
Abstract
Background
Breast cancer remains a major public health concern, where late-stage diagnosis is common. Breast self-examination (BSE) is a low-cost strategy for early detection; however, its practice is suboptimal.
Objective
To assess the practice of BSE and associated barriers among female diploma students at the State University of Zanzibar (SUZA).
Methods
A cross-sectional study was conducted among 300 female students from the School of Health and Medical Sciences (SHMS) and the Institute of Tourism (IT). Participants were selected using simple random sampling. Data were collected in a structured, pre-tested, self-administered questionnaire. BSE practice was categorized as adequate or inadequate based on a composite score. Descriptive statistics, chi-square (χ²) tests, and multivariable logistic regression were performed to identify factors independently associated with BSE practice.
Results
Overall, 59.7% of participants demonstrated inadequate BSE practice. In multivariable analysis, students from SHMS were more likely to practice BSE compared to IT students (adjusted odds ratio [AOR] = 3.20, 95% confidence interval [CI]: 1.90-5.40, P < .001). Having a family history of breast cancer (AOR = 2.60, 95% CI: 1.30-5.20, P = .007) and prior exposure to breast disease (AOR = 3.10, 95% CI: 1.75-5.48, P < .001) were also significantly associated with BSE practice. Age and marital status were not significantly associated. Knowledge-related barriers were more pronounced among non-health students.
Conclusions
Despite moderate awareness, BSE practice remains inadequate among university students. Educational exposure, personal risk factors, and prior clinical experience significantly influence practice. Targeted, skill-based interventions are needed to improve correct and consistent BSE behavior across all academic disciplines.
Recommendations
Targeted, hands-on educational interventions focusing on correct technique and routine practice should be implemented across all faculties. University-wide programs could strengthen early detection behaviors and reduce breast cancer morbidity.
Keywords
Introduction
Breast cancer is the most common malignancy among women worldwide, accounting for an estimated 2.3 million new cases and 685,000 deaths in 2020 alone.1-5 Despite advances in early detection and treatment, mortality remains disproportionately high in low- and middle-income countries, particularly in sub-Saharan Africa, where more than 70% of cases are diagnosed at advanced stages.6, 7 Late presentation and limited healthcare resources contribute to poor survival rates, making early detection strategies critical in these regions. 8
In Tanzania, breast cancer is the second most common cancer, representing 14.4% of new cancers, and is the second leading cause of cancer mortality among women.9, 10 Breast cancer represents a growing public health concern, with Zanzibar reflecting similar trends. The availability of mammography and other advanced screening modalities is limited, particularly outside urban centers, resulting in delayed diagnosis and treatment. Socioeconomic, infrastructural, and geographic constraints further reduce access to conventional screening, underscoring the need for feasible, community-based alternatives.11, 12
Breast self-examination (BSE) is a low-cost, non-invasive screening method that enables women to identify changes in breast tissue, such as lumps, discharge, or alterations in size or shape.13, 14 While BSE does not replace mammography, it serves as an accessible and practical early detection strategy in resource-limited settings, helping to bridge gaps in breast health awareness and prompt timely clinical consultation.15, 16
University students represent a critical demographic for health education and preventive interventions. As future professionals and community influencers, they are well-positioned to disseminate knowledge and adopt healthy behaviors. 17 Assessing BSE knowledge and practices among this population provides insights into both current awareness and potential areas for targeted educational initiatives. 18
Despite its benefits, evidence suggests that many students and teachers encounter barriers to regular and effective BSE. These include limited procedural knowledge, misconceptions about breast cancer risk, cultural or religious norms, psychological discomfort, and low perceived susceptibility. Such obstacles can significantly undermine the impact of BSE promotion efforts.19, 20
This study, therefore, aims to assess the practices and barriers to BSE among female students at the State University of Zanzibar (SUZA). Understanding these factors is essential for designing tailored interventions that improve early detection, promote reproductive health literacy, and ultimately reduce breast cancer morbidity and mortality within this population.
Objectives
To determine the level of BSE practice among female students at the SUZA.
To determine the barriers to BSE practice among female students at the SUZA.
