
Abstract
Male sexual functioning is influenced by a complex interplay of psychogenic, neurogenic, vascular, hormonal, psychological, and cultural factors. While global studies have examined sexual dysfunction and its psychiatric comorbidities, research in the Indian context remains limited, especially concerning prevalence, comorbidities, and sociocultural influences. To address this gap, a narrative review was conducted. Following Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines, the review examined studies published between January 2000 and February 2023 across databases such as Scopus, Google Scholar, Web of Science, and PubMed. Only original Indian studies with full-text availability were included. Studies involving comorbidities such as human immunodeficiency virus/acquired immunodeficiency virus (HIV/AIDS), autoimmune disorders, and major psychiatric or developmental conditions were excluded. Of the 482 articles screened, 12 met the inclusion criteria. The reported prevalence of erectile dysfunction and premature ejaculation ranged from 20% to 64% and 18% to 55%, respectively. Sexual activity among older adults declined significantly after age 60, influenced by biological and psychological factors. A consistently high prevalence of anxiety and depression as comorbidities was noted. Additionally, the sexuality of aging men is often stigmatized in Indian society, contributing to psychiatric morbidity and underdiagnosis. Cultural barriers further hinder help-seeking and treatment. In conclusion, Indian men appear particularly vulnerable to erectile dysfunction and premature ejaculation, with prevalence closely linked to psychiatric comorbidities, sociocultural stigma, and age-related changes. These findings underscore the need for culturally sensitive clinical practices and public health strategies targeting sexual health and associated mental health concern.
Keywords
Introduction
Sexual functions are essential in determining men’s emotional and physical health and well-being. 1 Male sexual functioning is a complex interplay of psychological, neurogenic, vascular, and hormonal factors that culminate in erection and ejaculation. The male sexual response involves desire, arousal, orgasm, and resolution, and disturbances in this continuum result in sexual dysfunction. 2 The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5 TR) categorizes male sexual dysfunctions into Male Hypoactive Sexual Desire Disorder (MHSDD), erectile disorder (ED), premature ejaculation (PE), and delayed ejaculation. 3
Men across the world are affected by sexual dysfunctions. Globally, 52% of men aged 40–70 experience sexual dysfunctions, which are caused by a combination of physical and psychological factors. 4 The prevalence rates of ED and PE, common sexual dysfunctions, vary across age groups. The prevalence of ED increases with age, reaching 30% for men aged 40–59, 40% for those in the 60–69 age group, and 75% for men in their 70s to 80s. Similarly, the prevalence of PE is high, with rates reaching 31% among men aged 18–59. 1 MHSDD has a prevalence of around 10% globally. 1
In India, male sexual dysfunction is a common health problem. Despite being the land of the Kama Sutra, sexual taboos in India lead to underdiagnosis. Men often feel reluctant to discuss these issues with healthcare professionals, seeking remedies from untrained and untrustworthy sources such as faith healers, the Internet, and pornography resources.5–7
Furthermore, to create comprehensive treatment regimens for males with sexual dysfunctions, it is critical to understand the comorbid psychological disorders. 8 Globally, there are large-scale studies on comorbid conditions with male sexual dysfunctions.9,10 However, the few studies conducted in the Indian context highlight the necessity of filling the knowledge gap and offering data that could guide future research. Consequently, the goal of this review is to investigate, compile, and evaluate the body of research regarding the prevalence and co-occurring disorders among Indian men who experience sexual dysfunction. By shedding light on this critical aspect of men’s health, we can foster a more informed dialogue and promote effective interventions to enhance the well-being of affected individuals.
Methods
This narrative review was conducted to understand the prevalence of sexual dysfunction and the psychiatric comorbidities in individuals with sexual dysfunction.
Data Sources and Search Strategy
A comprehensive search was conducted through electronic databases, including Scopus, Google Scholar, Web of Science, and PubMed. Studies from January 2000 to February 2023 were included. The search was carried out using combinations of keywords such as [sexual dysfunctions(tab) OR “sexual disorder” OR sexual* OR “sexual problems” OR “erectile dysfunction” OR “premature ejaculation”] AND “Indian male” OR “Indi*” AND [“comorbid” OR “comorbid conditions” OR “comorbid illness” OR “psychiatric conditions” OR “psychiatric morbidity” OR “psychological problems” OR “psychiatric disorders”] AND “Elderly sexuality” OR “Elderly sex” OR “Elder sexual health.”
