
Abstract
Sexual behaviors among adolescents have garnered significant scholarly research across many countries globally. While research on sexual behaviors in Botswana has been linked to health problems such as HIV and teenage pregnancy, this study provides empirical evidence on psychosocial functioning in sexual behaviors among adolescents in Botswana. Data used in this study were derived from a behavioral and biological cross-sectional survey conducted in 2016. The survey adopted a multistage design and yielded a sample of 7205 female and male adolescents from schools in urban and rural areas in Botswana. Using Statistical Package for Social Sciences (SPSS) version 28, the analysis used the chi-square test for bivariate analysis and logistic regression for multivariate analysis to show the association between sexual behaviors and psychosocial functioning. The results showed that individuals who had sex after taking alcohol or drugs, exchanged sex for gifts, money, or drugs, reported sexually transmitted diseases (STIs), and were forced to engage in sex showed higher prevalence of feeling hopeless, lack of self-confidence, and attempted suicide. Interestingly, the adjusted odds ratio shows that engaging in sex for money, gifts, or drugs was associated with hopelessness, attempted suicide, and lack of confidence. Moreover, engaging in sex under the influence of substances was associated with attempted suicide. The findings suggest the need for a broad strategy for a comprehensive strategy that encourages the need for safer sex education, abstinence, and awareness toward adolescents who turn to sexual activities as a means of gaining material things.
Introduction
The debate on sexual behaviors of adolescents has widespread implications1,2 and is extensively researched in many countries. 3 Botswana has in the past years experienced increasing prevalence of sexual behavior among adolescents and young adults, with more females (65%) reporting being sexually active compared to males (35%). 4 The sexual behavior among adolescents in Botswana has been a great concern, as it is linked with increased exposure to multiple risk factors, 5 including HIV-risk,2,6 unwanted pregnancy, school dropouts, and other sexually transmitted diseases (STIs), 7 school absenteeism, 8 and substance use, 9 as well as mental instability and stresses among adolescents. 10 There is a need for research that investigates the impact of sexual behavior on emotional well-being. In Botswana, it has been reported that since 2018, 25% of new HIV infections occurred among adolescent girls. 7 Engagement in sexual behavior has implications for the individual’s well-being 2 and negative mental health outcomes,11,12 which might result in other serious problems such as suicide. 13 An underlying issue is that adolescents may not be cognitively and emotionally ready to make responsible and healthy sexual decisions. 14 Moreover, engaging in early sexual behaviors could affect psychological well-being because sexual encounters for adolescents can be stressful. 15 On the contrary, popular directions of arguments in the literature show that mental well-being affects engagements in early sexual behaviors.9,14 Even though both directions are possible, 9 this study focuses on sexual behaviors’ implications on confidence, hopelessness, and suicide attempt. This research direction was selected due to the often underestimated yet profound consequences of psychosocial functioning, which adversely affect adolescents’ academic performance, physical health, substance addiction risk, and overall well-being. These directional outcomes usually go unrecognized because of a lack of knowledge and common societal ignorance.
Out of the many aspects of physical health and adolescent sexual behavior, mental health issue was a resultant factor. 16 Empirical studies have often linked sexual behaviors of adolescents to mental health issues such as depression, self-harm, 17 physical self-esteem, 14 and suicide ideation. 18 However, existing studies show a particular research gap on the effect of sexual behavior on feelings of hopelessness and confidence. Ramrakha et al. 19 and Kagan et al. 20 for example, have studied the effect of feeling hopeless on sexual behavior, not vice versa. Studies on suicidal ideation in sexual behaviors of adolescents were reported.18,21 Moreover, a meta-analysis study revealed a positive relationship between sexual behavior and self-esteem, confidence, and self-image. 22 This means engaging in sexual behavior boosts the self-esteem and confidence level of adolescents. Another study on the mental health of young people revealed that engagement in sexual behavior was associated with increases in feelings of sadness, worry, irritability, anxiety, and depression. 23 Moreover, several studies have been conducted on the association between psychological stresses, psychosocial functioning, mental health issues, and adolescent sexual behavior (Barchi et al.⁷; Nogueira Avelar e Silva et al.¹⁴; Vasilenko et al.¹⁶; Bennett and Bauman). 24 However, there are insufficient studies on this subject matter in Botswana. This study aims to determine how psychosocial functioning, such as lack of confidence, hopelessness, and suicide attempt are a result of sexual behaviors among adolescents in Botswana.
Materials and Methods
Data for our study were drawn from the Second Botswana Youth Risk Behavioral and Biological Surveillance Survey (BYRBBSS II) of 2016, a national survey focusing on several adolescent risks and health behaviors, including sexual behaviors. Even though this is a 2016 dataset, it provides unique, high-quality insights and is the only large-scale data that addresses our research objective at the national level. The survey participants were recruited from secondary schools throughout Botswana and were selected from a list of classes from each sampled school. 25 The survey report showed that all research protocols for consent, voluntary participation, privacy, and confidentiality were followed during the research process. 25 Weighted proportions of each student were matched to the national population proportion to ensure that the data were representative of all students in the districts, grades, and nationally. This yielded a sample size of 7,205 male and female adolescents. While our study used secondary data, permission to use data from the BYRBBSS was granted by the Ministry of Basic Education through a research permit number MESD 1/7/1 I (18)-C/SHE dated March 24, 2023. All ethical clearance procedures were followed by the Ministry of Basic Education before data collection. The survey protocol and questionnaire were reviewed and approved by the Health Research and Development Committee. 25 Informed consent was sought from parents or guardians, and voluntary participation was sought from students. 25
In this survey, sexual experience was measured using nine items that asked respondents if they ever “had sexual intercourse,” “used drugs or alcohol before having sex,” “forced to have sex when they did not want,” “used a condom during the last sex encounter,” “engaged in sex in exchange for money, drugs or gifts,” “ever had STI.” The response categories for these items were yes (1) and no (2). However, for easy analysis, these were coded into dummy variables where no = 0 and yes = 1. Demographic variables such as sex, age, form (level of education), living arrangement, and religious affiliation were essential in the regression models. The dependent variables (psychosocial functioning) used in this study were confidence, attempted suicide, and hopelessness. The selected questions asked respondents, “During the past 12 months, have you ever felt sad or hopeless almost every day?” and “Ever attempted suicide?” For confidence, respondents were asked, when you look at yourself in the mirror, are you unsure what do in life? The response categories for these items were yes (1) and no (2). These variables were further recoded “1” for adolescents who reported hopelessness, lack of confidence, and suicide attempts. Conversely, responses indicating hopefulness, confidence, and no suicide attempts were recoded as “0.”
