assessments
NITBUT and tear meniscus height (TMH) were measured three times consecutively using the Keratograph 5 M (Oculus, Germany) topographer, and the average values were recorded. 17 Specifically, an image of the inferior tear meniscus was captured instantaneously during the TMH measurement process. 18 TFLL assessment was performed with the DR-1 equipment, produced by Kowa in Nagoya, Japan. The results were evaluated on a scale of 1–5.16,19 The blink frequency is recorded through video. CFS was used to evaluate ocular surface injury, enhanced cobalt-blue illumination with a yellow filter, and graded using the Oxford Score (0–5 for the total cornea) TFOS DEWS II Diagnostic Methodology report.2,20 Schirmer’s I was assessed without topical anesthesia for 5 min. MG dropout was assessed using a Keratograph 5 M (Oculus, Wetzlar, Germany), which captured MG images using infrared light. MG dropout was scored from 0 to 3 for each eyelid (0 = no loss of MG; 1 = loss of MG <1/3 area; 2 = loss of MG 1/3–2/3 area; 3 = loss of MG >2/3 area). 21 For MG expression each part of five MGs in the nasal, middle, and temporal regions of the eyelid were evaluated on a scale of 0–3 (0 = expression from all 5 glands; 1 = expression from 3 to 4 glands; 2 = expression from 1 to 2 glands; 3 = no expression). 22 Meibum quality was evaluated from eight glands at the center of the eyelid using a score of 0–3 for each gland (0 = clear; 1 = cloudy; 2 = cloudy with granular debris; 3 = thick, like toothpaste). 23
Subjective assessments
A Chinese-language validated OSDI questionnaire was used to assess dry eye symptoms over the past 2 weeks. The OSDI questionnaire consisted of 12 questions, with a total score ranging from 0 to 100. A higher total score indicates greater severity of dry eye symptoms. 24
Treatment procedure
In group A, IPL treatment was administered bilaterally using the Eyesis device (MDC, Beijing, China) at 2-week intervals. The pulse intensity of Eyesis ranged from 5 to 15 J/cm2 and was determined by the combination of Fitzpatrick Skin Type Grading (scale I–IV). 25 Before treatment, protective opaque goggles were placed over both eyes, and a conductive gel was applied to the patient’s periocular area to conduct light and evenly distribute energy. 26 In each IPL treatment, five overlapping flashes were applied to the skin area below the lower eyelid of each eye with no pressure, with each pulse slightly overlapping the previous one. Routine treatment areas for IPL include the skin below the lower eyelid and the temples on both sides. 27 All treatments were performed by a trained clinician who was not involved in the data collection or statistical analysis. In group B, Step-by-step instructions were provided to each participant for nightly eyelid wiping pads at home. The ELH routine was identical across treatments. Participants in the ELH group were instructed to wash their hands, unfold a pre-moistened OLS cleanser pad, and wrap it around a finger. With the eye closed, they gently cleansed the eyelid using side-to-side strokes, taking care not to touch the eye directly. They then rinsed thoroughly and repeated the procedure on the other eyelid. 28
Safety assessment
The safety of the treatment was evaluated using the best-corrected visual acuity (BCVA) and intraocular pressure (IOP). BCVA was recorded as logMAR. IOP was assessed using a noncontact tonometer (NT-510; NIDEK, Japan). No systemic adverse events were recorded during the trial. BCVA did not vary substantially between the baseline and subsequent visits in either group.
Statistical analysis
Statistical analyses were performed using SPSS for Windows (version 26, IBM Corp.). Data from both eyes were collected at baseline, week 2 (first follow-up), week 4 (second follow-up), and week 6 (third follow-up) for all treated patients. Bilateral eyes of all participants are analyzed. Repeated-measures analyses were used to compare outcomes over time, and paired tests were applied to assess pre- versus post-treatment changes at specific visits. The Kolmogorov–Smirnov test was used to assess the normality of continuous variables. Baseline characteristics were summarized as mean ± standard deviation for continuous variables and as frequencies and percentages for categorical variables. Ordinal or non-normally distributed data were analyzed using analysis of variance (ANOVA). The primary outcome measures were OSDI scores before and after treatment. For the primary endpoint, between-group comparisons were conducted using ANCOVA, with baseline values as covariates, to obtain adjusted means, 95% confidence intervals, and p-values.