The inclusion criteria for the review were (a) peer-reviewed original studies, (b) studies reporting the prevalence of sexual dysfunction, and (c) studies involving the Indian population. Studies that focused on non-Indian populations, women, individuals with human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS), autoimmune diseases, or major psychiatric and developmental disorders such as autism, attention deficit hyperactivity disorder (ADHD), bipolar disorder, and schizophrenia were excluded from the review.
Study Selection and Data Extraction
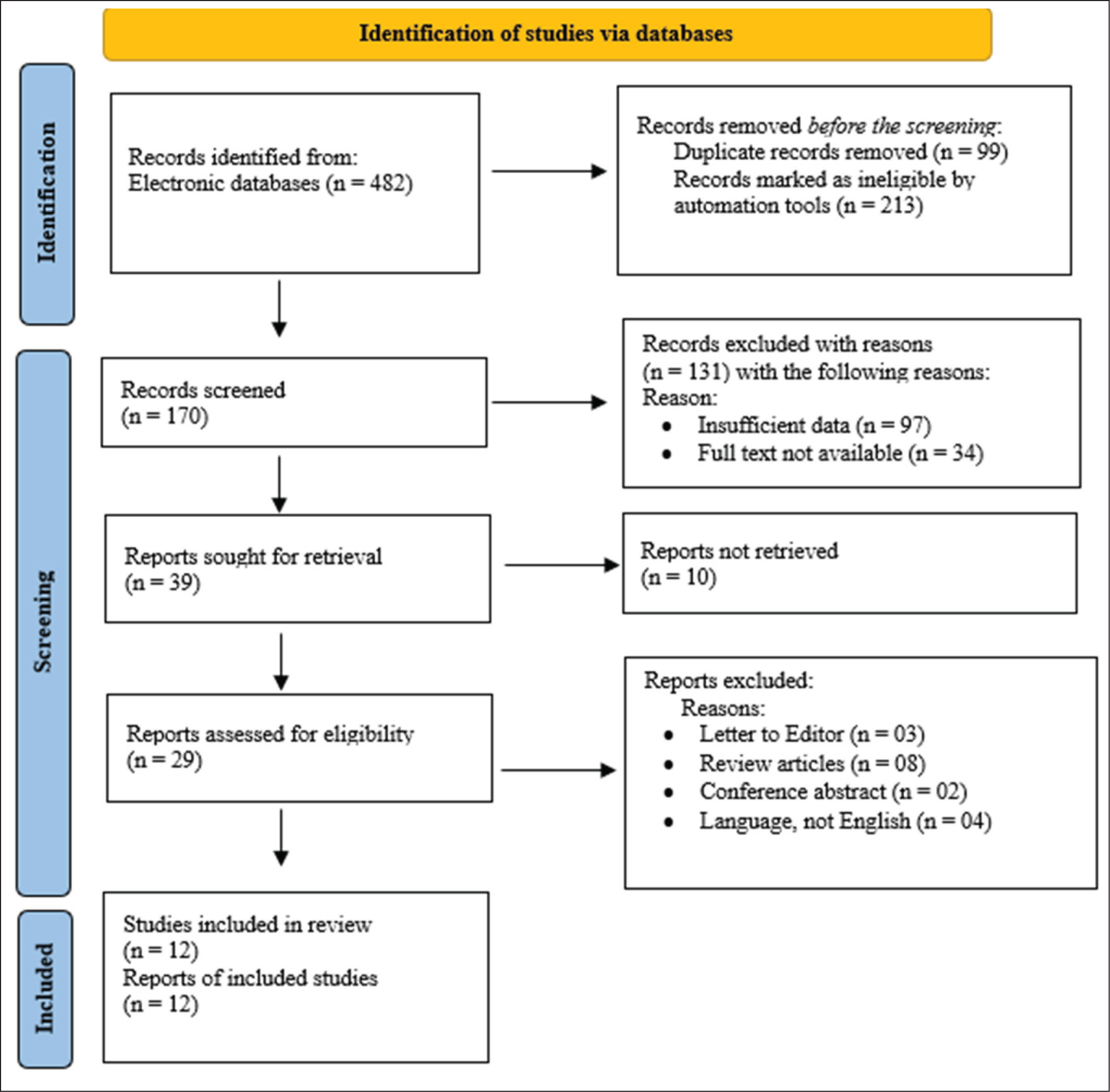
A team of two authors (SB and PK) conducted a literature search, identifying 482 articles. Four authors (SB, PK, MP, and TSSR) collaborated to screen the articles based on the study’s criteria. Another author (UK) resolved any discrepancies that arose during the screening process, resulting in the selection and inclusion of 12 studies in the current narrative review. Any differences regarding the articles and the screening procedure were discussed collaboratively. SB, PK, MP, and TSSR screened the eligible articles and finalized the content in the review table (Figure 1 and Table 1). 11
Studies on Sexual Dysfunctions and Comorbid Psychiatric Conditions.