Statistical analysis was conducted using Statistical Package for the Social Sciences version 28. Bivariate analysis using the chi-square test and multivariate logistic regression were employed to assess the prevalence and the relationship between sexual behaviors and the outcome of psychosocial functioning, specifically lacking confidence, hopelessness, and attempted suicide. The regression results were presented in Model I (crude model), which assessed the association between each of the functioning factors and each of the demographic and sexual behavioral factors independently. Model II (basic model) assessed the association between each of the functioning factors, adjusting for demographic variables. Moreover, the last Model III (full model) assessed the association between each of the functioning factors, adjusting for both demographic and sexual behaviors. The results were presented in Odds ratio (ORs) and Adjusted odds ratio (AORs), 95% confidence interval (CI), and a statistical significance level of P ≤ .05, P < .01, and P < .001.
Results
A total of 7,205 school going adolescents responded to the survey. There were 4,230 (58.7%) girls and 2,975 (41.3%) boys, of whom 216 (2.9%) were aged 12 years and below, 4,115 (56.8%) were 13–15 years, and 2,870 (40.3%) were 16–19 years as seen in Table 1.
Demographic Characteristics of the Sample. 25
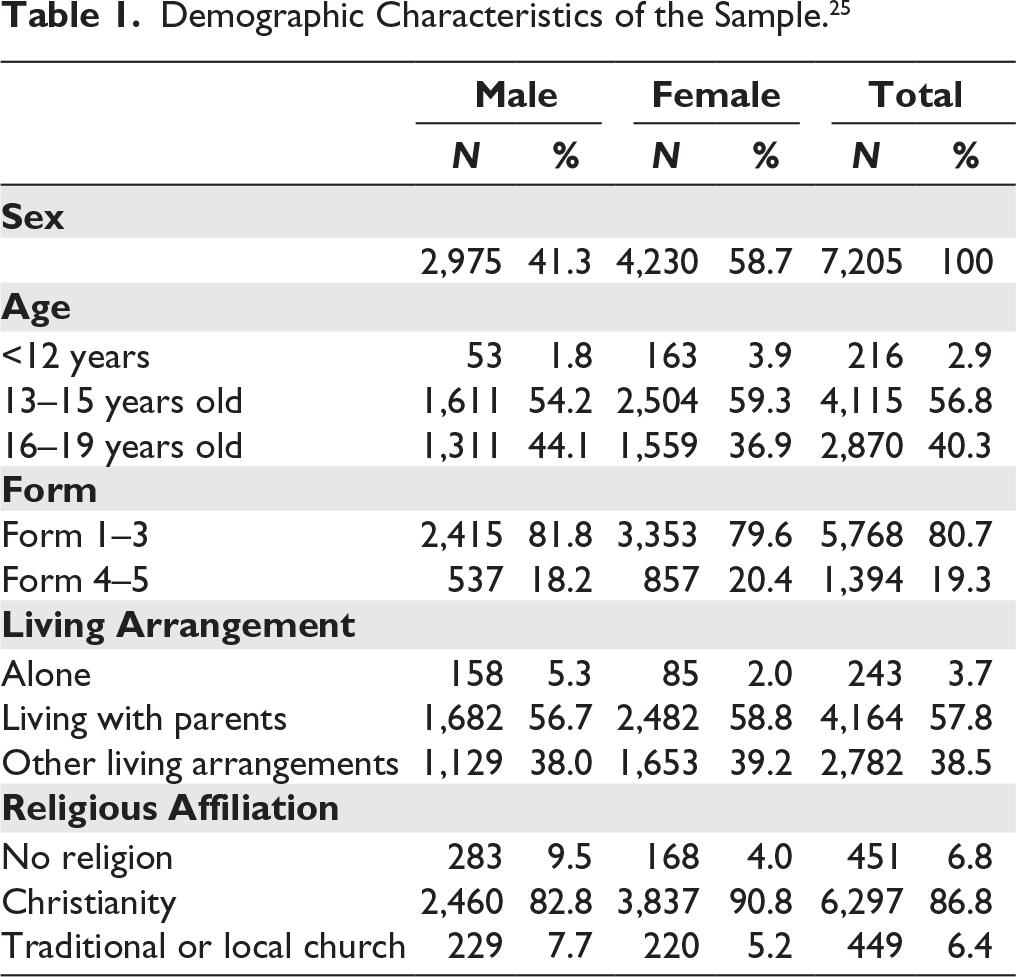
Table 2 shows that there is a statistically significant relationship between sexual intercourse and attempted suicide (chi-square value = 122.595***), feeling hopeless (chi-square value = 62.815**), and lack of confidence (chi-square value = 8.345**). Adolescents who ever had sexual intercourse were more likely to attempt suicide (34.1%), feel hopeless (59.9%), and lack confidence (29.3%) than those who never had sex. Those who never had sex did not attempt suicide (79.5%), never felt hopeless (51.6%), and had confidence (74.4%) more than those who ever had sex.
The Prevalence of Sexual Behaviors with Varied Psychosocial Functioning Among Adolescents.
