
Abstract
Aim:
To assess the effectiveness of photobiomodulation therapy for managing oral lichen planus (OLP) and recurrent aphthous stomatitis (RAS), including their outcomes and patient satisfaction with the safety profile.
Method:
A systematic review was conducted by searching electronic databases like PubMed Central, PubMed, Cochrane, CrossRef, Google Scholar, and Embase. Articles published until June 2025 were reviewed using MeSH (Medical Subject Heading) and various combinations of the keywords: oral lichen planus, Recurrent Aphthous Stomatitis, photobiomodulation therapy, and conventional drug therapy. We considered two different outcomes, such as pain and the size of the lesion. Due to the heterogeneity of the data, we did not conduct any statistical analysis.
Result:
Initially, 560 publications were selected for this review article, and after analyzing all these, only 12 articles fulfilled the inclusion and exclusion criteria. In all those studies, the laser wavelength, power output, and duration of irradiation changed between 630–980 m, 20–30 mW, and 10 sec–15 min have been described. Topical medications used in the comparative group were amlexanox, triamcinolone acetonide, granofurin, and socosenyl. Our findings showed that the photobiomodulation laser group is more effective for decreasing the pain and lesion size of RAS and OLP in comparison with the topical medication group.
Conclusion:
We can conclude that photobiomodulation therapy was better for treating RAS and OLP with greater healing, patient satisfaction, and lower recurrence rate in comparison with other topical drug therapies.
Keywords
Introduction
Recurrent aphthous stomatitis (RAS) is a common chronic condition where approximately 25% of the general population is affected, known as canker sores or aphthae, with the reorganization of multiple flat, painful ulcers that have shown nerve endings and are linked to pain.1–3 This type of frequent oral mucosal disease usually manifests 0.5% in Malaysia, 4 10%–15% in the USA, 5 17.7%–25% in Iran, 6 Canada 46.4%–69.4%, Europe 36%–37%, Sweden 0.5%–2%, Turkey 1.2%–2.3%, Jordan 78%, Iraq 28.2%, India 50% And Germany 2%–10%.After analysis of all the populations of these countries, we could establish that young adults and females with higher socioeconomic status are mostly affected by RAS.7,8 It could be harmful to the individual’s quality of life with the impairment of eating, swallowing, and speaking. 9 According to their magnitude, duration of outbreaks, and numbers, this lesion has been classified into major, minor, and herpetiform. The minor RAU identified approximately (70%–85%) of all cases covered by a greyish-white pseudo membrane bounded by an erythematous halo.10,11 Major RAS is the severe form of the disease and represents 10% of all cases. The herpetiform is 2–3 mm in diameter, which represents 10%–15% of all cases.12–15 The etiology of RAS is not clear. 16 However, the primary predisposing factors for this disease include alpha-hemolytic-streptococcal infection, genetic factors, deficiencies in folic acid or iron, vitamin B12 deficiencies, trauma, etc.17–20
OLP is a comparatively common chronic condition affecting 0.3%–2.3%of adults.21–23 It is classified into three major categories and recognized in the skin: genital mucosa, scalp, nail, and oral mucosa, which are located on the buccal mucosa, with skin lesions on the tongue and gingiva.11,24 Clinically, OLP is classified into three major groups: Atrophic, Reticular, and Erosive. Among the three, reticular forms are the most common and asymptomatic, and atrophic or erosive forms have erythematous and ulcerative areas with severe pain and burning sensation. 11 We did not find any specific cause for this lesion, but it may occur due to viral infection or collagenous disease. 24 In contrast, drug-associated lesions are uncommon at this time. However, if medically feasible, adjusting likely connected medications, such as antihypertensives, oral hypoglycemics, and non-steroidal anti-inflammatory or psychoactive drugs, are recommended. 25 On the other hand, patients with OLP often experience periods of remission and exacerbations associated with emotional stress and psychological disorders.22,26 The chances of transmission of OLP into malignancy are less than 1%, especially found in the tongue. 27 Traditionally, many therapeutic agents such as topical corticosteroids, tetracycline mouthwash, and local anesthetics are used for the treatment of RAS. 28 Among all these, the first treatment of choice is corticosteroid. However, the therapeutic laser, an emerging modality, can be used in the management of RAS. 29 Using these types of medicines like systemic or topical corticosteroids for prolonged periods could be harmful for the oral mucosa, such as oral candidiasis or thinning of the mucosa, discomfort during application, and adrenal suppression. 30 Gastrointestinal issues, liver problems, increased blood sugar level, and increased susceptibility to infection, etc., are the side effects of using long-term conventional treatments. Moreover, it was revealed in some previous studies that conventional treatment for RAS and OLP could also cause pain relief rather than a cure and could not detect the basic or fundamental cause of the disease, or did not prevent the high recurrence rate. The efficacy of systemic or topical corticosteroids is not sufficient for treating all types of patients, specifically those who are suffering from severe or persistent RAS and OLP. That is why numerous attempts have been made to discover the most effective treatment for RAS and OLP. 31 Photobiomodulation therapy (PBMT) has been proved as a more effective way and a popular alternate option for the treatment of RAS and OLP in recent years because of its non-invasive clinical application with anti-inflammatory, potential analgesic, and immuno-modulatory effects with minimum adverse effects32–37 associated with faster healing, less pain reduction, fewer side effects and less damage to the surrounding tissue during targeted therapy. Because of its low energy production, it may also improve the healing process and shorten the healing period, relatively safe and free of clinical consequences. 38
The objectives of this systematic review were to recapitulate the current research and systematize all the studies that analyze the use of PBMT for the management of RAS and OLP, evaluate the clinical effectiveness of PBMT in reducing pain, lesion size, recurrence in patients with RAS and OLP, explore safety profiles and patient satisfaction associated with PBMT, investigate the mechanism of PBMT and its interactions with oral tissues for the provision of the therapeutic effects, and search the following questions using the Patient-Intervention-Comparison-Outcome format:
What is the Effectivity of PBMT for the management of patients with RAS and OLP in comparison with other conventional drug therapy? How can the effectiveness of these types of lasers on patients’ pain outcome, recurrence outcome, or symptoms of ulcer or healing times be measured?
Materials and Methods
A converted framework for systematic review was carried out by Arksey and O’ Malley, but it was amended through some instructions later. 39 The Preferred Reporting Items of systematic and meta-analysis (PRISMA) were followed according to the participant, interventions, controls, and outcomes (PLCO) principles which are elaborated in Table 1. In the PRISMA method, each aspect of the research paper under review like title, abstract etc. need to meet a set criteria. Our focused question is, “Does laser therapy represent more effectiveness for the management of RAS and OLP in comparison with some other conventional drug treatment?”