Results
Studies were conducted on Indian males aged 18 to 50 years. One study covered data from across India, three from West India, two from South India, and one from North India. Most of the participants were married, with more than 50% educated up to the secondary level. The majority of the participants were Hindus. A nationwide study indicated that 60% of the males came from rural parts of the country, with lower- to middle-income levels. 12
Most of these studies used a cross-sectional study design, with sample sizes ranging from 54 to 780. Participants were predominantly recruited using purposive sampling techniques from clinical settings. Data on sexual dysfunction were primarily collected using measures such as the International Index of Erectile Function (3 articles) and the Arizona Sexual Experiences Scale (3 articles). Psychiatric comorbidity data were gathered using instruments such as the Dyadic Adjustment Scale (1 article), the Mini International Neuropsychiatric Interview (3 articles) to evaluate psychiatric disorders, the Hamilton Depression Rating Scale (2 articles), the Hamilton Anxiety Rating Scale (2 articles), the State-Trait Anxiety Inventory (1 article), and the Chinese Index of Premature Ejaculation (1 article). A couple of reviews also used ICD-10 criteria to assess both psychiatric comorbidity and sexual dysfunction.
In elderly-specific sexuality reviews, findings indicated that sexual activity declines sharply with advancing age. In a rural South Indian population, only 27.4% of males above 60 years remained sexually active, and none reported sexual activity beyond 75 years. 13 Among sexually active elderly males, ED was present in 43.5%, PE in 10.9%.
Clinical guideline reviews emphasized that psychological conditions, such as performance anxiety, depression, and generalized anxiety disorders, significantly overlapped with sexual dysfunctions, particularly in elderly males. 6
