
Abstract
Background:
Unconsummated marriage (UCM) is a significant yet underreported sexual health problem in South Asia, with a limited number of studies revealing limited information.
Objective:
To synthesize available literature on UCM in South Asia, focusing on risk factors, management strategies, clinical outcomes, and research gaps.
Methods:
A narrative review was conducted using PubMed, Scopus, Google Scholar, BanglaJOL, NepJOL, and Google. Original peer-reviewed studies published in English reporting on UCM in eight South Asian countries were included. Data on sample characteristics, etiologies, therapeutic interventions, and outcomes were extracted and analyzed descriptively.
Results:
Seven studies from India, Bangladesh, Pakistan, and Sri Lanka were included, with sample sizes ranging from single cases to 769 couples. Genito-pelvic pain emerged as the most common factor, followed by erectile dysfunction, premature ejaculation, and psychosocial factors such as fear, anxiety, and depression. Management strategies included psychosexual counseling and cognitive-behavioral therapy. Delays in seeking medical care ranged from days to over two decades, reflecting cultural taboos, lack of knowledge about sexual health, and social stigma.
Conclusions:
UCM in South Asia is an under-researched issue reflected by the number and designs of studies. Prospective studies with large sample and cross-cultural comparisons are essential to develop evidence-based management and improve sexual health outcomes for couples in the region.
Introduction
According to the International Society for Sexual Medicine, the inability of a heterosexual couple to achieve penovaginal sexual intercourse despite mutual desire and willingness from both partners is called unconsummated marriage (UCM). 1 UCM is sometimes termed as honeymoon impotence, wedding night impotence, and marriage blanc.2,3 It is a common medical and social problem, and up to 17% of visits to sexual health clinics occur due to UCM.4,5 Although it happens due to various factors in one partner, it usually affects the well-being of both. 2 It is influenced by biological, psychological, relational factors, sociocultural norms, and family pressures in different regions, particularly in the conservative Middle Eastern societies and in the developing countries.6,7
The causes of UCM are multifactorial. Physical factors such as erectile dysfunction and premature ejaculation, and psychosexual disorders such as vaginismus, are commonly reported. 8 In addition, psychological and psychiatric conditions such as performance anxiety, psychological distress, and depression may cause UCM. 9 UCM might be more prevalent in traditional and conservative religious communities, most probably due to the strict prohibition of premarital sexual exposure. 10 Inadequate sexual education and taboos about discussing sexual health could exacerbate the problem and create barriers to intervention.
Management strategies for UCM are based on etiology. Psychosexual counseling, behavioral and cognitive interventions, and sex therapy are commonly used in cases with psychological or psychosexual origins.11,12 Various studies reported uses of medication such as sildenafil and tadalafil improves UCM very effectively. 2 For couples who were primarily concerned with infertility, assisted approaches such as intravaginal insemination (IVI) provided them a practical alternative when conventional intercourse was not possible.13,14
South Asia consists of eight countries (Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan, and Sri Lanka) with about 2 billion people, covering about 25% of the global population, with various differences in cultural values, religious practices, gender norms, and healthcare access.15,16 In the region, marriage is mostly followed by tradition, religion, and societal expectations. 17 Although UCM has a detrimental effect on marriage, society, and the physical and mental well-being of the patient, research on UCM in South Asia is limited and mostly based on case reports, with only a few studies with large samples. There is a need to compile available literature to properly understand the epidemiology, causative factors, management approaches, and outcomes of UCM within the region. This review synthesizes the literature on UCM in South Asia, providing a broad overview of etiologies, interventions, and outcomes.
Methods
Study Design
This work was conducted as a narrative review, using a descriptive synthesis of published articles.
Search Strategy
A comprehensive web-based search was conducted between September 19, 2025, and September 20, 2025, without any time restrictions on publication date in PubMed, Scopus, Google Scholar, BanglaJOL, NepJOL, and Google using both Medical Subject Headings and free-text terms to ensure sensitivity and relevance. Boolean operators were applied to formulate the search string:
(“UCM” OR “non-consummated marriage” OR “unconsummated union” OR “Honeymoon Impotence”) AND
(“South Asia” OR “Afghanistan” OR “Bangladesh” OR “Bhutan” OR “India” OR Maldives” OR “Nepal” “Pakistan” OR “Sri Lanka”)
All retrieved records were screened manually for relevance based on titles, abstracts, and full texts, and duplicate records were removed.