Sample size
The sample size was computed using the PASS 2021. The computation of sample size is predicated on NITBUT. A sample size of 46 (23 per group) is adequate for the NITBUT to identify a clinically significant difference of 1 s between groups in alleviating DED, assuming a standard deviation of 1.0 s, utilizing a two-tailed t-test for mean differences with 90% power and a 5% significance level. Given a dropout rate of 10%, the required sample size is 50 (25 per group).
Results
Demographics data
Table 1 summarizes the demographics and ocular surface parameters of participants randomized to IPL (n = 50 eyes) and ELH (n = 50 eyes). The groups were broadly comparable at baseline, with two exceptions. Randomization achieved a good baseline balance across clinical, symptomatic, and tear film parameters. The IPL group was slightly older and had lower Schirmer’s I values, although this was not statistically significant.
Demographic Data
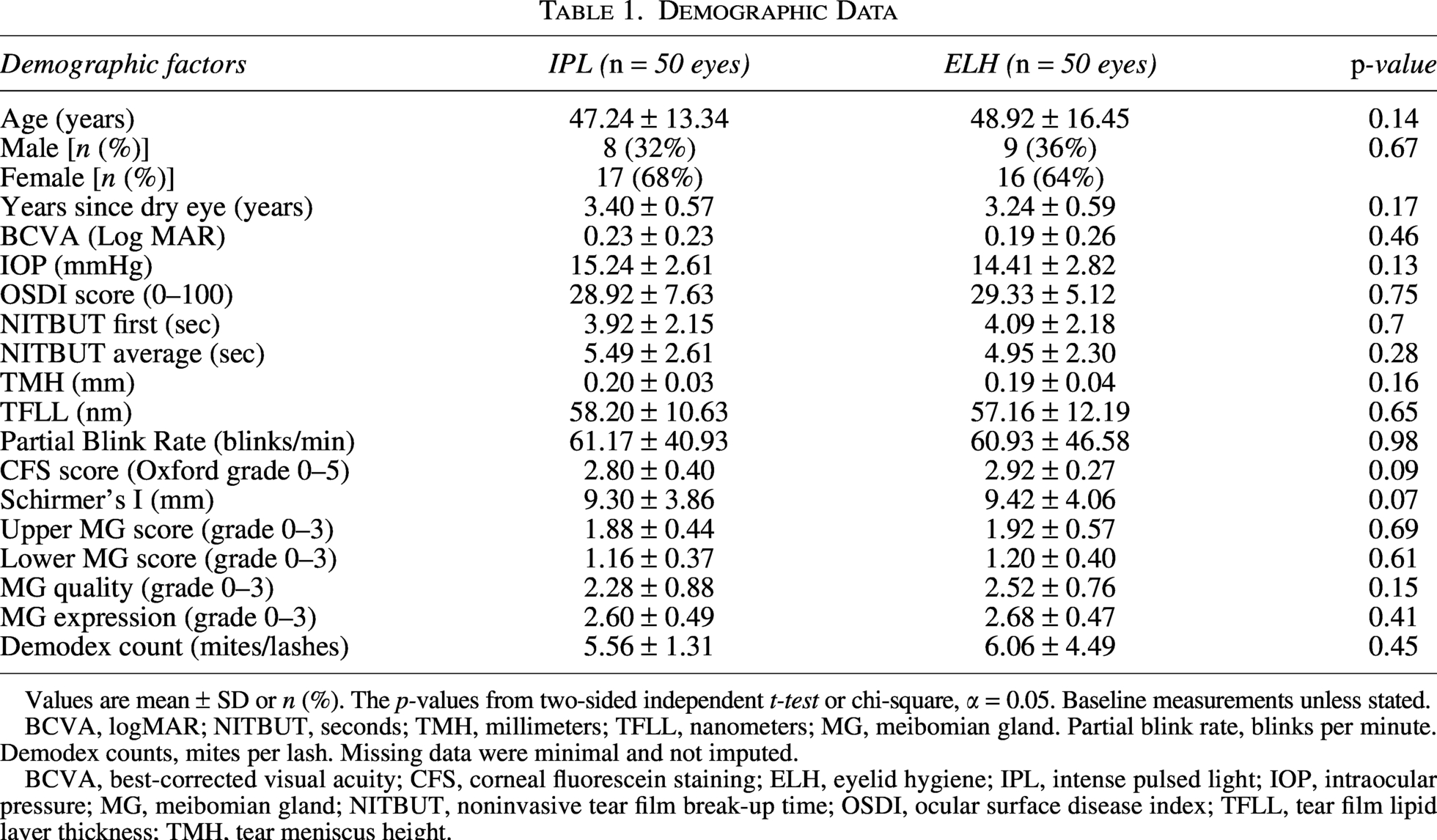
Values are mean ± SD or n (%). The p-values from two-sided independent t-test or chi-square, α = 0.05. Baseline measurements unless stated.