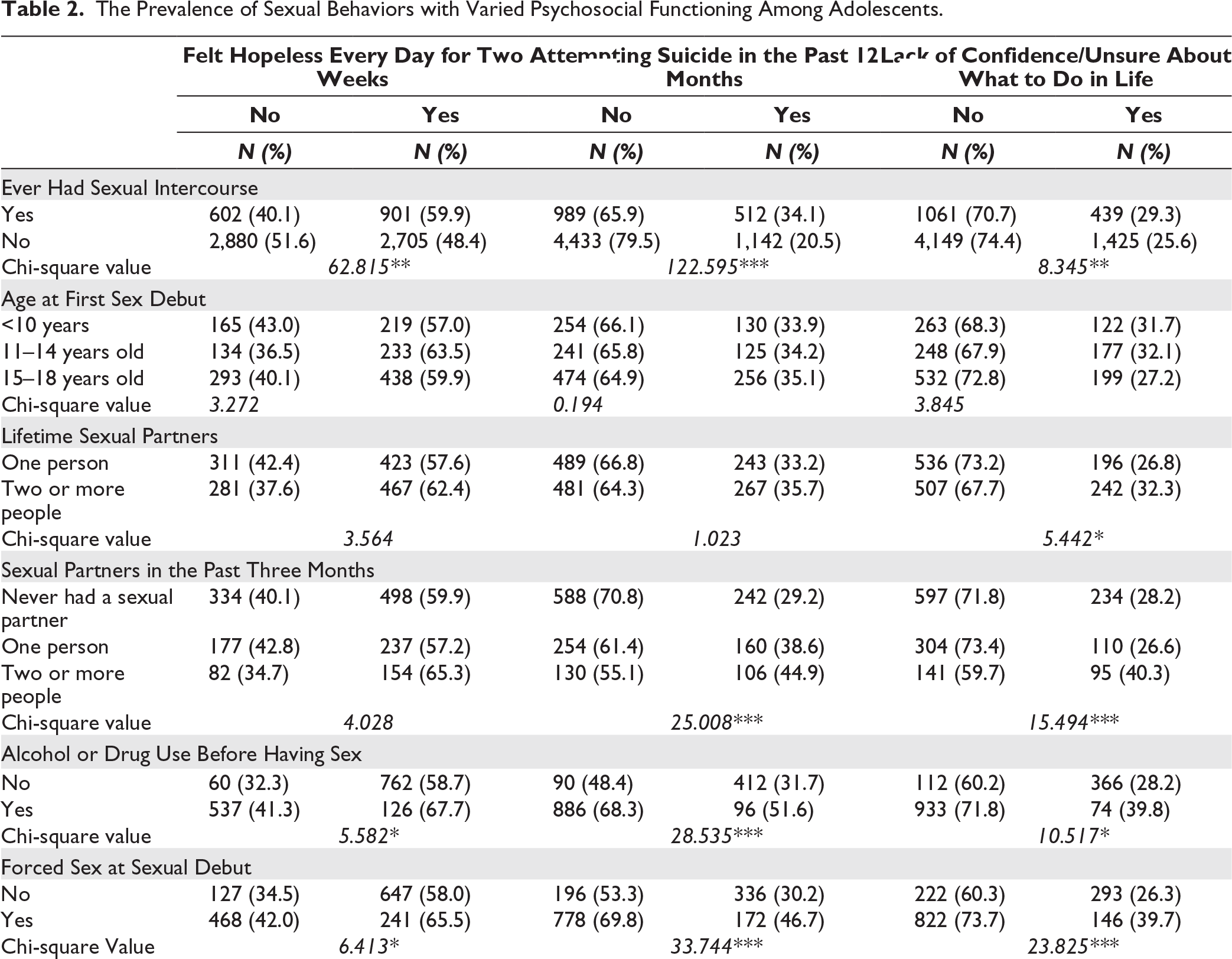
There is a significant relationship between lifetime sexual partners and lack of confidence, with a chi-square value of 5.442**. Adolescents who had two or more lifetime sexual partners were more likely to lack confidence (32.3%) than those with one lifetime sexual partner; those who had one lifetime partner were more likely to have confidence (73.2%) than those with two or more lifetime sexual partners. The relationship is also significant between sexual partners in the past three months and suicide attempt (chi-square value = 25.008***) and lack of confidence (chi-square value = 15.494***). Respondents who had two or more sexual partners in the past three months were more likely to attempt suicide (44.9%) and lack confidence (40.3%) than those with one sexual partner or never had a sexual partner. Those who never had a sexual partner reported never attempting suicide (70.8%), compared to those with one sexual partner and two or more sexual partners.
