
Abstract
The success and advancement of HIV prevention efforts with emerging adults from minority communities requires continued and diligent collaboration between researchers, community members, and community-based organizations. This paper provides an overview of a 3-year collaboration between a Minority Serving Institution of Higher Education, and a grassroots, minority servicing HIV prevention agency. In South Florida, a geographic area with high incidence of HIV, we relied on community-based participatory research (CBPR) to guide the implementation of culturally, linguistically, and developmentally appropriate HIV prevention programming for 18 to 24-year-old Latinx university students. The project partnership was organized around: (a) integrating community knowledge through formative research to understand needs and determine relevant risk factors, (b) building a highly collaborative relationship between a large academic institution and community-based service provider, and (c) designing and implementing ongoing, strategic environmental prevention activities through community-involved research. We describe the collaborative partnership and multiple prevention strategies that were implemented. The success of the community–university partnership was highly dependent on the depth and breadth of collaboration, mutual support, and respect among collaborators. To advance sexual health promotion programs designed for Latinx emerging adults, we describe lessons learned for future CBPR implementation that focus on involving members of priority populations in research teams, aligning project voices, navigating internal governmental systems, creating mutual and direct benefits of partnership, and utilizing networks to enhance sustainability.
Keywords
Background
Efforts to prevent HIV have been ongoing for four decades (U.S. Department of Health and Human Services [USDHHS], 2021). Together, researchers, service providers, and federal agencies have gathered substantial evidence to identify effective strategies to reduce the spread of new HIV infections and support those living with HIV in maintaining health. The Substance Abuse and Mental Health Services Administration (SAMHSA), as well as other federal agencies, support public health professionals in their implementation of focused and tailored health promotion programs in affected geographic regions and among groups at highest risk of HIV infection (USDHHS, 2020). Moreover, to support those most at risk through strategic prevention efforts and to move prevention science forward, federal and local agencies provide grant funding to community and academic partnerships to provide services and generate prevention research, concurrently (Beer et al., 2019).
Population
In the United States, an estimated 1.1 million people aged 13 years or older live with HIV (Centers for Disease Control and Prevention [CDC], 2020). Of those, approximately 50,900 are young people (i.e., 13–24 years old; CDC, 2020). While HIV affects all groups of people, certain groups and geographic regions maintain higher prevalence and risk than others. In the current project, we focused on a group at the intersection of high HIV prevalence and risk due to age, geographic location, and cultural background: Latinx emerging young adults in South Florida.
South Florida is home to 3 of the 10 metropolitan areas with the highest rates of newly diagnosed HIV in the country (Miami, Fort Lauderdale, and West Palm Beach, FL; CDC, 2018). Specifically, in Miami-Dade County, Latinx populations accounted for 45.4% of people living with HIV in 2018 and are therefore the focus of local community HIV prevention efforts (Florida Department of Health, 2019; Sullivan, 2017). In the U.S. overall, Latinx individuals’ HIV infection rates are 3 times as high as those of non-Hispanic White individuals (Rao et al., 2016). Among Latinx emerging adults (i.e., 18–24 years old) in particular, prevention challenges include high rates of sexually transmitted infections, high numbers of sexual partners, low testing rates, stigma, and inadequate education around HIV prevention (CDC, 2020). Emerging adults are the least likely, compared to any other age group, to be aware of their HIV status, increasing potential risk of transmission (CDC, 2020).
While risky sexual behaviors occur across the life span, emerging adulthood presents itself as a developmental period during which individuals have low perceived risk, limited access to appropriate HIV testing services, and increased substance use, potentially leading to risky sexual behavior (Willoughby et al., 2021). College experience has been associated with an increase in exploratory behaviors (Arnett, 2014) and is associated with increased risk for sexually transmitted infections and risky sexual behavior (Halpern & Kaestle, 2014). Moreover, college attendance is a risk factor for binge drinking, placing college students at a unique risk of adverse consequences; for example, when a person is drunk or high, they are more likely to engage in risky sexual behaviors, such as having sex without a condom, which is particularly true for South Floridian colleges (Trepka et al., 2008). In 2019, college students had a considerably higher prevalence (33%) of binge drinking (five or more drinks in a row at least once in the past 2 weeks) than their non-college peers (22%; Schulenberg et al., 2020). Because of unique and compounded prevention challenges, efforts designed to address HIV among Latinx emerging adults in university settings are needed and require development and access to relevant information and services that are responsive to their situations and needs.