BCVA, logMAR; NITBUT, seconds; TMH, millimeters; TFLL, nanometers; MG, meibomian gland. Partial blink rate, blinks per minute. Demodex counts, mites per lash. Missing data were minimal and not imputed.
BCVA, best-corrected visual acuity; CFS, corneal fluorescein staining; ELH, eyelid hygiene; IPL, intense pulsed light; IOP, intraocular pressure; MG, meibomian gland; NITBUT, noninvasive tear film break-up time; OSDI, ocular surface disease index; TFLL, tear film lipid layer thickness; TMH, tear meniscus height.
Comparative analysis
Table 2 displays the comparative assessments of the two groups. IPL and ELH produced significant improvements in symptoms and multiple ocular-surface signs, with several outcomes favoring IPL (Table 2). The OSDI score decreased significantly in each group (both p < 0.05). Between-group differences emerged from Follow-up 2 and were strengthened by Follow-up 3 (OSDI lower with IPL; p = 0.021 and p < 0.05, respectively). NITBUT-first and NITBUT-average increased substantially in both arms (all p < 0.05), with no significant between-group differences at any time point. TMH increased in both groups (both p < 0.05), but was consistently higher with IPL at Follow-ups 1–3 (all p < 0.05). Schirmer’s I test results increased in both arms (both p < 0.05), TFLL increased in both groups (both p < 0.05), with greater gains in the IPL arm (between-group p = 0.016 at Follow-up 1; p < 0.05, at Follow-ups 2 and 3). The partial blink rate showed no significant within-group changes (IPL: p = 0.30; ELH: p = 0.28). A transient between-group difference appeared at Follow-up 2 (p = 0.005), with higher rates in the ELH group. Oxford corneal staining scores decreased markedly in both groups (both p < 0.05). IPL scores were lower at Follow-ups 2 and 3 (both p < 0.05). Upper and lower MG scores were stable (no within-group changes; no between-group differences). In contrast, MG quality and expressibility improved substantially with IPL (both within-group p < 0.05) and were significantly better than those with ELH at Follow-ups 2 and 3 (both p < 0.05). ELH showed minimal changes (MG quality p = 0.58; MG expressibility p = 0.11). Demodex burden counts decreased significantly within each arm by the final follow-up (both p < 0.05), with no significant between-group difference at that time (p = 0.076).
