
Abstract
We report a rare and unique case of a 31-year-old male patient who initially experienced exclusively focal seizures in the form of auditory hallucinations immediately following seminal ejaculation, which over the years has progressed to GTCS. Neuroimaging studies (EEG, MRI, and PET CT) revealed epileptic foci in the left temporal lobe in contrast to past reported cases, often involving women and right hemisphere lesions. A diagnosis of ejaculation induced seizures was entertained, and he was started on treatment with anti-convulsant drugs with optimal dose titration and attained good control of seizures. This case contributes to the rarity of reflex seizures triggered by sexual activity and presentation with the psychotic phenomenon (temporal lobe phenomenon).
Introduction
Reflex seizures are seizures that develop in response to a particular stimulus. Reflex seizures have a 5%–6% prevalence among patients with epilepsy, 1 and they are the ones that are objectively and reliably shown to be elicited by the patient’s activity or a particular afferent stimulation. Afferent stimuli can be simple, like light flashes and startles, or complex. An activity can be simple, like moving an arm, or complex, like reading and playing chess, or both (reading aloud). 1 Photosensitive epilepsy is the most common type of Reflex Seizure. 2 Verbal or non-verbal auditory hallucinations can be seen as a part of an Epileptic Aura and can present as focal seizures. Seizures evoked by sexual activity and orgasms were first reported in 1960, followed by a few more case reports and a six-case series.3,4 Very few, that is, 15–20 case reports, have been published till now.
Case History
A 31-year-old male Mr. X, educated up to 10th class daily wage worker from a low socio-economic status, rural background. The patient attended the Department of Medicine for the management of generalized tonic-clonic seizures, with a referral prompted to the Department of Psychiatry for further management. On evaluation, the patient had a 10-year history of episodic auditory hallucinations followed by sexual excitement and semen ejaculation. The auditory hallucinations, characterized by multiple unfamiliar male and female voices abusing and threatening him, occurred in a clear sensorium and lasted for 3–5 minutes. During the initial episode, he got frightened, searched, and enquired about these voices, but did not find anyone. He noticed these episodes consistently followed by seminal ejaculation, leading the patient to perceive sexual activity as sinful, associating it with religious guilt. Consequently, he reduced the frequency of masturbation. However, these episodes continued after the marriage, following sexual intercourse. Stigma to disclose this history and apprehensive about hearing abusive and threatening voices, the patient gradually lost interest in sexual activity, which became an underlying cause for marital disharmony. Two years into marriage, he experienced a generalized tonic-clonic seizure following auditory hallucinations, associated with loss of consciousness for 2–3 minutes, and post-ictal sleep for 1 hour, prompting his first visit to a local doctor. He was prescribed anti-epileptics initially with one drug and later on with two drugs, but seizures remained uncontrolled. During succeeding years, along with sexual activity, seizure episodes were noticed in the time of strenuous physical activity, interfering with occupational functions. Gradually, the patient developed feelings of helplessness, irritability, and anger outbursts further intensifying conflicts with his wife, ultimately leading to their marital separation.
His past, family history, and birth history were uneventful. There is no history of childhood seizures or history of head trauma. There is a history of occasional alcohol intake, which does not fit into abuse criteria. He was evaluated and treated at various institutes with Tab. Phenytoin Sodium 300 mg per day, which was later augmented with Tab. Levetiracetam 500 mg was found to be refractory to the treatment.