PRISMA 2020 Checklist
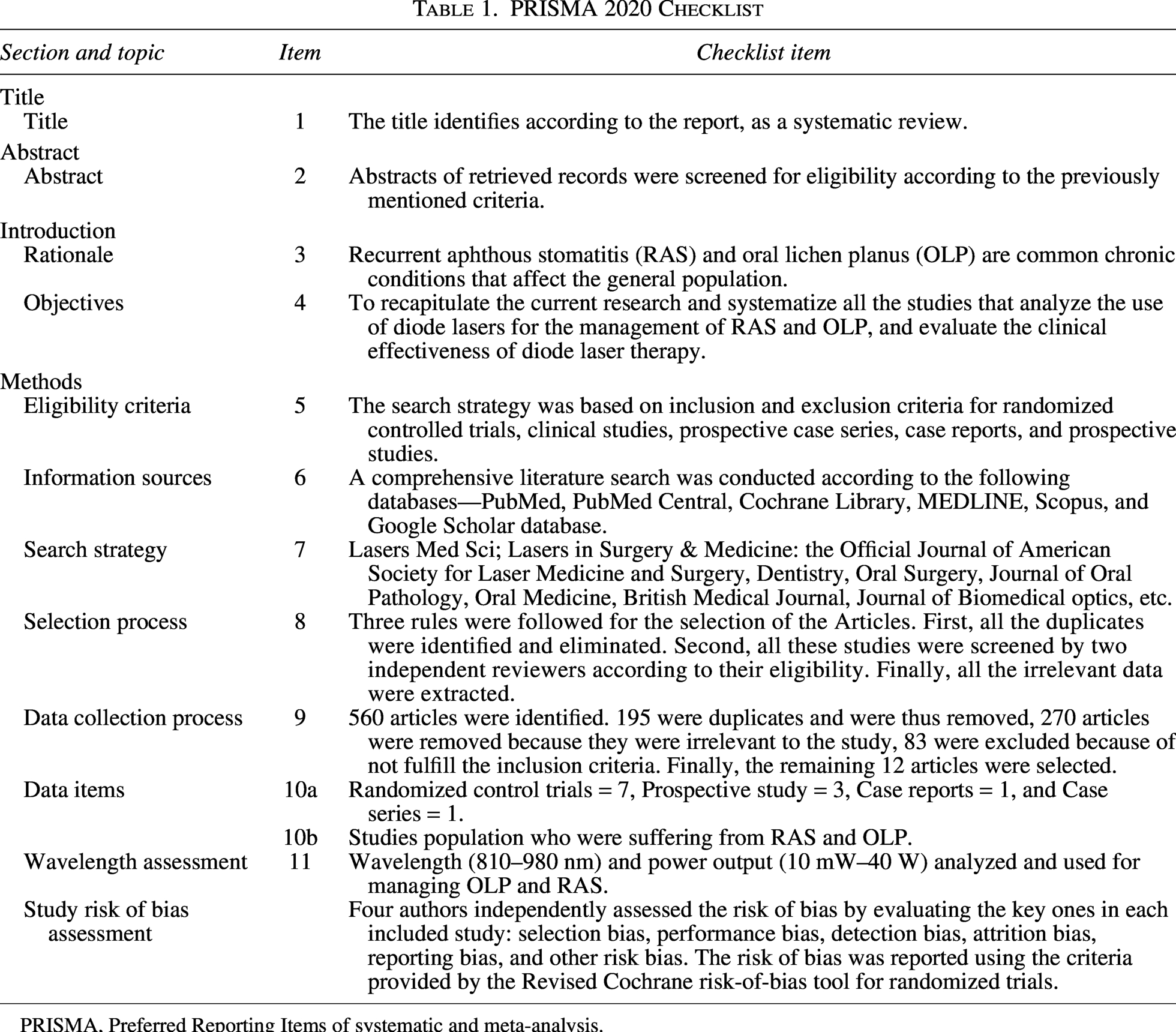
PRISMA, Preferred Reporting Items of systematic and meta-analysis.
Strategy, search and data sources
An extensive literature search was conducted according to the following databases—PubMed, PubMed Central, Cochrane Library, MEDLINE, Scopus, and finished by a random search in Google Scholar databases. All the relevant articles published in English until June 2025 using the following MeSH (Medical Subject Headings) keywords: oral lichen Planus, Photobiomodulation Therapy, Laser treatment, Topical medication, Conventional drug therapy, Recurrent Aphthous stomatitis, Management, etc. Finally, we searched all the reference lists of all the included studies, and all the records were input into the reference management software. The search strategy, along with the eligibility criteria for the systematic review article, is listed in Table 2.
Search Strategy Along with the Eligibility Criteria for the Systematic Review
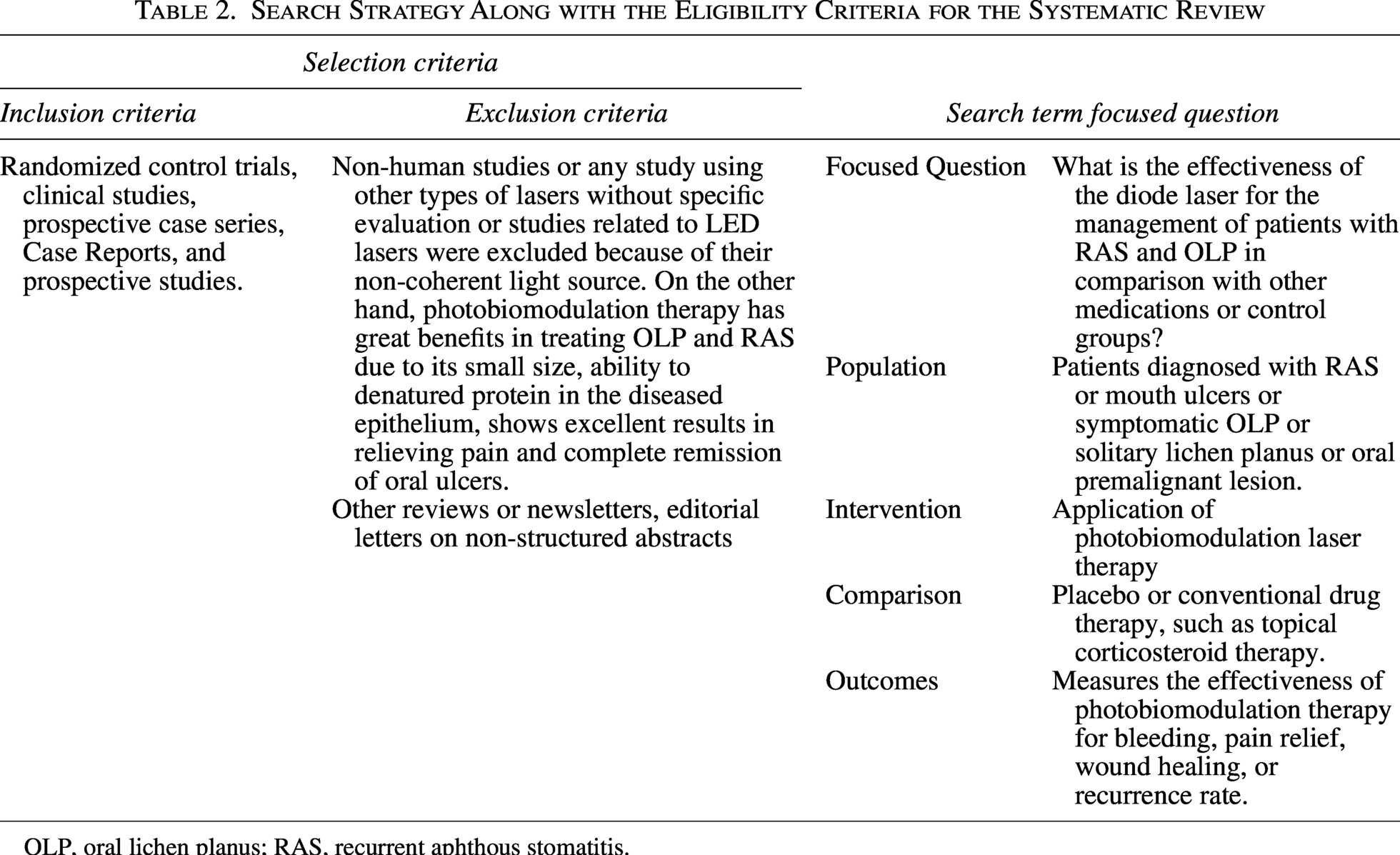
OLP, oral lichen planus; RAS, recurrent aphthous stomatitis.
Data search
Several criteria were considered for the data selection, such as articles published in English and studies where patients were diagnosed with OLP and RAS. The selected studies evaluated the effect of PBMT on pain reduction, fostering healing time with a low recurrence rate, and overall clinical improvement in patients with OLP and RAS. Also, all the observational and experimental studies, Randomized control trials, prospective case study reports, and case series revealed the uses of lasers with different wavelengths and other topical medications such as corticosteroid, Amlexanox, Clobetasol propionate, or triamcinolone acetonide used for the Rx of RAS and OLP were included for this review. Some studies, such as letters to the editor, newsletters, articles with non-structured abstracts, conference papers, review articles, or unpublished data, etc, were excluded from this study.