Methods
Study Design
A cross-sectional, comparative, descriptive study using a quantitative approach was conducted to assess and compare knowledge of breast cancer and BSE among female students at the SUZA. This design was appropriate as both independent and dependent variables were measured simultaneously, allowing assessment of associations between academic background and BSE knowledge and practices at a single point in time.
Study Area and Population
The study was conducted at SUZA’s Tunguu and Mbweni campuses, which host the School of Health and Medical Sciences (SHMS) and the School of Tourism, respectively. Female students enrolled in these schools were invited to participate. Inclusion criteria were female students aged 18 years or older, currently enrolled at the selected campuses. Male students and students from other campuses were excluded.
Sample Size and Sampling Technique
The minimum sample size was calculated using Kish and Leslie’s formula for cross-sectional studies
21
:

where Z = 1.96 (95% confidence interval), P = .5, q = 1 − pq = 1 – pq = 1 − p, and e = 0.05 e = 0.05 e = 0.05. The estimated sample size was 384; however, due to logistical constraints, 300 participants were recruited. A simple random sampling technique was used to select participants from each school and year of study to ensure representativeness. The selection of SHMS and the Institute of Tourism (IT) as the two comparison groups was theoretically motivated and methodologically deliberate. The primary research objective was to determine whether exposure to health-related academic training influences BSE knowledge and practice. SHMS students (nursing diploma) represent a group with structured, curriculum-based health education, while IT students (diploma in hospitality and tourism management) represent an equivalent academic cohort without such exposure. Both groups are drawn from the same institution, study at the same academic level (diploma), and share a broadly comparable socio-demographic and geographic profile, factors that minimize confounding and allow the effect of health curriculum to be examined with greater specificity.
Study Variables
Dependent variables: BSE practice and barriers to BSE practice.
Independent variables: Age, year of study, school attended, family history of breast cancer, place of upbringing, fear of detecting cancer, embarrassment, and source of breast health information.
Data Collection
Data were collected using a structured, self-administered questionnaire adapted from previously validated knowledge, attitude, and practice (KAP) instruments and modified for the local context. The questionnaire elicited information on socio-demographic characteristics, knowledge of breast cancer, BSE practices, and perceived barriers.
BSE practice was assessed across five dimensions: Awareness of BSE, knowledge of the correct technique (three fingers and palm), knowledge of what to examine (changes in size, shape, or discharge), frequency of practice (monthly), and duration (≥3 minutes). Each item was scored dichotomously (1 = correct, 0 = incorrect or unknown), yielding a composite score ranging from 0 to 5. Consistent with standard KAP scoring conventions, participants scoring ≥3 (≥ 60%) were classified as demonstrating adequate BSE practice, and those scoring <3 as demonstrating inadequate practice. Before data collection, verbal and written informed consent were obtained from all participants.
Pre-test
The questionnaire was pre-tested among 20 female students with similar characteristics at the Zanzibar School of Health. Based on the results, minor modifications were made to improve clarity and comprehension before the main study.
Ethical Considerations
Permission was secured from the SHMS, SUZA, and the IT. Participants were informed about the study objectives, and confidentiality, anonymity, and voluntary participation were emphasized. Signed informed consent was obtained from all respondents. Ethical approval was granted by the Zanzibar Health Research Institute (Ref No. ZAHREC/05/ST/March/2023/29).
Data Processing and Analysis
Completed questionnaires were checked for completeness, coded, and entered into epidemiological information software and the Statistical Package for the Social Sciences version 26 for analysis. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to summarize socio-demographic characteristics, BSE knowledge, practices, and barriers. Group comparisons were performed using chi-square (χ²) tests and odds ratios (ORs) for categorical variables. Median values were reported for skewed data. Data were presented in tables, graphs, and narrative form. Multivariable logistic regression was performed to identify factors independently associated with BSE practice, adjusting for age, faculty, marital status, family history of breast cancer, and prior breast disease exposure.