Figure 2 indicates the presence of various sexual dysfunctions in Indian males aged 18–50 years old. Reviews reported that the prevalence of ED ranges from 20% to 64%, followed by PE, which ranges from 18% to 55%. Further findings show that the combination of ED and PE has a more consistent prevalence, reported between 17% and 18%. Additionally, other sexual dysfunctions, including lack of sexual desire and orgasmic dysfunction, were found to affect 4% to 47% of participants in the studies (Figure 2).
Prevalence of Sexual Dysfunction.
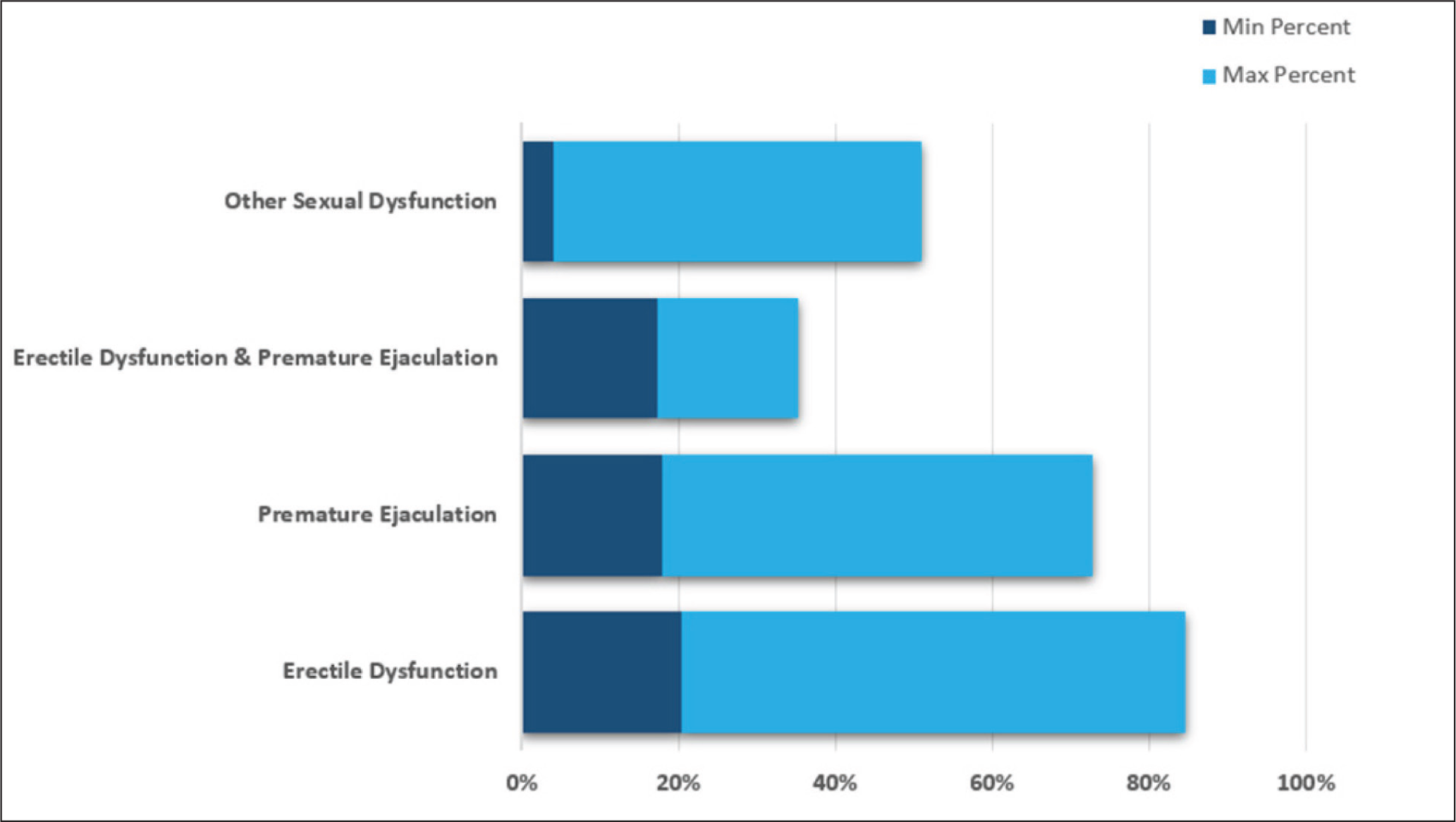
A review in West India highlighted that 13 cases of divorce were attributed to PE issues. 14 This study also reported that West India has the highest incidence of ED and PE rates (64% and 55%, respectively). While West, North, and South India have a similar lowest ED rate of 20%, South and West India have the lowest PE rate of 18%–19%. In North India, the lowest PE rate starts at 32%. No data was collected from North India regarding men with both ED and PE. In South and West India, 17% to 18% of men experience both ED and PE issues.
In Indian men, comorbidities between psychiatric problems and sexual dysfunctions are common. Studies consistently show links between these disorders (e.g., ED and PE) and psychiatric conditions like anxiety and depression.8,14–18 Rajkumar and Kumaran (2015) also stated in their study that some men even had suicidal thoughts. It has been observed that sexual dysfunction varies with age. 18 Younger men are more likely to experience PE, while older men are more likely to experience a combination of ED and PE. However, in a recent report by The Times of India, city-based andrologists and doctors in Hyderabad mentioned a growing trend of ED among youth and men aged 20–35. Increased anxiety and lifestyle issues are causing ED in these young men 19 (Figure 3).
Prevalence of Psychiatric Comorbidities.
