
Abstract
There is a collective agreement on having an age-appropriate sex education curriculum. However, proper implementation is lacking in most education boards around the world. This study explores the level of sexual health awareness and practices of young adults at the University of Delhi. We analysed the current awareness levels of these adults and tried to understand if and why there is a gap in their understanding through three components of sex education: awareness, practice and interaction with their partners and peers. Our study unfolds several layers of sex education or the lack of it, and argues for an immediate basic sex education programme to be incorporated into schools from the elementary level. Over 50% of participants learned about human reproduction before the 8th grade, primarily through informal sources. Our findings illustrate very low awareness of sexually transmitted diseases (STDs) and contraception methods in the young adults, even for HIV/AIDS, the awareness percentage is about half of the responses, which is astonishing. The study also reveals a lack of awareness about breastfeeding and HIV/AIDS, which could be due to earlier public advertisements not mentioning the same. Such a lack of awareness about sexual reproduction and STDs underlines the need for a comprehensive sex education programme in schools.
Keywords
Introduction
Sex education may be understood as the comprehensive knowledge of the biological, psychological, emotional and social determinants and implications of human sexual anatomy, reproduction, sexuality and associated sexual behaviours. Sex education is a lifelong process of acquiring information and forming attitudes, beliefs and values. It encompasses sexual development, sexual and reproductive health, interpersonal relationships, affection, intimacy, body image and gender. 1 Sex education plays a central role in enabling individuals to make informed decisions in this regard and lead sexually healthy lives by preventing sexually transmitted diseases (STDs) and unplanned pregnancies, as well as the negative emotions and distress that may arise as a consequence of certain choices made in the absence of such knowledge.
The need for detailed and properly delivered sex education is especially pertinent to adolescents owing to the number of changes, both biological and otherwise, that adolescents undergo. Equipping the adolescent and youth population with factually consistent ‘sex education’ can enable them to understand themselves better as well as others around them and, in doing so, help them sail smoothly through this often-treacherous period. Improving adolescents’ knowledge and understanding of sexual and reproductive health, including HIV/AIDS, and thus improving their skills in life to take care of their own health, is a crucial step in the direction of meeting their health needs and fulfilling their rights. 2
Ironically, despite being home to a large youth population, India has consistently shied away from the very idea of sex education. Any conversations around sex and sexuality continue to be taboo amongst a considerable number of households in India, and the situation is not much different in schools either. More often than not, adolescents in India have had almost no structured sex education in their lives or have only been introduced to sex education as reproductive biology in school. There is content on the biological aspects of the reproduction system in the school syllabi and textbooks, but education in these elements cannot be complete by simply giving biological information. There is a need to focus on the physiological, emotional and sociocultural dimensions of adolescent reproductive and sexual health (ARSH) in a holistic manner. 3 Due to the lack of information, young people tend to turn to their friends or online sources for information that may or may not be accurate. As a result of the stigma around sex in society, there also exists a certain communication gap between children and their parents, and this results in teens growing up with very limited guidance and, often, a fear of being reprimanded for their curiosities. Parents should also do their part to provide a comfortable environment at home where they can talk about these issues freely and openly. 4
This short article will discuss the existing practices, levels of awareness and discussions about sex education among college-going adults in India. The study has been conducted primarily on the students at the University of Delhi to assess their awareness of sex, sexuality and safe sex practices. Starting from their basic school-level knowledge about sex education, it will look at how this knowledge is transmitted into their daily safe sex practices and everyday discussions about sexual health. We identify that there is a lack of knowledge that has caused inadequate and unsafe sex practices and led to the construction and reinforcement of taboos related to STDs (which translates to larger discrimination against people who have STDs in Indian society). The research raises these important questions and concerns regarding the consequences of the lack of knowledge about sex education in the Indian youth. However, this study cannot conclusively comment on the behaviours and practices of all youth in India; the sample taken is quite diverse, with representation from most of the Indian states.
Our focus will be on reiterating the fact that ‘Sex Education’ is not about teaching the act of sex. Rather, it prepares young children to handle different conditions they will eventually face. The idea is that children should know what good and bad touch is, what authentic sources they should rely upon for such queries, and if they need help related to these issues, they can talk without fear of taboo and shame. An essential component of sex education, apart from teaching the physiological and biological factors, is an undercurrent of sexual harassment that needs to be addressed under the banner of ‘Sex Education’ because there is no other modality where how to behave decently, dynamic nature of consent and what is right/wrong can be taught, it needs to be imparted within the umbrella of sex education. However, sex education needs to be delivered through structured educational institutions instead of the current cycle of friends, the Internet and sexist humour. Education is not just an appendage to ‘Sex Education’; it is a means to scientifically inculcate overall societal well-being.
Literature Review
Currently, India has one of the highest rates of population growth in the world; it shares 11% of teenage pregnancy births worldwide. 5 Complications arising from pregnancy and unsafe abortions are a leading cause of death among women aged 15–19 years. 6 The risk of maternal mortality among adolescent mothers stands twice as high as that of mothers aged 25–39 years. Education about family planning, conception and contraception could ameliorate the situation and give young women the opportunity to make their own informed decisions. India also has the 2nd highest HIV/AIDS infection rate; more importantly, adolescents in the age group of 15–24 years contribute to a disproportionate 31% of the AIDS burden in India, demonstrating their unique vulnerability to the infection. 7 According to the last UNAIDS report, there were 2.5 million people 15 years and above living with HIV in India. 8 These statistics underline the importance of comprehensive sexuality education in India.