Results
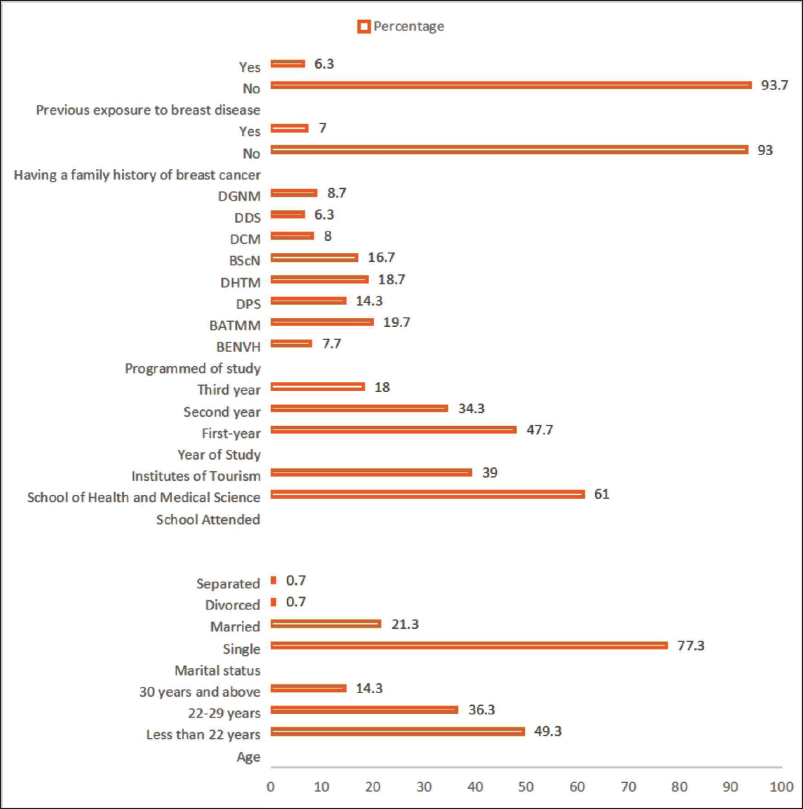
The sample primarily consists of single young women (85.6% under 30) in health (61%) or tourism (39%) programs, allowing meaningful comparison between health-related and non-health disciplines. Most are single (77.3%) and are first-year students with limited personal or family history of breast disease (under 7%), reflecting a population with low clinical exposure despite their academic focus (Figure 1).
Socio-demographic Profile of Students from the SHMS and the IT SUZA (N = 300).
Health sciences students show significantly higher awareness (OR = 2.56) and technical competence in BSE than tourism students. However, both groups lack consistent monthly practice. While academic background improves knowledge and accuracy, it does not bridge the gap to regular preventive behavior, highlighting a need for skill-oriented, university-wide education (Table 1).
Cross-tabulation of Practices of BSE by School Attended (N = 300).

Both groups exhibited suboptimal BSE practices (~72%), with no significant difference between health and tourism students (P = .643). Academic registration did not translate into behavior, highlighting a gap between theory and practice. The study recommends university-wide, practical training rather than purely theoretical instruction to enhance preventive health outcomes (Table 2).
Cross-tabulation of BSE Practices by School Among University Students (N = 300).

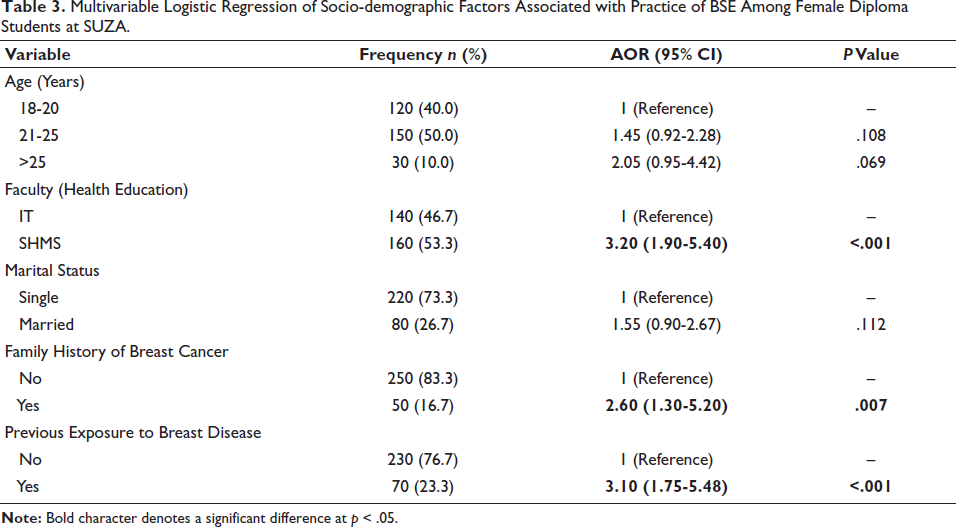
A multivariable logistic regression analysis showed that students from the SHMS were significantly more likely to practice BSE compared to those from the IT (adjusted odds ratio [AOR] = 3.20, 95% confidence interval [CI]: 1.90-5.40, P < .001). Additionally, having a family history of breast cancer (AOR = 2.60, 95% CI: 1.30-5.20, P = .007) and previous exposure to breast disease (AOR = 3.10, 95% CI: 1.75-5.48, P < .001) were independently associated with a higher likelihood of practicing BSE (Table 3).