Selection of articles
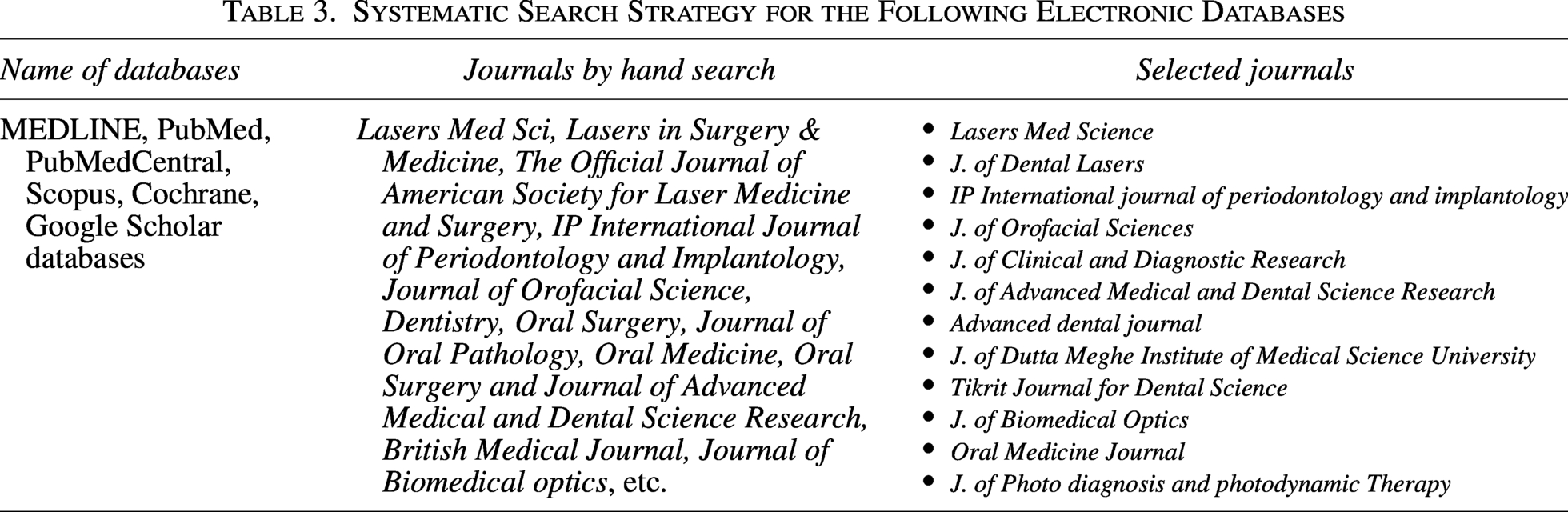
Three rules were followed for the selection of the Articles. First, all the duplicates were identified and eliminated. Second, all these studies were screened by two independent reviewers according to their eligibility. The titles, abstracts, and full texts of the selected studies were assessed by both authors. Finally, all the data that were irrelevant to the aim of the review were extracted and tabulated by one author using a data extraction sheet with the inclusion of study details, population characteristics, and intervention protocol, as well as comparison groups with outcome measures. The databases of journals and the selection of articles are listed in Table 3.
Systematic Search Strategy for the Following Electronic Databases
Risk of bias in studies
Four authors independently assessed the risk of bias by evaluating the key ones in each included study: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other risk bias. The risk of bias was reported using the criteria provided by the Revised Cochrane risk-of-bias tool for randomized trials.
Results
Study selection
Using the search strategy flowchart (Fig. 1) 560 articles were identified. Among those 195 were duplicates and were thus removed. After analyzing the abstracts and titles of the records, 270 articles were removed because they were irrelevant to the study. The remaining 95 studies were selected for full-text reading, and among all the articles, 83 records were excluded due to non-fulfillment of the inclusion criteria (Fig. 1). Finally, the remaining 12 articles were selected for this systematic review, further analysis, and data extraction.
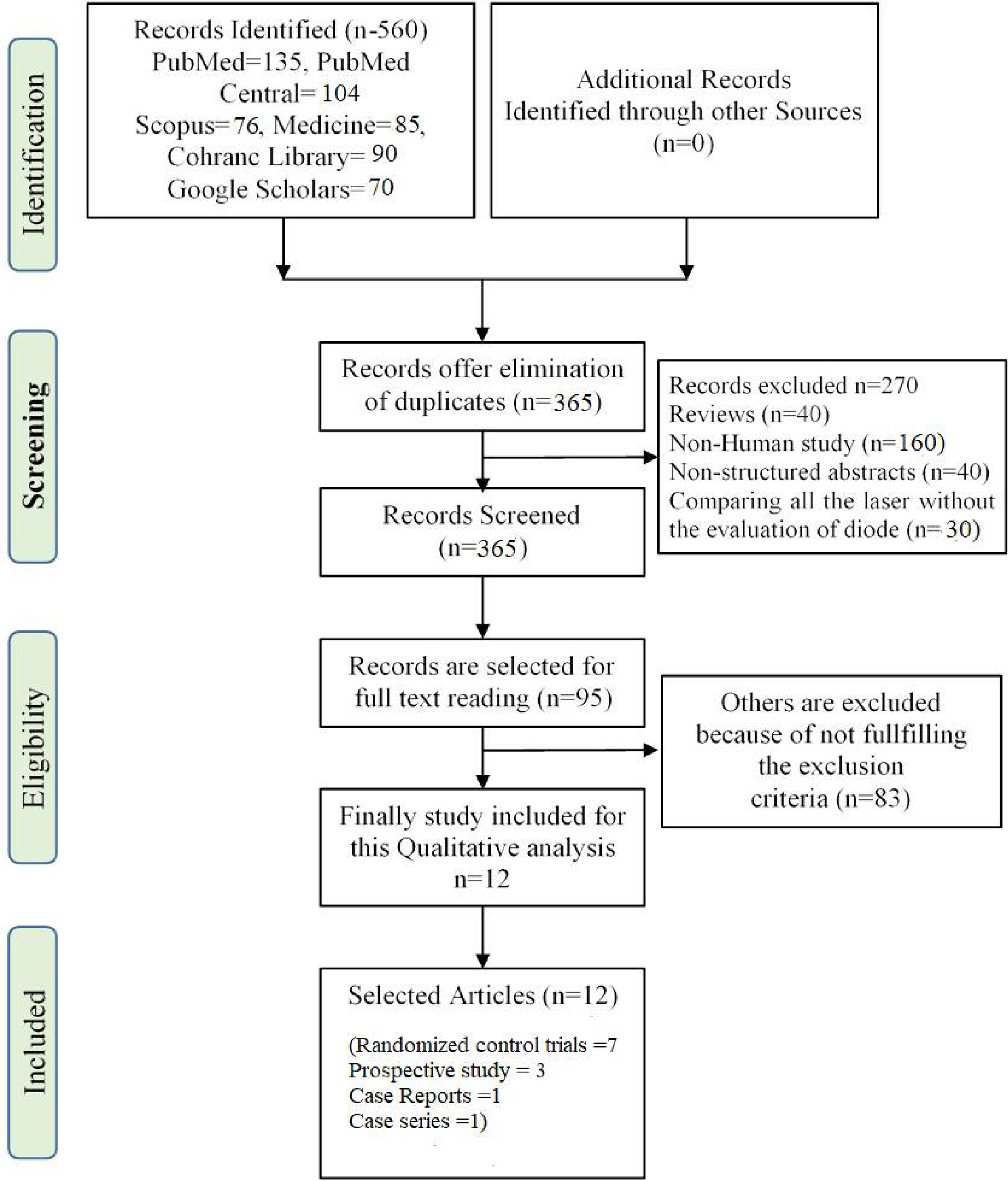
Flowchart of the PRISMA guidelines displaying the study selection process. PRISMA, Preferred Reporting Items of systematic and meta-analysis.
