
Abstract
Public health crises that increase the demand for healthcare professionals (HCPs) often result in increased mental distress in HCPs. The current study investigated the specific mental health ramifications of the COVID-19 pandemic on HCPs and perceived support from their places of work. Data was collected from US-based HCPs (N = 325) working as physicians (21.8%), nurses (26.8%), mental health professionals (MHPs; 30.5%), and allied healthcare professionals (AHPs; 20.9%) from April 2020 to April 2021 amidst the COVID-19 pandemic, using an online self-report survey. Descriptive and correlational statistical analyses assessed worry, stressors, psychological functioning, and perceived support. A majority of participants expressed worry about the pandemic broadly (93%), and approximately half (50.5%) indicated that their degree of worry was moderate to extreme. Respondents worried most about the risk of infection for family and relatives. HCPs reported not having been able to enjoy daily activities (66.9%), losing sleep (43.1%), and feeling constantly under strain (66.9%), compared to usual. Most HCPs indicated a strong desire for clear communication regarding the pandemic and psychological support from their workplaces. This paper provides recommendations to support HCP mental health by both ameliorating distress caused by the COVID-19 pandemic as well as protecting the health and wellness of HCPs more generally. HCPs and institutions that employ them should seek out or provide access to mental health resources and services, engage with or provide opportunities and activities to actively address mental health, and improve communication regarding COVID-19 or other topics HCPs demonstrate interest in.
High rates of COVID-19 infection and hospitalization during the year 2020 heightened demand for healthcare professionals (HCPs). Prior research shows that increased workplace demand on HCPs during public health crises results in HCPs experiencing psychological difficulties, including concerns for the safety of oneself, colleagues, and family members, as well as psychological difficulties unrelated to direct threats to health (Khalid et al., 2016). HCPs working during a crisis may experience excessive workloads, lack of adequate support, and severe emotional distress related to their proximity to trauma on an almost daily basis (Lee et al., 2018). Furthermore, HCPs falling ill because of increased exposure to COVID-19 worsened an already severe shortage of HCPs able to work during 2019 and 2020 (Buerhaus et al., 2020; Jackson et al., 2020). Considering that COVID-19 is a highly infectious and easily transmitted virus, HCPs likely also experienced severe mental distress related to the danger of their work (Shanafelt et al., 2020).
HCPs serve as an essential pillar of the U.S. healthcare system, and when the well-being of HCPs is threatened, our healthcare systems are at risk on a broader scale. A meta-analytic review of international studies documented that various types of HCPs (e.g., nurses, doctors, and other medical staff members) experienced poor mental health, including high levels of stress, anxiety, depression, and insomnia, while working during the COVID-19 pandemic (Spoorthy et al., 2020). Research is still emerging on the preventative measures that can be taken to protect HCP mental health in the face of future public health crises. Scholars must continue to research the pandemic’s mental health ramifications on working HCPs if we are to adequately address their ongoing mental health struggles and improve access to mental health resources in a sustainable way (Centers for Disease Control and Prevention, 2020). This study seeks to add to that knowledge base to address that need.
This community-driven research study was designed to respond to the needs of various community-based health clinics in South Florida, by exploring the experience of the COVID-19 pandemic and identifying specific stressors and mental health impacts among various types of HCPs. Leaders in the healthcare community of South Florida approached the current research team to collaboratively study how diverse HCPs were experiencing workplace stress related to the COVID-19 pandemic. Local HCPs had provided anecdotal evidence that an inability to adaptively address stress related to the COVID-19 pandemic was having a deleterious effect on various HCPs’ ability to perform their duties. Specifically, they shared that individuals working in the healthcare field experienced stress not only related to their own health, but also in response to the trauma that constantly surrounded them (e.g., holding the hand of a stranger as they passed away because their loved ones could not come into the hospital). The goal of this research partnership was to understand these stressors and how local institutions can better support the mental health of HCPs during and after the pandemic and inspire larger systemic change within healthcare institutions. This study thus sought to present recommendations for how both local- and larger-level institutions employing HCPs can reduce psychological harm by developing tailored systems of mental health care for HCPs.
Beyond addressing the concerns of the community-based health clinic, this study also addresses questions relevant for the healthcare field more broadly. While prior research demonstrated that public health crises tend to have consequences for HCP mental health, it was unclear whether and how these general findings reflected the experience of HCPs working in various local settings (e.g., community health clinics serving patients of color, primarily those who are first- and second-generation immigrants). We also reasoned these effects might differ based on whether the HCP worked directly with COVID-19 patients and whether they were members of minoritized groups, who often experienced high levels of burden and distress through the pandemic. Further, research conducted early in the pandemic indicated that some HCPs were particularly worried about contracting COVID-19, but this research had not indicated whether exposure to COVID-19 shared a relationship with work-related anxiety (Shanafelt et al., 2020). Additionally, although research on the topic of the intersection of racial trauma and the COVID-19 pandemic was emerging (Liu & Modir, 2020), limited research focused on this topic as it pertained to diverse HCPs. Therefore, this study also sought to explore how mental health may have differed for HCPs working directly with COVID-19 patients and diverse HCPs.