Multivariable Logistic Regression of Socio-demographic Factors Associated with Practice of BSE Among Female Diploma Students at SUZA.
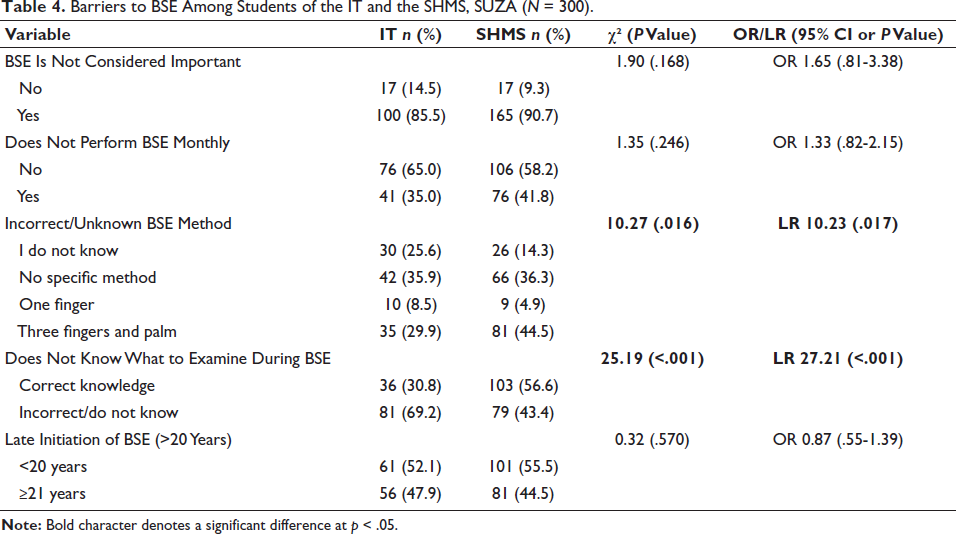
Tourism students face significantly greater knowledge barriers, specifically regarding correct BSE methods (70.1%) and what to examine (69.2%), compared to health students. However, both groups share similar attitudes and timing issues. This suggests that while motivation exists, practical procedural gaps, especially in non-health disciplines, require targeted, technical education (Table 4).
Barriers to BSE Among Students of the IT and the SHMS, SUZA (N = 300).
Discussion
The socio-demographic and academic characteristics of the study participants were as follows: The cohort was predominantly young adults, with nearly half aged below 22 years (49.3%) and over one-third aged 22-29 years (36.3%), reflecting the typical university-age population. Almost three-quarters of the participants were single (77.3%), consistent with the age distribution, whereas married, divorced, and separated students constituted a small minority. These results are aligned with other studies conducted in Tanzania 10 and another that involved three Arab countries. 22
Academically, the majority were enrolled in the SHMS (61.0%), with the remainder from the IT (39.0%), providing a meaningful contrast between health-related and non-health disciplines. Nearly half were first-year students (47.7%), with fewer second- and third-year students, which may influence exposure to health education and knowledge of BSE. Participants were drawn from a diverse set of programs, with the Bachelor of Arts in Tourism and Marketing Management, the Diploma in Hospitality and Tourism Management, and the Bachelor of Science in Nursing comprising the largest groups, suggesting a heterogeneous academic background.