Previous literature has noted the lack of a comprehensive sex education programme in India. There are many reasons for this, for instance, the absence of political will. Political parties and politicians consider sex education as a contentious topic and avoid the risk of advocating for it. 9 Even in initiatives like the Adolescent Education Programme, which focuses on providing some form of sexuality education to Indian adolescents during their schooling years. Research has found that there are substantial gaps in the programme, including covert and confusing usage of terms like sexuality, and sexual health, exclusion of people with disability, exclusion of intersex people, lack of discussion of conception, contraception and abortion, exclusion of rape and harassment in gender-based violence. 9
The knowledge about STDs like HIV/AIDS amongst youth remains low even after several awareness programmes and advertisements. India also has the 2nd highest HIV/AIDS infection rate; more importantly, adolescents in the age group of 15–24 years contribute to a disproportionate 31% of the AIDS burden in India, despite the whole demographic comprising about 25% of the country’s population. According to a study conducted in Gujarat, a considerable number of adolescents had correct knowledge about modes of HIV/AIDS transmission, but they lacked details about the disease. Only 35% knew the full form of HIV/AIDS, and less than 20% knew that women were more susceptible to the disease. 10 This can also be seen in another study where only a small proportion of the participants knew that contraceptives prevent HIV/AIDS. 11 It can be clearly seen that the lack of sex education among adolescents has caused grave problems for the youth, leading to unhealthy and unsafe practices and putting them at a much higher risk. Only 19% of girls and 35% of boys in India have complete knowledge about HIV/AIDS, while only 15% of boys and girls (15–24 years) said that they received sex education. 12 Among those people who had sexual intercourse between the age group of 15–19 years, 10.5% of girls and 10.8% of boys reported having sexually transmitted infection (STI) or symptoms of STI, and 0.07% of girls and 0.01% of boys were found to be HIV positive. 13
Previous research on the accessibility and exposure to sex education has demonstrated an urgent need for sex education programmes in schools. For instance, a study administered to students in junior colleges in Mumbai (ages 15–19) revealed that over 90% of students believed that it was important to have sex education as a part of their school curriculum. However, only 60% received some kind of sex education in school, while only 45% were satisfied with the information they received about contraception and sexual health. 14
The lack of sex education forces youth to resort to unreliable and sometimes incorrect sources like pornography, Internet forums and peers. There is research that indicates that such youth exposed to sexually explicit content without supervision at a young age are more likely to engage in unsafe sex practices, including the risk of STDs and pregnancy. 15 The need for a comprehensive sexuality education programme has also been backed by nonprofit organisations like Nari Raksha Samiti, which submitted a report stating that such a programme could play an important role in addressing the rising number of rape and harassment cases in India. It is interesting that most Indian youth realise the importance of sexuality education programmes. However, most of them did not receive any form of sexuality education through school and family. Those who did receive sexuality education reported being better informed about their sexual health, methods of contraception and so on. 16 It is interesting to note that some topics within sexuality education received greater support than others. For instance, abortion, pregnancy and infections received more support, while more controversial topics like pleasure and sexual expression received less support from the youth. 17 This was also evident in our research; however, those findings are beyond the scope of this article.
Methodology
Since a sample frame is not available for such a sensitive issue; therefore, we did a non-probability sampling with a combination of convenience sampling and snowball sampling. The questionnaire was administered both in person and online. The survey was circulated amongst the various hostel and college groups in which the first author participated. Then, those participants were asked to circulate the questionnaire within their respective circles and friend groups. Researchers went to various student hostels to administer the in-person questionnaire while they distributed the online questionnaire through WhatsApp groups and email lists.
Questionnaire Design
The questionnaire was inspired by the UNESCO guidelines on comprehensive sexuality education, which outline key learning objectives and content areas of comprehensive sexuality education (CSE).
18
Questions were designed to assess awareness, sexual health practices and sources of sex education. Contents included:
Demographic Information Knowledge of Sexual and Reproductive Health Safe Sex Practices Sexual Identity and Orientation Understanding of Consent, Good Touch/Bad Touch Attitudes toward Sex Education in India
Items were reviewed for cultural sensitivity and clarity, with particular attention to avoiding stigmatising language. The questionnaire included both closed-ended questions (Likert scale, Yes/No, multiple choice) and open-ended questions to allow participants to elaborate on their understanding and personal experiences.
Sample Description
There were a total of 875 participants: 379 males and 496 females.
The participants for this part of the study belonged to the age group of 18–25 years and were all senior secondary qualified, college-going. Students below the age of 18 were not included in the study.
Ethical Considerations
Informed consent was obtained from the participants. The data obtained from the participants was kept confidential and was used only for academic purposes.
Pilot Study
After the initial draft, a pilot study on a sample of 30 was conducted, and the questionnaire was reframed. Participants were asked to complete the questionnaire and provide feedback on clarity, relevance and comfort level with the questions. There was a high acceptability of the topic, with participants emphasising the need for such a study. Specific feedback led to refinements in wording for clarity and addition/removal of items based on relevance and perceived sensitivity. For example, in the question based on good touch/bad touch, an option ‘self-realised’ was added. An open-ended question to assess the basic idea of sex education among students was added. Some questions were removed owing to the relevance of the research. Questions regarding the effectiveness of sex education were asked to understand whether it impacts students or not.
Analysis
The analysis section is split into three main sections—awareness levels of college students regarding the idea of human reproduction and sex, discussion around sex and their knowledge about safe sex practices.
Awareness Levels
According to the NCERT course structure, human reproduction is taught in the 8th standard, but our research shows that 51.29% of males and 43.56% of females are getting knowledge before the 8th standard, and 24.61% of males and 18.49% of females, even after that (Figure 1). The time when girls become aware of human reproduction aligns with the time of their menarche, that is, 12–13 years. This graph states that human reproduction needs to be taught before the 8th standard, preferably the 6th standard, if not the 5th. A significant number of boys get to know about the sexual nature of human reproduction before it is formally introduced in the 8th standard through various informal sources. These informal sources can be a cause of the misinformation and disinformation about sexual practices among young adults.