In sum, this study aims to understand how HCPs in the community, overall and by specific healthcare profession, the extent of COVID-19 contact, and minoritized group identification, were experiencing the impacts of the COVID-19 pandemic in their workplace. Aligned with exemplary community-based research practice, the university–community partnership served as foundational to all decisions made regarding this project, ranging from the identification of the research question to the dissemination of results to local HCPs.
Methods
This study assessed the perceptions of HCPs with regard to the psychological impact of COVID-19 using an online platform to collect quantitative survey data on their experience of worry and psychological distress.
Procedure
The research team created an online survey using Qualtrics to collect data from self-identifying HCPs between April 24th, 2020 to April 16th, 2021. Inclusion criteria consisted of being 18 years of age or older and self-identifying as actively working as an HCP. Participants were recruited via convenience sampling through social media and emails to various organizations, professional groups, and healthcare systems nationwide. Participants consented via an online link; those that consented were then presented study materials. Descriptive and correlational statistical analyses were conducted using SPSS version 26.
Participants
Current healthcare professionals providing services during the COVID-19 pandemic were recruited to participate in this study. Participants consisted of 325 self-identified healthcare professionals ages 21 to 81 (M = 45.75, SD = 14.51). Over three-fourths of the sample identified as female (78.8%). Participants identified as White (44.3%), Black (27.1%), Hispanic (14.2%), Asian (6.5%), Biracial (0.9%), Native American (0.9%), “Other” (0.6%), or did not report their race (5.5%).
Participants reported their job titles, which were used by the research team to divide the sample into professional groupings. Leaders in the South Florida healthcare systems indicated that physicians, nurses, and mental health care workers were populations of particular interest based on their phenomenological experience in the early months of the pandemic.
While the literature review supported assessment of these occupational categories, a multitude of healthcare professionals that are crucial to upholding our local healthcare systems were not represented by these categories and are not well represented in the literature despite their significant contribution to the field of healthcare. Consultation with community partners led the current researchers to the conclusion that these voices, albeit heterogeneous, should be included in data analysis, and these individuals were grouped together based on their common role in providing critical support as “Allied Healthcare Professionals.” While the exact role of each allied healthcare professional in our data may differ, this category reflects the imperative role of participants that do not identify as doctors, nurses, or mental health professionals in supporting and upholding our healthcare systems. Our research team thus identified the following professional groupings: physician (21.8%), nurse (26.8%), mental health professionals (MHPs) (30.5%), and Allied Healthcare Professionals (AHPs) (20.9%).
Physicians that answered this survey provided self-reported professional titles with the largest group identifying as MDs (43%). Within the self-reported responses that chose the nurse descriptor, respondents identified most commonly as RN out of any other nursing title (43%), followed by APRN (8%). Those that identified as mental health professionals categorized themselves primarily as student trainee (23%), psychologist (14%), social worker/licensed clinical social worker (14%), clinical psychologist/licensed psychologist (10%), and clinical mental health counselor (4%). Allied health professionals consisted of a wide variety of professional titles such as student trainee (10.29%), physician assistant (7.35%), ER technician (4.41%), and pharmacist (4.41%). All other unaccounted responses in each professional group either did not specify title or were specific to current role instead of professional designation (e.g., postdoctoral fellow, nursing supervisor, and hospitalist).
Participants identified their primary place of work with the largest group working in a hospital setting (46.5%), followed by community clinic (15.7%), private practice setting (7.1%), research setting (1.2%), and other/did not specify (29.5%). By profession, 45% of physicians had exposure to COVID-19 patients, 55% of nurses, 11.1% of MHPs, and 32% of AHPs. All participants were based in the United States.
Measures
Following the completion of an online consent form through Qualtrics, the questionnaire was self-administered online through Qualtrics as well and consisted of three sections: a demographics questionnaire, the Professional Stress Questionnaire (PSQ; Goulia et al., 2010), and the 12-item General Health Questionnaire (GHQ-12; Goldberg et al., 1997). The PSQ had good internal consistency when used in this study (α = .75), as did the GHQ-12 (α = .85) for understanding psychological functioning.