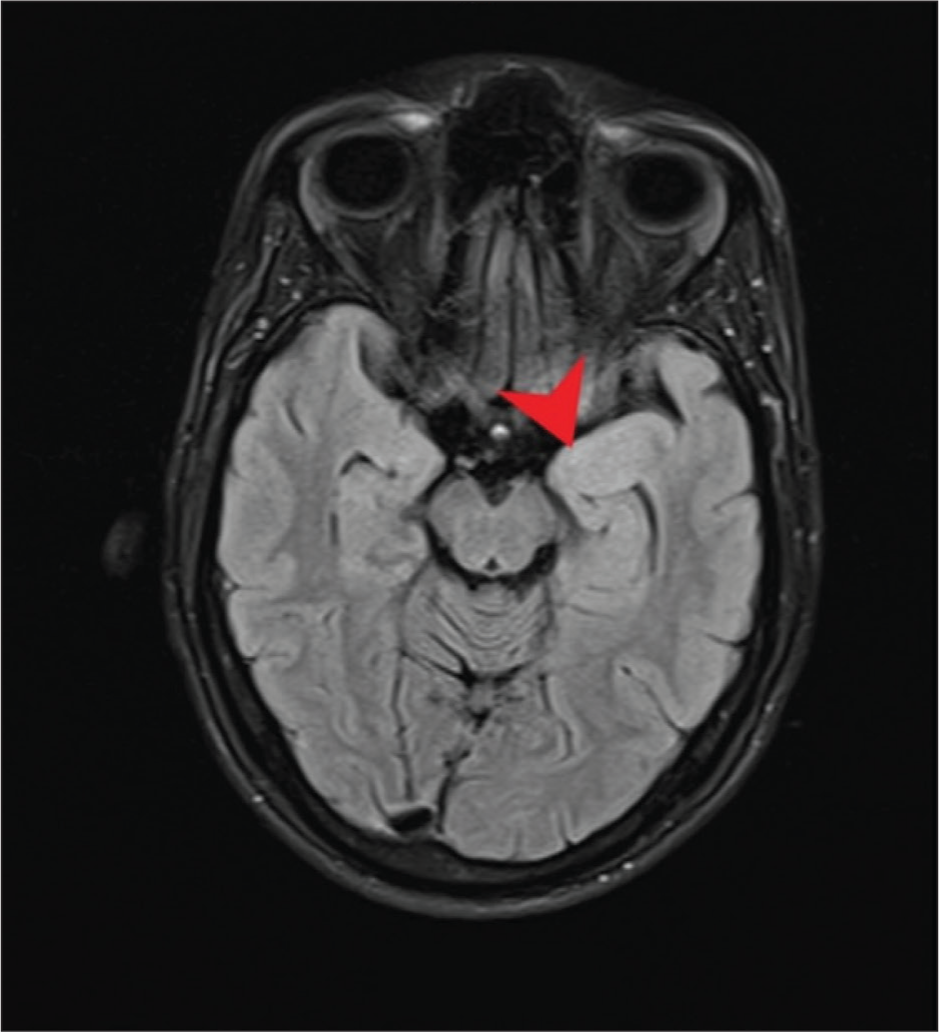
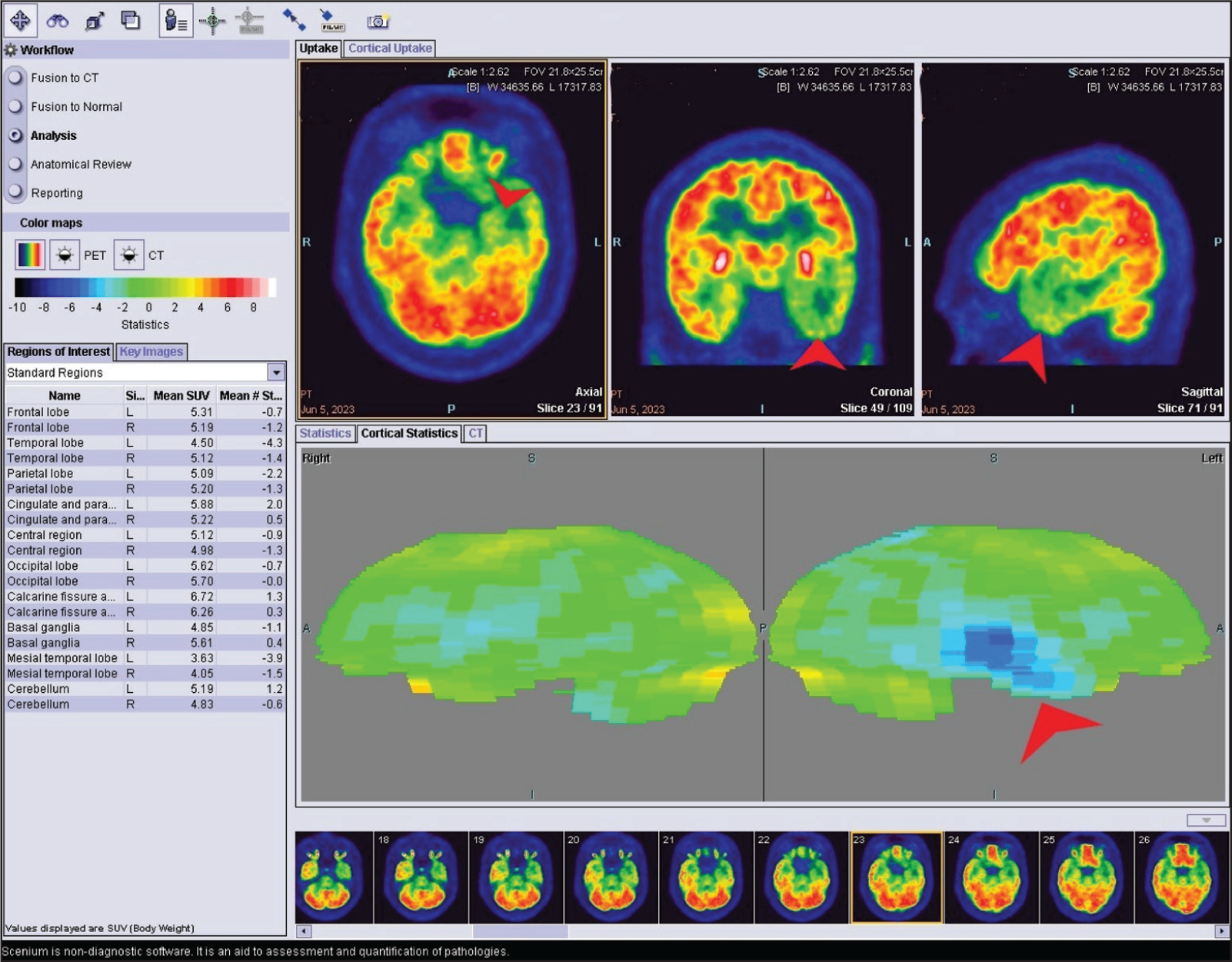
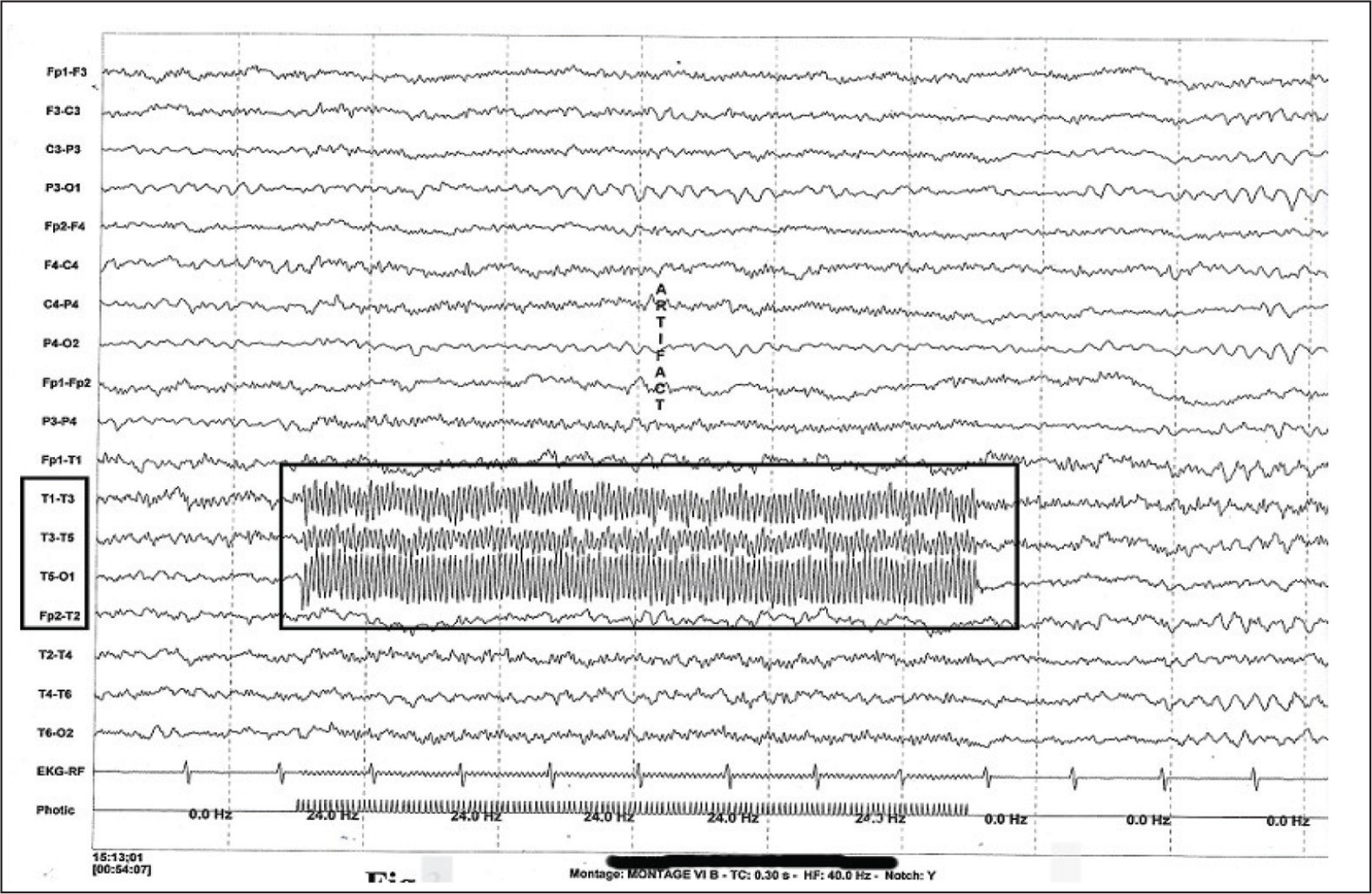
On examination, the patient has anticipatory anxiety, emotional dysregulation, and cognitive impairment. CSF analysis, including S. autoimmune encephalitis panel and Serology for viral markers, is negative. MRI Brain showed a bulky left medial temporal lobe and hyperintensity on flair (Figure 1). FDG PET & PET CT images showed decreased FDG concentration in the left temporal lobe, both medial and lateral regions (Figure 2). EEG after sleep deprivation revealed epileptic foci on photic stimulation in the left temporal lobe (Figure 3). Ictal EEG could not be taken due to test administration challenges.
