
Abstract
We present a challenging case of a 9-year-old female with a background of perinatal adversity and pervasive developmental delays, who manifested atypical genital tics concurrent with additional motor and vocal tics, attentional impairments, and behavioral disturbances. Diagnostic delays arose from the initial misattribution of symptoms. Following a detailed psychiatric assessment, pharmacotherapy comprising risperidone, clonidine, and ginkgo biloba was commenced, yielding substantial and enduring amelioration of tic severity, as quantified by validated instruments. This report illuminates the intricacies of diagnosing uncommon tic variants in childhood, advocating for meticulous evaluation, interdisciplinary collaboration, and comprehensive therapeutic strategies to mitigate associated neurodevelopmental and psychosocial sequelae.
Introduction
Tics are characterized by abrupt, rapid, recurrent, nonrhythmic movements or vocalizations, classified as simple or complex. 1 Predominantly, motor tics involve craniofacial and upper limb regions, whereas phonic tics include nasal sounds, throat clearing, or guttural noises; however, genital tics represent an infrequent and underrecognized entity prone to diagnostic oversight. 2 Herein, we delineate the clinical trajectory of a 9-year-old girl exhibiting a multifaceted profile of developmental impairments, behavioral dysregulations, and genital tics, underscoring diagnostic pitfalls and the imperative for an integrative management paradigm in pediatric neuropsychiatric disorders. Her perinatal history of complications, protracted milestone attainment, and progressive behavioral manifestations suggests a multifactorial pathogenesis typical of such presentations. Initial misreading of self-regulatory behaviors compounded diagnostic complexity, reinforcing the necessity for holistic appraisal transcending overt symptomatology.
Case Presentation
The patient, a 9-year-old female in third grade residing in New Tehri, Tehri Garhwal, Uttarakhand, India, was delivered at term via lower-segment cesarean section to an elderly primiparous mother. The perinatal course was marked by meconium aspiration syndrome, requiring neonatal intensive care unit admission. Subsequent developmental trajectory revealed lags in social interaction, expressive language, and gross motor domains, with preserved fine motor progression.
Verbal responsiveness was absent initially, with name recognition emerging at age 3 years. Communicative modalities relied on gestural cues, progressing to 4–5 lexical items by age 3 and rudimentary sentences by age 4. Early childhood was characterized by hyperkinetic behavior and sustained attentional deficits impacting academic and domestic tasks. Independence in activities of daily living, such as oral hygiene and toileting, was achieved only at 8.5 years, necessitating ongoing oversight.
Stereotyped facial gestures commenced circa age 3, accompanied by autoerotic genital manipulation culminating in facial erythema. These were first documented by personnel at the local Anganwadi preschool, attended from age 2.5, and relayed to guardians. Behavioral interventions proved inefficacious in suppression.
Scholastic advancement, notably upon entering second grade at age 7, was hindered by escalating attentional lapses and academic decline. Prolonged lavatory sojourns involving genital manipulation prompted classroom segregation, exacerbating educational hurdles. Symptom exacerbation occurred during screen-based activities at home.
Initial dermatological consultation yielded a prescription for topical clotrimazole, yet persistence prompted psychiatric referral. Psychiatric intake encompassed a comprehensive anamnesis and examination. Routine hematologic, hepatic, renal, thyroid, and glycemic assays were unremarkable. Cerebral magnetic resonance imaging was recommended to exclude organic etiologies. Provisional diagnosis of Persistent (Chronic) Motor or Vocal Tic Disorder (DSM-5: 307.22/ICD-11: F95.1) 3 was posited, predicated on stereotyped genital friction and intermittent grimacing. She did not report any pre-morbid symptoms. Pharmacologic intervention was instituted (Table 1), with parental endorsement of symptomatic alleviation post-initiation.
Summarizes the Patient’s Pre-treatment Status and the Improvements Observed at 15-day and 30-day Follow-up Visits, Based on Parental Reports and Yale Global Tic Severity Scale (YGTSS) Findings.