Which Standard—Idea of Sex.
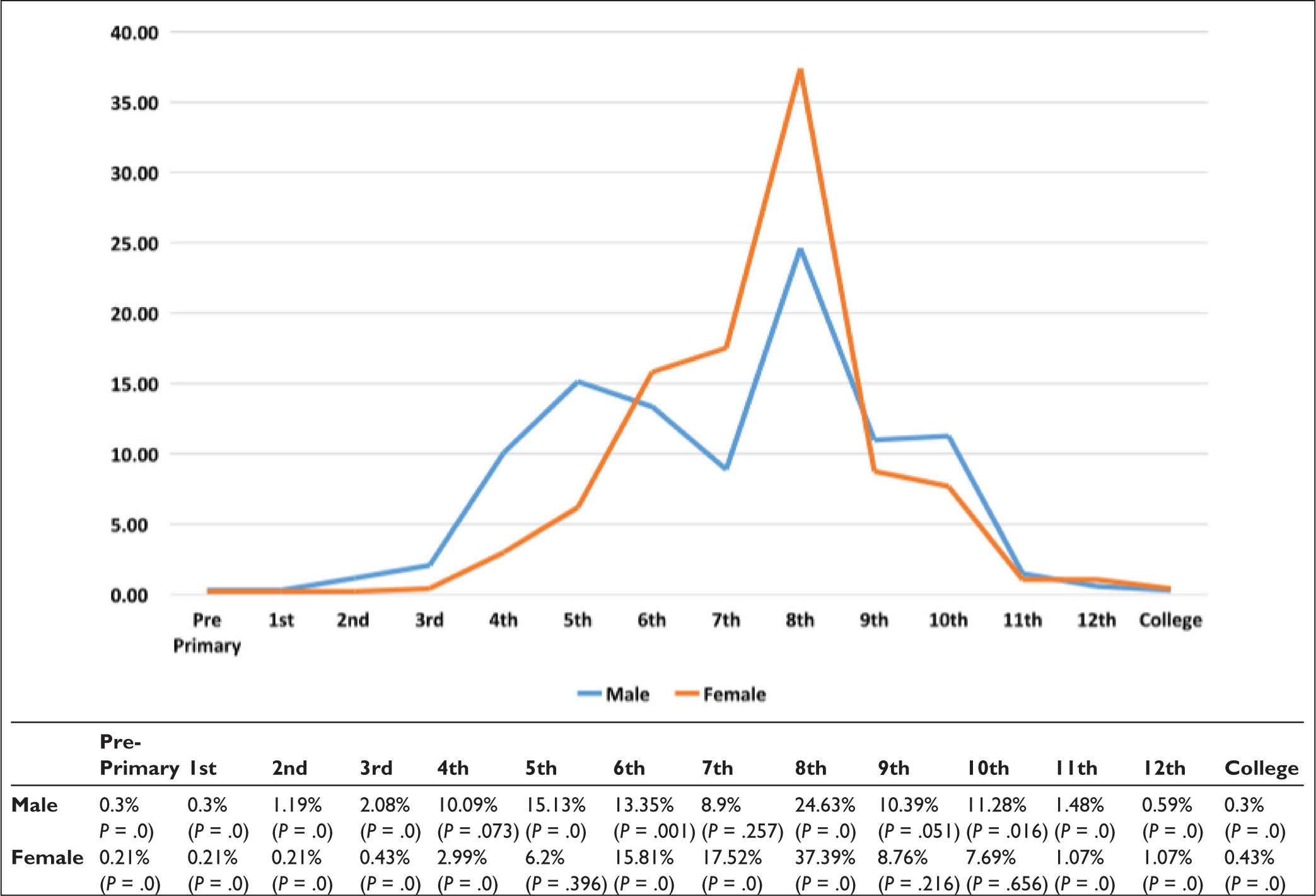
Table 1 demonstrates how and when students learned about good and bad touch. The data shows that males and females are mostly self-taught in this case; however, girls are taught more about this at home than boys. School is somewhat the same for them and extremely low, but the problem is of ‘self-realised’, ‘cannot differentiate’ and ‘not taught’, which needs to be addressed structurally because if most of them are self-realised which means they could only know about it after they know about human reproduction first but this needs to be taught before human reproduction part because child sexual abuse happens to young children who are unaware of ‘its functioning’. A large number of participants said that they self-realised the concept of good touch and bad touch, which also raises a question about how this ‘self-realisation’ happened, that is, through actual experiences or through theory. It’s also interesting to note that more female students were taught about good and bad touch at home than male students. This connects to the widescale prevalence of sexual harassment against Indian women, which is why parents are more open to talking to their daughters about that.
Learning about Good Touch/Bad Touch: from Kindergarten to self Realisation.