Demographic Questionnaire. The Demographic Questionnaire is a 15-item measure that assessed participant age, sex, race, ethnicity, nativity, career length, occupation, and living and working conditions. The questionnaire and format of the demographic questions were developed based on a previous study with input from the authors’ community partners. More specifically, racial and ethnic identity were measured separately because racial/ethnic descriptors are often intersectional and can be described in multiple ways by participants. The racial identity question was multiple choice with the option for free-text response if the participant chose “Biracial” or “Other,” while ethnicity was free-text response (i.e., no fixed options). The demographics section also included questions about whether participants’ work involves the COVID-19 pandemic, either directly through patient contact or indirectly through research regarding prevention and treatment. Profession data were collected by a multiple-choice question asking participants to choose which option best describes their occupation. Participants could choose all professional titles that apply to them from a list of the following choices: Physician (MD, DO), Physician’s Assistant (PA), Nurse (APN, RN CNMS, CRNA, etc.), Mental Health Worker (PhD, PsyD, MSW, MHC, etc.), Scientist/Researcher, Administrative Staff, or Other (fill-in). The questionnaire had two follow-up questions asking for professional title and specialty (both fill-in responses).
Professional Stress Questionnaire. The 20-item Professional Stress Questionnaire (PSQ; Goulia et al., 2010) was originally developed during the A/H1N1 influenza pandemic and assesses concerns about the pandemic, anxieties about perceived sufficiency of information regarding the pandemic, and intended behavior in the daily experiences of healthcare workers and whether these factors are associated with psychological distress. To our knowledge, no data has been collected