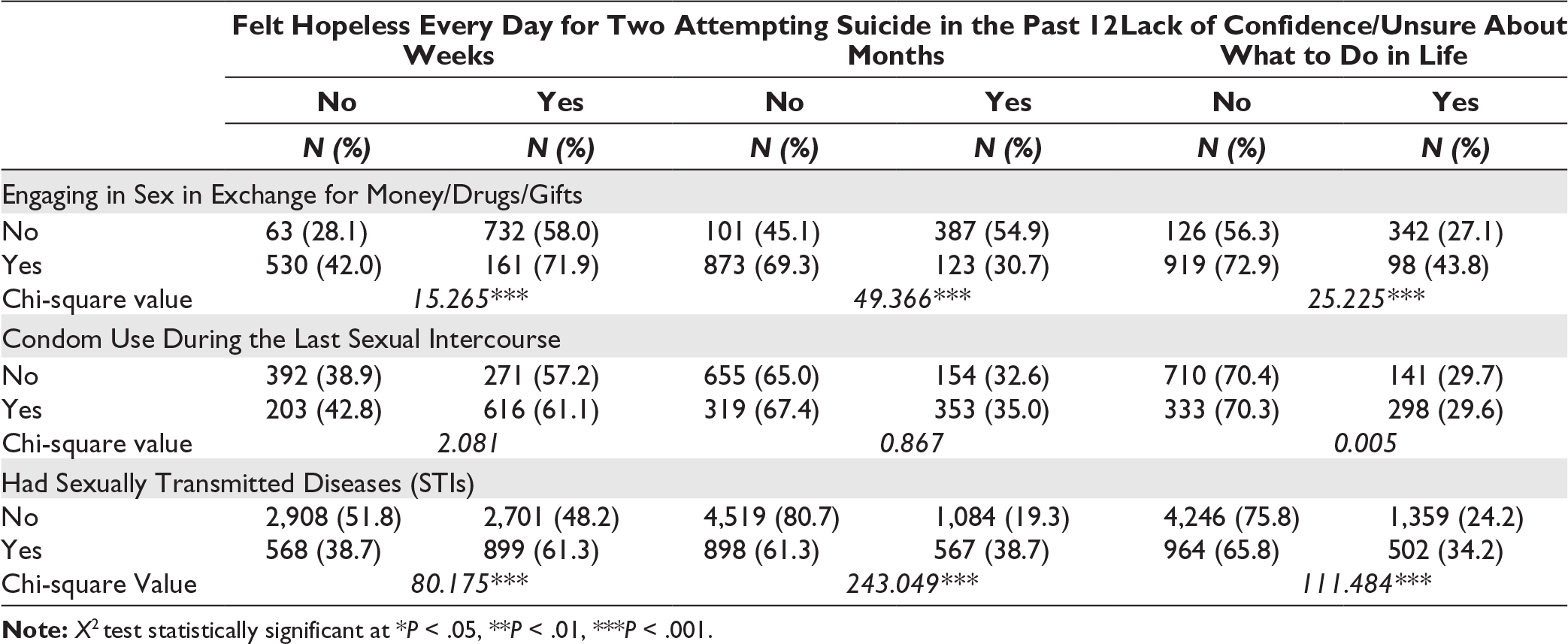
A significant relationship is also illustrated between alcohol and drugs before sex and feeling hopeless (chi-square value = 5.582*), attempted suicide (chi-square value = 28.535***), and lack of confidence (chi-square value = 10.517*). Those who used alcohol and drugs before sex were likely to feel hopeless (67.7%), attempt suicide (51.6%), and lack confidence (39.8%) more than those who did not use alcohol or drugs before sex. Respondents who were forced at their sexual debut were likely to feel hopeless (65.5%, chi-square value = 6.413*), attempt suicide (46.7%, chi-square value = 33.744***), and lack confidence (39.7%, chi-square value = 23.825***) than those who were not forced to engage in sex. Those who engaged in sex in exchange for gifts were likely to report feeling hopeless (71.9%, chi-square value = 15.265***), attempting suicide (30.7%, chi-square value = 49.366***), and lacking confidence (43.8%, chi-square value = 25.225***) than those who did not. Adolescents who reported having sexually transmitted infections were likely to feel sad or hopeless (61.3%, chi-square value = 80.175***), attempt suicide (38.7%, chi-square value = 243.049***), and lack confidence (34.2%, chi-square value = 111.484***) than those who did not have STIs.
As seen in Table 3, all the demographic factors (Model I) were associated with hopelessness. But when adjusting for demographic variables (Model II), level of education was eliminated as a predictor of hopelessness. When adjusting for demographic and sexual behaviors (full model), only gender and living arrangements had a significant relationship.
Logistic Regression Model Results of Hopelessness Among Adolescents.
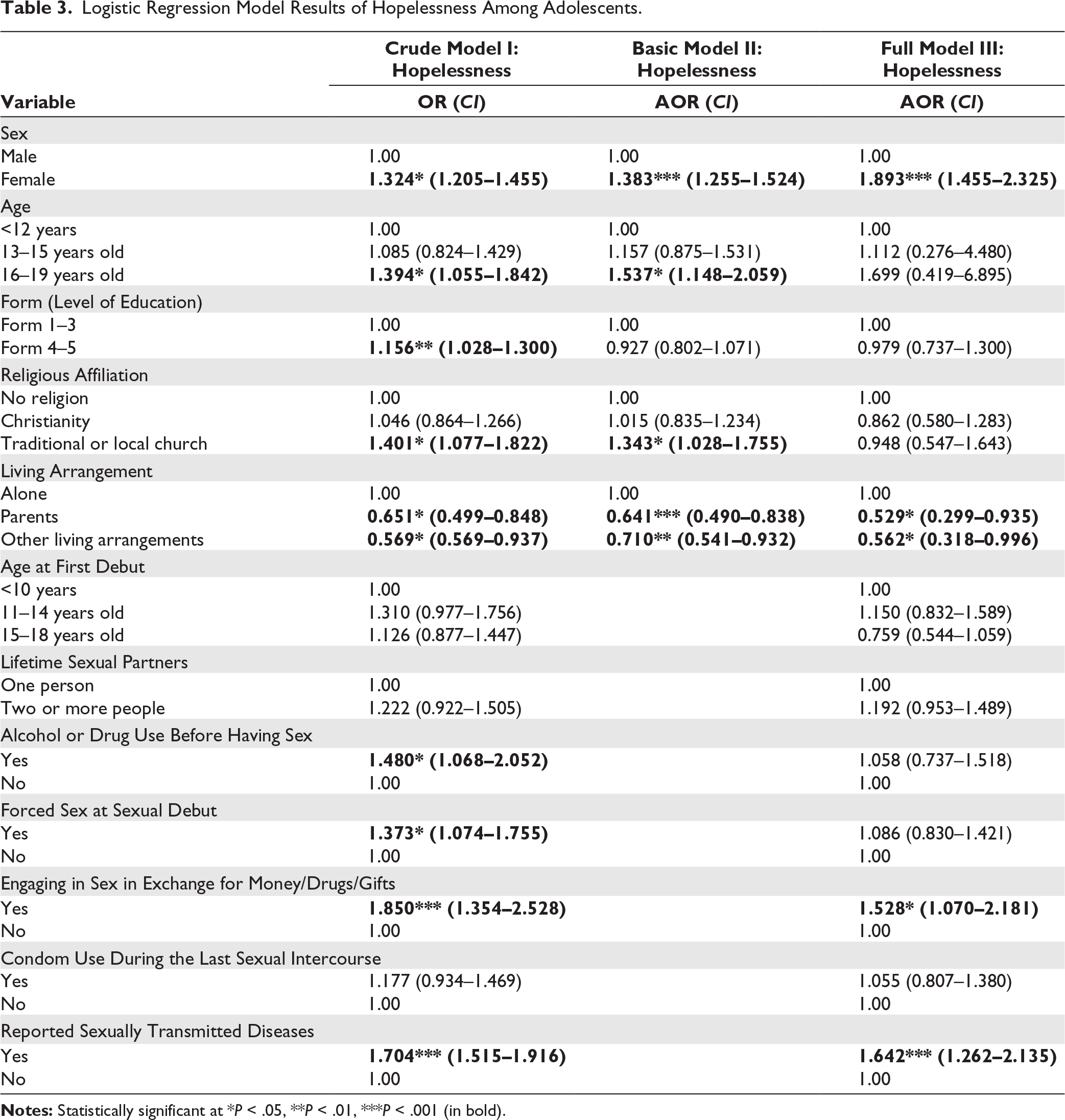