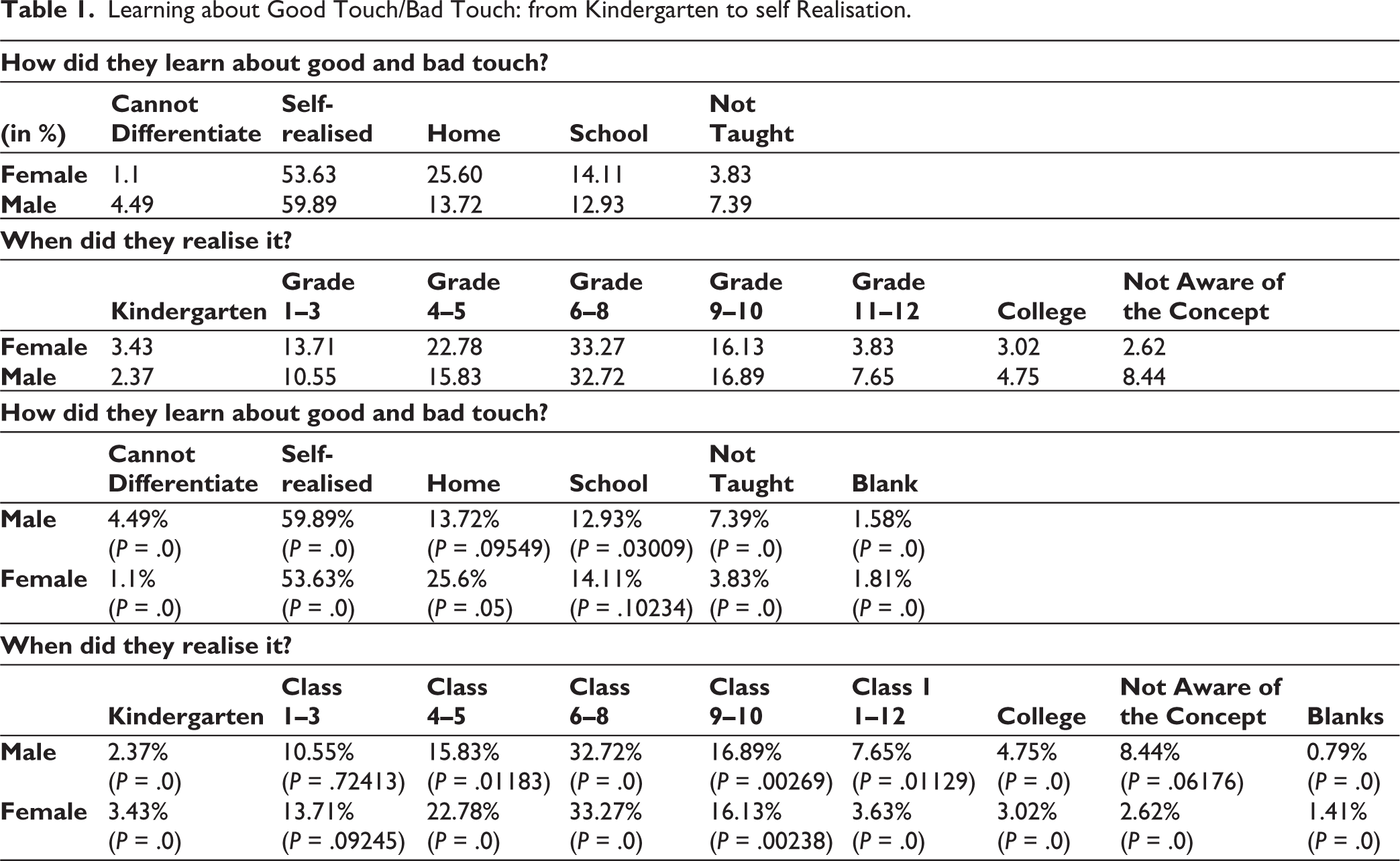
The result when they learned about good/bad touch is synchronous with teachings of human reproduction as most students get to know about it between classes 6 and 8. The earlier data shows that most students ‘self-realised’ to differentiate between good and bad touch, that is, they did not learn it in schools. Interestingly, overall, female students knew about the good and bad touch earlier than male students, which again points to whether this ‘self-realisation’ happened due to their own experiences of sexual harassment in public places.
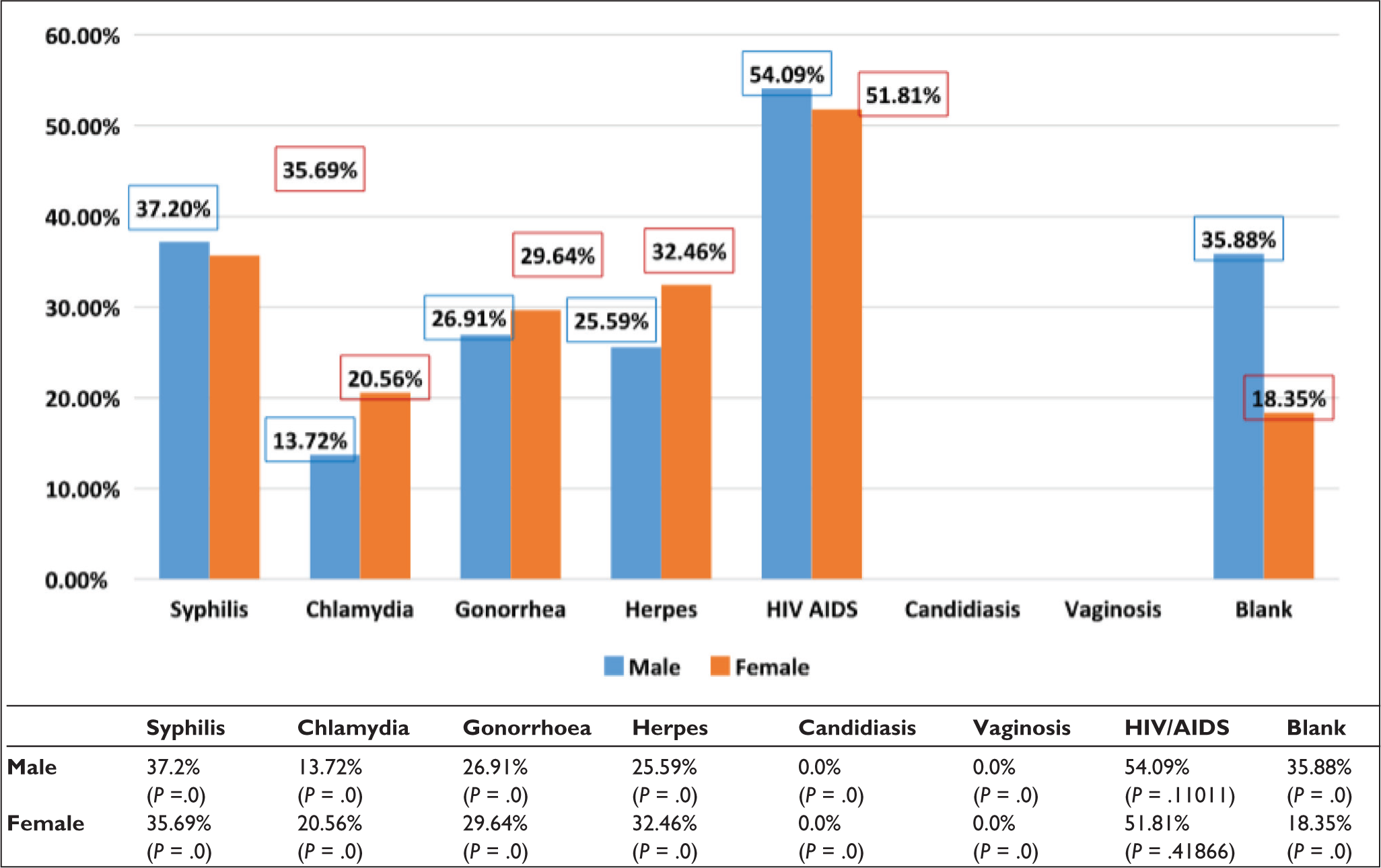
Figure 2 demonstrates the strikingly low levels of awareness about STDs among young adults in India. Just over 50% of students knew about HIV/AIDs. Despite government advertising on television/radio, the level of awareness about HIV/AIDS was still not up to the mark of satisfactory level. This could be linked to the efficacy of existing traditions in school pedagogy. This graph shows that a large number of students still do not know about STDs, which is highly alarming, even though they are college-going students. The lack of such important information at such an age can cause high susceptibility to STDs amongst the Indian youth. This data also corresponds with what we have initially speculated about the lack of appropriate information about sex education among young adults.