regarding validity or reliability of the original measure, and it had not yet been adapted to study the COVID-19 pandemic effects on stress. For this study, all mentions of H1N1 language in the PSQ were changed to COVID-19 language. Questions regarding the amount of information received about COVID-19, beliefs about infection and treatment, and overall worry about risk were responded to on a 9-point Likert scale of agreement (i.e., strongly disagree to strongly agree).
The 12-item General Health Questionnaire. The General Health Questionnaire-12 (GHQ-12; Goldberg et al., 1997) is a short, 12-item screening instrument used to detect common psychiatric disorders including symptoms of anxiety and depression. Prior studies exploring the mental health of HCPs during public health crises have demonstrated the measure is reliable, with a Cronbach’s alpha ranging from .80 to .85 (Lee et al., 2007; Nickell et al., 2004). The GHQ-12 uses 4-point Likert scale questions to ask about levels of stress and anxiety relative to how a participant usually feels. Although we used the Goulia et al. (2010) study as a model, we did not conduct scoring for the GHQ-12 as a complete measure; rather, individual question mean scores are described in the results section. Mean scores for individual questions are reported to understand the specific experiences of depressive and anxiety symptomology reported by HCPs overall and by specific profession.
Results
Worry and Psychological Distress Related to the COVID-19 Pandemic
Worry and Psychological Distress of Healthcare Professionals Related to the COVID-19: Dichotomous Variables.
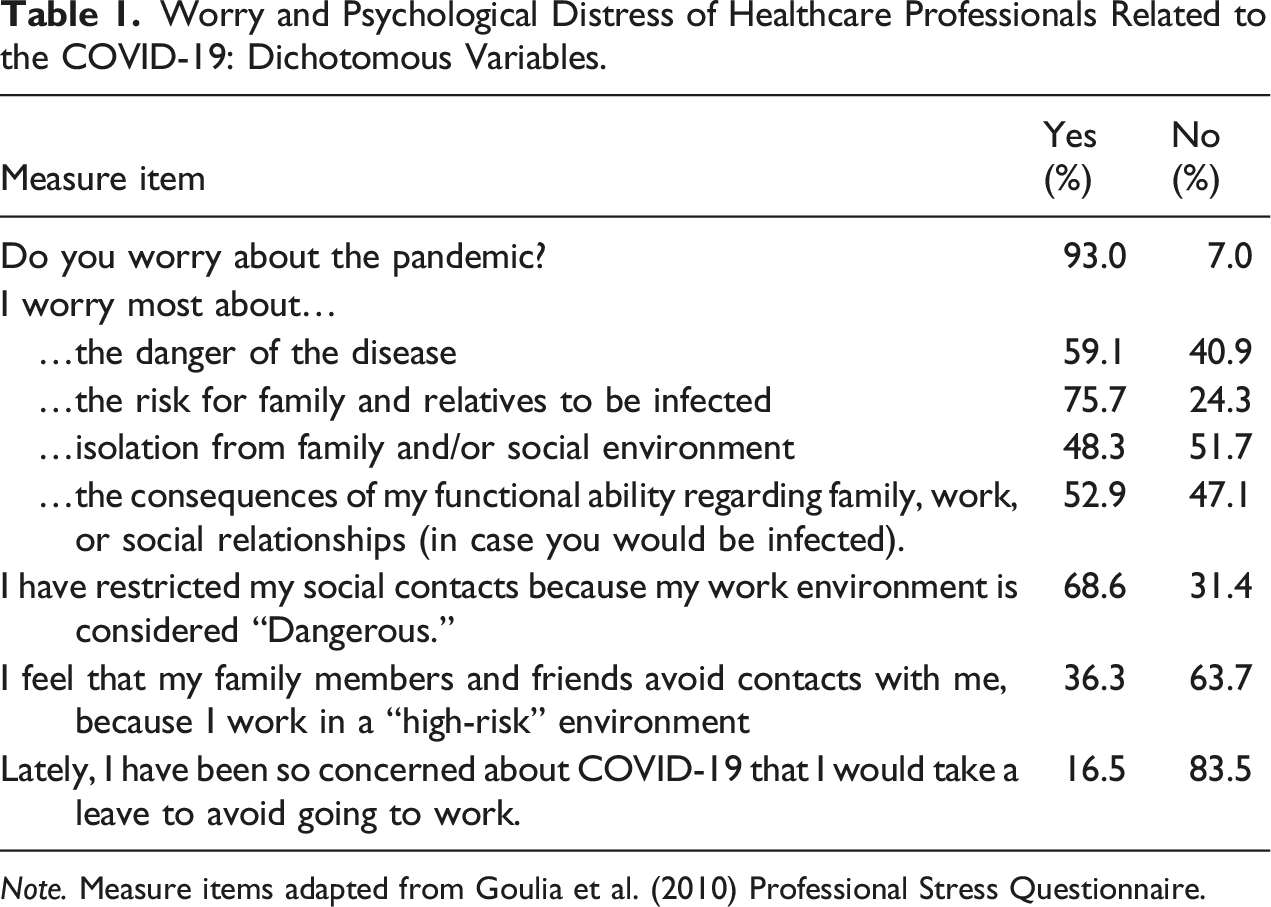
Note. Measure items adapted from Goulia et al. (2010) Professional Stress Questionnaire.
Worry and Psychological Distress of Healthcare Professionals Related to the COVID-19: Ordinal Variables.
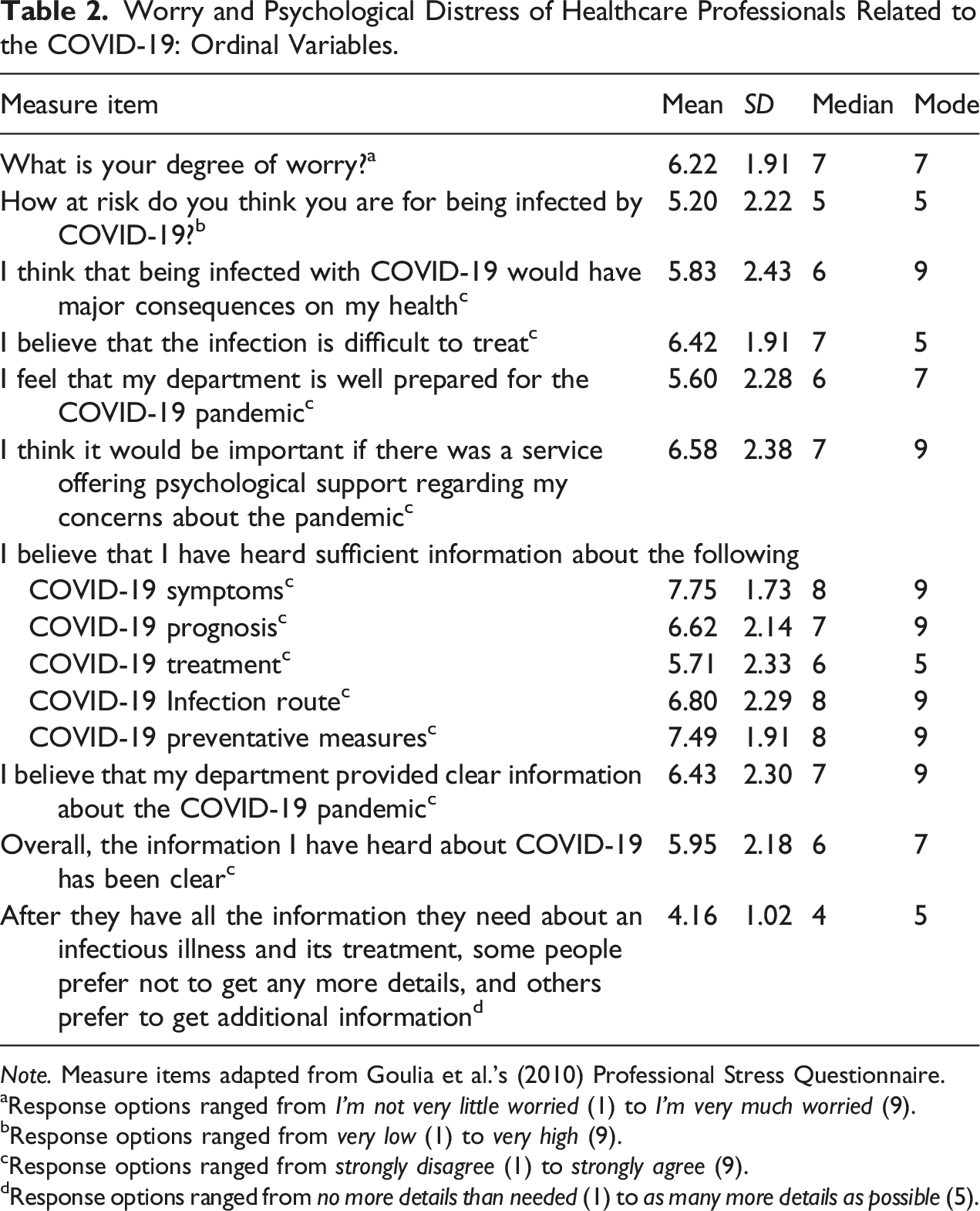
Note. Measure items adapted from Goulia et al.’s (2010) Professional Stress Questionnaire.