Inclusion Criteria
The study was included if it focused on a UCM that occurred in eight South Asian countries. Research articles eligible for inclusion were original studies, case reports, case series, and quantitative analyses available in full-text form. Only peer-reviewed articles published in English were included.
Exclusion Criteria
Studies were excluded if they were review articles, editorials, opinion pieces, qualitative studies, multiple reports published from the same data, or reports based solely on media coverage. In addition, studies on migrant populations residing outside the South Asian region were excluded to ensure geographic specificity. Duplicate records were removed, and all retrieved studies were manually screened for relevance based on titles, abstracts, and full texts.
Outcome Variables
From each included study, the following variables were extracted:
Authors, publication year, country, sample size, population characteristics, associated factors, therapeutic interventions, and clinical outcomes. All extracted data were analyzed descriptively using Microsoft Excel.
Results
Study Characteristics
This review included seven articles from four South Asian countries published between 2002 and 2024 (Table 1). The majority were conducted in India (n = 4, 57.1%),13,18-20 followed by Bangladesh (n = 1, 14.3%), 21 Pakistan (n = 1, 14.3%), 14 and Sri Lanka (n = 1, 14.3%). 12 No study was identified from Afghanistan, Bhutan, the Maldives, or Nepal. Study designs ranged from single case reports18,19,21 to larger prospective and retrospective analyses.12–14 Sample sizes varied widely from a single patient18,19,21 to 769 couples. 14
Characteristics of Included Studies on Unconsummated Marriage in South Asia.
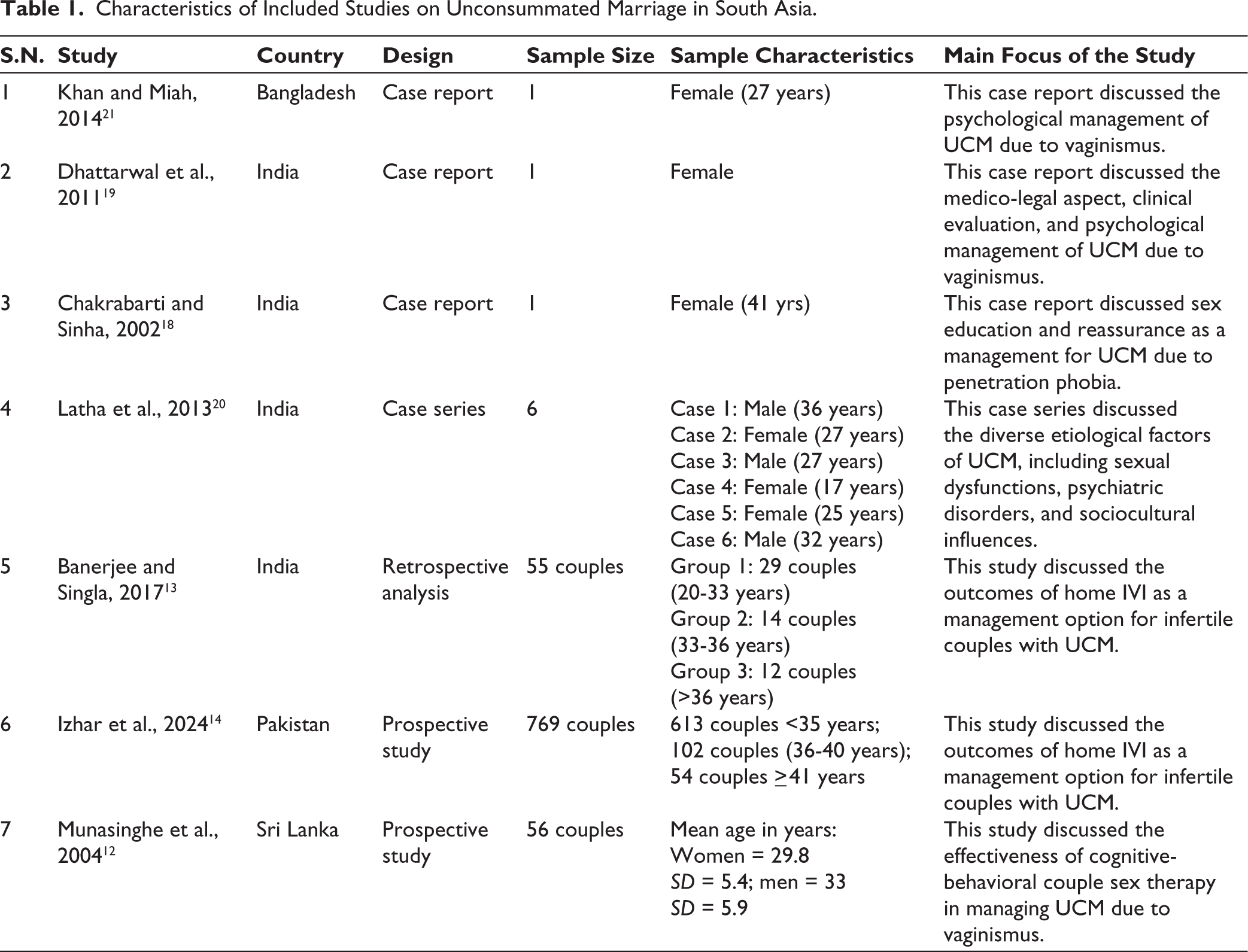
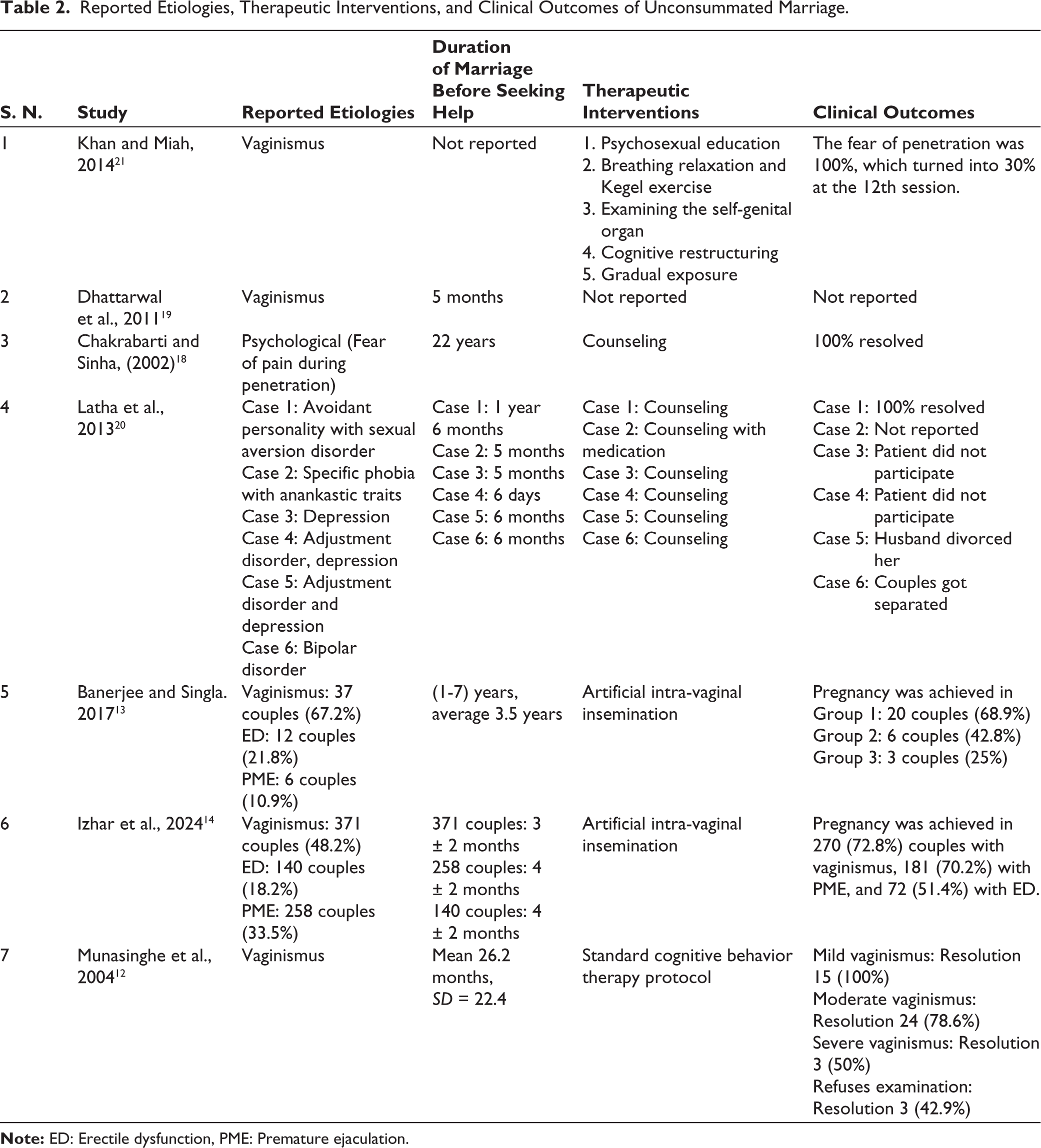
The majority of cases involved women in their 20s and 30s, although isolated reports documented cases up to 41 years of age. 18 The duration of marriage before couples sought professional help showed wide variability. In case-based reports, help-seeking ranged from only a few days 20 to as long as 22 years. 18 Larger cohort studies indicated an average delay of 2–4 years, with Banerjee and Singla (2017) 13 reporting a mean of 3.5 years and Munasinghe et al. (2004) 12 reporting a mean of 26.2 months (more than two years). However, Izhar et al. (2024) 14 reported delays of 3–4 months in the majority of couples.
Research Focus
The included studies primarily examined the causes, clinical characteristics, and management of UCM. Case reports and series, including Khan and Miah (2014), 21 Dhattarwal et al. (2011), 19 and Chakrabarti and Sinha (2002), 18 focused on psychological and behavioral factors of UCM, assessing the effectiveness of cognitive-behavioral interventions with partner involvement to reduce anxiety, sexual dysfunction, and relational distress.
However, observational studies, such as Banerjee and Singla (2017) 13 and Izhar et al. (2024), 14 extended their research spectrum to fertility outcomes, and they evaluated home-based IVI as a simple, low-cost alternative to assisted reproductive techniques. Munasinghe et al. (2004) 12 specifically investigated couples with vaginismus, which represents one underlying cause of UCM, rather than studying UCM. They explored clinical and demographic profiles of couples with vaginismus and assessed structured couple-based sex therapy as treatment.
Reported Etiological Factors
Several etiological factors were reported in the studies (Table 2). Although vaginismus was the most common cause, and it was reported in five studies from all four countries,12–14,19,21 cohort studies reported erectile dysfunction and premature ejaculation as important causes of UCM.13,14 In addition, psychiatric conditions such as personality traits, phobias, depression, and bipolar disorder were noted in Indian case reports and series,18,20 which showed how psychological and sexual factors are closely linked with UCM.
Reported Etiologies, Therapeutic Interventions, and Clinical Outcomes of Unconsummated Marriage.
