
Abstract
Good communication within the family shapes an individual’s behavior, choices, and beliefs. Sexual communication between parents and children is important as it affects children’s sexual and reproductive health (SRH) behavior, choices, development, and values. However, SRH is a domain of discussion that is often avoided due to the social stigma attached to it. This article aims to understand the influence of family communication patterns (FCP) on the amount of family sexual communication (FSC) through a comparative research design. The data was collected from 134 parents (64 fathers and 70 mothers) of children aged 13–19. The Revised FCP and Weighted Topics Measure of FSC were administered. Kruskal-Wallis H test and Mann-Whitney U tests were used to analyze the influence of the FCP and parent-gender on the extent of FSC. A significant influence of FCP and parent-gender on the amount of FSC was found. Results indicate that pluralistic FCPs have the highest amount of FSC, and mothers were found to be engaging in FSC more than fathers. It is recommended to develop programs aimed at increasing conversation-oriented family communication within families as it has a positive influence on the extent of FSC between parents and children.
Keywords
Introduction
The World Health Organization 1 defines sexual health as “a state of physical, emotional, mental, and social well-being concerning sexuality; not merely the absence of disease, dysfunction, or infirmity.” Sexual health is a complex domain affected by a myriad of interconnecting factors of an individual’s nature and nurturance. In the discourse surrounding sexual health education, there is an ongoing debate regarding whether the primary responsibility lies with schools or parents. It is reported that the teachers are not comfortable engaging with students on matters of sexual health and related issues. 2
The National Education Policy (NEP) 2020 in India does not specifically address “sex education” in its official documentation, although it was included in the 2019 draft. Nevertheless, it underscores the significance of an education that encompasses subjects about sexual and reproductive health (SRH) within a broader well-being curriculum.3,4 Two consecutive administrations in India have struggled with the matter, as conversations in the public sphere regarding this subject often draw influence from religious, social, and cultural values, with limited focus on scientific perspectives. 5 The fear of enabling “sexual anarchy” or “moral decadence” has actively hampered any attempts by legislative bodies to improve this. 6
The SRH needs of adolescents in India are currently neglected or not adequately understood within the healthcare system. 7 No data is available on the percentage of adolescent girls and young women who make informed decisions about sexual relations, contraceptive usage, and reproductive health care in India. Making informed decisions, reporting Sexually Transmitted Infections (STI)s, age of first sexual intercourse, and usage of contraceptives are considered indicators of SRH behaviors while profiling the health of adolescents. 8
International literature on adolescent sexual health reveals behavioral trends toward the initiation of sexual intercourse among late adolescents, often linked to sexual risk-taking behaviors due to a lack of general awareness, mainly regarding contraception, and the perils of sexual abuse.9–11 A 2019 survey study reported that the one-year prevalence of child sexual abuse in Kerala, India, is 16.7% and the rate of abuse was found to be higher among families with a history of alcohol abuse. 12 It also reported that boys have a higher rate of sexual abuse than girls, and the socio-cultural factors cause significant underreporting of cases. 12 This is worsened by the fact that prevalent systems do not provide an environment conducive for men to speak of being the victim in such cases. 13 The need to maintain a “macho demeanor” hinders their ability to feel safe while discussing such matters openly. 6 Many times, not knowing what consent, gratification, and desire mean, these behaviors are significantly influenced by social and contextual factors, closely tied to issues such as peer pressure, alcohol consumption, and obvious gender power dynamics.
Parents play a crucial role as significant protective factors in the health of adolescents. They substantially impact shaping their children’s general attitudes and behaviors related to health, including SRH. 14 Parents concur that it is essential to impart sexual health information to their children, but socio-cultural and internal family practices and norms. 15 In a collectivistic culture, such as India, open conversations about sexual health and sexuality are not encouraged.16,17 A review article across various countries observed that communication between parents and adolescents on sexual matters is not frequent, lacks detail, and is often of poor quality when it does occur. 18 Talking about sexual intercourse and contraceptives leads to feelings of discomfort and embarrassment, making it challenging for both parents and children to have open discussions on these subjects. 19 Adolescents often rely on close friends or the internet for sexual information, which may not always be reliable, exposing them to various health risks. Consequently, it is crucial to provide appropriate support and services to ensure adolescents receive accurate and reliable information. 20 A dyadic analysis study revealed greater alignment between mothers and their children in reporting Sexual Health Conversation (SHC) compared to fathers and their children, suggesting a potential need for additional resources to facilitate fathers in effective sexual health conversations with adolescents. 21
In comparison to adolescents, parents commonly present a more optimistic portrayal of their sexual communication with their adolescents. 18 In 2023, it was reported that the majority of adolescents and their parents never engaged in SRH-related communication, or it was unsatisfactory concerning frequency and quality. 14 As a result, the authors suggested that establishing a conducive home environment for adolescents and organizing awareness programs in collaboration with local government authorities for respective schools, it could contribute to enhancing communication between adolescents and parents.
Family communication patterns (FCP) theory suggests that the family’s communication style is linked to various factors, such as family unity, style of parenting, values, and the behavioral and psychological impact on children. Likewise, family communication practices impact the socialization of interpersonal behaviors through conversational or conformity communication within the family structure. 22 The analysis revealed two family communication types, namely protective and pluralistic, derived from scores on conversation and conformity orientations. A recent study explored FCP and discovered that the correlation between conversation and conformity orientation had a connection to adolescent sexual self-efficacy and their intentions to discuss sex with their partners. 23 In families with high conversation and low conformity, adolescents displayed notably higher sexual self-efficacy in comparison to other FCP.
This article aimed to explore the influence of FCP on the amount of family sexual communication (FSC) between Indian parents and their children. Parents, schools, health care institutions, mental health professionals, and non-government organizations working with this population could benefit from the results of the study in identifying the influence of FCP on sexual communication and interventions that can be used to capacitate parents to break through unbeneficial FCP and build a healthy, accepting, safe, and encouraging environment for children of all genders and sexual orientations.