When adjusting for both demographic and sexual factors (full model), sex of respondents, living arrangements, engaging in sex in exchange for gifts, money, or drugs, and reported STI showed a significant association. Females were 1.893 times more likely to be hopeless than males (CI: 1.455–2.325). When compared with adolescents who lived alone, those who had other living arrangements were 0.569 less likely to be hopeless (CI: 0.569–0.937), whereas those who lived with parents were 0.529 less likely to be hopeless (0.299–0.935). Adolescents who engaged in sex in exchange for gifts were more likely to be hopeless (AOR = 1.528, 95% CI: 1.070–2.181). In addition, students who had sexually transmitted infections were more likely to be hopeless (AOR = 1.642, 95% CI: 1.262–2.135).
Reference groups are equal to 1.00. Model I (crude model), Model II (adjusted for demographic variables), and Model III (includes demographic and sexual behaviors).
As seen in Table 4 (the unadjusted model), there was an association between level of education, religious affiliation, and living arrangements, with level of education and living arrangement having negative associations, while religious affiliation have positive association with attempted suicide. When controlling for other demographic variables (basic model), there was no major change in the model.
Logistic Regression Model Results of Attempted Suicide Among Adolescents.
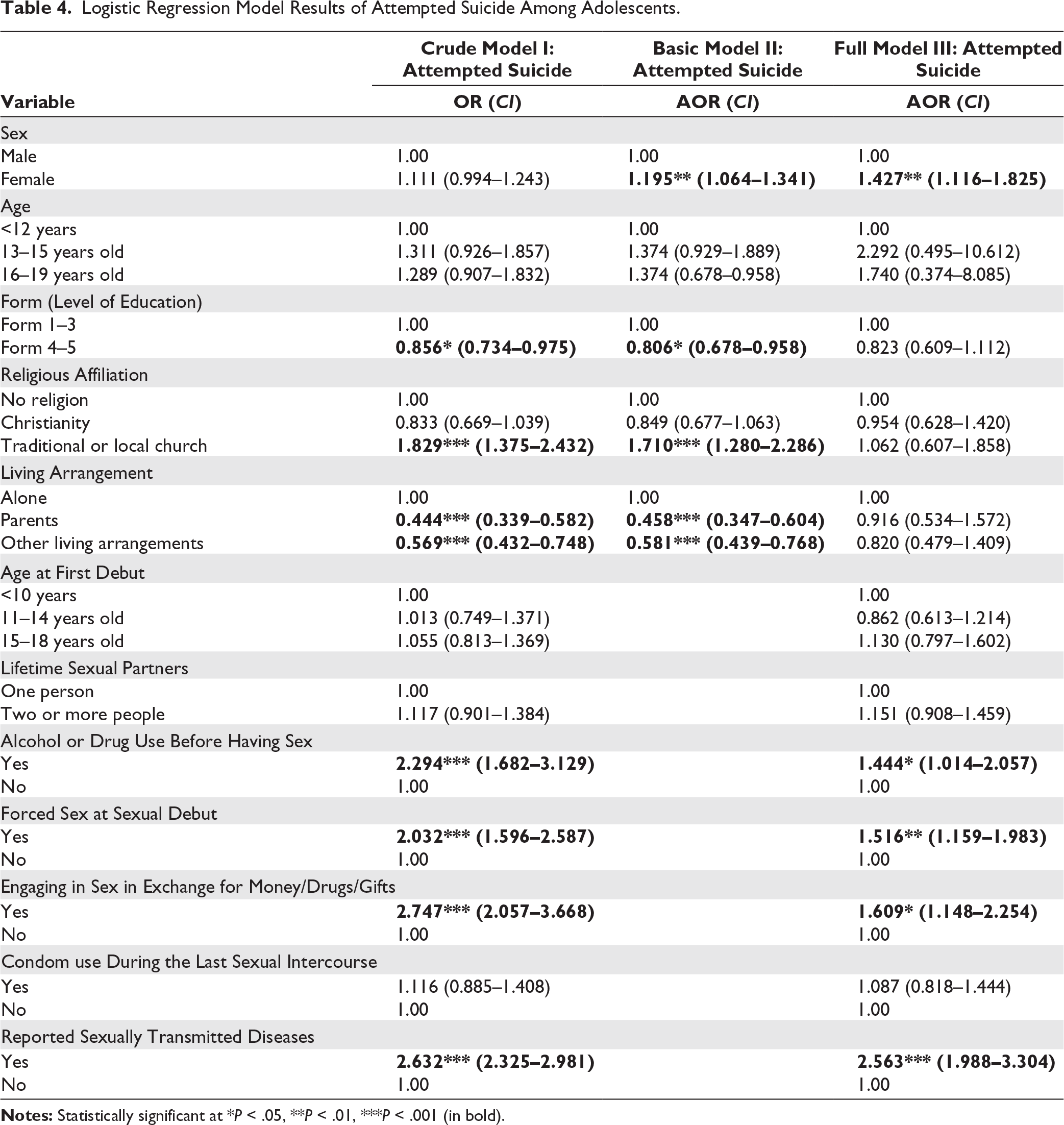
The full model shows that use of alcohol or drugs before sex, forced sex at sexual debut, engaging in sex in exchange for gifts, money, or drugs, and reporting STIs were associated with suicide attempt. But when controlling for demographic variables (basic model), the results produced no associations. The full adjusted model, where we controlled for both demographic and other sexual variables, revealed some associations between sexual behaviors of adolescents and suicide attempt. Adolescents who used alcohol and drugs before sex were more likely to attempt suicide than those who did not (AOR = 1.444, CI: 1.014–2.057). Adolescents who were forced