General characteristics of the included studies
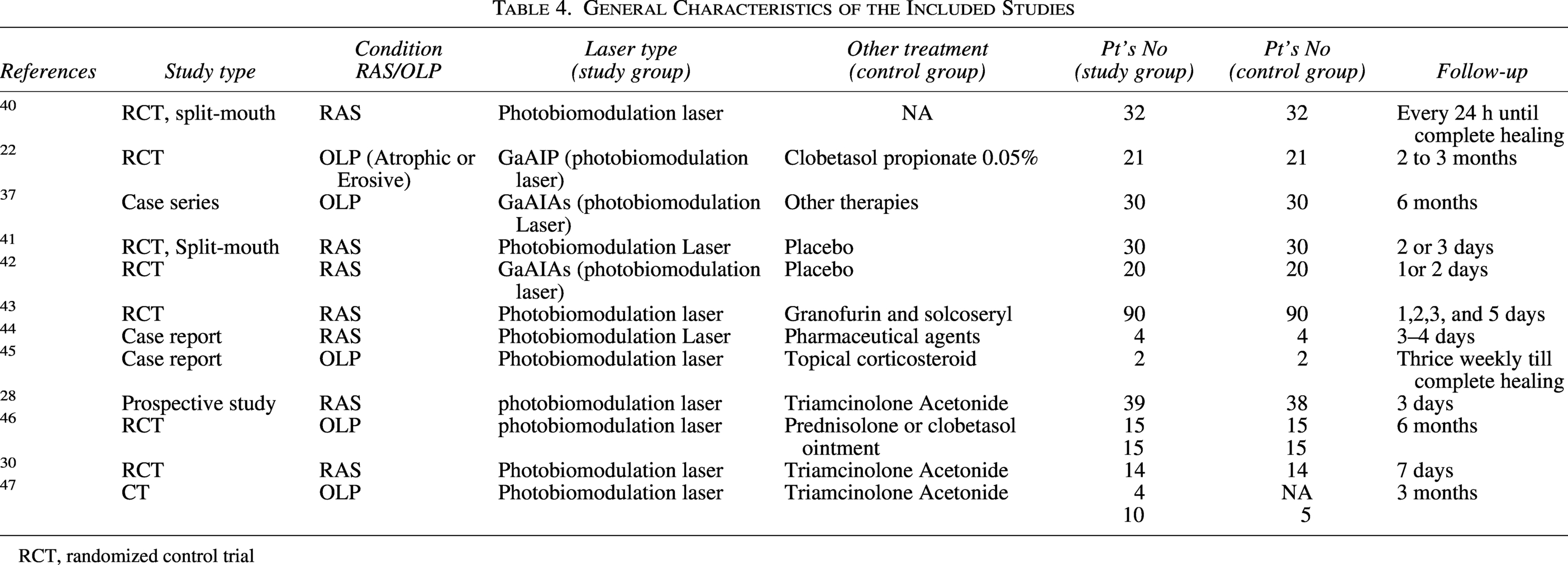
All the information, such as study design, conditions of the lesion, study sample or types of interference, and control of each study, is sketched and decorated in Table 4. The buccal mucosa, or labial mucosa, the floor of the mouth, and the tongue are the most common sites for RAS and OLP cases.24,28,30,35,37,38,46,48 The number of cases incorporated in the population group ranged between 4 and 90 for RAS and 2 and 30 for OLP. Several studies evaluated the effectiveness of photobiomodulation laser therapy in combination with corticosteroids,22,28,30,37,43,44,46 while other studies compared photobiomodulation laser therapy with two other treatment modalities.40,45 One study compared topical corticosteroid therapy with photodynamic therapy, 47 while the other compared placebo laser treatment with corticosteroid therapy.41,42 One study assessed the reticular, atrophic, and erosive scores of OLP. 22 Finally, one study showed the use of the photobiomodulation laser in pulse 40 and another in continuous mode. 42 A large number of studies revealed the use of the photobiomodulation laser in indirect contact or noncontact22,28,30,37,41,43–47 mode with approximately 2–8 mm gap between the tip of the ulcer and the photobiomodulation laser. All the studies reported follow-up ranges from 1 day to 6 months.
General Characteristics of the Included Studies
RCT, randomized control trial
Laser-related characteristics of the included studies
Lots of changes with modifications were observed in the laser parameters utilized for the selected studies. In all the 12 studies22,28,30,37,40–47 the wavelengths of the lasers ranged from 810 nm to 980 nm and power output ranged from 10 mW to 40 W. Seven studies22,37,42,43,45–47 presented the density of laser energy ranged from 1.5 to 6.3 J/cm2 and total energy was examined by only three studies30,40,41 and the exposure of all the studies ranging from 6 sec to 5 min. The surface areas exposed in only four studies, which ranged from 0.04 to 4 cm2. A total of four to 12 laser sessions were reported (Table 5).
Laser Parameters of Included Studies
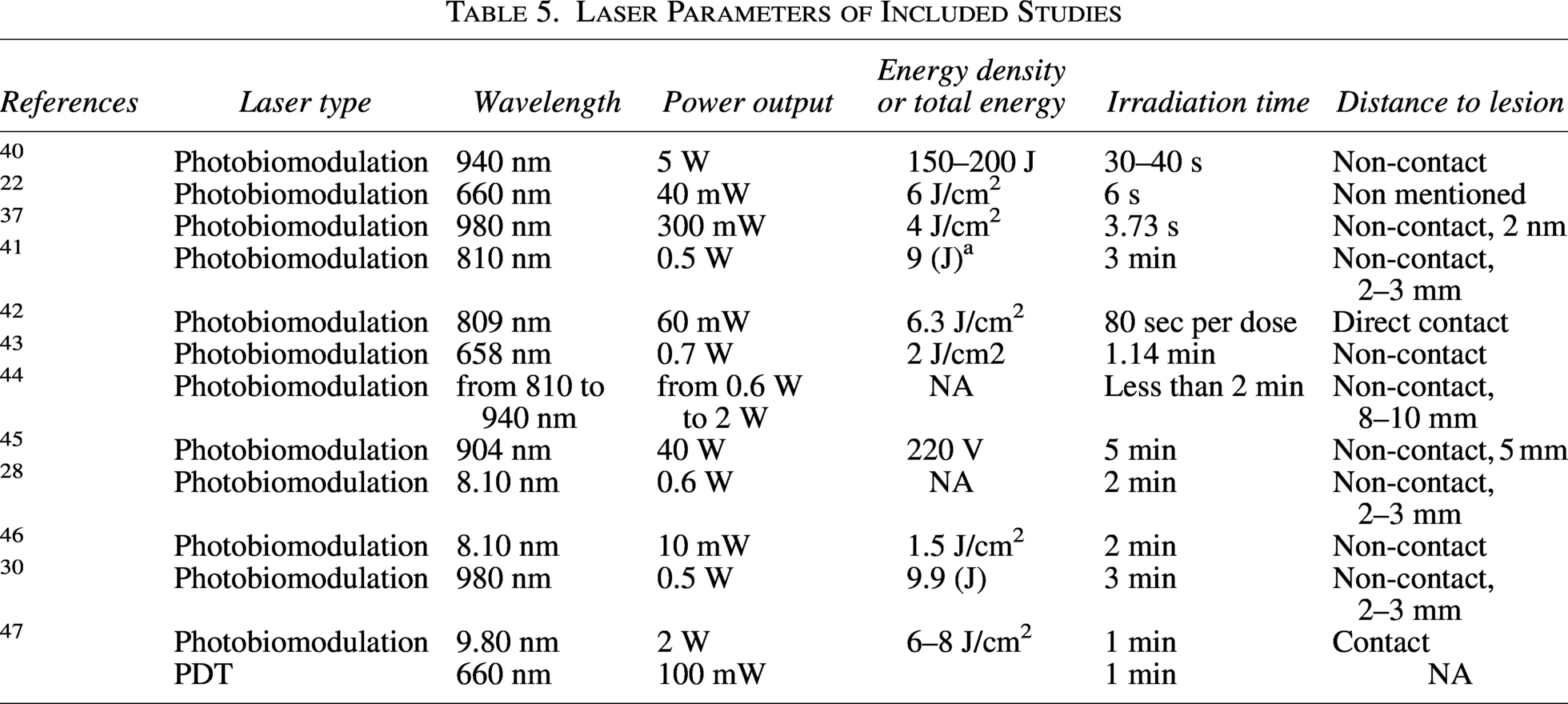
The factors that are mentioned in Table 5 include the safety parameter, high-level, non-prescriptive scientific explanation of how wavelength (810–980 nm), power output (10 mW–40 W), and irradiation time influence the types of biological effects observed in lasers commonly used for managing OLP and RAS. The interpretation of Table 5 suggests that the 810–830 nm wavelength has a lower energy range, shows less thermal effects but provides the best pain reduction, anti-inflammatory effects, and epithelial repair support as a result of relevance. On the other hand, 940–980 nm wavelength falls in the medium-/high-power range, showing strong thermal effects but is not used for gentle modulation of oral lesions. Wavelengths of 810–830 nm and mean doses of 0.8–9 J for 18–160 sec are reported as optimal.