Materials and Methods
Non-experimental comparative research was conducted on the married parents of adolescents aged 13–19. Responses were obtained through a convenience method of sampling. A sample size of 134 was considered out of the total number of responses of 146. The socio-demographic details of the population were collected through a basic questionnaire that included the parents’ gender, age, marital status, educational qualification, occupational status, gender of the children, religion, and religiosity. Religiosity is measured on a Likert item indicating how important religion is in one’s life. Ranging from very unimportant (0) to very important (4). The Revised Family Communication Pattern Instrument 24 was used to measure FCP. It is a 26-item Likert scale measuring two underlying dimensions of FCP: Conversation orientation (15 items) and Conformity orientation (11 items). To measure the amount of FSC, the Weighted Topics Measure of Sexual Communication 25 was used. It objectively measures the amount of communication about sexuality that has occurred between parents and their adolescent children.
The questionnaire was distributed among parents known to the researcher. The nature of the study was explained, and informed consent was collected from the participants. Fifty-five percent of the data was collected online using Google Forms, and the remaining through in-person reporting. The data was filtered to ensure the inclusion and exclusion criteria were met and processed with Microsoft Excel. The analysis was carried out using SPSS version 20. Precautionary measures were taken to ensure confidentiality was maintained at all stages of data collection and analysis. Mean, median, mode, and standard deviation were estimated. The normality check was carried out using the Kolmogorov-Smirnov test to find out the normal distribution and Levene’s test for homogeneity of error variances within the sample. The assumption of normality and homogeneity in error variances was found to be violated in the collected sample. The influence of FCP and the gender of the parent on the amount of FSC was analyzed using Kruskal-Wallis H and Mann-Whitney U tests, respectively.
Results
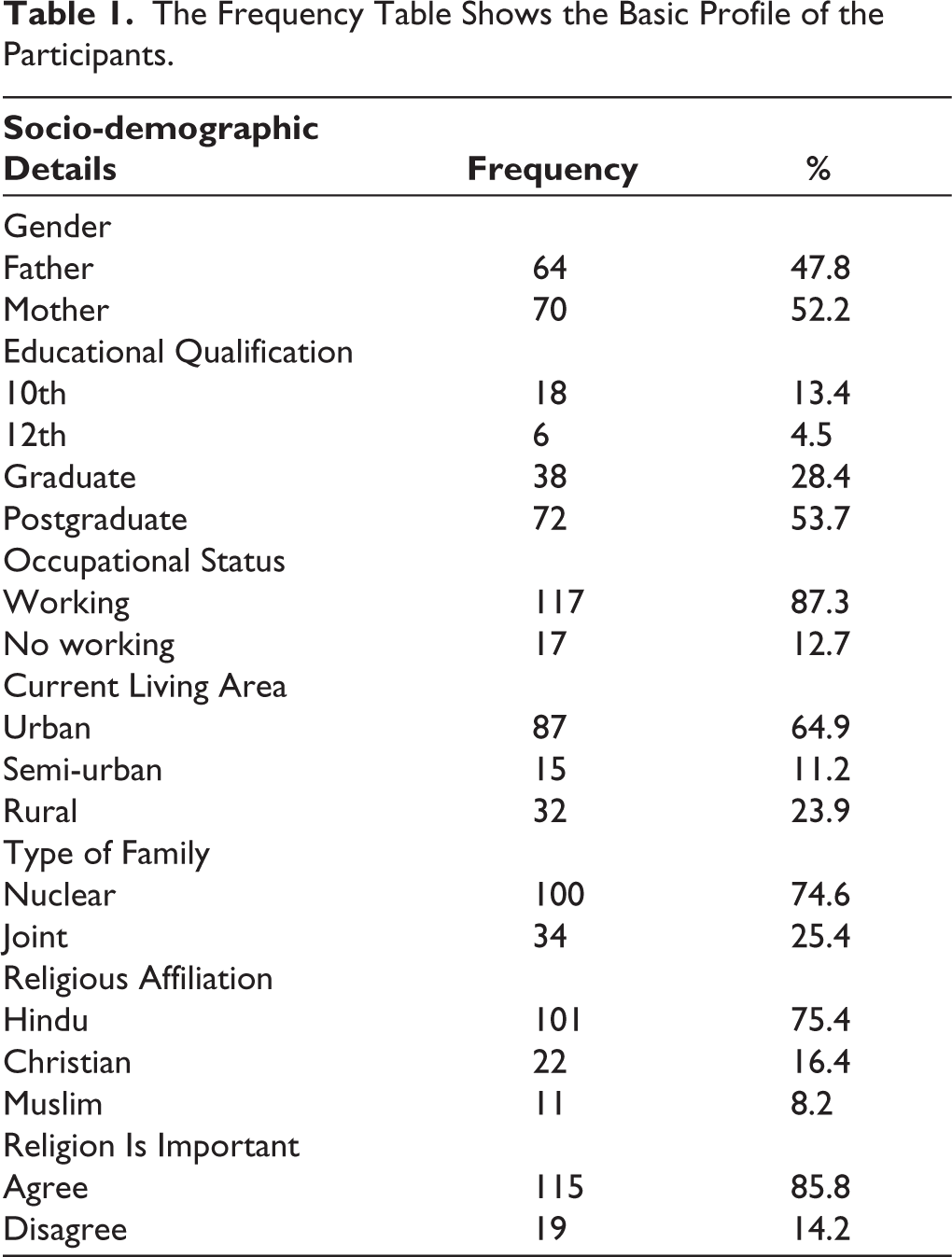
Table 1 shows the socio-demographic details of the sample studied. Out of the current sample (N = 134), fathers make up 47.8% of the total responses, and mothers comprise 52.2% of the responses. Concerning educational qualification, a major part of the population (53.7%) has attained postgraduate degrees, 28.4% have obtained graduate degrees, 4.5% have completed only 12th grade, and 13.4% have completed 10th grade. 87.3% of the sample are working, and 12.7% are not working. Among the total samples, 64.9% of the sample currently live in urban areas, 11.2% in semi-urban areas, and 23.9% in rural areas. Out of the total samples of the current study, 74.6% of the respondents are from nuclear families and 25.4% are from joint families. It was found that 75.4% of the sample practiced Hinduism, followed by 16.4% with Christianity and 8.2% with Muslim. Among the total participants, the majority (85.8%) agreed that religion was important. There is a visible indicator of their beliefs about the importance of religion among the sample.