into sex at their sexual debut were more likely to attempt suicide than those who consented (AOR = 1.516, CI: 1.159 to 1.983). Engaging in sex in exchange for gifts, money, or drugs was associated with attempted suicide, with those who engaged in such being more likely to attempt suicide that who did not. (AOR = 1.609, CI: 1.148–2.254). Adolescents who reported having sexually transmitted infections were twice as likely to attempt suicide as those who did not have STIs (AOR = 2.563, CI: 1.988–3.304).
Reference groups are equal to 1.00.
Model I (crude model), Model II (adjusted for demographic variables), and Model III (includes demographic and sexual behaviors).
As seen in Table 5, almost all demographic variables were associated with lack of confidence except sex (gender) in the crude and basic model. But when adjusting for demographic and sexual variables, gender and level of education were significant.
Logistic Regression Model Results of Lack of Confidence Among Adolescents.
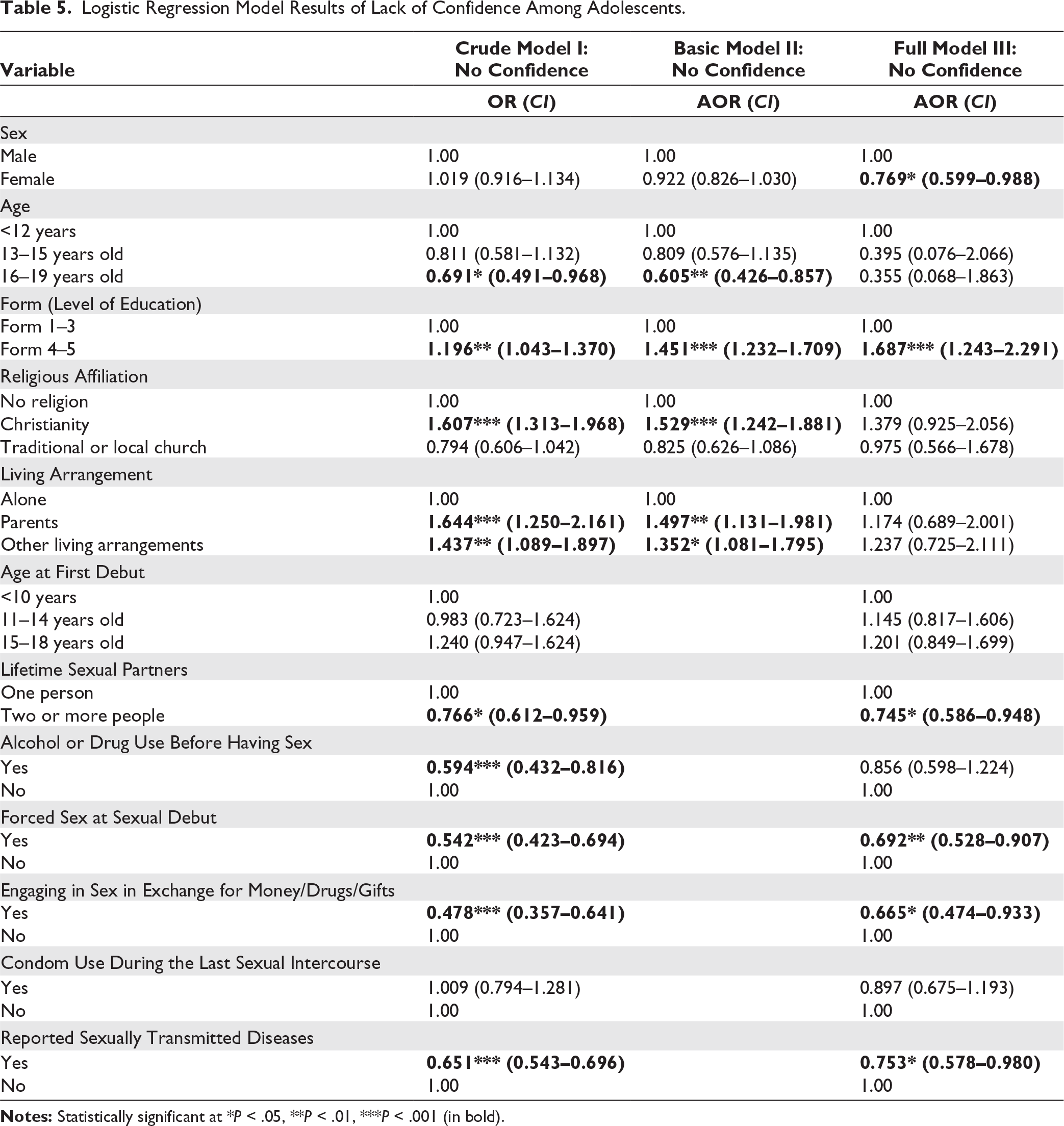
The full model shows that the association between lifetime sexual partners, forced sex at sexual debut, engaging in sex in exchange for gifts, money, or drugs, and reporting sexually transmitted infections was associated with lack of confidence. Adolescents who had two or more lifetime sexual partners were less likely to have no confidence compared to those with one lifetime sexual partner (AOR = .745, CI: 0.586–0.948). Those who were forced into sex at their sexual debut were also less likely to lack confidence than those who were not forced (AOR = .692, CI: 0.528–0.907). Those who engaged in sex in exchange for gifts, money, or drugs were less likely to lack confidence than those who did not (AOR = .665, CI: 0.474–0.933). Adolescents who reported sexually transmitted infections were less likely to lack confidence compared to those who did not report having any STIs (AOR = 0.753, CI: 0.578–0.980).