Table 6 demonstrates the effect of the diode laser on Visual Analogue Scale (VAS) ratings, pain outcomes, effects on symptoms, healing time, and recurrence outcomes in improving patients’ quality of life. Although there are differences in healing time and VAS ratings, the study articles have shown statistically significant reductions in pain, lesion size, and recurrence rates. All the studies evaluated the effect of photobiomodulation laser on pain reduction and complete resolution with clinical improvement of the patients of both RAS and symptomatic OLP, with faster wound healing. The VAS was used to measure pain22,28,30,37,40–43,45–47 in cases of nine studies for both RAS and OLP cases with clinical signs and symptoms. Among all these records, the studies were used for clinical score scaling to assess the complete resolution or size and dimension of the lesions of all the cases of OLP. Eleven studies evaluated the recurrence rate of the lesion22,28,30,37,40,41,43–47 and one study assessed the difficulty in brushing score level. 42
Effect of Diode Laser Revealed Among the Studies
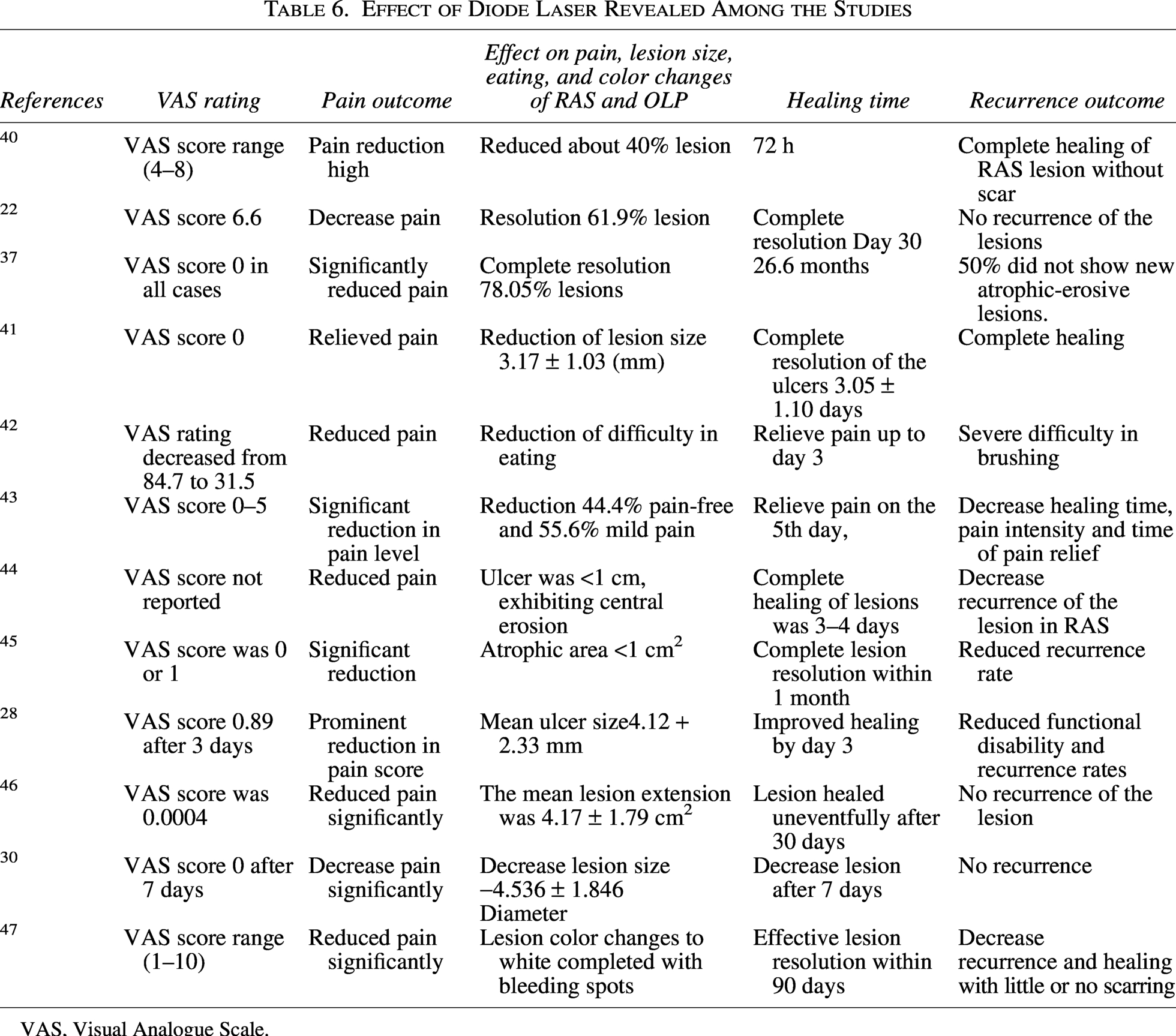
VAS, Visual Analogue Scale.
VAS rating and pain outcome
The VAS scoring system was used to assess patients’ pain reduction. Pain is usually reduced from 0 to 10 points after assessing the VAS score. There was an instant alteration in the pain scores after the diode laser application. The patient feels less pain, and on a scale of 1–10, their pain scores drop from 4 to 8, with an average drop of six points. 40 The overall mean VAS score was 6.6, indicating a significant reduction in pain within 14 days when using the diode laser22,37 assessed the patient’s pain, where the VAS score was 0 points for all measures (Table 6).
Further, pain scores were significantly reduced, which improved the patient’s quality of life. Aggarwal et al. 41 showed complete relief from pain as assessed by pain reduction based on VAS score after diode laser application. The pain score in the diode laser changed from a VAS rating from 1 to 100 changed from 56.2 to 31.5 in 2 days. 42 Comparing the photobiomodulation laser group to the corticosteroid group, the pain level analysis revealed a significant decrease in pain starting on the third day. 46 The photobiomodulation laser identified a statistically significant drop in VAS on the seventh day. 30 VAS scoring was recorded, which significantly reduced the patient’s pain. 47
Sign symptom: The 12 selected articles mentioned the symptoms of the sign, which varied in the size of the lesions and scars after photobiomodulation laser application. Approximately 40% to 78.05% of lesions were reduced, and the resolution was observed under the influence of a photobiomodulation laser.22,37,40 Aggarwal et al. 41 expressed a sense of photobiomodulation laser reduction of lesion size of 3.17 ± 1.03 (mm). The mean ulcer size was 4.12 + 2.33 mm; 28 the lesion color changed to white, completed with bleeding spots due to the diode laser effect. 47
The analysis of seven studies was combined for forest plot analysis of standard mean differences of VAS pain score between the two groups, namely photobiomodulation laser therapy vs. Corticosteroids. The overall VAS score is the mean of all items answered with values between 0 and 10. It was shown that corticosteroids were superior to photobiomodulation in terms of VAS scores after treatment. The combined studies were homogeneous. The VAS score was tested for reliability with Laser therapy and conventional drug therapy. The VAS score was tested for reliability with photobiomodulation laser and conventional drug therapy. The score is a useful tool for comparative clinical studies, addressing the outcome after different methods of treatment (Fig. 2).