The Frequency Table Shows the Basic Profile of the Participants.
The results in Table 2 indicate that the amount of FSC data is not normally distributed as the Kolmogorov-Smirnov test statistic (0.171) is significant (P = .000). Similarly, the Levene’s test (Levene statistic 7, 126 = 3.131) is significant (P = .004), which indicate that the variances of the four groups are significantly different; that is, they were not homogeneous. Hence, it was concluded that both the assumption of normality and the homogeneity of variance are violated. Hence, instead of the ANOVA, non-parametric tests such as the Kruskal-Wallis H test and Mann-Whitney U test were run to find out the influence of FCP and gender of the parent on the amount of FSC between parents and adolescent children, respectively.
Normality and Homogeneity Test for the Amount of Family Sexual Communication (N = 134).
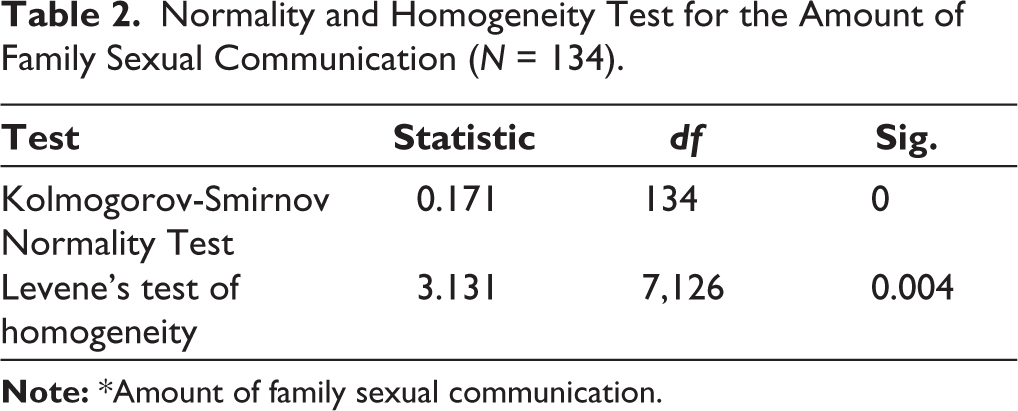
Table 3 shows the mean ranks of the amount of FSC for the four different FCPs. From the sample (N = 134), parents with pluralistic FCP (n = 35) have a mean rank of 81.99, Consensual FCP (n = 46) have a mean rank of 66.48, protective FCP (n = 43) have a mean rank of 60.09, and laissez-faire FCP (n = 10) have a mean rank of 53.35. Parents with pluralistic FCP have the highest mean rank for the amount of FSC. The Kruskal-Wallis H test revealed a statistically significant difference, Kruskal-Wallis H (3) = 7.90, P = .048 at the .05 significance level. Hence, the research hypothesis stated as “there is a significant influence of FCP on the amount of FSC between parents and adolescent children” has been accepted.
Mean Rank Table and the Test Statistic for the Kruskal-Wallis H Test.

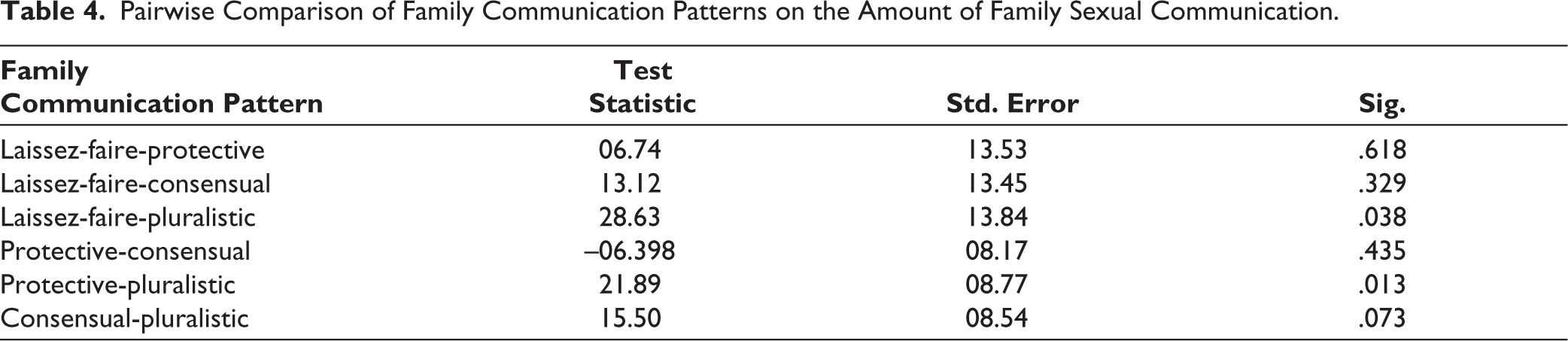
Further, the pairwise comparison revealed that Protective FCP and Pluralistic FCP (Z = 21.89) show a statistically significant difference at the .05 level of significance (P = .013). From Table 4 and Figure 1, it is observed that pluralistic FCP has a higher mean rank (81.99) than protective FCP (60.09). Laissez-faire FCP and pluralistic FCP also show a statistically significant difference (Z = 06.74) at the .05 level of significance (P = .038), in which pluralistic FCP has a higher mean rank (81.99) than laissez-faire FCP (53.35).