Sexually Transmitted Disease.
Discussion About Sex
Clearly, friends are the most relied option for both boys and girls, which may not be the most correct and comprehensive source for information about sexual practices (Table 2). Interestingly, books are also a good option for girls. The difference in the second most important source of information is stark between boys and girls, as more boys depended on the Internet and more girls depended on books. Internet and TV/Film are also not very good options as they are just mediums, and we cannot be sure about the content, so getting knowledge from non-normative sources is a large and frequent problem. It can be clearly inferred that a significant number of participants get the information from informal sources like friends and the Internet, which might lead to the transmission of incorrect information and often taboos.
Source of information and discussion about Sex among the Young Adults.
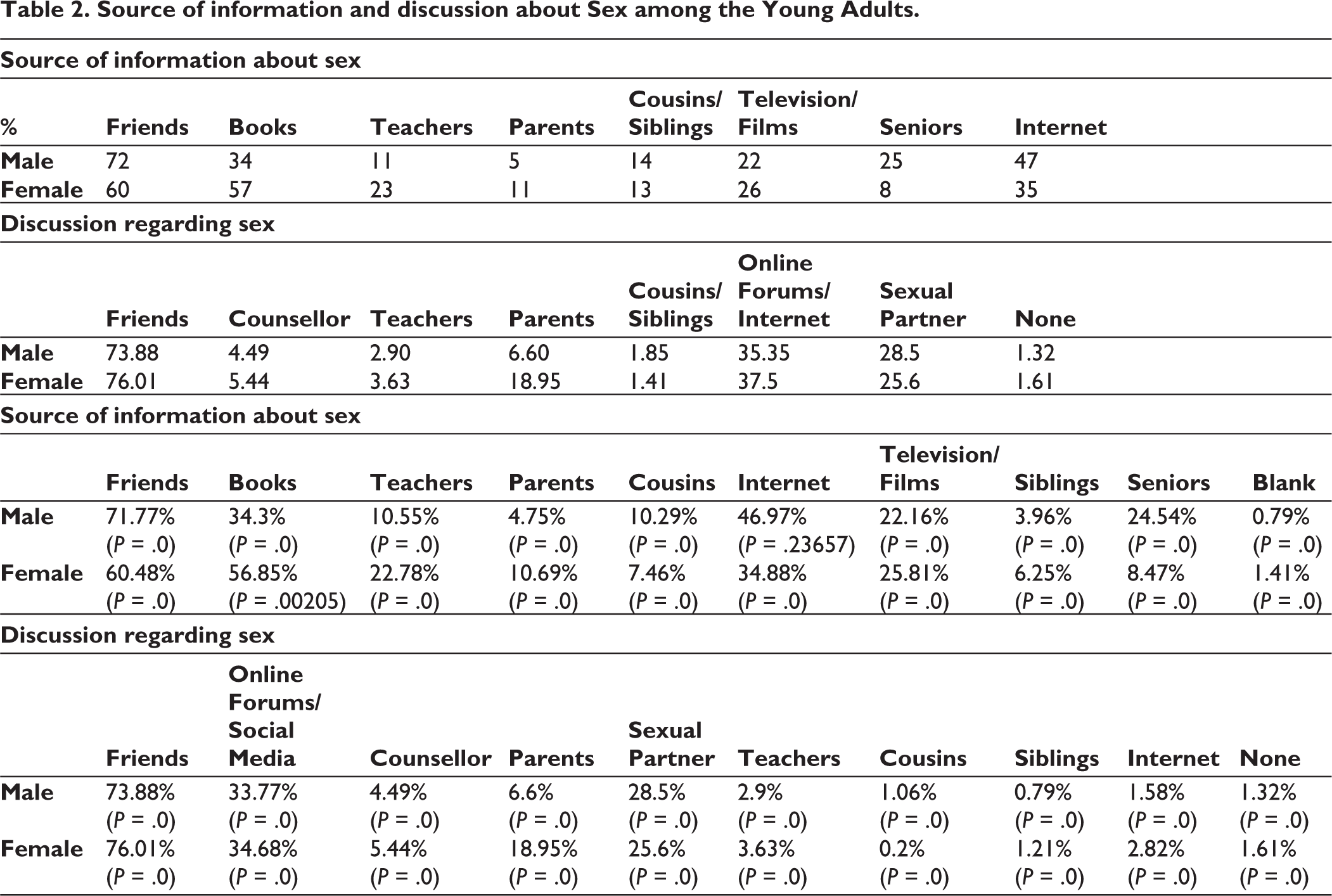
In the case of discussion, most of the discussion about sex is not with teachers, counsellors or parents but with friends (because of the trust factor) and online forums (because of the anonymity factor). Interestingly, females