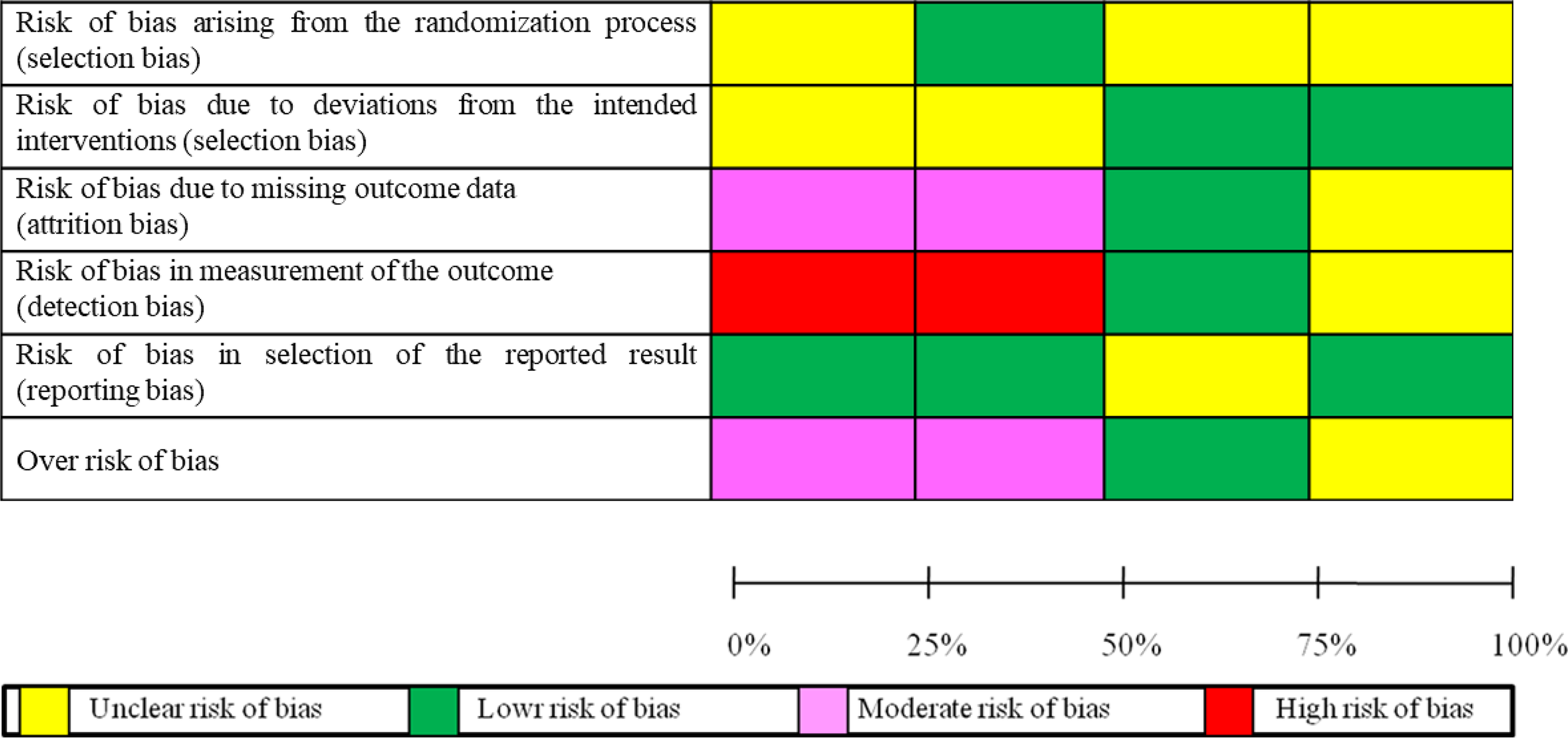
Schematic diagram summarizing the risk assessment of bias.
Healing time and recurrence outcome
Healing and recurrence were also evaluated by healing time in selected articles after laser photobiomodulation application. Hazeem et al. 40 reported that the photobiomodulation laser represents complete healing of the Aphthous Ulcers without scarring 72 h after use. There was a highly significant reduction in lesion duration in irradiated ulcers. Other articles have also shown low recurrence rates and no recurrence of lesions after photobiomodulation laser treatment. The reduction of the size of the lesion is a sign of a successful healing process. RAS has been successfully controlled after the use of photobiomodulation laser and has shown varying degrees of success. All patients’ ulcers were successfully treated and managed within 3 days. 43 The majority of recurring cases were associated with pain. In all the integrated studies, the patients treated with diode laser had lower pain scores and decreased recurrence and period of aphthous ulcer healing. 30
Risk of bias
The risk of bias for the study is presented in Figure 3. It shows unclear and low risk for selection bias and reporting bias, while attrition bias and over-risk bias showed moderate risk. On the other hand, detection bias showed a level of risk that was often high. The valuation was commenced by two independent reviewers, and the risk of bias findings for each area were almost identical. Nevertheless, the studies had quantified the practice of randomization, but they did not offer any explanation of the procedure. Maximum revisions had “some concerns “in the allocation bias field. There was no missing data in any of the included studies. Hence, none of the comprised revisions could be measured to be of great superiority.
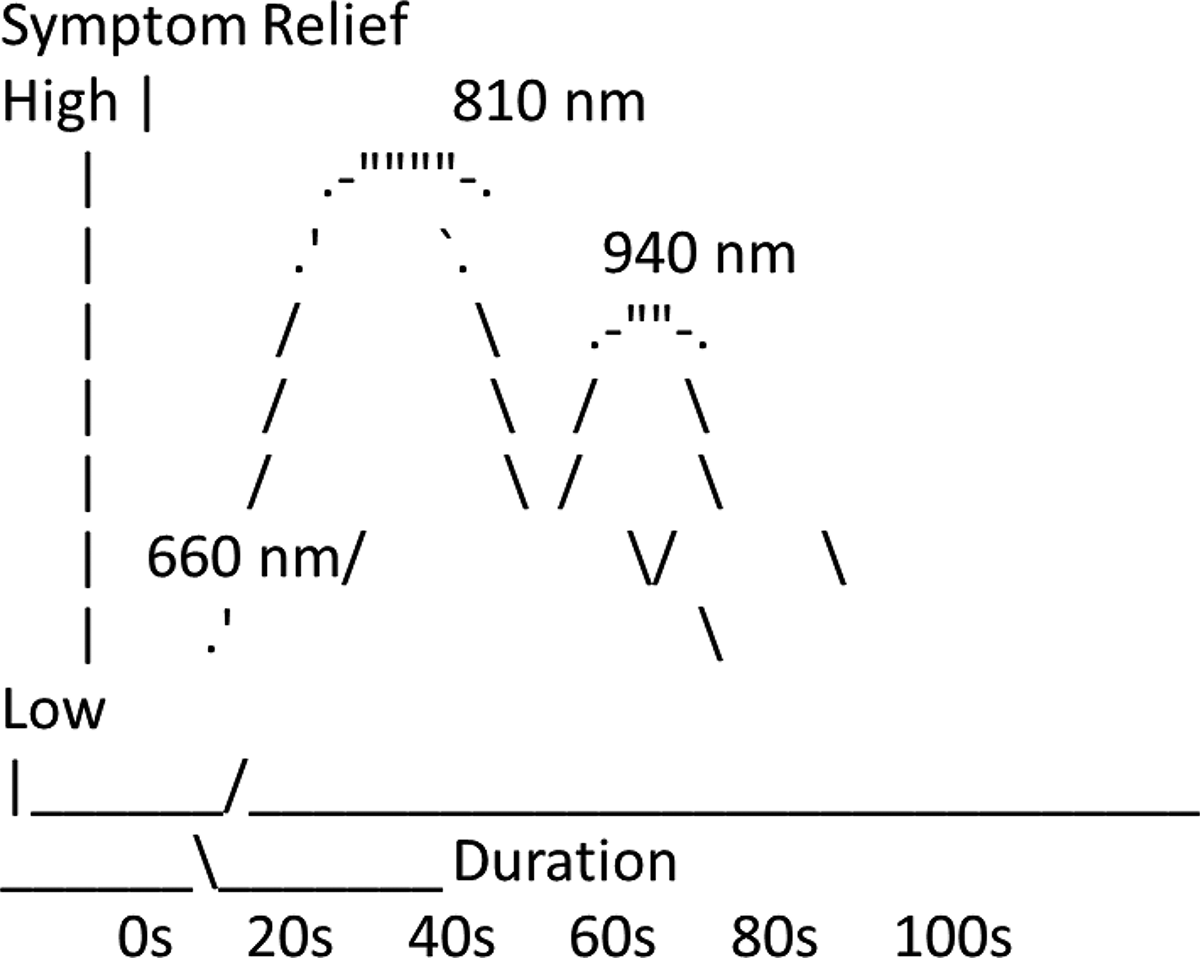
The typical level of symptom improvement (pain/inflammation reduction) as duration increases for common diode wavelengths.
