
Abstract
Introduction:
The gap between cognitive-psychosocial development and physical-sexual maturity in children with intellectual disability (ID) can result in inappropriate sexual behaviours, leading to negative social and legal consequences. Parents are unaware of such behaviours and may resort to punishment or feel guilty of these behaviours. While sex education has been proposed as a solution, no studies in India have thoroughly examined sexual behaviours in individuals with ID or caregiver attitudes toward these behaviours.
Aims and Objectives:
To assess the types and frequency of sexual behaviours in individuals with ID and caregiver attitudes towards them.
Methods and Materials:
It was a cross-sectional study conducted after approval from the Institutional Ethics Committee, which included 100 patients with ID and their caregivers. Sociodemographic details of caregivers and individuals with ID were collected. Two questionnaires were administered: one assessed sexual behaviours, and the other explored caregiver attitudes on topics like sexual education, concerns about sexual abuse, dating and intimacy. Data was analysed using mean, standard deviation and frequency, as required.
Results:
Masturbation was the most frequent behaviour (37%), followed by consumption of pornography (33%) and undressing in public (33%). Inappropriate touching (13%), voyeurism (14%) and explicit conversation (9%) were less frequently reported. Our study found that only 40% of caregivers believed sex education was important, while over half felt discussing sexuality might encourage inappropriate behaviour. Just 26% of caregivers had discussed sexuality with their ward, and 64% believed dating and intimacy should not be allowed.
Conclusions:
Inappropriate sexual behaviours are prevalent among individuals with ID, and caregiver attitudes reveal a lack of acceptance and reluctance to address sexual education, exacerbated by cultural taboos in India. The study’s findings can guide the development of tailored intervention programmes to address sexual behaviour in individuals with ID in the Indian context.
Introduction
Intellectual disability (ID), as per the Centres for Disease Control and Prevention, is a neurodevelopmental disorder that involves early childhood deficits in intellectual and adaptive functioning. 1 It may be classified based on intelligence quotient (IQ) as mild (51–70), moderate (36–50), severe (20–35), or profound (<20). 2 Individuals with ID have delayed cognitive development. Despite this, their range of sexual needs, urges and desires is similar to others of their age. 3 This gap between their cognitive-psychosocial development and physical-sexual maturity, accompanied by a lack of appropriate sex education for such children, may lead to the display of inappropriate sexual behaviours by them. 4 Sexual behaviours of concern include behaviours such as public masturbation, exhibitionism, voyeurism, touching private body parts of another person or discussing inappropriate sexual subjects.3,5
Individuals displaying such behaviour will consequently have an increased risk for coming in contact with the criminal justice system, or may encounter negative social consequences, restricted community access and barriers to independence. Previous studies have suggested the use of intervention programmes such as behavioural skills training to tackle this challenging behaviour. Appropriate sexual education for those with ID as well as for their caregivers has also been suggested as a prevention and rectification measure. 6
Unfortunately, very few studies worldwide, and none in India, have been conducted to research in depth the prevalence, types and frequency of sexual behaviour in adolescents and individuals with ID. Additionally, in India, little is known about the attitudes and concerns of the parents of these children towards their child’s sexual behaviour. This study aims to analyse the type and frequency of different sexual behaviours exhibited by individuals who have ID and to assess the attitudes of parents or caregivers towards these behaviours.
Methodology
This cross-sectional study was conducted in the Psychiatry Out-Patient Department of a tertiary care hospital over the course of 12 months after obtaining approval from the Institutional Ethics Committee (IEC/359/23). All consecutive participants seeking treatment for ID were invited to participate in the study. The convenience sampling method was applied, and the sample size was taken as 100. Individuals 10 years and above, having an established diagnosis of ID with a reliable primary caregiver above 18 years of age, were included in the study after taking written informed consent from the caregiver. Primary caregivers having a diagnosed case of any psychiatric illness were excluded from the study.
The study began by acquiring demographic details of the parent/caregiver and the individual with ID. The IQ of the participant was also measured using the Binet-Kamat Test of Intelligence. The Binet-Kamat Test is the Bombay-Karnatak version of the Binet-Simon Intelligence Scale and was administered by a trained psychologist. Measured IQ was then graded into the following categories: Mild (52–75), moderate (36–51), severe (20–35), and profound (<20). 2 Two questionnaires were used to collect further data.