aResponse options ranged from I’m not very little worried (1) to I’m very much worried (9).
bResponse options ranged from very low (1) to very high (9).
cResponse options ranged from strongly disagree (1) to strongly agree (9).
dResponse options ranged from no more details than needed (1) to as many more details as possible (5).
Concerns, Worries, and Psychosocial Distress by Profession
The following section details pertinent worries, concerns, and psychosocial distress by healthcare profession.
Physicians. A significant majority (92.8%) of physicians expressed concern about the pandemic. Approximately half (66.2%) of all physicians indicated that their degree of worry was moderate to extreme. Most were primarily concerned about the risk for family and relatives being infected (74.6%), followed by the disease’s danger (71.8%). Further, slightly more than half (89.2%) of physicians have restricted social contacts due to their work environment being dangerous. Slightly more than half of all participants (51.5%) strongly agreed that it would be important to have access to services offering psychological support to help them address their concerns about the pandemic. Almost all physicians (96.8%) indicated they preferred at least slightly more information than the bare minimum necessary for their job. Regarding psychological distress, slightly more than half (56.3%) of physicians have struggled to enjoy their normal day-to-day activities. More than half (59.4%) have felt constantly under strain. Slightly less than half (46.9%) have lost sleep over worry. Slightly more than one-third (36%) expressed feeling unhappy or depressed.
Nurses. A significant majority (91.3%) of nurses expressed concern about the pandemic. Approximately two-thirds (66.7%) of all nurses indicated that their degree of worry was moderate to extreme. Most were primarily concerned about the risk for family and relatives being infected (72.4%), followed by the disease’s danger (59.8%). Further, approximately three-fourths (76.9%) of nurses have restricted social contacts due to their work environment being dangerous. Most nurses (88.8%) strongly agreed that it would be important to have access to services offering psychological support to help them address their concerns about the pandemic; slightly less than half indicated they strongly agreed this service would be important (43.8%) Almost all nurses (90.9%) indicated they preferred at least slightly more information than the bare minimum necessary for their job. Regarding psychological distress, more than half (70.7%) of nurses have struggled to enjoy their normal day-to-day activities, have struggled to feel happy (51.3%), and have felt constantly under strain (71.4%). Approximately half (50.7%) have lost sleep over worry and expressed feeling unhappy or depressed (49.4%).
Mental health professionals. A significant majority (98%) of MHPs expressed concern about the pandemic. More than half (64%) of all MHPs indicated that their degree of worry was moderate to extreme. Most were primarily concerned about the risk for family and relatives being infected (88.9%), followed by the disease’s danger (62.6%). Slightly less than half (44.2%) of MHPs have restricted social contacts due to their work environment being dangerous. More than half (70.8%) strongly agreed that it would be important to have access to services offering psychological support to help them address their concerns about the pandemic. Almost all MHPs (90.2%) indicated they preferred at least slightly more information than the bare minimum necessary for their job. Regarding psychological distress, more than half (66.3%) of MHPs have struggled with concentration and have struggled to enjoy their normal day-to-day activities (70.5%). Slightly less than half (48.9%) of MHPs have struggled to feel happy, losing confidence in themselves (41.1%), feeling unhappy or depressed (44.7%), and more than half (73.4%) have felt constantly under strain.