With respect to clinical background, only 7.0% reported a family history of breast cancer, and 6.3% had prior breast disease, indicating that most participants lacked direct personal or familial experience that could enhance awareness or knowledge of breast health. Consistent with us, there is one study from Turkey that reported a family history of BC in 8.5% of the female participants. 23 Multivariable logistic regression identified health education and prior exposure as the strongest predictors of BSE practice. Students from the SHMS were significantly more likely to practice BSE than those from the IT (AOR = 3.20, 95% CI: 1.90-5.40, P < .001). Likewise, a family history of breast cancer (AOR = 2.60, 95% CI: 1.30-5.20, P = .007) and previous exposure to breast disease (AOR = 3.10, 95% CI: 1.75-5.48, P < .001) independently increased the likelihood of practice similar to one study from India. 24 In contrast, age and marital status were not significant, 25 underscoring that BSE practice is primarily influenced by health-related knowledge and experiential factors rather than basic socio-demographic characteristics.
Our findings are consistent with emerging evidence that while awareness of BSE is common among young women, correct knowledge and routine practice remain suboptimal. In a large cross-country study of young females in Qatar, although roughly half reported knowing how to conduct BSE, only a small fraction practiced it monthly, highlighting a persistent awareness-practice gap. 26 Similarly, Nigerian research among undergraduates found that good knowledge of BSE was significantly associated with correct practice, yet overall practice levels were low. 27 As in our data, where health sciences students had better technique but similar overall practice frequency, research conducted with university students in Bahrain showed that even when students understood that BSE should be performed monthly, a majority did not do so regularly. 28
However, despite higher awareness, knowledge of how to perform BSE, and the perception of its importance did not differ significantly between the two schools, a finding that mirrors reports from Tanzania, Uganda, and Malaysia, where awareness does not necessarily translate into adequate procedural knowledge. This persistent gap suggests that even health sciences curricula may insufficiently emphasize practical BSE skills.
The monthly performance of BSE was low in both groups (41.8% in SHMS vs. 35.0% in Tourism), with no statistically significant difference, aligning with several African and Asian university-based studies that report irregular or inconsistent BSE practice despite positive attitudes.29-31 This contrasts with practice rates reported in Hungary among university students: 50.2% performed BSE regularly, 41.8% occasionally, and 8% never. 32 Likewise, a significant percentage change in BSE practices was observed between pre-test and post-test after the educative intervention (21.3% vs. 33.8%; P < .001). 33 Notably, SHMS students were significantly more likely to use the recommended technique of three fingers and the palm and to examine key breast changes (P < .001), findings that are consistent with studies among medical students in Ghana. 34 These differences highlight the impact of formal clinical instruction on the quality of BSE technique rather than on its frequency.
In contrast, variables such as time spent performing BSE, frequency, reasons for performing BSE, and age at initiation showed no significant inter-school differences, echoing findings from multicenter studies indicating that sociocultural beliefs and personal risk perception often outweigh academic background in influencing sustained preventive practices. These patterns suggest that educational interventions must go beyond raising awareness to include hands-on skills training, confidence-building, and behavioral support, especially in low-resource contexts where clinical screening options are limited.
The findings indicate that a majority of participants (59.7%) demonstrated inadequate BSE practices, while only a minority engaged in good practices. This pattern is consistent with studies conducted among female university students in low- and middle-income countries, where knowledge and skills often do not translate into regular, correct BSE behavior.35-37 The predominance of inadequate practice may reflect several factors, including limited exposure to structured health education, insufficient emphasis on procedural skills in non-health curricula, and low perceived personal risk, particularly among students without a family history of breast cancer.
The observed gap between awareness and practice underscores a well-documented discrepancy in preventive health behavior: Although students may be aware of BSE, this does not necessarily lead to regular monthly examination or correct technique. 38 Moreover, a similar study in Gambia reports that BSE practice rates are very low among female university students, suggesting that the findings from the SUZA align with regional trends while highlighting the persistent challenge of translating knowledge into consistent and effective practice. These results emphasize the need for targeted, skill-oriented interventions that go beyond awareness campaigns, focusing on hands-on training, reinforcement of correct techniques, and motivation strategies to promote regular and accurate BSE among female students, particularly in non-health faculties.