In this study, green color indicates low risk of bias, pink color indicates moderate risk of bias, and red color indicates low risk of bias, as highlighted in Figure 3. Risk of bias is generally moderate to high across both OLP and RAS trials due to small samples, inadequate blinding, and short follow-up. Efficacy evidence is strongest for topical corticosteroids in both conditions, though they provide symptom control rather than a cure. Therapy shows benefits for severe or refractory disease but carries more adverse effects and is studied in small or high-bias trials.
Moderate levels of detection and selection bias in the studies reduce the credibility of the reported results for both OLP and RAS. In a GRADE framework, this results in low to moderate confidence in the current evidence base. Stronger conclusions would require more rigorous, well-controlled, adequately conducted clinical trials. The overall certainty of the evidence is low to moderate (Table 7).
Interpretation of Risk of Bias

Clinically interpretive summary
Photobiomodulation lasers (660–685 nm) are best for pain relief and inflammation, with no burning/thermal damage, and are safe for frequent sessions, but require longer exposure times (Fig 4).
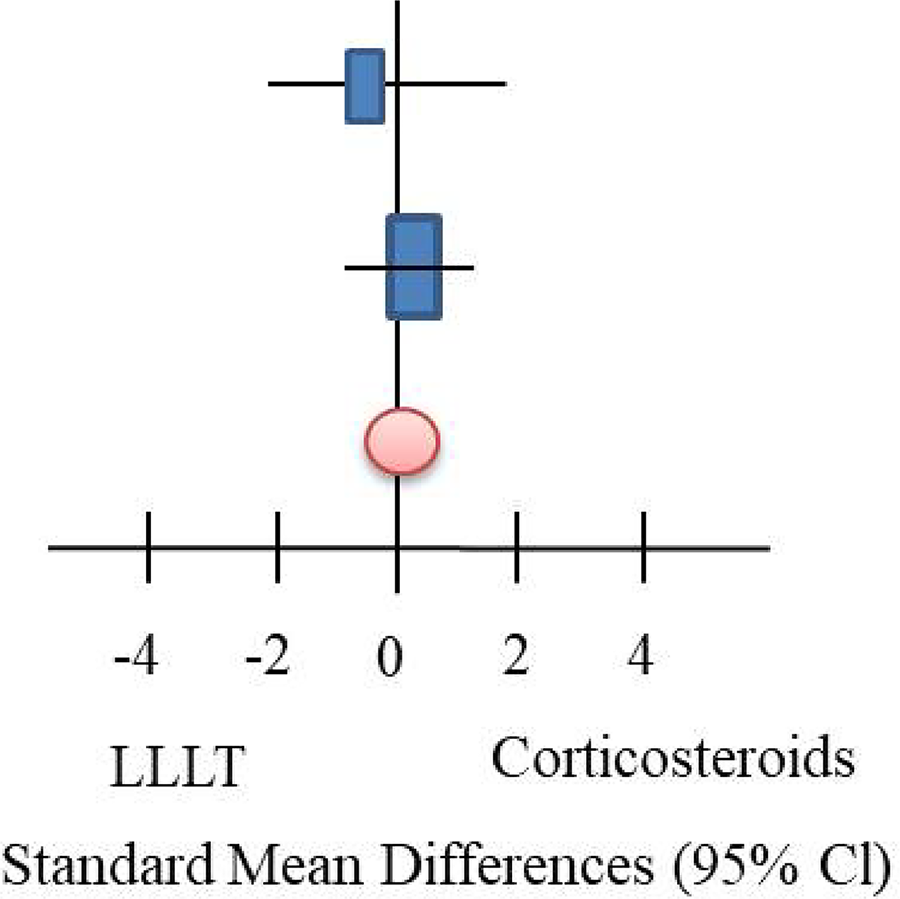
Shows forest plot of standard mean differences of clinical severity between the two groups (photobiomodulation vs. corticosteroids) with 95% confidence interval (heterogeneity chi2 = 0.47, df = 1, I2 = 0%).
Mid-wavelength diodes (810–980 nm) provide strong symptom relief, reduce lesion size, and shorter exposure times, but heat must be managed (pulsed mode recommended above 940 nm) (Fig. 4).
Interpretation
660 nm (LLLT): Needs longer exposure, excellent anti-inflammatory effect. 810 nm: Balanced effect; good improvement with moderate duration. 940–980 nm: Require shorter duration but produce quick, strong symptom relief due to thermal-assisted action.
Discussion
The outcome of this systematic review was analyzed to confirm the therapeutic efficacy of PBMT for the management of OLP and RAS with particular focus on pain reduction, vas ratings, recurrence outcomes, and healing time. This review article also emphasizes the significant potential of diode laser therapy, specifically photobiomodulation laser therapy, in the management of RAS and OLP, which are prolonged, aggressive infections associated with a comprehensive destructive manipulation on the patient’s life. Diverse nature of research in progress from the size and period of the wound, follow-up time, an intractable or fresh case of OLP, type of laser, the wavelength of photobiomodulation laser, irradiation time of PBMT, and distance to the lesion. 48 This work shows 940–980 nm wavelength falls in the medium/high power range, showing strong thermal effects but is not used for gentle modulation of oral lesions. Wavelengths of 810–830 nm and mean doses of 0.8–9 J for 18–160 sec are reported as optimal. Taylor et al. (2020) exhibited therapy parameters were effective for reducing levels of pain and inflammation at wavelengths of 670–830 nm, dosages of 1–20 J/cm2, output powers of 10–100 mW, and irradiation durations of 10 sec to 2.7 min, which is almost similar to our judgments. 49
On the Other hand, 810–830 nm wavelength has a lower energy range, shows less thermal effects but provides the best pain reduction, anti-inflammatory effects, and epithelial repair support as a result of relevance because of the 810 nm wavelength offers precise cutting and coagulation (when used in high power) or biostimulation (when used in lower power) with extremely thermal small zones of necrosis in surrounding tissues. This prevents unnecessary damage to healthy mucosa, which is critical for sensitive lesions such as OLP and RAS. Moreover, RAS and OLP generally present as Superficial and small or medium-sized lesions. So, care should be taken to prevent the surrounding tissue and deeper tissues.
Based on recent studies, the 810 nm PBMT is often considered more effective than 940 nm because of its superior ability to reduce inflammation during the healing process. Ebrahimi et al. revealed some experimental studies comparing istrogenic oral ulcers in rabbits exhibited that both 810 nm and 940 nm lasers reduce inflammation, but 810 nm irradiation significantly decreased the severity of inflammation in oral wounds created in buccal mucosa of rabbits in a time-dependent manner. 50 810 nm PBMT also has strong biomodulatory effects, which can promote faster granulation tissue formation, improved wound closure, and faster re-epithelization in comparison with 910 nm diode laser. In 2021, Rezaei F et al. mentioned that at lower and non-ablative dose 810 PBMT has been shown to increase the viability of gingival fibroblast where the same dose 940 nm has shown an inhibitory effect in a central setting. 51 Talebi et al. suggested in their study that 810 nm laser could be better than a 940 nm laser in nerve repair. 52 So, finally, it is established that 940 or 980 nm lasers are also effective, but the 810 nm wavelength is often highlighted for its optimal balance between its ability to manage, deep penetration, tissue absorption, and thermal safety.