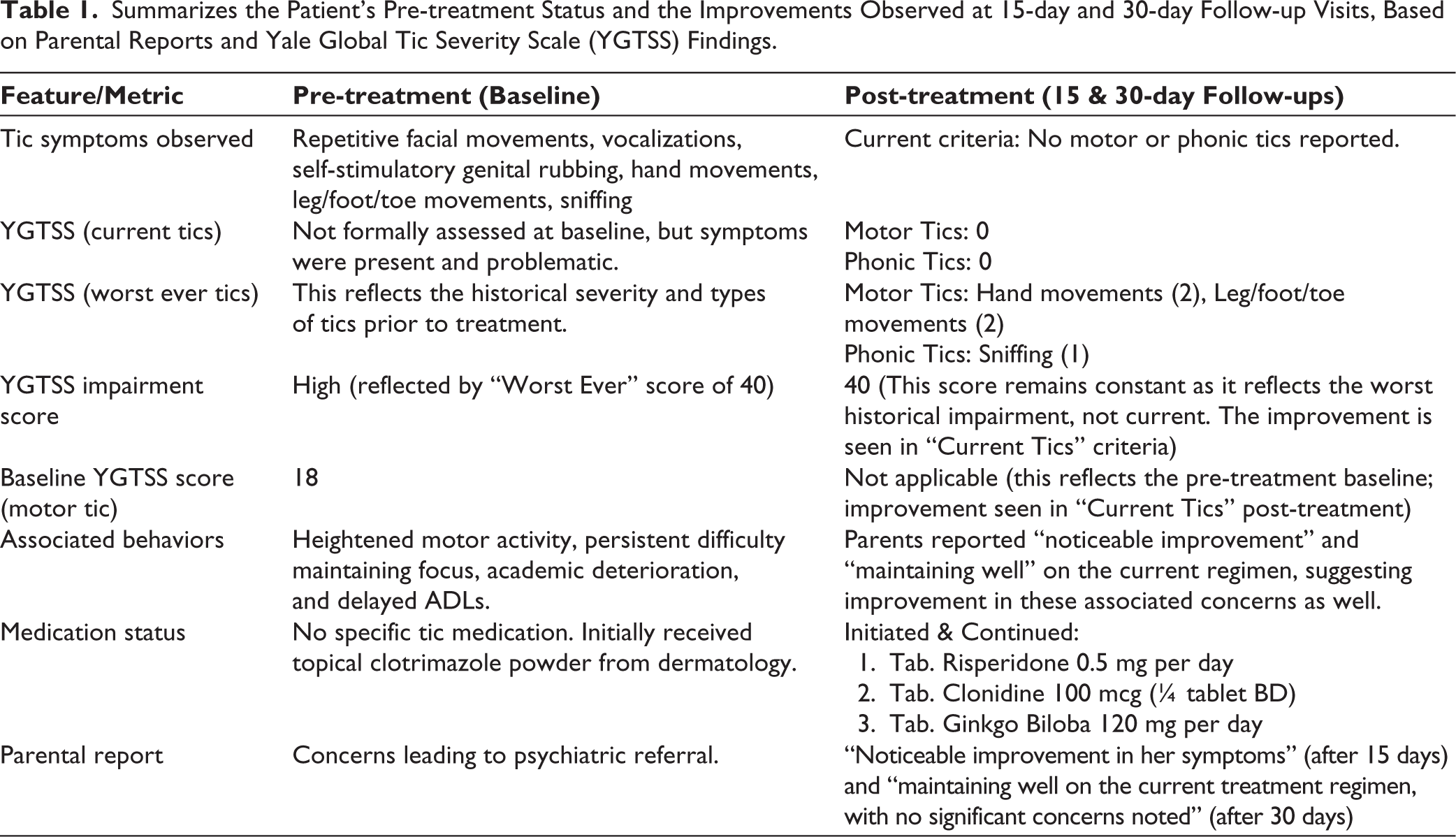
Table 1 delineates baseline characteristics and therapeutic responses at 15- and 30-day intervals, informed by caregiver narratives and Yale Global Tic Severity Scale (YGTSS) metrics. Follow-up evaluations at 15 and 30 days incorporated YGTSS administration, revealing the absence of motor or phonic tics per current criteria. Continuation of pharmacotherapy was advised, with reassessment scheduled in two months.