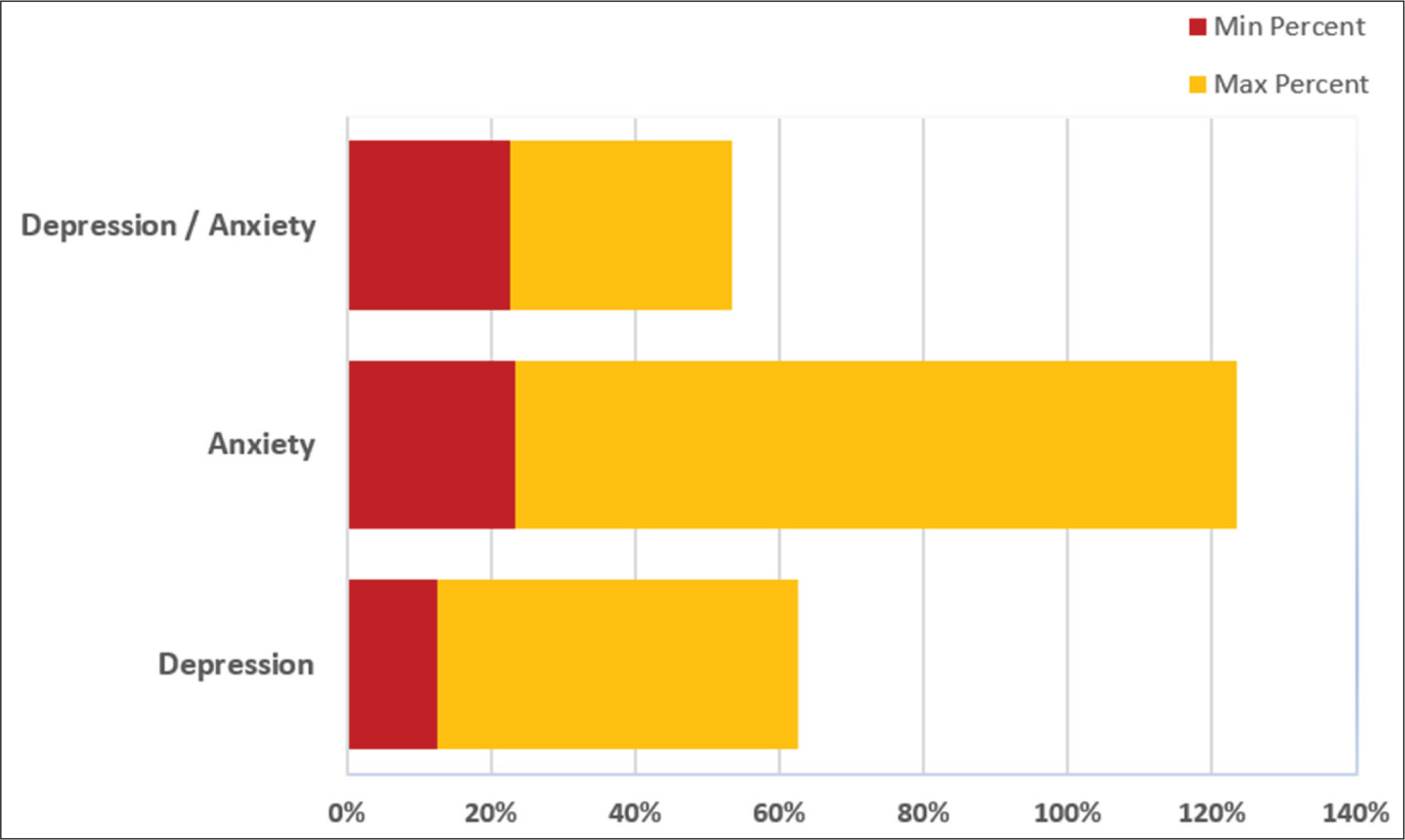
In Figure 3, studies reported that the prevalence of depression ranges between 13% and 50%, while anxiety affected 23% to 100% of all men in the studies. It is interesting to note that all men in the studies from West India suffered from anxiety problems. Rajkumar and Kumaran (2015) mentioned that anxiety issues are mainly related to performance anxiety in men with PE problems. 18 No data for the prevalence of anxiety was obtained from North India. Between 23% and 31% of men in the studies had both depression and anxiety issues across North, West, and South India. Again, West India has the highest prevalence of depression at 50%, while the lowest prevalence came from South India at 13%.
This concise summary emphasizes the frequency of sexual dysfunctions, the co-occurrence of mental health issues, cultural factors, and age-related trends among Indian men.
Discussion
Demographic Characteristics
From the 12 reviews including supporting elderly-specific studies, it has been noted that sexual dysfunction can occur between the ages of 18 and 50 years and continues to affect older males. In rural elderly populations, only 27.4% of individuals remained sexually active beyond 60 years, and no sexual activity was reported after 75 years. 13 This observation reinforces that sexual dysfunction and silence around the issue are even more pronounced in rural India.