Questionnaire A
The first questionnaire was to assess the types and frequency of sexual behaviour displayed by individuals who have ID. It was a semi-structured questionnaire that was based on the book ‘Age-Appropriate Sexual Behaviours in Children and Young People’ published by the South Eastern Centre Against Sexual Assault and Family Violence (SECASA). 7 It was validated by three psychiatrists and three psychologists of a tertiary health care centre and designed to be administered to the parents of individuals with ID. Behaviours assessed included the following aspects: masturbation in public and private, exhibitionism, voyeurism, accessing sexually themed content online, engaging in sexually explicit conversation or acts, and inappropriately touching other people.
The frequency of each behaviour was assessed as ‘Never’, ‘Often’ and ‘Rarely’. The terms were categorised based on the following:
8
No display of such behaviour in the past: ‘Never’ Display of such behaviour at least once per week: ‘Often’ Frequency between the two extremes: ‘Rarely’
Questionnaire B
The second questionnaire was to assess the attitudes of parents/caregivers to the sexual behaviour of the individual with ID. It was a semi-structured questionnaire that had been adapted and formulated after review of several similar research papers.9–11 It was also validated by three psychiatrists and three psychologists of a tertiary health care centre. Aspects assessed by the second questionnaire included parental attitudes to the display of sexual behaviour, importance of sex education, concern of sexual abuse, presence of sexual needs, desires and impulses, dating, marriage and intimacy.
Data collected was entered into an Excel sheet, following which it was subjected to appropriate statistical analysis using computerised software. Analysis was done by calculating the mean and standard deviation for quantitative data and frequency and percentages for qualitative data.
Results
Table 1 shows the sociodemographic details of the informant as well as the child (N = 100). The age of the informant ranged from 18 to 77 years, with a mean of 46.37 years. 51% of informants were male, while 49% (n = 49) of the informants were female. 87% of them were married and more than half of them were employed. The mean age of the ID individual was found to be 22.94 ± 7.39 years. Our study had more male ID population than females. 64% of them belonged to the mild ID category, 27% of them had moderate ID, and 9% belonged to the severe ID category.
Demographic Details of Study Population.
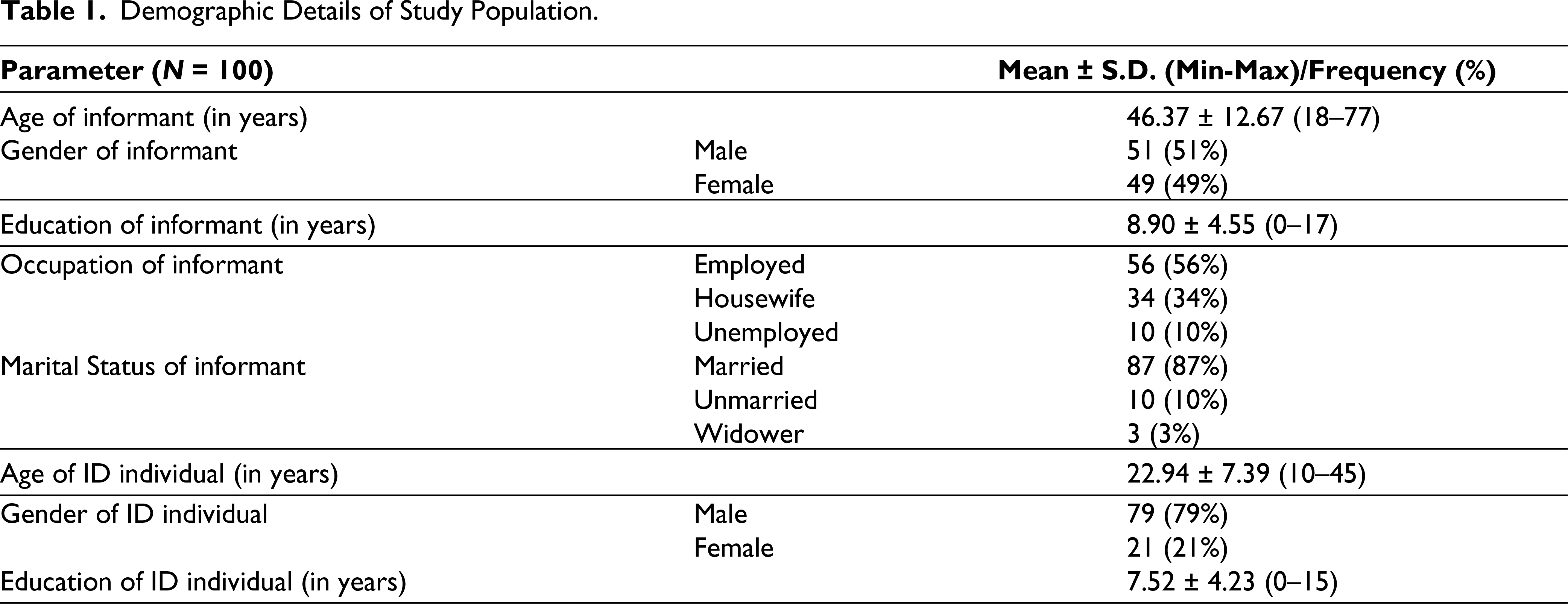
Table 2 shows the prevalence and types of sexual behaviour exhibited by individuals with ID. The most frequently observed behaviours were masturbation, with 19% exhibiting it often and 18% exhibiting it rarely. Many had been accessing pornographic content or sexually explicit media as well (15% of them often and 18% rarely). Caregivers reported that several participants often undressed in public or enjoyed being nude, the total frequency of which was found to be 33% (14% often and 19% rarely). Sexual behaviour displayed also involved touching private parts of other children and adults or touching them inappropriately, and less frequently, ones were trying to rub their genitals on other people and a history of playing with toys in a sexual way.