Discussion
This vignette exemplifies the diagnostic intricacies inherent in pediatric neuropsychiatry, wherein atypical tic phenotypes intersect with developmental and behavioral comorbidities. The patient’s evolution—from perinatal hypoxia to pervasive delays and genital tics—necessitates a nuanced, multidimensional diagnostic lens.
Symptomatic onset at age 3, featuring facial stereotypies, vocal emissions, and genital autoerotism, was initially misattributed dermatologically, deferring psychiatric engagement. This underscores the exigency of contextualizing ostensibly self-regulatory conduct within neurodevelopmental frameworks, rather than silos of specialization. Although scarce, genital tics are documented and may mimic autoerotism or maltreatment.1,2 Differentiation hinges on involuntariness, stereotypy, and partial suppressibility, elusive in juveniles.
Perinatal meconium aspiration and ensuing delays in sociolinguistic and motor spheres intimate neurovulnerability. Hypoxic-ischemic insults predispose to tic disorders and attention-deficit/hyperactivity disorder (ADHD).4,5 Concomitant hyperkinesia, inattention, and scholastic regression align with ADHD comorbidity prevalent in tic syndromes. 5 Aggravation in early schooling corroborates this nexus.
YGTSS deployment at intervals facilitated objective quantification of tic burden and therapeutic efficacy. Post-intervention null scores for current tics denote robust remission, while a historical impairment score of 20 attests to prior functional encumbrance. This bifurcated metric affords a longitudinal vista of interventional impact.
The therapeutic triad—risperidone, clonidine, and ginkgo biloba—merits scrutiny. Risperidone, via dopaminergic antagonism, is efficacious in tic suppression, notably in Tourette syndrome. 6 Clonidine, an α2-agonist, mitigates tics and ADHD features synergistically. 7 Ginkgo biloba, albeit with equivocal evidence in tics, may augment cognition adjunctively. Caregiver-reported enhancements validate regimen suitability. Neuroimaging referral prudently obviates structural anomalies; though idiopathic in preponderance, tics may herald neoplasms, vasculopathies, or encephalitides. 8 Sustained remission at 30 days portends favorable prognosis, informing protracted surveillance.
In summation, this case elucidates the interwoven neurodevelopmental tapestry underpinning atypical pediatric tics, mandating prompt identification, interdisciplinary synergy, holistic interventions, and familial empowerment. It imparts pedagogical value, enjoining vigilance for deviant tic expressions amid intricate neuroprofiles.
Footnotes
Authors’ Contribution
Vivek Pant and Vidhushi contributed to the concept, study design, data collection, and discussion. Shobit Garg contributed to the concept, data collection, and discussion. Mohan Dhyani contributed to the study design, data collection, statistical analysis, and discussion.
Availability of Data and Materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This manuscript involves a single case report involving an intervention not beyond standard care, so ethical approval is not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was obtained from the participant included in the study. Informed consent was taken from the patient’s guardians regarding the details and publishing of the case material and this conforms to the provisions of the Declaration of Helsinki.
Statement of Adherence to Preprint Policy
This submitted manuscript is an original contribution not previously published and is not under consideration for publication elsewhere.
Use of Generative AI
We acknowledge the use of Gemini Flash (via Google AI Studio) to assist in refining the language in this declaration. The prompts used focused on improving sentence structure and identifying potential grammatical errors. I have carefully reviewed and edited the AI-generated suggestions to ensure the final content accurately reflects my intended statement.