Allied health professionals. A majority (86.3%) of AHPs expressed concern about the pandemic. Approximately half (61.3%) of all AHPS indicated that their degree of worry was moderate to extreme. Slightly over half were primarily concerned about the risk for family and relatives being infected (61.8%). Further, approximately three-fourths (76.9%) of AHPs have restricted social contacts due to their work environment being dangerous. Slightly less than three-fourths of nurses (72.3%) strongly agreed that it would be important to have access to services offering psychological support to help them address their concerns about the pandemic. Almost all AHPs (95.2%) indicated they preferred at least slightly more information than the bare minimum necessary for their job. Regarding psychological distress, more than half (68.5%) of AHPs have struggled to enjoy their normal day-to-day activities, and slightly more than half (54%) have felt constantly under strain.
Psychological Distress of HCPs with Direct COVID-19 Contact
We compared the responses of the 36.6% of study participants who indicated that they either worked directly with COVID-19 patients or they were working on research directly related to COVID-19 with those who had no direct contact. HCPs working directly with COVID-19 patients and/or research had a significantly higher degree of worry toward COVID-19 compared with peers not working directly with COVID-19, [t(291) = −3.144, p = .002]. Compared to the HCPs not working directly with COVID-19 patients or research, HCPs with direct COVID-19 contact lost more sleep over worry [t(272) = −4.59, p < .001], felt more constantly under strain [t(225.49) = −4.138, p < .001], and had been feeling more unhappy or depressed [t(270) = −2.23, p = .027] during this time period. However, on average, this group was less likely to consider taking leave to avoid going to work compared to peers without direct COVID-19 contact, [t(174.7) = 2.05, p = .042]. Compared to their non-direct contact peers, the HCPs with direct COVID-19 contact felt that they were playing a useful part in things more so than usual, [t(269) = 4.14, p < .001].
Psychological Distress of Minoritized Groups
Half (50.2%) of study participants identified racially and/or ethnically with a minoritized group. Given the unequal burden minoritized groups experienced throughout the pandemic (Chen & Krieger, 2021), a subgroup analysis was done with minoritized HCPs, or HCPs identifying as Black, Hispanic, Asian, Biracial, Native American, or some other non-White race or ethnicity, to determine if this unequal burden was felt in our sample. On average, non-White HCPs were more worried about the pandemic than White HCPs, [t(287) = −3.11, p = .002], with non-White HCPs enjoying daily activities “less than usual” compared to their White peers [t(266) = −2.00, p = .046]. On all other variables related to psychological distress, White and non-White HCPs were experiencing similar amounts of psychological distress and worry.
Discussion
Historically, public health crises have wreaked havoc on the mental health of HCPs (Shah et al., 2020). During and after these crises, HCPs may experience post-traumatic stress disorder (PTSD), depression, anxiety, and burnout (Lee et al., 2018). This study identifies worry and psychological distress in HCPs working during the pandemic, and highlights how these experiences were similar or variable when stratifying participants by professional field. The specific experiences of worry and psychological distress HCPs experienced informs recommendations to improve systems of care for HCPs that put their physical and mental health at risk to address public health crises.
Worry and Psychological Distress of Participants Related to the COVID-19 Pandemic
Most survey participants reported experiencing high levels of concern regarding various aspects of working during the COVID-19 pandemic. This study provides unique insight into the nature of South Florida HCPs worry from April 2020 to April 2021 of the COVID-19 pandemic. Results demonstrated that HCPs worried about not only their own health and the health of their loved ones, but also more broadly about the COVID-19 pandemic itself. The uncertain long-term implications of this sustained worry are a cause for concern as the pandemic continues to impact, and at times overwhelming, medical systems across the nation (Lee et al., 2018; Shah et al., 2020).
Overall, findings related to HCP worry align with studies focused on prior pandemics (Goulia et al., 2010). Specifically, both the current study and prior studies have demonstrated that HCPs experience worry about the fact that their occupation becomes particularly hazardous (Khalid et al., 2016). Further, although this study was limited to South Florida, it is possible that the findings reflect broader, less localized, trends of HCPs’ psychological distress as the findings align with those of its predecessors (Cai et al., 2020; Goulia et al., 2010; Kang et al., 2020; Khalid et al., 2016; Lee et al., 2018; Spoorthy et al., 2020).
The current study findings highlight that HCP experiences with stress, insomnia, emotional distress, changes in mood, and the ability to enjoy day-to-day activities are consistent with previous studies (Lee et al., 2018; Phua et al., 2005; Spoorthy et al., 2020). While this study did not assess the possible causal relationship between pandemic-related worry and psychological distress, it is possible that symptoms of psychological distress (e.g., mood disturbances, insomnia, or other manifestations) inform or are informed by the increased levels of stress HCPs have navigated during the pandemic (Shanafelt et al., 2020).