Reference groups are equal to 1.00. Model I (crude model), Model II (adjusted for demographic variables), and Model III (includes demographic and sexual behaviors).
Discussion
This is the first study in Botswana that investigated the resultant psychosocial functioning of adolescent sexual behaviors across the whole country. The prevalence of sexual behavior among adolescents in our study was 22.1%, which is greatly lower compared to the prevalence in a study by Millanzi et al. 26 which reported a prevalence rate of (69.7%). The bivariate results show that adolescents who had sexual intercourse in their lifetime, drank alcohol, and used drugs before having sex, were forced to engage in sexual intercourse, engaged in sex in exchange for drugs, money, or gifts, and those who had reported having sexually transmitted infections showed a higher likelihood of lack of confidence, attempted suicide, and hopelessness. Existing literature shows several risk behaviors that have been found to be associated with several negative states of functioning. For example, risky sexual behavior, substance use, and anti-social behaviors were associated with suicide, 27 psychological stress 17 and young people’s mental well-being. 28 Many studies found significant associations between positive sexual health indicators and lower anxiety, depression, and higher quality of life. 29 Thus, it is expected that safe sexual encounters would result in a positive and good state of functioning in adolescents.
The findings from this research revealed that gender was significantly associated with lack of confidence and feelings of hopelessness. On the first-hand females were less likely than males to show a lack of confidence, while on the second-hand females were more likely than males to show feelings of hopelessness. In Botswana, males are expected to show confidence in everything they do and not show feelings of weakness or sadness when facing a situation. Research has revealed that being a male is associated with higher levels of confidence than in females. 30 Surprisingly, our results also show that suicide attempt was highest among females, which is contrary to Beautrais 27 who found that males have higher odds of suicide attempt than females. Current research evidence has revealed that females have higher rates of suicide ideation and attempts than males.31,32 This difference can be accounted for by several underlying risk factors, such as traumatic experiences and sexual violence among females. 33 Furthermore, the results of multivariate analysis when controlling for other variables revealed a certain influence of sexual behavior on suicide attempt.
Adolescents who lived with parents and those who lived with relatives or neighbors were less likely to have feelings of hopelessness compared to those who lived alone. In the context of Botswana, this can be explained using the family environment in which young people grow up. For example, adolescents who live with parents get support, motivation, encouragements and are raised in families with stronger family cohesion. Living alone is a lonely experience for an adolescent because they would not be monitored, guided, and supported as they would be living with a relative or parents in the home. Consequently, such a form of living arrangement and experiences enhances the risk of feeling hopeless among adolescents who grow up in such environments. Furthermore, education differences were also observed for confidence. Adolescents doing Form 4 and 5 had greater odds of no confidence compared to adolescents doing Form 1–3. This means adolescents with higher education had higher odds of a lack of confidence. McClure et al. 34 stated that several risk factors, such as school dropout and absenteeism, are associated with low self-esteem in adolescents. Older juveniles usually engage in wayward behavior more than younger juveniles, and the outcome of these experiences would result in a reduced level of confidence. Moreover, when controlling for other demographic factors, the basic model results show that Christian adolescents were more likely to have no confidence than those who did not affiliate with any religion. Therefore, religion was not a confidence-boosting factor in the model. This is not consistent with other studies, which have shown that religious people feel great about themselves, with a tendency toward self-esteem and better psychological adjustment than non-believers. 35 Further results from the full model revealed that being a Christian was not significantly associated with attempted suicide, lack of confidence, and hopelessness.
Further, the study noted that adolescents who have reported having sexually transmitted infections were more likely to report feeling hopeless and attempting suicide. Reasons for this could be that adolescents are often limited in their ability to access sexual and reproductive health information, resources, and adolescent-friendly clinical care, inability to negotiate safe sex or to seek care or post-exposure prophylaxis to prevent HIV transmission. 7 The outcome of having sexually transmitted infections exhibits a lot of stress and unpredictable health outcomes that may endanger adolescents in the future. For example, risky sexual behavior has been revealed to be associated with sexually transmitted infections and unwanted pregnancies. 28 The interpretation of this finding is that lack of confidence, hopelessness, and suicide attempt are a result of the young person not being ready to be pregnant, and the process of waiting to see if they are pregnant could result in them opting for suicide or feeling sad about their decision. Similarly, a study in Nigeria found that poor sexual health also affects the individual’s mental health with increased risk of low self-esteem, depression, and suicidal tendencies. 17 Other important findings in this study revealed that lack of confidence, hopelessness, and attempted suicide were significantly associated with sexually transmitted infections. People with STIs experience frustration, anxiety, anger, fear of rejection, isolation, guilt, embarrassment, shame, and feelings of physical filth or contamination. 36 These negative psychological effects would consequently result in a lack of confidence, hopelessness, and attempted suicide among adolescents. Adolescents with sexually transmitted infection diagnoses tended to have greater odds of attempting suicide, 37 feeling sad, depressive disorders 38 than those who have never reported sexually transmitted infections.