Pairwise Comparison of Family Communication Patterns on the Amount of Family Sexual Communication.
Pairwise Comparison Plot of Family Communication Pattern on the Amount of Family Sexual Communication.
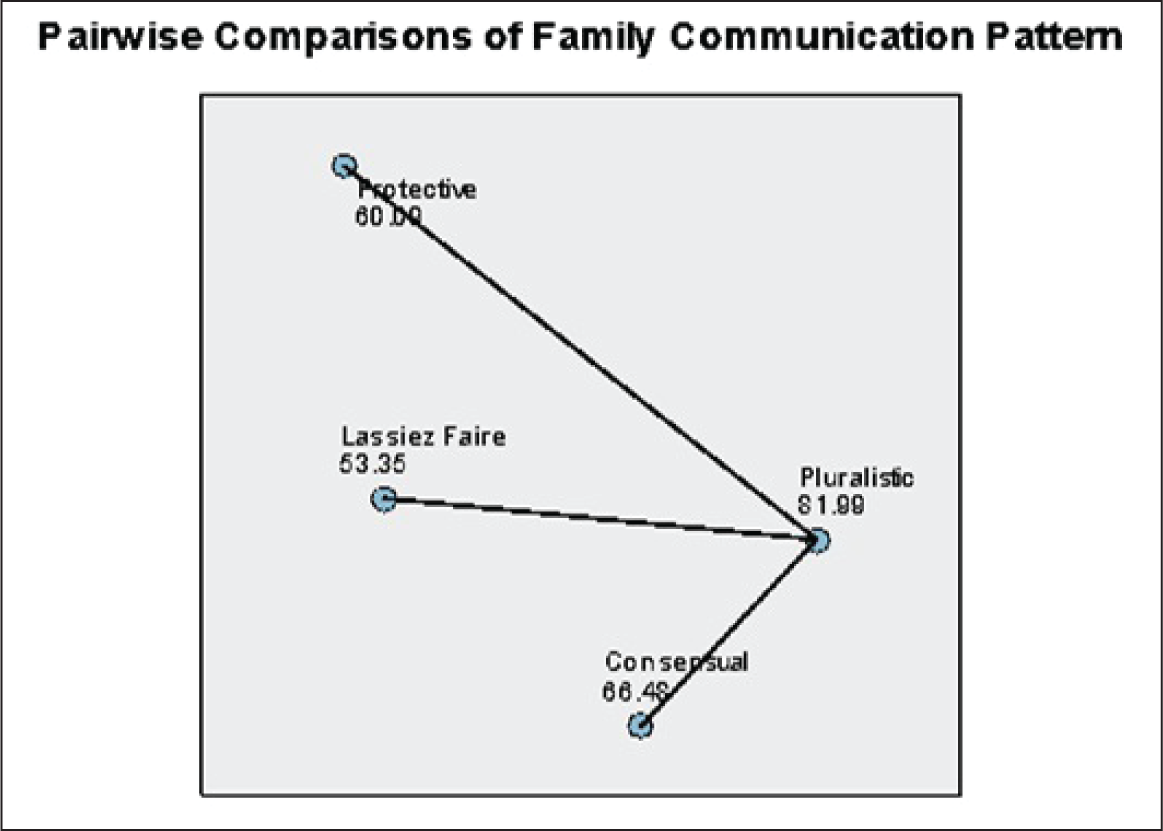
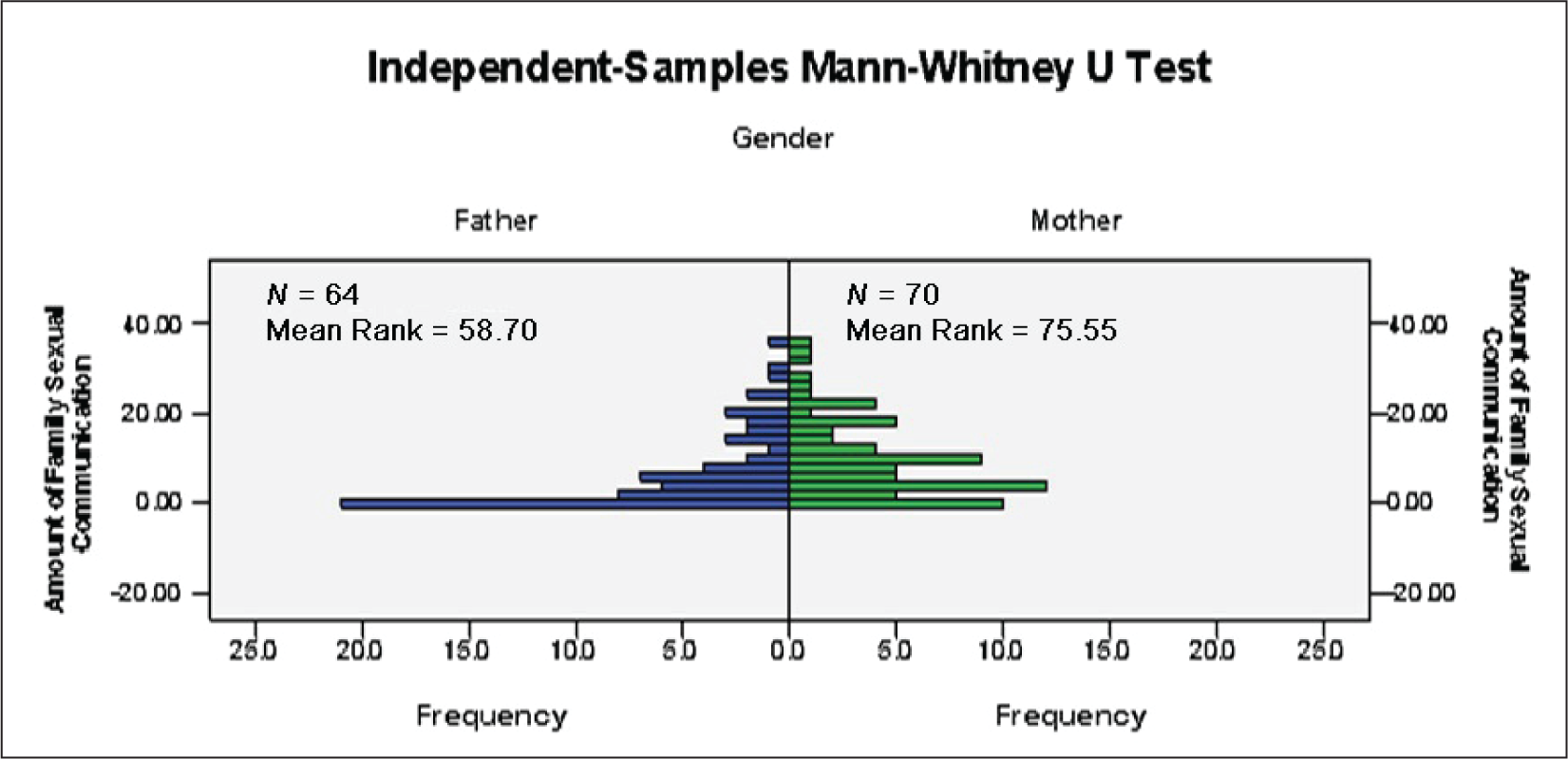
Table 5 shows that the mean ranks of the amount of FSC for mothers (n = 70, mean rank 75.55) are higher than for fathers (n = 64, mean rank 58.70). The Mann-Whitney U test results indicated that there is a significant difference in the amount of FSC between mothers and fathers, U = 1676.50, Z = −2.52, P = .011 at the .05 significance level. Figure 2, the graphical representation of the same, indicates a clear increase in the frequency of fathers who scored low on the weighted topics measure of FSC. Hence, the research hypothesis stated that “there is a significant influence of the gender of the parent on the amount of FSC between parents and adolescent children” has been accepted.
Mean Rank and the Test Statistic for the Mann-Whitney U test.

Graphical Representation of the Difference in the Amount of Family Sexual Communication Between Mothers and Fathers.