Longitudinal Comparative Group Assessments
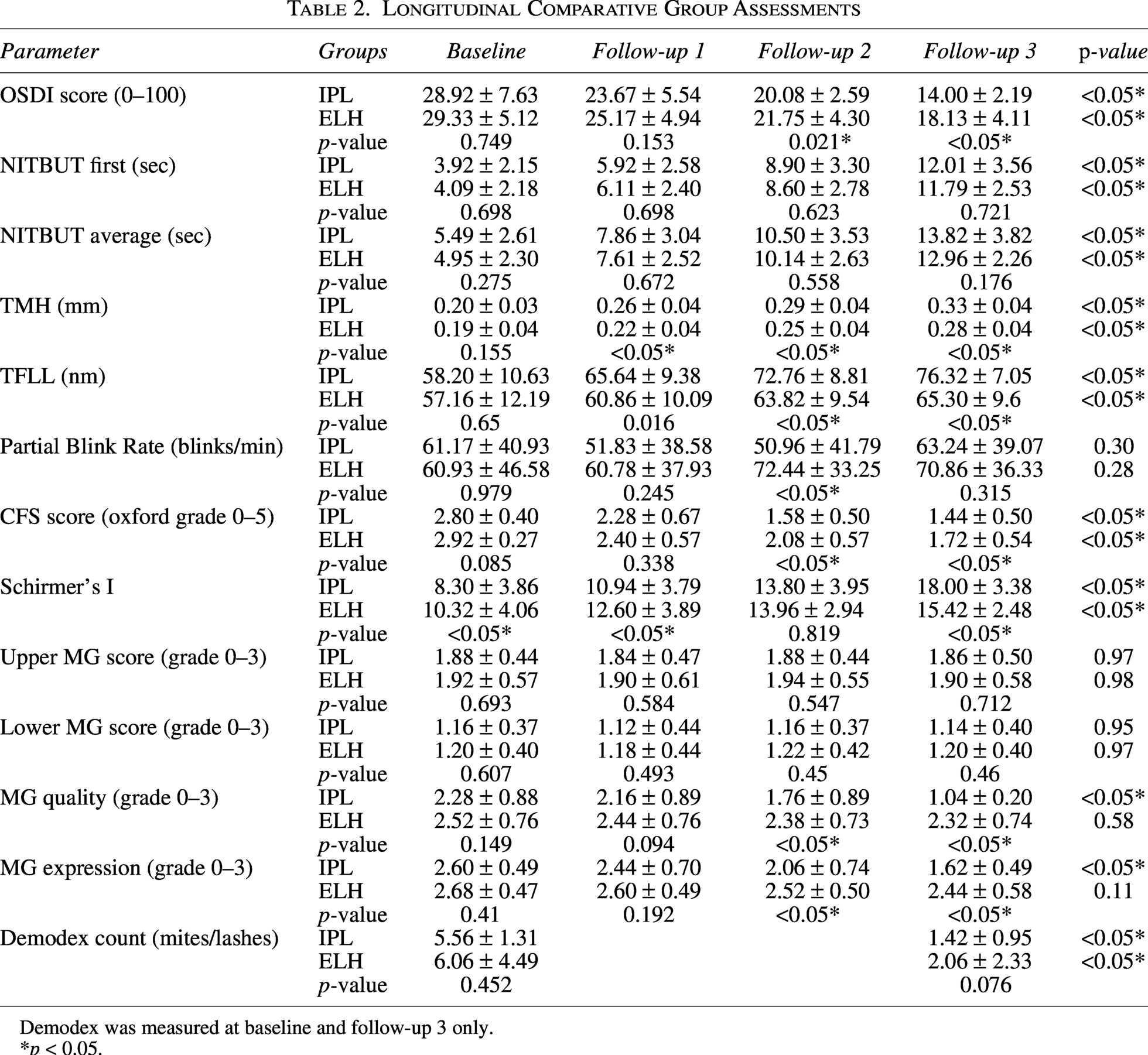
Demodex was measured at baseline and follow-up 3 only.
p < 0.05.
Comparison of Safety Parameters between the IPL and ELH Groups
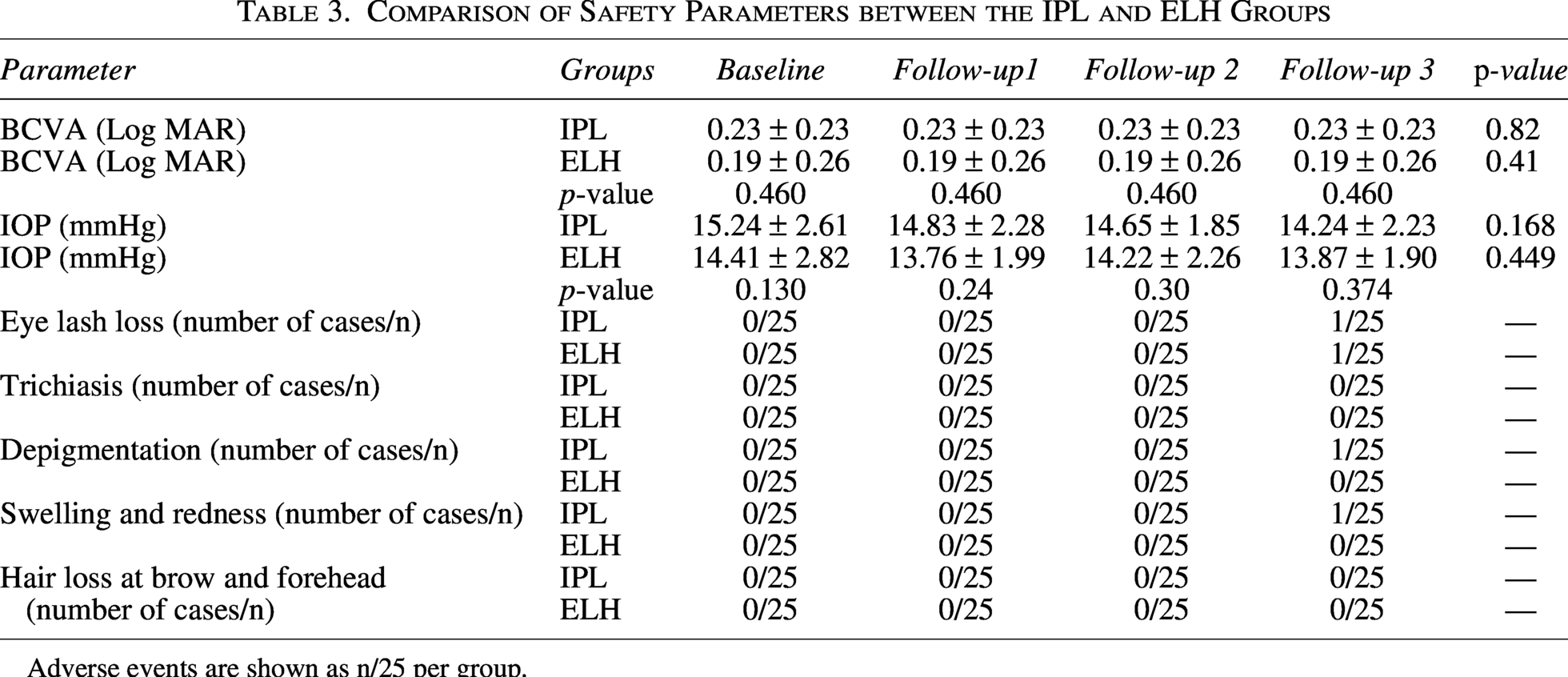
Adverse events are shown as n/25 per group.
Safety assessment
As depicated in Table 3, BCVA and IOP remained stable in both groups, with no within-group change (IPL: BCVA p = 0.82, IOP p = 0.168; ELH: BCVA p = 0.41, IOP p = 0.449) and no between-group differences at any visit (BCVA all p > 0.05). Adverse events were rare: eyelash loss 1/25 per group at follow-up 3; depigmentation and transient swelling/redness 1/25 in the IPL-only group; no trichiasis or brow/forehead hair loss. However, none of the reported events were clinically significant. No clinically significant depigmentation, blistering, edema, ocular surface redness, hair loss, or eyelash loss was observed after IPL therapy.
Discussion
In this randomized controlled study, we compared the therapeutic effects of IPL and ELH using tea tree oil-based lid wipes in patients with Demodex-associated MGD. Both treatments produced meaningful improvements in symptoms and ocular-surface parameters; however, IPL yielded faster and more pronounced gains in tear film stability, MG function, and patient-reported comfort over 6 weeks. These findings align with growing clinical evidence supporting IPL as an effective intervention for refractory MGD and evaporative DED, particularly in patients with Demodex infestation.14,29
Prior studies have suggested possible sex-related differences in infestation rates, linked either to androgen-mediated sebum production30,31 or increased cosmetic use in women, 32 but our findings suggest that local lid hygiene practices and glandular function may be more relevant determinants than sex alone.
IPL demonstrated a higher reduction in Demodex counts compared with ELH. Laboratory and clinical observations indicate that IPL’s photothermal effects can exceed temperatures required for mite survival, impairing cellular integrity and inducing coagulative necrosis.13,33,34 IPL also produces vascular-selective photothermolysis along the lid margin, reducing telangiectasia and local inflammatory mediator release. 35 Additionally, IPL heats and liquefies inspissated meibum, facilitates gland expression, and improves lipid layer thickness. 35 Experimental studies suggest that IPL may further enhance mitochondrial ATP production and fibroblast proliferation, potentially supporting acinar cell function and microstructural remodeling.36,37 These mechanisms collectively explain the superior improvements in MG quality and expressibility observed in our IPL group.