Therapeutic Interventions
Management approaches varied according to etiology and study design (Table 2). Psychosexual and behavioral therapies, including cognitive restructuring, relaxation exercises, and gradual exposure, were used effectively in case-based reports.18,21 Cognitive-behavioral therapy (CBT) protocols showed positive clinical outcomes in Sri Lanka, with complete resolution in mild vaginismus cases and partial success in moderate to severe cases. 12
Overall, outcomes varied by cause and treatment modality. Counseling and CBT achieved complete resolution in selected cases;12,18 however, one study demonstrated that a lack of patient enthusiasm may result in a poor prognosis in counseling or non-invasive therapeutic interventions. 20
Discussion
Conceptual and Terminological Clarification
This review reinforces that UCM should not be conceptualized as a sexual disorder. Rather, it represented a marital condition in which sexual dysfunctions, psychological distress, and relational difficulties may act as causative factors. Sexual problems such as vaginismus, erectile dysfunction, dyspareunia, and performance anxiety should therefore be understood as risk factors rather than defining features of UCM.
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) introduced the diagnosis of genito-pelvic pain/penetration disorder; 22 however, the term vaginismus was used in this review because all included studies reported vaginismus as a clinical entity. Dyspareunia and pain-related penetration difficulties were not ignored; rather, terminology was preserved to maintain consistency with the original literature.
Scarcity of Research in South Asia
This review highlights the striking scarcity of research on UCM in South Asia, despite the region’s large population and persistent cultural taboos surrounding sexual health. 23 Only seven studies in four countries were identified over more than two decades. Among the seven studies, three were case reports18,19,21 and one was a case series with a sample size of six. 20 The remaining three were original studies with larger samples.12–14 Since most of the studies were case reports and case series, this lack of data contrasts with the significant psychosocial and clinical impact of UCM, highlighting that it still remains an under-recognized public health issue. The methodological limitations of the available studies also weaken the strength of the evidence. Most studies reported only descriptive data, lacked standardized diagnostic criteria, and did not include long-term follow-up.
Etiological Patterns
Despite their limitations, the reviewed studies collectively suggest a multifactorial etiology of UCM in South Asia. According to the included studies, vaginismus emerged as the most frequently reported etiology. Similar findings were found in Turkey, where in a study of 449 cases, vaginismus was identified as the most prominent cause, 81% of UCMs occurred due to vaginismus. 8 Similar results were found in Saudi Arabia. 24 However, in Egypt, another study of 191 patients reported psychogenic factors as the predominant cause in 74.4% of cases, with performance anxiety alone responsible for 52.9%, while vaginismus accounted for only 8.4%. 9 Although we found five studies from four different countries of South Asia that reported vaginismus as the most common cause, we also found two Indian studies that reported psychosocial factors, such as fear, anxiety, and depression, led to UCM.18,20
The predominance of vaginismus in South Asia might be due to cultural taboos, negative attitudes toward sex, lack of premarital sexual exposure, inadequate sexual education, and marital conflict, which caused anxiety and fear associated with intercourse. 25
Other causative factors of UCM that we found were erectile dysfunction and premature ejaculation. These were not predominant yet still caused UCM for many couples. Similar findings were found in the USA, Saudi Arabia, and Turkey.8,24,26
Help-seeking Behavior and Delay in Care
Although psychosexual counseling and CBT were commonly reported as effective interventions, an important finding of this review was the delay in seeking medical or psychological help. This delay might occur due to limited awareness of counseling and sex therapy as legitimate healthcare services, sociocultural stigma surrounding sexual problems, and the perception that medical health professionals are not the actual people to help the couple due to their problem. Most of the studies reported that couples waited for average periods of several months to multiple years before seeking medical advice from healthcare professionals. Such delays not only exacerbate marital strain but also reduce the likelihood of successful intervention. In one study, couples went to the doctor after 22 years of UCM, 18 of which indicated the cultural taboo and insufficient sexual knowledge that couples from South Asia had. Similarly, in China, cultural beliefs and lack of sexual knowledge were important factors influencing UCM. 27
Since UCM causes infertility, and in South Asia, family members and society have high expectations about fertility, women might face severe social stigma, which would cause psychological distress, depression, and social isolation. 28
Therapeutic Approaches
The therapeutic approaches reported in the included studies had both psychosexual counseling and reproductive-focused interventions. Studies where psychological counseling and cognitive behavior therapy were done had good outcomes.12,18,21 Similar findings were reported in two different studies in Turkey.29,30 Case-based reports demonstrated the effectiveness of cognitive and behavioral strategies, including cognitive restructuring, relaxation, and gradual exposure. 21
A systematic review about etiological factors and clinical management of UCM reported various surgical methods of treatment, such as penile venous surgery, penile plication, hymenectomy, and other minor surgeries. 2 Although medications such as sildenafil, tadalafil, and phentolamine have been reported in various studies,3,5,26,31,32 none of the studies conducted in South Asia used them as a treatment.