Additionally, descriptive analysis of the responses to the weighted topics measure was conducted to understand the preferences of the parents on nine topics, such as pregnancy, fertilization, intercourse, menstruation, sexually transmitted diseases, birth control, abortion, prostitution, and homosexuality. The results are discussed below.
Figure 3 shows the responses of parents concerning the amount of FSC for each of the nine topics. It is found that the most talked about topic is menstruation, with 67.9% of the parents engaging in menstruation-related communication with their children, followed by pregnancy at 56.7%. The least talked about topics are intercourse (28.4%), followed by birth control (33.6%) and homosexuality (37.3%). Seven out of the nine topics recorded over 55% under the “Not at all,” which reflects as overall tendency of the sample to have low FSC.
Responses of Parents to the Weighted Topic of Family Sexual Communication.
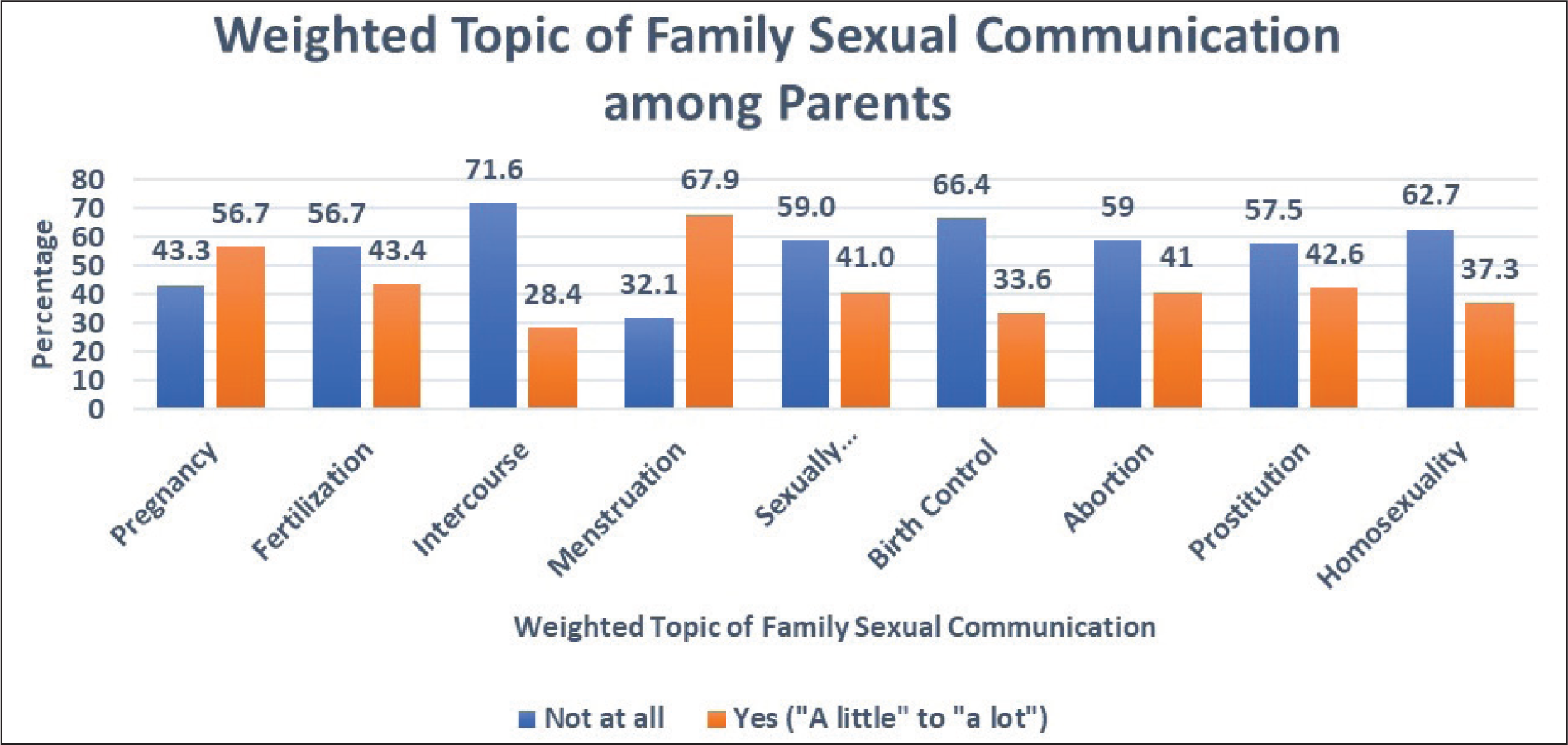
Figure 4 is a graphical representation of the fathers’ responses to the amount of FSC for each of the nine topics in percentage. It is found that the majority of the responses lean toward no communication of all nine FSC topics. All nine topics recorded over 50% “Not at all” responses. None of the nine topics seems to be favored by fathers. However, among the nine topics, fathers were engaged in communication more on menstruation (48.5%) and pregnancy (56.9%), respectively.