Sexual Behaviour Displayed by ID Individuals.

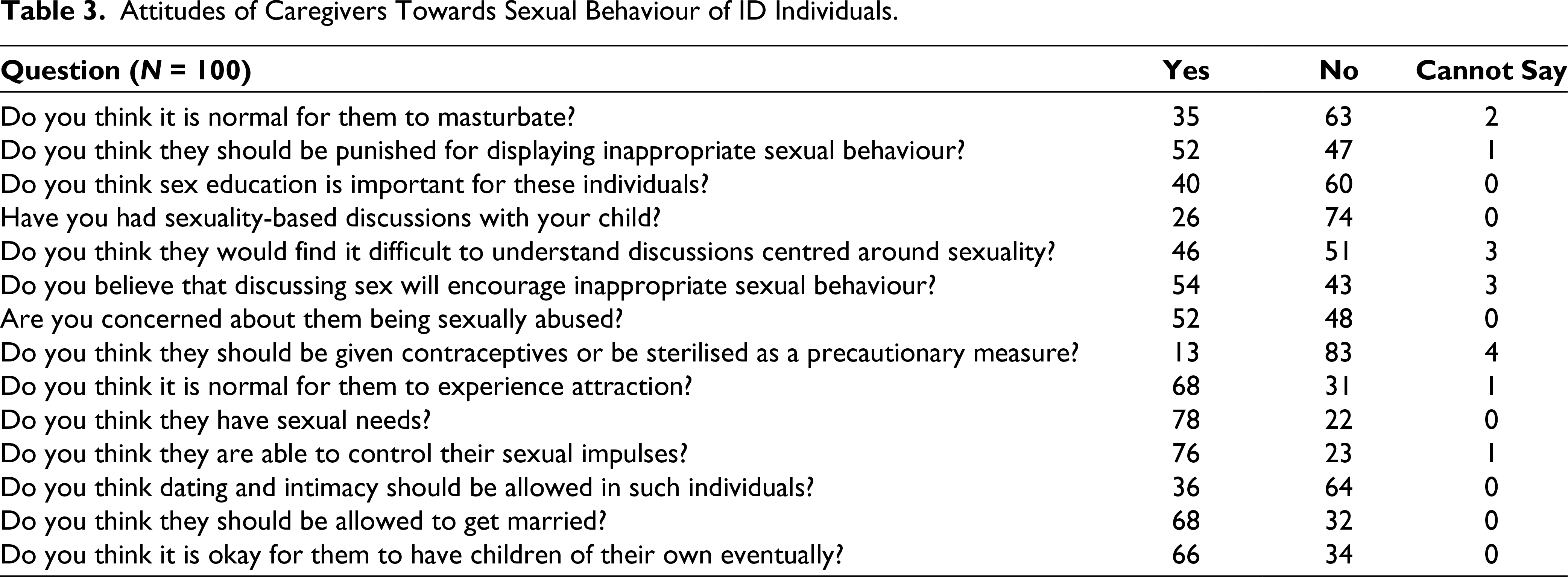
Table 3 shows the data regarding attitudes of caregivers towards the sexual behaviour of ID individuals. Most caregivers (63%) believed that it is not normal for their children/these individuals to masturbate. Additionally, 57% of parents believed that punishment should be given for the display of inappropriate sexual behaviour. Less than half of the parents (40%) believed that sex education is necessary and important for these children. This may be supported by the fact that 54% of parents felt that discussions centred around sexuality would encourage inappropriate sexual behaviour. In accordance, only 26% of them had previously had sexuality-based discussions with their children. Around half of the parents were concerned about their children being sexually abused. While most caregivers accept that their children have sexual needs, less than half of them believe that dating and intimacy should be allowed for them. Many parents believed that marriage and having children should be allowed and accepted in these individuals.