HCPs Worry, Psychological Distress, and Professional Field
Similar to prior research, some specific experiences of worry and psychological distress shared similarities and differences across HCP fields of work (Centers for Disease Control and Prevention, 2020; Spoorthy et al., 2020). In this study, most physicians experienced increased worry during the pandemic as well as an inability to enjoy normal daily activities, feeling unhappy, losing sleep, and constantly feeling under strain. Nurses also experienced increased worry during the pandemic as well as an inability to enjoy normal daily activities, feeling unhappy, losing sleep, and constantly feeling under strain, but also reported being receptive to the idea of receiving psychological support to navigate the pandemic. The specific worries and psychological distress physicians and nurses experienced may result in long-term consequences (such as developing PTSD) in some cases if not identified by the individual as an issue or adequately addressed (Lee et al., 2018).
Further, high levels of worry in MHPs were associated with increased feelings of indecisiveness. When considering these findings in the context of prior research that indicates symptoms of anxiety lead to impaired decision making, it is possible that COVID-19–related worry is directly impacting MHPs’ ability to make decisions at work (Park et al., 2016). It should be noted that MHPs’ experiences with stress and psychological distress may reflect a systemic unpreparedness to navigate the sharp influx of individuals seeking treatment for an ongoing disaster. Specifically, MHPs typically must seek out specific education or training to treat individuals experiencing or recovering from large-scale disasters; however, due to the specialized nature of this work, it is likely that many of the MHPs serving at this time did not have adequate preparation. This may have implications for the education requirements for MHPs. Moreover, while AHPs demonstrated lesser levels of worry, they still indicated great desire for clear and abundant information.
Lastly, HCPs that work directly with COVID-19 patients and/or research reported a higher degree of worry than HCPs that did not have direct contact. These individuals were more likely to have sleep disturbances, feel constantly under strain, and experience feelings of unhappiness or depression. Considering the higher level of worry and psychological distress these individuals have experienced, it is possible that they may require special attention to navigate both the short-term and long-term impacts of this psychological distress on their mental health. However, it appears that this group experiences the unique protective factor of feeling they are playing a useful part in things to a greater degree than HCPs that do not have direct contact. This protective factor may be leveraged in psychological work with HCPs experiencing psychological distress.
Taken all together, these findings indicate that almost all participants experienced worry and psychological distress related to the pandemic. Further, this study highlighted some similarities and variations in the specific worries, manifestations of the psychological distress, and the relationship between these variables when participants were stratified by field of work. The study’s results signify that HCPs’ mental health suffered across the first year of the COVID-19 pandemic in the United States. While these findings are distressing and possibly unsurprising, they may catalyze action. With a newfound awareness of the specific psychological impacts HCPs are experiencing, these individuals and the institutions that employ them can intervene with these negative outcomes and proactively mitigate further impact.
Systemic Considerations for the Findings
While these findings reflect the experiences of many South Florida HCPs during the first year of the pandemic, they do not fully encompass or reflect the various pre-existing systemic issues aggravated by COVID-19 that may have significantly altered an individual’s experience during the pandemic. This study identified that non-White HCPs experienced a greater degree of worry and were less able to enjoy their day-to-day activities than White HCPs; however, a significantly greater amount of research is needed to understand the nuanced experiences of individuals that hold intersectional identities that may be privileged or marginalized. Understanding the specific phenomenological ways systemic injustice and inequity may have informed individual HCPs’ experiences with the pandemic is unfortunately beyond the scope of this paper. However, it remains critical to acknowledge the systemic factors at play for researchers to address systemic inequity in future research.
Limitations
While the present study has many strengths, the community-based nature of the sample likely limits the generalizability of the findings. However, while the recommendations that follow are inspired by the findings from this community-driven study, they are empirically supported by more nationally representative studies and can likely be effectively implemented in other locations Moreover, because study participants were recruited via convenience sampling, a large percentage of responses were collected from White, US-born, female HCPs. Specifically, study participants were overwhelmingly female, meaning it may be difficult to determine how the findings generalize to individuals that do not identify as female (e.g., males or non-binary individuals). The lack of diversity within this study’s sample should be considered a limitation. Future studies should prioritize collecting data from diverse participants.
Additionally, the Professional Stress Questionnaire (Goulia et al., 2010) used in this study does not currently have any published reliability or validity data since its inception; this should be considered when reviewing results. Lastly, the authors acknowledge that the heterogeneous nature of the data analysis group “allied healthcare professionals” combines a disparate group of people based on their supportive role in the field of healthcare. Future studies should focus on more specific professions that play a supportive role in our healthcare systems to better understand the experience of those that maintain the field.