are threefold more than males in discussions with parents and maybe with only their mother, because the mother–daughter relationship is stronger due to information exchange on periods from a very young age. This is in line with their greater reliance on parents as a source of information regarding the idea of sex. This supplements the need for structural change so that the teachers and counsellors (if not parents) will be the go-to option for them, which will be authentic and reliable. This data corresponds with the source of information about sex, in which friends and the Internet were the most important sources for the participants rather than formal sources.
Practices
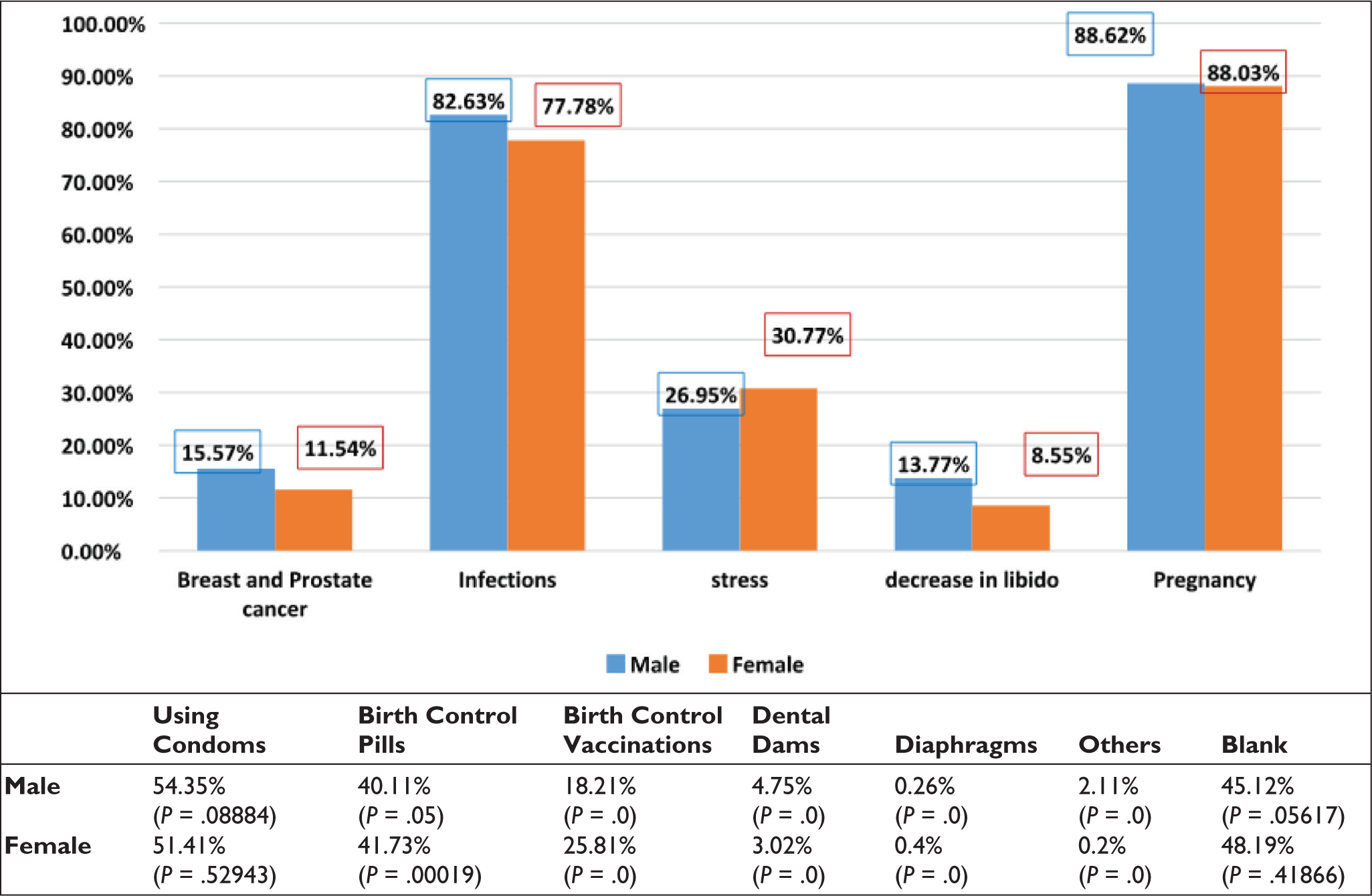
This graph clearly shows a gap in the levels of knowledge about the different methods of contraception. While condoms score the highest (amongst both boys and girls), close to 50% left the question blank (which correspondents to their lack of awareness about the different methods of contraception). While condoms and birth control pills are the most common and popular among young adults, they have little knowledge about birth control vaccinations, dental dams and diaphragms. The level of knowledge about methods of contraception also hints at their sexual health practices.