Attitudes of Caregivers Towards Sexual Behaviour of ID Individuals.
Discussion
Individuals with ID experience the same level of sexual needs and desires as others of their age. 3 They exhibit a variety of sexual behaviours. However, due to their delayed cognitive development, they may struggle to learn acceptable sexual behaviour and may engage in inappropriate sexual behaviours as well. 4
In this study, it was found that masturbation, undressing in public and accessing pornography or media content with sexual material were the most commonly reported behaviours. Other behaviours such as touching private parts of other people, chronic peeping behaviour and engaging in sexually explicit conversation were less frequently reported.
These findings were consistent with a study by Ruble and Dalrymple in 1993, which stated that masturbation, publicly undressing and inappropriate touching were relatively common, occurring in 18%–28% of individuals with intellectual or developmental disabilities. 12 Another factor that is crucial in guiding the sexuality of these individuals and tackling inappropriate sexual behaviour is the role of caregivers. Parental attitudes have been shown to be significant predictors of the sexual functioning of persons with ID. 13
In the Indian context, discussions centred around sexuality are considered taboo, and the majority of youth report never having received sex education. 14
In this study, it was found that more than half of the caregivers did not think that sex education is crucial for these individuals, and most of them had never engaged in any sexuality-based discussions with their wards. Many parents in this study believed that imparting sex education would encourage inappropriate behaviour, a finding consistent with a study conducted by Pryde and Jahoda in 2018. 15
General caregiver attitudes towards sexuality in persons with ID have varied across multiple previous studies. For example, a study from Mexico in 2011 shows positive attitudes 16 and another from Taiwan in 2016 reports negative attitudes. 17
In this study, most caregivers accepted that their wards had sexual needs and believed it was normal for their wards to masturbate. While only a few accepted the ideas of dating and intimacy for persons with ID, the concept of marriage and children was accepted by more than half the caregivers. Many parents expressed concern over the possibility of sexual abuse, but very few were in favour of administering contraceptives as a precautionary measure.
The findings of this study dictate a need for the development of intervention programmes to appropriately tackle this problem. Certain studies mention behavioural intervention programmes such as Differential Reinforcement of Alternative Behaviour, Response-Interruption Time-Out, etc. 12 In addition to these, there is a great need to impart sex education to caregivers and affected individuals alike. Inculcating awareness amongst caregivers and guiding them on how to approach this issue, overcoming their moral and ethical convictions, is of utmost importance. These programmes must fit the cultural context of India, given the existing taboos around sexuality and disability. Interventions should be tailored to target female caregivers, as they are more likely to approach conversations with their ward regarding the same, and are often the primary caregiver in Indian households.
Our study is unique in the sense that it is the first Indian study that studies sexual behaviours in ID patients and attitudes of caregivers towards them. The limitations of this study are as follows: The study was conducted in a single setting, and findings cannot be generalised to the entire population. Also, there can be recall bias by the caregivers and ignorance of the sexual activity exhibited by the child, which would not be reported by caregivers.
Conclusions
In conclusion, inappropriate sexual behaviours—such as masturbation, pornography consumption and public nudity—are prevalent among individuals with ID. The study highlights that caregiver attitudes often reflect a lack of acceptance and reluctance to engage in discussions about sexuality, influenced by pervasive cultural taboos in India. These findings underscore the urgent need for context-specific intervention strategies. Potential approaches include the development of culturally sensitive sex education programmes, targeted awareness and training initiatives for caregivers—particularly women—and the implementation of cognitive behavioural therapy to manage problematic behaviours. Such interventions can play a crucial role in promoting healthier sexual expression and enhancing the quality of life for individuals with ID in the Indian socio-cultural setting.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding Any Prior Publication of the Work
This data has not been published previously.
Ethical Approval
This study was approved by the Institutuional Ethics Committee of LTMMC & GH, Sion, Mumbai and approval letter no. is IEC/359/23 dated 08.08.2023.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was obtained from the caregivers of children having Intellectual Disability as they were our study sample.