Recommendations
The findings of this study signal HCPs experienced mental distress from April 2020 to April 2021. This is inherently concerning, considering the role HCPs play in upholding our nation’s public health during the COVID-19 pandemic. Specifically, the current study demonstrates that HCPs experienced increased burden and felt inadequately supported during the first year of the pandemic. Research has demonstrated that these variables may lead to a deteriorated quality of patient care (Sloane et al., 2018). As the emergence of the Delta variant of COVID-19 demonstrated in late months of summer 2021, the pandemic is not over; action must be taken to protect HCP mental health to sustain those that depend on them.
Based on the specific ways that working during COVID-19 affects US-based HCPs’ mental health, the authors of this paper recommend that HCPs and institutions employing HCPs take the following actions to address and proactively mitigate experiences of worry and psychological distress: (a) seek out or provide access to mental health resources and services, (b) engage with or provide opportunities and activities to actively address mental health, and (c) improve communication regarding COVID-19.
Access to mental health services and resources. To remedy ongoing mental health struggles and develop healthy coping skills for future experiences of mental distress, HCPs should seek mental health resources and services such as individual or group therapy. For HCPs unable to engage with psychotherapy in person, telehealth serves as a safe and effective alternative (Shigekawa et al., 2018). Institutions that employ HCPs can play a substantial role in facilitating the usage of mental health resources and services by highlighting their accessible and culturally relevant in-house services. Further, these institutions should be aware that like the lay public, mental health stigma may prevent many HCPs from pursuing psychological services (Wallace, 2012). To lessen the impacts of stigma on HCP help-seeking, institutions may frame their services as supportive or strengths-based programming rather than programming that focuses on deficits in mental health or mental illness (Wallace, 2012). An example of in-house services that institutions might actively advertise is on-site individual or group psychotherapy, such as empirically supported cognitive-behavioral skills training groups (Gardiner et al., 2004).
Providing opportunities and activities addressing mental health. Beyond seeking mental health resources and services, HCPs may engage in activities that facilitate well-being. This might include maintaining a healthy diet, exercising, or connecting with one’s spirituality. Given that mental health stigma may interfere with HCPs’ pursuit of these activities, institutions might invest resources in various empirically based programs designed to support the well-being of HCPs (West et al., 2016). For example, a recent systematic review demonstrated that HCPs found yoga programs helpful for managing stress (Cocchiara et al., 2019). Alternatively, institutions can provide exercise programs to increase psychological well-being in HCPs (Weight et al., 2013) or educational programs that focus on developing skills that promote psychological well-being, such as mindfulness (Fortney et al., 2013; West et al., 2014). To ensure HCPs are able to engage with in-house mental health resources and well-being programs, institutions might protect at least one hour in the HCP’s weekly work schedule.
Improve communication between institutions and employees. Emphasis on mental health awareness in the workplace requires improved communication between institutions and their employees. Institutions can improve communication regarding COVID-19 by adequately preparing staff for the challenges they will face during the pandemic using clear language and no false reassurances (Greenberg et al., 2020). Further, individuals in leadership positions should reach out regularly and often to colleagues and staff members to discuss what aspects of the pandemic HCPs wish to receive more information about or what specific concerns they might have (Greenberg et al., 2020; Shanafelt et al., 2020). Lastly, peer support programs may be implemented to provide a space in which HCPs can openly discuss pandemic-related stress in an affirming and safe environment (Greenberg et al., 2020).
While these recommendations focus on the joint responsibility of HCPs and their employers towards mitigating stress of HCPs, the onus should be placed on institutions hiring HCPs to create an environment promoting health and well-being of their employees and not just the patients they serve. The authors of this paper recommend that hospitals, community clinics, private practices, and all other HCP-hiring entities provide access to mental health resources and services, provide opportunities and activities to address mental health, and improve communication. Not only will this help HCPs mitigate the psychological distress associated with being a front-line worker during a pandemic, but it would also serve as a preventative measure, improving the overall stress tolerance of the workplace and promoting employee well-being.
Conclusion
These findings highlight the experiences of stress and psychological distress South Florida HCPs experienced between April 2020 and April 2021 of the COVID-19 pandemic. More research is needed to understand how the pandemic continues to take a toll on the mental health of HCPs across the United States. The psychological suffering of HCPs serving during a global crisis is an obstinate problem magnified by its far-reaching consequences for public health. Addressing the mental health crisis that HCPs experienced during this pandemic and crises they may face in the future must be a national priority if our healthcare systems are to adequately support the mental health of those who care for the public.
Footnotes
Acknowledgments
We acknowledge Dr. Marie Etienne and Dr. Sidney Coupet for their support in recruiting study participants and disseminating the study recommendations to healthcare professionals.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.