In our study, the findings have shown that a single session of photobiomodulation laser irradiation can be used to produce an immediate, significant, dramatic, and long-lasting analgesic impact on RAS lesions. The VAS score dropped from 4 to 8, including a mean VAS score of 6.6, which indicated a significant reduction of pain within 14 days. The analysis of seven studies was combined for forest plot analysis of the standard mean differences of VAS pain score between the two groups. (LLLT vs. Corticosteroids). The overall VAS score is the mean of all items answered with values between 0 and 10. It was shown that corticosteroids were superior to LLLT in terms of VAS scores after treatment. A similar study was conducted by Aggarwal (2017), where he observed a mean reduction in VAS score from 7.8 to 1.4 within 2 days. 53 Another study was done by Bello-Silva, who showed substantial VAS score reduction in OLP lesions from 6.5 to 2.0 after just one larger lesion, 54 and Sattayut et al. revealed that laser therapy causes superior pain relief compared to corticosteroids in OLP management.55,56 Similarly, this type of outcome has been shown in previously conducted studies.28,30,41–43 A diode laser was utilized with wavelengths ranging from 8.10 nm to 980 nm and power output between 10 mW and 40 W. The wavelength of the photobiomodulation laser made it highly effective as a bio-stimulation device, while its output parameters enabled it to function efficiently as a powerful thermal laser. 40
The included studies revealed that photobiomodulation laser therapy is more effective than conventional treatments, such as corticosteroids, in reducing pain, improving lesion healing, and minimizing recurrence rates in both RAS and OLP. The primary outcomes of this study assessed pain reduction and lesion size, demonstrating marked improvements in the laser-treated groups compared to controls. Pain reduction, a critical factor in improving patient satisfaction and compliance, was consistently measured using the VAS. The reported significant reductions in VAS scores post-laser therapy align with the known analgesic and anti-inflammatory effects of the photobiomodulation laser. In this study, the VAS scoring system was used to evaluate patients’ pain reduction. Pain is usually reduced from 0 to 10 points after assessing the VAS score. Numerous clinical trials report immediate pain relief in patients treated with PBMT for aphthous ulcers. A similar study was done by Aggarwal et al., 41 where 60 patients experienced a significant reduction in pain immediately after laser application, with the effect lasting for several days. The most similar result was found in Pakfetrat et al.’s 57 research. The researchers have demonstrated that at the end of the follow-up period, 8 patients reported being pain-free, while 2 patients showed a reduction in their VAS score from 3 to 1. There was no significant difference between the two groups regarding their mean VAS and lesion diameter. 58 VAS score was 2.5 points after 24 h and 0 points after 7 days of surgery. 59
This review article provides information on the healing time for the recurrence of lesions of oral lichen planus after PBMT. The broad variation in reported recurrence rates may be attributed to differences in follow-up durations, laser application techniques, and all of which result in varying levels of cellular destruction. 60 Most of the lasers showed a higher percentage of patients with inferior pain scores and reduced ulcer size. 61 A PBMT can effectively reduce pain and achieve a complete regression of the lesion within 4 days. 62 Similar types of investigations were done by Khademi et al., 63 where they reported that PBMT-treated RAS lesions healed 50% faster than untreated lesions, and Yilmaz et al. reported that healing in erosive OLP was significantly faster with PBMT than with topical triamcinolone. 64 Mücke et al. 65 reported a recurrence frequency of 38.2% for lichen Planus, and lasers have implications for managing patients with OLP and provide conclusions regarding the recurrence rate of OLP. Dalirsani and Seyyedi 66 expressed that lasers could be employed for OLP lesions; however, some degrees of recurrence may occur. PBMT has demonstrated efficacy in reducing the size and severity of erosive lesions in patients with OLP. A clinical trial by Al-Mohaya et al. 67 showed that PBMT led to quicker resolution of OLP lesions compared to corticosteroid treatment. A clinical study by Aras et al. 68 demonstrated that PBMT significantly reduced the healing time of aphthous ulcers compared to conventional therapies. Ulcers treated with the PBMT healed in 3–5 days, while those treated with topical agents took 7–10 days to heal. The recurrence rate of the lesions was very low when treated at an early stage, and the effectiveness of laser in managing OLP where decreased recurrence rates.38,69,70
It can be determined based on the outcomes of the existing study and detailed review of the remaining works that the PBMT laser can decrease the healing time, pain intensity, size, and recurrence of the lesion in RAS, and can be measured as the most suitable treatment modality for RAS. The initial cost of PBMT is high because of its expensive and highly modern equipment, but in the long-term cases, it could be cost-effective for chronic conditions because of its limited sessions or one-time session, according to the nature and severity of the diseases. It could also lead to promoting healing and longer remission associated with minimal invasive and painless treatment and fewer side effects, which may reduce the overall treatment cost. On the other hand, corticosteroids are less expensive than diode laser initially, but in the long term, they could increase the total treatment cost of the disease because of fewer side effects such as immunosuppression, adrenal suppression, skin thinning, osteoporosis, or high recurrence rate, which may need additional medical costs for managing these conditions. The accessibility of PBMT can be limited, particularly in rural areas, due to low resources and a lack of trained professionals. On the other hand, corticosteroids are more easily accessible and available in all the pharmacies, clinics, and even in rural areas.
Conclusions
This systematic review demonstrates that PBMT is one of the most effective treatment options for providing pain relief, faster wound healing, with the improvement of patient comfort and satisfaction, resulting in more favorable results when compared to placebo, other conventional treatments, or no therapy for the management of RAS and OLP. Photobiomodulation laser therapy could also offer better long-term cost-effective treatment with fewer side effects for certain chronic conditions. But its limited accessibility can be a barrier. On the other hand, corticosteroids are more accessible and affordable initially, but in the long term, they may increase the treatment cost due to side effects. In conclusion, we could say that more research is needed about the treatment modality of photobiomodulation Laser therapy because of its promising benefits, intensive pain relief, and patient satisfaction. RAS and OLP symptoms and lesion severity have been reported to improve over time with PMBT laser therapy. Specifying optimal PBMT laser parameters, such as wavelength, power output, mode of operation, and exposure duration, has been shown to achieve the most satisfying outcomes. Highlighting the real-world factors would provide a more comprehensive understanding of the diode laser’s role in the management of OLP and RAS and support more informed clinical decision-making.
660 nm (PBMT): Needs longer exposure, excellent anti-inflammatory effect. 810 nm: Balanced effect; good improvement with moderate duration. 940–980 nm: Requires shorter duration but produces quick, strong symptom relief due to thermal-assisted action.
Authors’ Contributions
Conceptualization, Tasnia Habib and S.M. Shahinul Islam; methodology, Tasnia Habib and Tahsinul Haque; software, Fatema Akhter; validation, Tahsinul Haque, S.M. Shahinul Islam, Mohammed Afroz, Manna Haque Akhanda and Fatema Akhter; formal analysis, Tasnia Habib; investigation, S.M. Shahinul Islam, Fatema Akhter; resources, Tasnia Habib, Fatema Akhter, S.M. Shahinul Haque; data curation, Tasnia Habib, Mohammed Afroz; writing—original draft preparation, Tasnia Habib and S.M. Shahinul Islam; writing—review and editing, S.M. Shahinul Islam, Mohammed Afroz, Tahsinul Haque, Fatema Akhter, Manna Haque Akhanda; project administration, S.M. Shahinul Islam; funding acquisition, S.M. Shahinul Islam. All authors have read and agreed to the published version of the article.
Footnotes
Acknowledgments
The authors would like to express their appreciation to all the researchers and clinicians whose academic work formed the construction of this review. Their invaluable contributions to the field of diode laser therapy have provided insights that guided this work. The authors are deeply grateful to their academic advisors and colleagues for their contributions, constructive feedback, and encouragement throughout the research process. This review was inspired by a commitment to advancing clinical practice and improving patient care in managing oral mucosal conditions. The authors hope this work serves as a stepping stone for future research in this area.
Data Availability Statement
The data presented in this study are contained within the article.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This research received no external funding.