Clinical Outcomes and Prognosis
Clinical outcomes in South Asian studies were variable and depended on patient and partner cooperation. Some reports demonstrated complete resolution following counseling;18,21 however, some other studies revealed poor prognosis due to noncompliance of the patient, lack of motivation, or spousal separation. 20 These findings highlight the importance of a multidisciplinary approach that would have combined psychosexual therapy, medical management, and culturally sensitive counseling. Importantly, sociocultural considerations such as stigma and cultural taboos must be reduced for long-term success.
Implications for Practice and Research
The review highlights that couples with UCM in South Asia often delay seeking professional help, sometimes for several years, which might be influenced by low literacy, cultural taboos, and enduring social stigma surrounding sexual health. Proper diagnosis and management of UCM is delayed by these barriers, and it deteriorates the psychosocial and marital outcomes of the couple, including divorce and separation. Incorporating sexual education into premarital counseling, increasing awareness of psychosexual conditions, and training clinicians in this sensitive matter could reduce the incidence of UCM. Comparative studies across different South Asian cultural contexts are also necessary to understand the effect of religion, tradition, and gender roles in UCM.
Additionally, future investigations should focus on the role of sexual misconceptions, anxiety, and psychological distress caused in UCM. Focusing on the benefits of combined medical and behavioral approaches is also necessary. Conducting research on both the individual and societal dimensions of UCM can help us to develop comprehensive prevention strategies, enhance clinical practice, and ultimately improve sexual health outcomes for couples in South Asia.
Strengths and Limitations
To the best of our knowledge, this is the first review on UCM in South Asia. The study highlighted the range of reported cases, their etiological factors, therapeutic approaches, and clinical outcomes.
Despite these strengths, several limitations should be acknowledged. First, the number of studies on UCM was limited (only seven), and the majority of included studies were case reports or case series, limiting the generalizability of findings. Second, most of the studies were descriptive in nature and used different methods to measure outcomes, so direct comparison across studies was not possible. Third, data from several South Asian countries, including Afghanistan, Bhutan, the Maldives, and Nepal, were not available, so regional representation was not possible. Fourth, ethical approval and informed consent were recorded in most of the studies; however, several older or case-based studies did not explicitly state ethical clearance. Final, preventive perspectives such as the role of premarital counseling, sexual education, or community awareness were absent in all studies, which limits understanding of how the incidence of UCM could be reduced.
Conclusion
Despite the severe marital, psychological, and reproductive consequences, UCM remains an underreported and underexplored topic in South Asia. Current studies are case series and case reports. UCM has multifactorial causation; the most prominent causes were vaginismus, erectile dysfunction, premature ejaculation, and psychosocial factors such as fear, anxiety, and cultural taboos about sexuality. Psychosexual counseling and cognitive-behavioral approaches had good outcomes. Because of the psychosocial burden, social stigma, and delayed care-seeking mentality in UCM, future work should prioritize culturally tailored interventions and preventive measures such as the integration of sexual education into premarital counseling and the development of multidisciplinary treatment frameworks. High-quality prospective studies and cross-cultural comparisons are needed to establish evidence-based guidelines that would address both biomedical and sociocultural determinants of UCM in South Asia.
Footnotes
Authors’ Contribution
SMYA: Conception
SH: Data curation
SH: Writing original draft
SMYA, SH: Writing review and editing
All authors have read and approved the final version of the manuscript.
Data Availability Statement
Data will be provided to the query request of the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study used data from publicly available published academic literature. No human participants were directly involved in this study. Therefore, no formal ethical clearance was sought for conducting the review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
NA.