We further assessed their knowledge about the consequences of having unprotected sex (see supplementary graph 1). Infection and pregnancy as a consequence of having unprotected sex were known to most students (both men and women). However, there was disinformation around the topic as well, as some students marked breast and prostate cancer and a decrease in libido as consequences of having unprotected sex (Figure 3). This demonstrates a gap in our education system as well, where students do not have access to a comprehensive sexuality education programme.
Consequences of Practising Unprotected Sex.
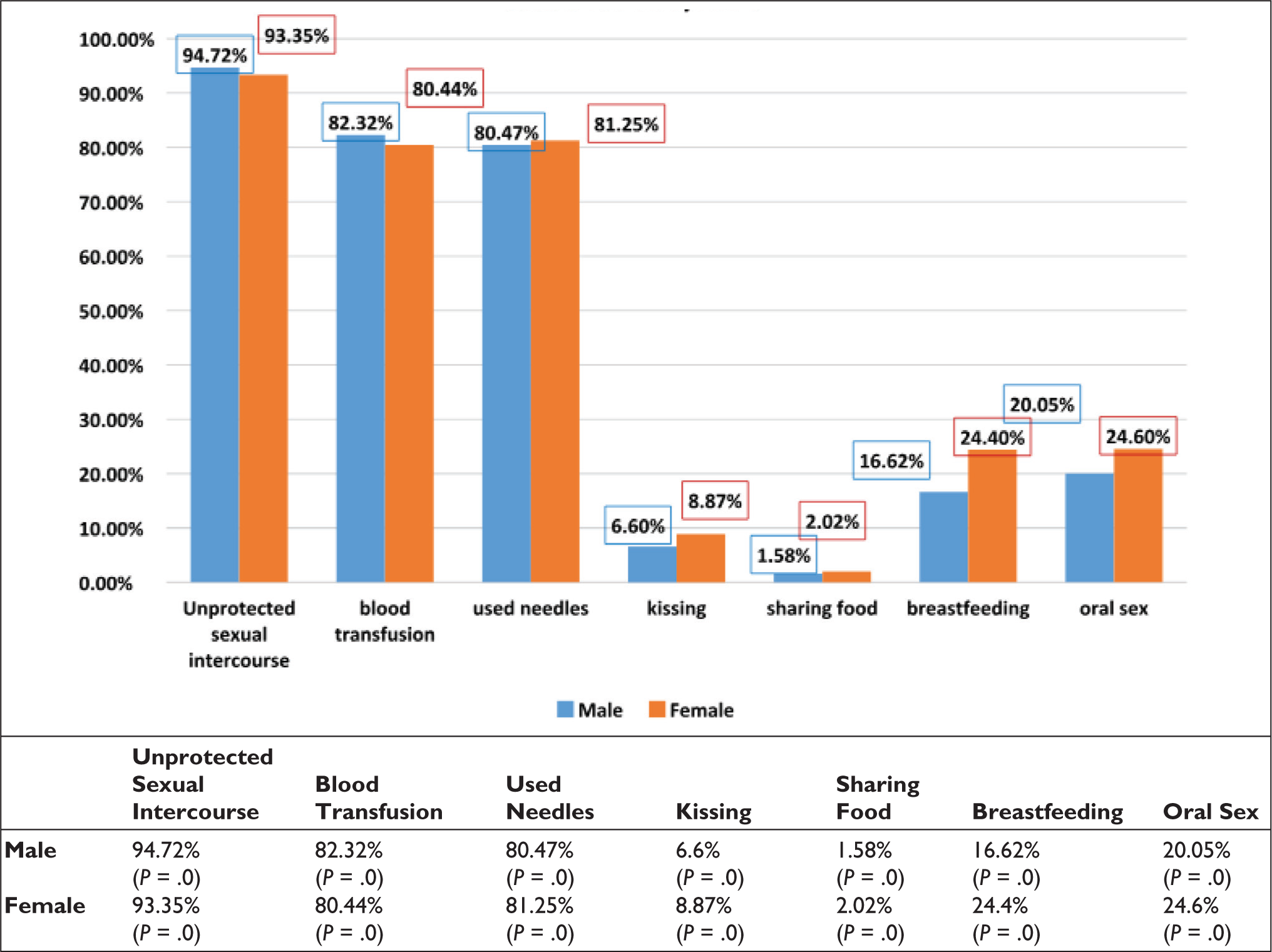
On being asked about the causes of HIV/AIDS, most students identified the main causes—unprotected sexual intercourse, blood transfusion and used needles (Figure 4). However, breastfeeding as a means is still less talked about. It is almost shocking that very few participants knew that breastfeeding can transmit AIDS. This can be because of inadequate and non-comprehensive advertising, as most of the government ads on AIDS do not talk about breastfeeding as a way of transmission. Whole and authentic information must be provided in school; otherwise, misinformation, such as sharing food and other wrong information, will be part of the practice.
Cause for HIV/AIDS.