Responses of Fathers to the Weighted Topic of Family Sexual Communication.
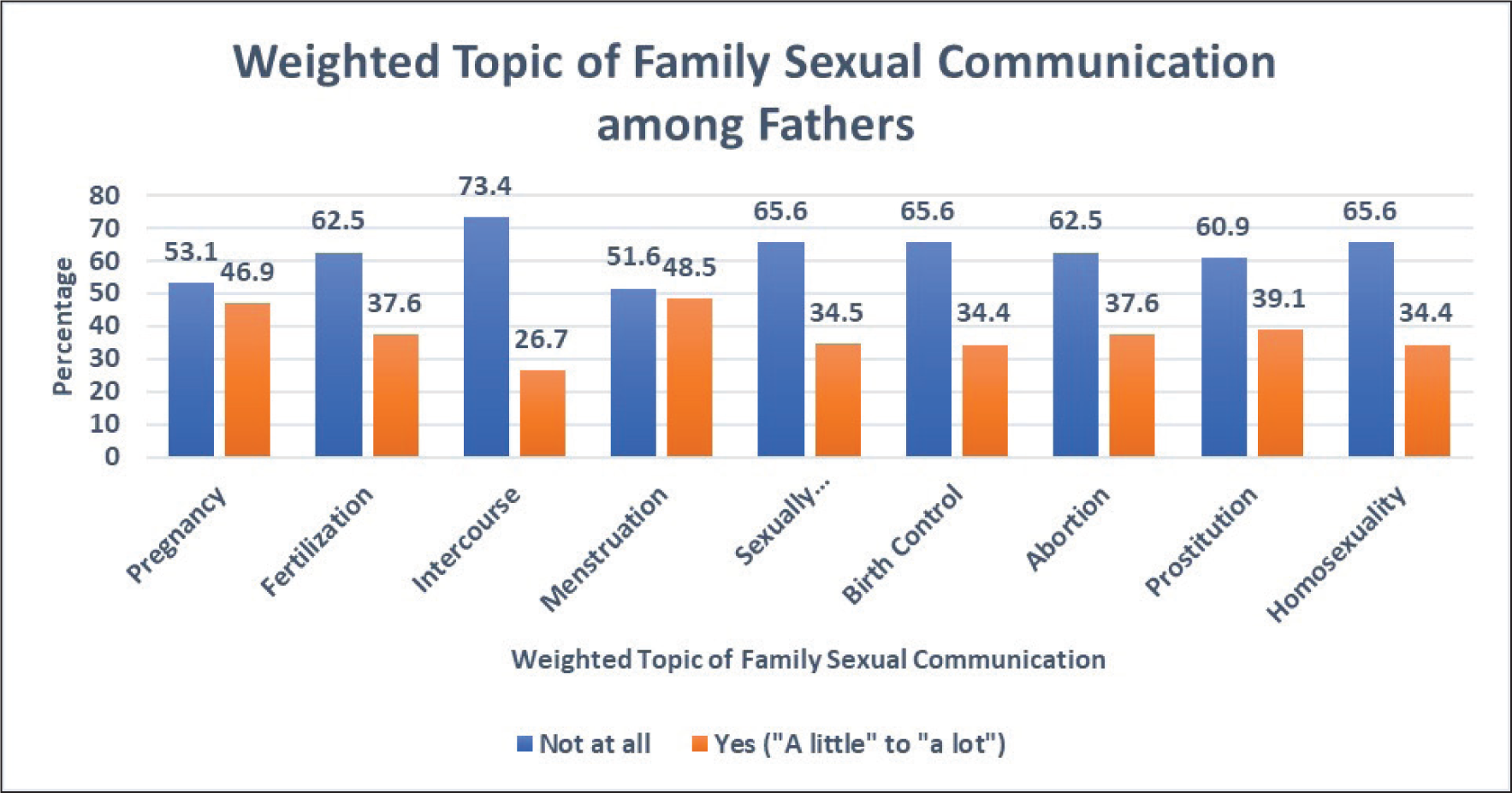
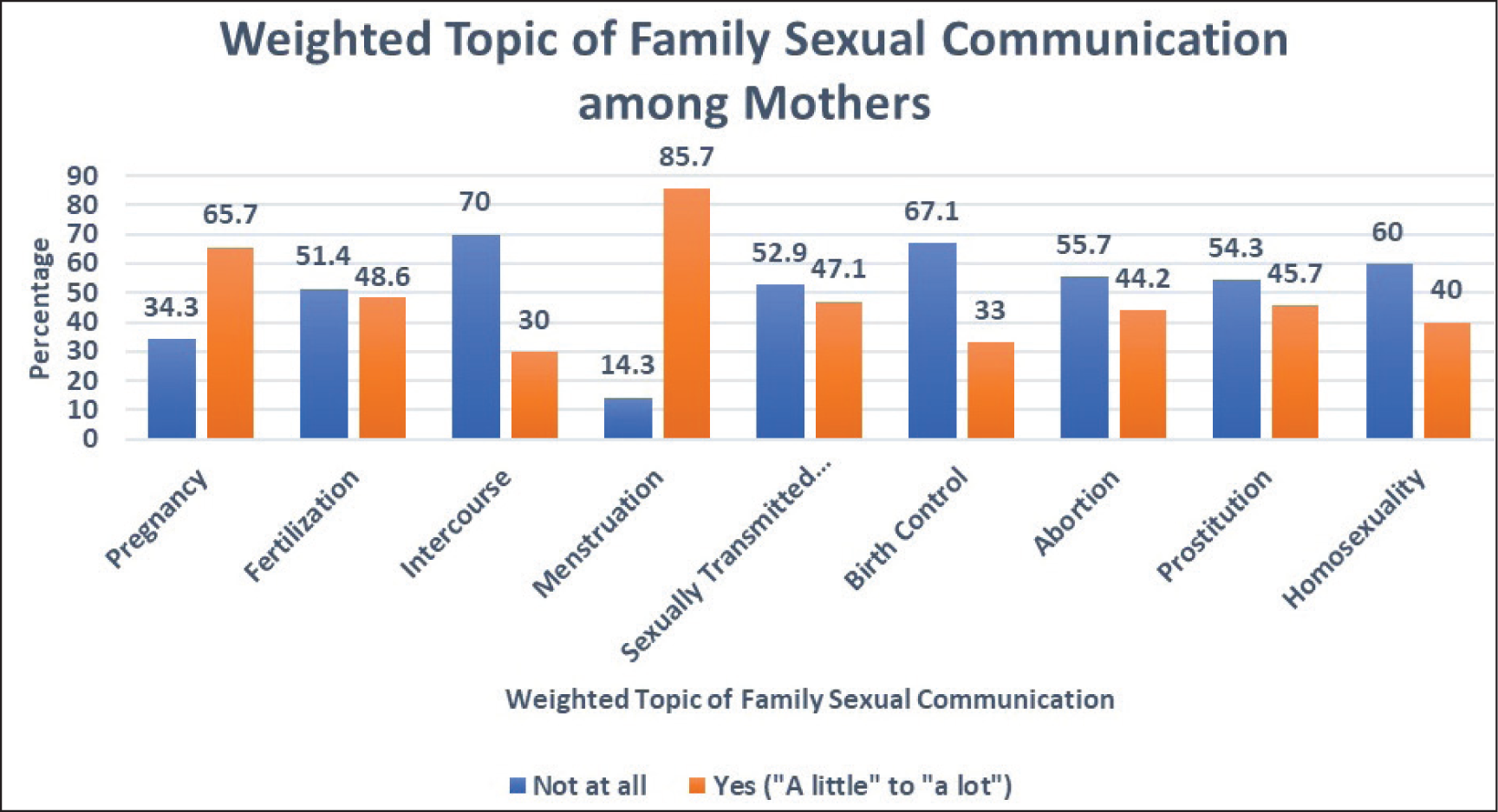
Figure 5 is a graphical representation of the mother’s responses to the amount of FSC for each of the nine topics in percentage. The most favored topic of FSC among mothers was menstruation (85.7%), followed by pregnancy (65.7%). The other seven topics showed over 50% of the sample answering “Not at all.” The least discussed topics by mothers are intercourse (30.0%) and birth control (33.0%).
Responses of Mothers to the Weighted Topic of Family Sexual Communication.
Discussion
The sample selected for this study was married, Indian parents of teenagers aged 13–19 years. The age group was carefully selected based on the fact that adolescents are more susceptible to SRH challenges 14 and the presence of a significant lack of awareness and interest among teenagers. 26 Among 134 Indian parents from urban, semi-urban, and rural areas of the country, 70 (52.2%) were mothers and 64 (47.8%) were fathers.
The descriptive analysis of the sample’s response to the weighted topics measure of FSC shows in detail that the sample of Indian parents have a significant hesitation in engaging with their adolescents on topics related to SRH. A recent study in Nepal among adolescents found similar findings as the parents were never engaged in any SRH-related communication, nor were they unsatisfied with SRH-related communication with them. 14
The major finding of this study was that the FCP has a significant influence on the amount of FSC between parents and adolescent children. The descriptive statistics indicated that parents with pluralistic FCP have a higher amount of FSC than parents with consensual FCP, protective FCP, and laissez-faire FCP, respectively. This finding was in line with the observation from a recent study among USA adolescents that in families with high conversation and low conformity (pluralistic FCP), adolescents displayed notably higher sexual self-efficacy in comparison to other FCP due to better sexual communication. 23 The pairwise comparison pointed out a significant difference between the pluralistic and protective FCP and the pluralistic and laissez-faire FCP.