MRI Brain Showing Bulky Left Temporal Lobe and Hyperintense on the FLAIR.
EEG Done After Sleep Deprivation has Revealed Epileptic Foci on Photic Stimulation in the Left Temporal Lobe.
After further evaluation along with his clinical presentation and investigation findings, a diagnosis of ejaculation induced seizures was made, ruling out other differentials like Autoimmune Limbic Encephalitis and Herpes Simplex Encephalitis. As foci are in the temporal lobe, medication was changed to tab carbamazepine with 200 mg OD titrated to 400 mg BID along with levetiracetam 500 mg HS. The patient was psycho educated about medication compliance and regular follow-up.
Discussion
Certain normal motor activities are known to trigger epileptic phenomena, which are called reflex epilepsies. Any autonomic changes during sexual activity are known to trigger seizure phenomena from an epileptogenic area in the brain. 5 Most of the cases reported were among women, and they were focal seizures with impaired awareness and localization in the right hemisphere.5–7 This case stands out from past reported cases due to its distinct presentation of episodic auditory hallucinations following ejaculation, a rare occurrence of ejaculation induced seizures. Medical attention was sought only after progression to generalized tonic-clonic seizures following sexual activity. The diagnosis became more evident only when the patient started developing GTCS.
Unfortunately, because it is associated each time with sexual activity led to marital, social, and occupational problems. Additionally, the patient exhibited features of depressive and anxiety disorders and cognitive impairment, underscoring the profound impact of this unique manifestation on various aspects of the individual’s life. The other important thing to be noted is that there were clear-cut epileptogenic foci in the left temporal lobe, unlike in other reported cases, where the lesion used to be on the right side. He started responding to Tab. Carbamazepine along with Tab. Levetiracetam, it was noticed that he did not get a seizure, despite having a few ejaculations in the past few months.
Conclusion
In conclusion, we are reporting this rare focal seizure of the left temporal region, which was presented in a misleading manner of psychotic features triggered by sexual activity, a rare phenomenon. Finally, the evolution into a GTCS has confirmed the epileptogenic nature of the psychotic feature.
Patient Perspective
Upon reaching the psychiatrist, the patient was distressed due to uncontrolled seizures, despite being on medication. He had discontinued work for the past four years, and his wife had left him, leaving him alone with his father, who became his sole caregiver. This challenging circumstance compounded the patient’s emotional and social struggles. After optimizing anticonvulsants and attaining seizure control, remission of anxiety, and depressive features patient is now planning to resume his work.
Footnotes
Acknowledgements
The authors express their sincere gratitude to R. Nandhagopal, Professor, Department of Neurology, and T. C. Kalawat, Professor and Head, Department of Nuclear Medicine, Sri Venkateswara Institute of Medical Sciences, Tirupati, for their support.
Authors’ Contribution
G. Siva Krishna Goud, T. Jaya Priya, Dinesh P., and T. Padma Sudhakar contributed to concepts, design, definition of intellectual content, literature search, data analysis, manuscript preparation, manuscript editing, and manuscript review. G. Siva Krishna Goud acted as the guarantor.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the Institutional Ethics Committee. Institutional Ethical committee-Apollo Institute of Medical Sciences and Research-Chittoor. No.PG/ 031/IEC/AIMSR/2023.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient(s) for publication of this article.
Patient Consent
Patient has given consent for publication in the Telugu language.
Prior Publication
This manuscript has not been published previously and is not under consideration elsewhere.
Presentation at a Meeting
This work was presented at APPSYCON 2023, IPS AP State Conference, held at Rajamahendravaram, Andhra Pradesh, India, on 9 July 2023.