Our last question examined their experiences regarding sexual harassment at work/academic settings, public places, sexual abuse in a relationship, sexual abuse at home/family settings and infidelity (supplementary graph 2). The data shows that over half of female participants have faced sexual harassment in public places, which means that many males are practicing it, and it is a serious pedagogical failure. This needs to be addressed at the primary institutional level; consent must be part of sexuality education. Also, workplace harassment and sexual abuse in relationships are serious challenges, and they disproportionately affect female students. Similarly, almost twice the number of female students (as compared to male students) had experienced sexual abuse at home/family settings. Interestingly, most women learn about good touch and bad touch by self-realisation (discussed earlier). There is a strong correlation between more women experiencing sexual harassment and abuse and self-realisation of good touch and bad touch. This also points towards the gap in our education system that does not equip our young people with the tools and knowledge to know the difference between good and bad touch before it happens to them.
Discussion and Conclusion
A questionnaire was designed to conduct a survey on college students to assess their views towards sex education as well as gauge the level of sex education they had received. It is comprised of a holistic view of sex education that includes sexual health, practices and stigma. A total of 875 respondents participated in the survey, of which there are 379 males and 496 females. The respondents were between the ages of 18–25 and were from many different colleges all over the country, though a majority were from the University of Delhi.
The findings of the study were consistent with the existing literature on the paucity of comprehensive sexuality education programmes in India. The lack of knowledge about sexual health, safe sex practices and STDs further highlights the lack of sex education in present times. Currently, sex education in educational setups is largely limited to the sexual nature of human reproduction and does not include key information about sexuality, sexual health and safe sex practices. The results of our study also correspond with what previous research on sex education; for instance, Das, 9 reported that most of the students felt sex education was an important aspect that should be a part of school curricula, but only a few of them reported having had some prior sex education. One of the most concerning findings of the study was that the students’ reliance on peers, the Internet or sexual partners for information, while only a negligible percentage consulted parents or teachers. It was found that our respondents relied most on friends (74% male and 74% female), online forums/social media (35% male and 34% female) and lastly, sexual partners (28% males and 25% females) when they had any questions about sex. This further highlights the gap in communication with parents that was found earlier. This highlights that sex education still remains taboo and stigmatising even in urban metropolitan areas like Delhi, which was noted in the previous literature, like Thomas and Thomas, 4 who argue how curiosity around sex is punished, and questions around these topics are ignored.
Another alarming finding was the high levels of sexual harassment reported by respondents, particularly female respondents, coupled with the absence of formal sexuality education programmes that educate students on how to recognise and address these issues. This finding aligns with the earlier literature on how gender-based violence is excluded from the sexuality education programmes existing in India. 9
Despite these issues, the receptivity to sex education was strong amongst students. A majority of students expressed a desire for more robust, age-appropriate and inclusive sex education as part of their formal schooling. This finding suggests that Indian youth are ready and eager to engage with comprehensive sexuality education that reflects their real-life questions and needs. As such, the study aligns with the previous research on sex education that has pointed out that most students believed that sex education should be administered as a part of their formal school curriculum. 14
The study has a small scope because all the respondents belonged to urban, well-educated backgrounds with Internet access. Thus, it cannot be representative of the entire Indian youth. Nonetheless, the location where the survey was carried out, that is, Delhi, has one of the highest migrant populations from across the Indian states, so part of India’s diversity is represented. As it is, it may not capture the experience of rural, poor or out-of-school adolescents, who would even more likely have additional barriers to sexual health information. Future research requires a larger longitudinal study across several Indian states, combining community and ethnographic research that reaches more diverse and marginalised community groups. Furthermore, the utilisation of self-reported data may have led to the underreporting of sensitive issues like harassment or sexual activity due to social desirability bias.
Future studies need to achieve broader demographic representation, including the representation of marginalised and rural populations. Longitudinal and ethnographic studies would offer greater understanding of how sex education (or its absence) influences sexual behaviour, health outcomes and gender relations over the longer term. Studies are also required into how digital media and informal networks are mediating young people’s knowledge and understanding of sex in the context of the absence of school-based education.
Implications
The findings of this study have several key implications for educational policy, public health and parental engagement in India:
Policy Reform: India must immediately revise and expand its sex education curriculum in schools according to UNESCO’s comprehensive sexuality education model. These should include gender, consent, Internet safety, emotional health and sexual orientation at a minimum, alongside basic reproductive biology. Capacity Building and Trainer Training: Not only should teachers be trained in the content to be delivered, but also in how to create safe, non-judgmental spaces for students to discuss sex and sexuality. Parental Involvement: Parent sensitisation workshops must be included in programmes to close the communication gap within homes and foster open, healthy dialogue between caregivers and youth. Cultural Adaptation of Materials: Learning materials must be tailored to local languages, cultural customs and religious feelings without sacrificing the content of the information being communicated.
This study quotes from the earlier studies to establish that Indian sex education is still poor in terms of reach and scope. However, what we find is a strong potential: young people want to learn. We can prevent sexual disease as well as lessen deep-seated stigmas and empower a more equal and educated community by responding to their needs with compassion, evidence-based and equitable interventions. Meeting young people’s needs with empathetic, evidence-based and inclusive programmes, we cannot only push for sexual health but also defy deeply ingrained stigmas and empower a more knowledgeable society that empowers equally.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Consent to Participate
The participants signed a consent form stating their consent to participate in the study. The form was the first part of the survey (administered both online and offline).
Consent for Publication
The participants signed a consent form stating their consent to participate in the study. Further, the clause also included consent to any publications that may arise from the study. The form was the first part of the survey (administered both online and offline).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
The study followed all the standard ethical procedures at every stage of the research which included data confidentiality, participant anonymity and protection of data during the stages of collection, analysis and storage. When the study was conducted there was no institutional review required, however, the standard procedures were followed to conduct the research.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.