The analysis of barriers to BSE among female students at the SUZA highlights a clear distinction between knowledge-related barriers and attitudinal or timing factors. While attitudes toward BSE and the age of initiation were generally consistent across academic disciplines, knowledge deficits emerged as a major barrier, particularly among students from the IT. Specifically, a significantly higher proportion of tourism students reported using incorrect or unknown methods for BSE than their counterparts in the SHMS (70.1% vs. 55.5%; χ² = 10.27, P = .016). Furthermore, knowledge of what to examine during BSE was markedly lower among tourism students, with nearly two-thirds unable to identify the correct assessment points, compared with less than half of health sciences students (69.2% vs. 43.4%; χ² = 25.19, P < .001).
Despite a high proportion of students in both schools recognizing the importance of BSE, regular monthly practice remained suboptimal and did not differ significantly across academic disciplines. This discordance between positive attitudes and preventive behavior has been consistently reported among university students in Africa and Asia, where awareness alone has not translated into sustained practice.39, 40 Similar to our findings, a recent study from Ethiopia showed that, despite perceiving BSE as important, fewer than half of the students practiced it monthly. 41 These observations align with behavioral frameworks endorsed by the World Health Organization, which emphasize that knowledge must be reinforced by skills training and perceived self-efficacy to effect behavioral change. 42
Significant differences between schools were observed in technical barriers, particularly regarding correct BSE methods and knowledge of what to examine, with health sciences students demonstrating superior performance. These findings are consistent with recent potential barriers or enhancement of breast cancer prevention in a systematic review, 43 where knowledge and training were associated with improved procedural accuracy and recognition of warning signs such as breast lumps, asymmetry, and nipple discharge. 44 Nonetheless, the persistence of incorrect techniques and knowledge gaps, even among health sciences students, mirrors reports from Kenya, suggesting that curricular emphasis may favor theoretical awareness over practical competency.45, 46 Late initiation of BSE (>20 years) across both groups further reflects delayed exposure to breast health education, a pattern widely documented in low- and middle-income settings. 47 Collectively, these findings indicate that while health-related education mitigates technical barriers, broader institutional strategies are needed to address behavioral and educational gaps across all university programs.
Collectively, these results underscore the need for targeted, skill-based educational interventions across university faculties, focusing on hands-on demonstration of correct BSE techniques, identification of key breast changes, and reinforcement of practical competence. Tailoring interventions to non-health students may be particularly effective, as these groups appear to be at greatest risk of procedural knowledge deficits despite having similar awareness and attitudes toward BSE. Implementing such strategies could improve early detection behaviors and ultimately contribute to breast cancer prevention in young women.
Limitations
The cross-sectional design limits causal inference between knowledge and practice.
Self-reported data may be affected by recall or social desirability bias.
The study was limited to two campuses, restricting generalizability to other SUZA campuses or universities.
Resource constraints prevented a full sample size of 384 participants.
Conclusions
BSE awareness among SUZA students is moderate, but correct and routine practice remains inadequate. Health sciences students demonstrated greater technical knowledge, highlighting the influence of the curriculum on procedural competence. Knowledge-related barriers, especially among non-health students, underscore the need for skill-based educational interventions.
Recommendations
Implement structured, hands-on BSE training across all faculties.
Integrate BSE modules into university health education programs.
Encourage peer-led awareness campaigns to reinforce skills and motivation.
Conduct longitudinal studies to monitor the effectiveness of interventions.
Footnotes
List of Abbreviations
ANOVA: Analysis of variance
BScN: Bachelor of Science in Nursing
BATMM: Bachelor of Arts in Tourism and Marketing Management
BSE: Breast self-examination
CI: Confidence interval
DHTM: Diploma in Hospitality and Tourism Management
Epi Info: Epidemiological information software
KAP: Knowledge, attitude, and practice
LR: Likelihood ratio
OR: Odds ratio
SHMS: School of health and medical sciences
SPSS: Statistical Package for the Social Sciences
SUZA: State University of Zanzibar
WHO: World Health Organization
χ²: Chi-square
Acknowledgments
The authors thank the SHMS and the IT, SUZA, for their administrative support. We appreciate all participants for their time and cooperation, and the research assistants for their help with data collection and entry.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical guidance and approval were granted by the SHMS Ethics Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.