On the other hand, OLS contains terpinen-4-ol (T4O), the most active component of tea tree oil, which disrupts mite cell membranes, leading to immobilization and death, and is more effective than whole tea tree oil at equivalent concentrations. 8 Its antimicrobial properties reduce Bacillus oleronius-related antigenic stimulation, thereby diminishing eyelid margin inflammation. 6 Regular lid debridement also removes CD, improves meibomian orifice patency, and decreases gland obstruction, supporting better meibum flow and tear film stability in Demodex-associated MGD. 23 Although gland function improved significantly, MG dropout scores remained unchanged over the 6-week follow-up. This is consistent with previous work showing that gland atrophy reflects chronic structural change influenced by aging, sex, and longstanding gland obstruction.35,38 Anatomical differences may also contribute; inferior glands tend to exhibit greater obstruction due to the counter-gravitational flow of meibum, predisposing them to atrophy. 39 Lateral gland loss is also more common than central loss, with nasal-side disease often predominating. 39 Longer-term studies are needed to determine whether IPL can induce structural recovery or simply improve function within existing gland architecture.
Both IPL and ELH demonstrated favorable safety profiles. IPL requires careful periocular shielding to prevent unintended exposure to ocular tissues, as improper protection has been associated with pigmentary change, follicular damage, or rare inflammatory complications. No serious adverse events occurred in this study. The mild and transient effects observed, such as temporary redness or discomfort, are consistent with prior reports.35,40 The comparative efficacy observed in this trial supports a multifactorial pathophysiology for Demodex-associated MGD, in which both acaricidal and anti-inflammatory mechanisms are therapeutically relevant. IPL provides robust mite reduction, improves glandular function, and enhances tear film stability, making it an effective modality for patients with significant gland obstruction of MG or refractory dry eye symptoms.14,41,42 ELH remains an accessible first-line therapy, particularly given the proven acaricidal activity of terpinen-4-ol in tea tree oil.43–45 The complementary mechanisms of IPL and ELH underscore the potential value of combination or staged therapy in clinical practice.
The sample size was modest, and the follow-up period was relatively short to assess long-term gland structural changes. Additionally, standardized treatment intervals for IPL have not been established, and the optimal dosing regimen remains unknown. Future multicenter trials with larger cohorts and longer observation windows are necessary to refine treatment protocols and assess the durability of therapeutic effects.
Conclusion
In this randomized controlled study, both IPL and ELH improved symptoms and ocular-surface parameters in Demodex-associated MGD. However, IPL produced faster and greater improvements in MG function, tear film stability, and patient-reported outcomes. These effects likely reflect IPL’s combined photothermal, anti-inflammatory, and acaricidal mechanisms, which extend beyond the surface-level benefits of ELH. MG structure did not change over 6 weeks, highlighting the chronic nature of gland atrophy. Overall, IPL appears to be a more effective short-term treatment option for Demodex-associated MGD, with favorable safety and clinical utility.
Ethical Approval
All procedures performed in studies involving human participants were conducted in accordance with ethical standards and the Institutional Review Board, as well as the Helsinki Declaration and its later amendments, or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Authors’ Contributions
Review and editing: S.J., Q.L., Y.J., Z.Y., H.L., E.E.P., S.Z., and Y.H. Final approval of article: E.E.P., S.Z., Y.H., S.J., and Q.L. contributed equally to this study. S.J.: Study design, data collection, analysis, article drafting, and article editing. Q.L.: Study design, data collection, analysis, article drafting, and article editing. E.E.P., S.Z., and Y.H.: Study design, interpretation of results, article editing, study oversight, and provision of feedback. S.J. and Q.L.: Article editing, interpretation of results, and provision of feedback. E.E.P., S.Z., and Y.H.: Study design, interpretation of results, article editing, study oversight, and provision of feedback.
Footnotes
Acknowledgments
The authors would like to thank all participants and their colleagues involved in this study.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This study was funded by the Tianjin Key Medical Discipline Construction Project (TJYXZDXK-3-004A-2).