Despite India being a large country with a huge population, we faced significant difficulties and limitations in retrieving literature on this topic. The reviews were scattered, with one from nationwide India, a few from North, South, and West India. The wide age group highlighted in these seven reviews may not accurately represent the entire sexual dysfunction scene in India.
A nationwide study indicated that 60% of males came from rural parts of the country with lower to middle income levels. 12 This may imply that there are even more men from rural areas with sexual dysfunction who do not come forward to seek treatment. Possible reasons could include high medical costs, which they are unable to afford for consistent treatment, and low-to-mid educational levels, making it difficult to communicate or discuss their sexual concerns openly with doctors. Cultural factors may also contribute to this. As a result, getting the right treatments early is often missed. Sexuality issues are often underdiagnosed, and most men live in silent suffering with sexual dysfunction, along with physical and psychological problems associated with the sexual disorder. Some men would rather consult their friends instead of seeking professional help, or they may look up self-cure remedies or solutions on the Internet. Some may eventually seek the help of healers or untrained professionals to quickly fix the problems, perhaps due to cheaper costs. 5
Kalra et al. (2015) stated that PE occurs in younger men aged 18–30 years, while both ED and PE occur more frequently in the older age group, 41–50 years. 17 While this seems to be the trend, the results could be reinforced with stronger support by adopting the International Premature Ejaculation Questionnaire (IPE), which is missing in the measures. In fact, the IPE seems to be missing as a checklist for PE assessment in all studies.
Sexual Dysfunction
Sexual dysfunction is increasing in India due to a complex interaction of physiological, psychological, and cultural variables. Studies conducted in South India and across the country have demonstrated the high incidence of sexual dysfunctions in Indian men. The current review reports the prevalence of ED in Indian men from South India ranges from 20% to 38%, while PE ranges from 19% to 45%, notwithstanding the inherent biases caused by differences in study design, measures, population site location, and sample size.12,16,18 Rao et al. (2015) reported that 15.77% of the South Indian rural population has ED, and 8.76% has PE. 20 Here, we can see the growing trend of both ED and PE over the years. A recent survey by Chennai based institutions, quoted in The Times of India, reported a rapid increase in male sexual dysfunction in the clinic. It was found that at least a third of men who participated in an online survey suffered from ED, and at least one in five had PE. 21 This yet-to-be-published survey suggested that changing lifestyles, an increase in uncontrolled hypertension and diabetes, inactive lifestyles, unhealthy diets, and the use of gadgets such as laptops and mobile phones are all linked to an increase in sexual dysfunctions.
Likewise, reviews from North India report that between 20% and 50% of individuals have ED, and 32%–46% were reported to have PEs.8,12 In a study by Singh et al. (2018), it was reported that 81% of men have at least one sexual health disorder in North India, with ED at 5% and PE at 4.6%. 22 While it is correct that at least 81% have sexual health disorders based on the North India reviews, the prevalence of ED and PEs seemed too far off. More in-depth studies are needed to verify the data here.
Reviews also showed that vascular disease and other biological variables are the main causes of ED in elderly males. Rao et al. (2015) noted that ED and PE rates in South Indian population have been sharply rising over time, indicating a significant public health concern. 13 Emerging evidence suggests that lifestyle changes, including sedentary behavior, unhealthy diets, and technological overuse, have exacerbated sexual dysfunction trends.
These issues reflect global trends and are impacted by the cultural diversity and evolving social dynamics within India, as illustrated by studies from Rao and reports from
Sexual Dysfunction in Elderly Males
Sexual dysfunctions in elderly males necessitate a specialized approach. Management strategies, as per Rao et al. (2018) and Avasthi et al. (2017), include:6,25
Psychosocial Interventions: Counselling, education about aging-related sexual changes, and couple therapy to address relationship dynamics. Medical Management: Use of phosphodiesterase inhibitors (e.g., sildenafil) in ED, with careful cardiovascular assessment. Psychiatric Care: Examining patients for anxiety and depression, particularly when sexual dysfunction is the symptom. Lifestyle Changes: Promoting exercise, a balanced diet, good sleeping habits, and minimizing the negative effects of polypharmacy that affect sexual function.
Relationship satisfaction, psychological anguish, and general well-being are all enhanced by the comprehensive treatment of sexual health concerns in the elderly.