The second gender of the parent indicated a significant influence on the amount of FSC between parents and adolescent children, and here, mothers were seen to have significantly higher FSC than fathers. This was supported by the literature, which indicates greater sexual health conversation between mothers and their children compared to fathers and their children, and suggested potential interventions to facilitate fathers in effective sexual health conversations with adolescents.21,27 However, a 2012 study in Punjab reported that among parents and teachers, fathers had shown a favorable positive attitude toward sex education for adolescents. 28 Nevertheless, multiple research findings indicate that mothers engage in more FSC with their adolescent children compared to fathers.21,27 Another study observed that males were more withdrawn and showed contempt, receiving more directive messages from their mothers during parent-child sexual communication, while females were more expressive and engaged in more mutual exchanges with their mothers. Responses to their study noted a preference for same-gender discussion among adolescents. 19
In literature, it was also noted that a gendered pattern in how SRH information is discussed in families. 27 When asked about body changes, more female adolescents from Uganda reported discussing these topics with their mothers. Conversations about SRH were often gendered, with girls receiving more cautious guidance. Culturally, fathers were not expected to discuss puberty-related issues with their daughters, and most discussions on female adolescents’ SRH took place in women’s social spaces. 27 Fathers’ conscious and deliberate involvement in discussing these topics, especially with their sons, is necessary. In conclusion, the sexual health communication between parents and children is less in terms of its frequency, quality, and types of information to be communicated, which was again reported in various studies across countries. 18
Other major findings from this study were that menstruation and pregnancy were the most common topics that were discussed between parents and children, while intercourse, birth control, and homosexuality were the least discussed or never discussed topics. This was again in line with the existing literature, as religious morality inhibits the conversation about these topics in the family. 29 A qualitative study among emerging adults in the USA reported that the discussion on sexual intercourse and contraceptives with parents leads to discomfort and embarrassment, and it is a challenging process for both parents and children to have open discussions on these subjects. 19 Another study observed that the SRH-related communication on abstinence, safe sex, and HIV/AIDS was negatively related to parents’ comfort level. 30
In India, sexuality and reproductive health continue to be viewed as taboo subjects due to entrenched cultural, traditional, and religious beliefs. The absence of reliable information and minimal communication about SRH with trusted adults often forces adolescents to turn to unsafe sources, both online and offline, potentially harming their physical and mental well-being. 31
The major finding of this study implies that a pluralistic FCP (high conversation orientation and low conformity orientation) is comparatively more ideal for better FSC. One of the strengths of the FCP theory is that it is based on a cognitive model. 32 Unlike other family typologies, this theory explains how families create a shared social reality through co-orientation, which is the process of arriving at similar beliefs, attitudes, and perceptions through communication. This opens up the scope for research in interventions to increase conversation orientation and decrease conformity orientation, which leads to pluralistic FCP among not only parents but also any role that requires interacting with adolescents and struggles with sexual communication. The perpetuation of low conversation and high conformity is reflected in school teachers, healthcare workers, and society at large, which again has a negative influence on open sexual communication with children. Hence, it is important to develop a working and practice model in the area of SRH-related communication in the family, school, and community at large. Also, more emphasis is required on developing and providing training programs on SRH topics among parents, with more focus on fathers.
There are a few limitations observed in this study. First, the sample was limited to 134 participants and was mostly restricted to southern India. The distribution of the sample on other socio-demographic specifics, such as current living situation, type of family, annual income, and religious affiliation, was not significant enough to identify any additional influences on the amount of FSC. The second limitation is that the study could not include the subjective narratives of the participants and their personal experiences. The perspectives of parents on sexual health communication in the family would add more value to the findings and literature. Quantitative data alone may not be enough to subsume the nuances and variations in the family dynamics and their voices coming as a result of a multitude of socio-demographic variables that are inevitable in such a gendered topic as sexual health.
Conclusion
The findings of this study summarized that both FCP and the gender of the parent have a significant influence on the amount of FSC between the parents and adolescent children in Indian families. The parents with pluralistic FCPs (high conversation and low conformity orientation) and mothers have significantly higher amounts of sexual communication than parents with other FCPs and fathers, respectively. Among the domains of sexual communication, menstruation, and pregnancy gained the most attention from parents, while intercourse, birth control, and homosexuality were rarely discussed in Indian families. These results indicate the need to develop new practice models to conscientize the families about the need to enhance FCP to a pluralistic model, and normalize sexual communication, including all the domains. The study recommends further innovative research and interventions on sexual communication and SRH aspects within families, considering all other extraneous factors with a large and representative sample from various socio-cultural backgrounds.
Footnotes
Authors’ Contribution
All four authors have significantly contributed to the study’s conception and preparation of the study protocol. The first author collected the data and processed it under the guidance of the second, third, and fourth authors. All four authors have participated in the quantitative data analysis. The first author has prepared the first draft of the manuscript with relevant literature and theoretical evidence. All four authors have read the manuscript and revised and approved the final version. The authors declare that there is no conflict of interest in the overall process.
Consent to Participate
All the participants gave written informed consent to participate in this study before the data collection.
Consent to Publish
The consent to publish was obtained from the participants and is kept confidential under the custody of the first author.
Data Availability Statement
Upon request, anonymized data will be provided by the first author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No generative AI tools were used for this manuscript to collect or gather data, produce images or graphs, or write the manuscript. Authors assume full responsibility for the entire content of the manuscript.
Ethical Approval
This is a part of the dissertation of the first author’s postgraduate course. It was obtained from Research Advisory Committee (RAC), IIPR, Bangalore, in February 2024.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
The present study, entitled “Influence of FCP on Amount of Sexual Communication among Parents,” was carried out as part of the academic requirements of the postgraduate course in psychology at the Indian Institute of Psychology and Research, Bangalore. The research project was conducted by Gopika Surendran under the guidance of faculty supervisors of IIPR. Participants were requested to give their voluntary consent to participate in the study. Any information collected during the process was kept confidential and used strictly for research purposes. Participants were free to withdraw from the study at any time without any prejudice. Each participant provided written informed consent before participation, confirming that they had read the information carefully and agreed to take part in the study.