The study also found the odds of hopelessness and suicide were greater among adolescents who engaged in sex in exchange for money, drug or gifts than those who did not engage in sex in exchange for money, drug or gifts. Scholars linked this to unstable housing, 39 food insecurity, or those who use drugs. 40 In Botswana, economic challenges are a concern in Botswana. 41 Adolescents would engage in sexual behaviors in exchange for material things such as money, food, clothes, and drugs. This is consistent with a previous study that found that the odds of having exchanged sex for drugs or money were higher for adolescents who used drugs, had run away from home, were depressed, and had engaged in various sexual risk behaviors. 39 Negative circumstances of life usually would force young people to engage in sex in exchange for money, drug or gifts. Sometimes it is not a young person’s will to engage in sex in exchange for something, but rather the economic situations from home. Thus, feeling hopeless and suicidal is because the young person is not fully in control of the situation, and the situation forces them to be in that circumstance. Moreover, adolescents who use drugs would engage in sex for the exchange of drugs because they would not afford to buy drugs for themselves. On the contrary, the odds of an adolescent lacking confidence were lower among adolescents who engaged in sex in exchange for money, drugs, and gifts than those who did not engage in sex in exchange for money, drug or gifts. It could be argued that young women actively use their sexuality as an economic resource, often entering into relationships primarily for economic gain, while in males, it boosts masculine esteem. 42 Engaging in sex in exchange for money, drugs, or gifts boosted the confidence of adolescents in Botswana. Future research in Botswana should explore reasons why young males and females engage in sex in exchange for material things.
Moreover, the results also show a consistently significant association between being forced to engage in sexual intercourse and lack of confidence and attempted suicide. Thus, being forced to engage in sex resulted in reduced confidence and increased suicide attempts. Evidence from the existing literature shows that sexual abuse is associated with suicidality and hopelessness. 21 Moreover, Stepakoff 43 stated that sexual victimization may foster not only feelings of hopelessness and thoughts of self-harm, but also nonfatal suicidal behavior. However, there was a lack of significant associations between hopelessness and being forced to engage in sexual intercourse. This contradicts the findings in Bergen et al. 21 which show that sexual abuse is more strongly associated with hopelessness.
Our results revealed that adolescents who had two or more sexual partners were less likely to report a lack of confidence than those with one sexual partner. Here, the odds ratios reflect that for every one unit increase on number of sexual partners, the odds of a student lacking confidence are decreasing. This means that having more than one partner boosted the confidence of male and female adolescents in Botswana. This finding corroborates 44 which found that high self-esteem males and females had a significantly greater number of sexual partners. An important argument in this debate is that males who reported several sexual partners may think positively about themselves in response to the celebrations they receive from other male peers when reporting their number of sexual partners. 45 For females in Botswana, they would mostly have multiple sexual partners because they also obtain money or gifts from their male sexual partners, which would boost their confidence when they tell their female peers what they obtained from their sexual partners. Further results revealed that the odds of adolescents attempting suicide increased among adolescents who drank alcohol and used drugs before having sex. A similar result was observed by Kim and Kim, 46 who stated that while drinking alcohol, cigarette smoking, and sexual intercourse have been highly correlated, this relationship also predicted suicide ideation and attempts.
Age at first sexual debut was not associated with either of the selected negative states of functioning in this study. The age at which adolescents in Botswana started intercourse did not affect their negative state of functioning. However, existing literature shows that the age at which adolescents begin sexual intercourse would affect their mental health. For example, results in Vasilenko et al. 16 revealed that first intercourse may be a major life event that can impact the mental health of young people. The study findings indicate patterns of emerging psychosocial functioning due to risky sexual behaviors. Future research should explore other factors that affect psychosocial functioning among adolescents. The main limitation was that the researchers were not part of the data collection process and, therefore, did not have control over the methodology. Furthermore, the initial collection of the data answered different research questions that were different from the current research questions. Thus, the selection of items was limited to using variables that were found in the dataset. However, the selected items from the dataset were suitable for answering the research questions for our study.
In conclusion, the findings of our research indicate that engagement in risky sexual behaviors resulted in negative functioning among adolescents in Botswana. Sexual behaviors such as having sexually transmitted infections, having sex in exchange for gifts, money, or drugs, having more than one sexual partner, taking alcohol or drugs before having sex, and being forced to engage in sexual behavior were key correlates of negative psychosocial functioning. Key results show that engaging in sex for money, gifts, or drugs was associated with hopelessness, attempted suicide, and lack of confidence. Moreover, engaging in sex under the influence of substances was associated with attempted suicide. Thus, these sexual behaviors play an important role in the prevalence and in determining the state of functioning among adolescents. Our study advocates for a positive state of functioning and well-being in adolescents who are sexually active. Therefore, Botswana’s national and strategic plan should focus on developing a framework that brings awareness about the effects of sexual behaviors, which encourages safer sex and abstinence. Importantly, the strategy should raise awareness among adolescents who turn to sexual activities as a means of gaining material things.
Footnotes
Acknowledgements
The authors would like to thank the Ministry of Basic Education of Botswana, who are the data source, for their permission to allow the researchers to use BYRBBSS II.
Data Availability Statement
Data supporting the findings of the study are available on request from the lead author, Khumo Motshwari upon request. Alternatively, the data can also be requested from the Ministry of Basic Education of Botswana
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The data used was secondary data. Since we did not involve the utilization of human subjects or invasive experiments, the University of Augsburg did not require ethical clearance for it. However, permission to use the data was sought from the Ministry of Basic Education of Botswana.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
There was no direct contact between the researchers and the individuals whose information appears in the data set.