Psychiatric Comorbidities
The coexistence of anxiety and depression with sexual dysfunction highlights the complex relationship between mental health and sexual satisfaction. The interplay of anxiety, stress hormones, and testosterone levels creates a web that affects an individual’s overall well-being. A holistic approach to managing these interconnected issues is vital. The impact extends beyond sexual performance and significantly affects an individual’s mental health and quality of life.
In elderly population, this relationship is intensified by loneliness, bereavement, declining physical health, and social isolation. 13 Elderly’ anxiety about being misinterpreted or judged keeps them from seeking help in a timely manner, which exacerbates mental health conditions. 26 Research highlighted that anxiety and depression not only coexist but also frequently aggravate sexual dysfunction, resulting in a vicious cycle whereby one condition worsens the other. 6
Dhat syndrome (DS) presents a distinct cultural dimension to the discourse, shedding light on the profound impact of cultural beliefs on sexual health. DS is a concern in North India among young individuals and is associated with anxiety over semen loss during sleep, through urine, or masturbation. Cultural beliefs contribute to performance myths. These DS patients are mostly young, recently married, poor, and from rural families with traditional views on sex. Both DS and anxiety about potency are topics that researchers often avoid discussing at length in India. 6 DS can be found in ICD-10 under neurotic disorders, while anxiety about potency is not mentioned.
Anxiety about one’s potency and associated myths are common in India. Beliefs such as masturbation before marriage leading to loss of potency in marital relationships, penis shrinkage, penis curving sideways, and watery semen are a few among them. These exaggerated “understandings” often lead to sexual performance anxiety and worries during the “first wedding night.” 6
The co-occurrence of sexual dysfunction, depression, and anxiety in people with DS highlights the psychological consequences of cultural preconceptions. The reluctance to seek medical intervention and the reliance on alternative remedies underscore the challenges faced by individuals in navigating cultural stigmas and limited access to specialized care.12,15
Cultural Factors
Cultural taboos surrounding elderly sexuality continue to present major barriers to diagnosis and management. 26 Social expectations often invalidate sexual needs in the elderly, reinforcing the misconception that aging individuals should be asexual. This deep-rooted stigma discourages help-seeking behavior, fosters emotional suppression, and perpetuates mental health deterioration among older adults. 26
Also, discussed in Forbidden Fruit in the Golden Years, cultural denial of elderly sexuality leads to confusion, frustration, and feelings of isolation among the aging population. To overcome these embedded cultural hurdles, awareness campaigns and healthcare provider sensitivity are desperately needed. 26
Ignoring the elderly’s sexual health needs can lead to untreated dysfunctions that negatively affect their quality of life. More recognition and acceptance of sexual well-being as a crucial aspect of senior health is urgently needed. Guidelines also emphasize the need for doctors to actively ask about sexual health concerns in older patients because stigma and humiliation frequently discourage self-reporting. 27
Pharmacological Considerations
Clinical guidelines advocate a “start low, go slow” approach to pharmacotherapy in elderly individuals with sexual dysfunction. Due to age-related changes in pharmacokinetics and pharmacodynamics, careful measurement and monitoring are essential to ensure safety and efficacy. 6
Classification Updates
The classification of sexual dysfunctions has been impacted by updates to both the DSM-5 and ICD-10. In order to improve diagnostic clarity and decrease over pathologization, the DSM-5 offers gender-specific classifications and highlights the necessity of a minimum duration of symptoms (6 months) and frequency (75%–100%) for diagnosis.3,6
Impact on Quality of Life
Sexual dysfunctions can significantly harm one’s physical health, mental stability, relationships, and general quality of life. These disorders can affect people of all genders and ages and include issues with desire, arousal, orgasm, or pain. In relationships, sexual dysfunction can create tension and misunderstandings between partners, leading to frustration, inadequacy, or rejection, which can strain communication and intimacy. Unresolved issues can lead to broader relationship problems, such as decreased emotional connection and increased conflict over time. Individuals experiencing sexual dysfunction may struggle with feelings of shame or embarrassment, which can gradually destroy self-esteem. This diminished self-worth can extend beyond sexual encounters, affecting various aspects of life, including personal and professional relationships. The psychological impact of sexual dysfunction can be challenging on mental health. Individuals may experience anxiety, depression, or stress related to their sexual health. The fear of performance issues or the stigma surrounding sexual dysfunction can aggravate these mental health challenges, creating a cycle that is difficult to break. Anxiety can lead to increased stress levels, which may further impair sexual function, creating a vicious cycle.
Future Directions
The authors of this review recognize that the rates of occurrence and the presence of other psychiatric and medical conditions associated with ED and PE may vary due to differences in study design, measures used, location of the study population, and sample size. These variations can introduce biases that raise questions about the accuracy of the data and representation of reality. Hence, there is a need for conducting nationwide multicentric studies with consistent research designs, measures, population estimates, and analysis patterns to arrive at conclusive findings about the prevalence and comorbid conditions associated with ED and PE in Indian males. These findings can guide clinicians and researchers in developing comprehensive management and preventive approaches for these conditions.
Multidisciplinary Team Approach
A multidisciplinary approach is crucial for effectively addressing sexual dysfunction. This may involve partnerships with healthcare providers such as:
Primary care physicians: Assess overall health and refer patients to specialists as needed. Urologists or gynecologists: Address specific medical issues related to sexual function. Endocrinologists: Evaluate and treat hormonal imbalances. Pharmacological therapies: Provide necessary medical interventions.
Holistic Comprehensive Approach
A holistic approach involving mental health professionals such as psychologists or psychiatric social workers is essential to support the emotional, psychological, and psychosocial aspects of sexual dysfunction. Mental health conditions are among the leading causes of disease burden worldwide. The WHO reports India’s mental health issues burden at 2,443 disability-adjusted life years (DALYs) per 100,000 population, with a 21.1 suicide rate, and causing an estimated $1.03 trillion in economic loss between 2012 and 2030. 28 Education about sexual health, fostering a supportive environment, and encouraging open discussion or communication can empower individuals to seek help and improve their sexual health.
Lifestyle Modifications
Lifestyle modifications such as exercise, yoga, meditation, diet, weight management, stress management, and limiting alcohol intake can significantly impact sexual health and overall well-being. By integrating various treatment modes, healthcare providers can create a personalized treatment plan that addresses the unique needs of each individual. By tackling these issues, individuals can improve their quality of life, strengthen their relationships, and foster a healthier self-image.
Limitations
This review has several limitations due to the scarcity of studies on sexual health in India, regional differences, and cultural taboos that prevent open discussions on the topic. The lack of research material makes it challenging to obtain a comprehensive overview of sexual health in India, highlighting the need for further investigation. Furthermore, regional variations in the prevalence of sexual dysfunctions within India make it difficult to generalize findings across the country. Additionally, cultural inhibitions surrounding sexual health discussions contribute to fragmented data, limiting the depth and breadth of this review. Obtaining representative sample sizes and addressing high dropout rates are also challenging tasks that complicate understanding the intricacies of sexual health in India’s diverse landscape.
Conclusion
Sexual health is crucial for overall well-being and quality of life. In India, sexual dysfunction is common and complex, influenced by physiological, psychological, and cultural factors. The high rates of PE and ED underscore the need for standardized research and multidisciplinary approaches. Addressing these issues requires destigmatizing discussions about sexual health, investigating comorbid conditions, and implementing targeted interventions that include elderly population. A holistic approach involving medical and mental health professionals can improve sexual function and quality of life, emphasizing the importance of further research and enhanced healthcare strategies in India.
Footnotes
Authors’ Contribution
Subrahmanaya Bhat and Pradeep Kumar PC helped in concept and design, literature search, drafting of the manuscript, critical review and verification of the manuscript for important intellectual content, acquisition, analysis, or interpretation of data.
Manoj K Pandey contributed to concept and design, drafting of the manuscript, critical review and verification of the manuscript for important intellectual content, acquisition, analysis, or interpretation of data.
T. S. Sathyanarayana Rao helped in critical review and verification of the manuscript for important intellectual content, acquisition, analysis, or interpretation of data.
Udayakumar K contributed to critical review and verification of the manuscript for important intellectual content.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TS Sathyanarayana Rao is a member of the Editorial Board of the Journal of Psychosexual Health. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Ethical Approval
The study approved by institutional ethics committee (JSS/MC/PG/6722/2023-24).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable, as this study is a narrative review and did not involve direct participation of human subjects.