CBPR Approaches to Address HIV in Latinx Emerging Adults
Community-based participatory research (CBPR) has been a successful approach to improving health outcomes in young adult Latinx populations (Suarez-Balcazar et al., 2018), providing important insight into the lived experience of Latinx young adults (Guarnero, 2013), and providing insight into what is needed to make prevention and intervention efforts effective and culturally tailored (Fernandez et al., 2018; Rhodes et al., 2014). However, there remain considerable obstacles to successful implementation of HIV testing programs including basic accessibility (Boyd et al., 2020; Carnevale et al., 2020). Guilamo-Ramos and colleagues outline large-scale priority areas to address HIV in Latinx populations, which include (a) the reduction of HIV stigma, (b) increasing access to treatment, (c) the development of tailored interventions, and (d) keeping in mind the diversity within the Latinx community, including sexual and gender diversity (Guilamo-Ramos et al., 2020). CBPR approaches offer practical and significant promise to addressing these continued health priority areas and needs.
In CBPR efforts designed for minority communities, constructive relationships between academic and community-based agencies (i.e., community–university partnerships) contribute positively to effective HIV programs, yet difficulties in these relationships have challenged the planning and implementation of effective HIV prevention efforts (Wilson et al., 2018). Barriers to effective collaboration between academic institutions and community-based agencies include historically justified mistrust among partners, conflicting priorities, slowed decision making, and lack of willingness to share resources (Drahota et al., 2016). On the other hand, major benefits include improved program delivery and increased access to and use of programs and resources that are community driven (Drahota et al., 2016), as well as co-creation, or production of collaborative knowledge (Greenhalgh et al., 2016). Truly collaborative partnerships are thought to be those in which members of multiple organizations share vision, mission, power, and resources, to work together to achieve a desired goal (Hogue et al., 1995).
Systematic reviews of the literature have established the utility of CBPR in addressing health among racial and ethnic minority groups in health promotional programs and clinical trials (McFarlane et al., 2022). Despite this, research is needed to improve the effectiveness of CBPR efforts. For example, in a recent systematic review of CBPR sexual health interventions designed for racial/ethnic minorities, researchers identified substantial variability within CBPR studies regarding the description and role of community partnership (McCuistian et al., 2021). Findings underscore the need to be more transparent and thorough in the description of the role of the partnership, given that lack of description and detail hinders analysis and replicability in future research (McCuistian et al., 2021).
There is a need for increased dissemination of lessons learned and successful collaboration components, as well as targeted effort to report specific details on the roles played by community members in programs and partnerships. These contributions can be important for replication, can help advance best practices and, ultimately, improve access to and quality of evidence-driven HIV prevention services for communities of focus. The current paper seeks to build on existing targets and literature for CBPR development by outlining the activities of a project that was successful in increasing the availability and accessibility of rapid HIV care testing services as a screening tool for the detection of HIV infection among Latinx emerging adults in an urban, minority-serving university, through a highly collaborative community–university partnership.
Project Purpose
The project at hand was a 3-year partnership funded by SAMHSA (MSI community-based organization [CBO] Grant Number SP020653). The project brought together (a) a large urban, minority-serving institution of higher education with 58,836 students enrolled in 2020 to 2021 (70% of undergraduate students identifying as Latinx); (b) a grass roots community-based HIV/sexually transmitted infections testing agency in South Florida; and (c) a Latinx-led media consulting company. The project was developed in response to the high rates of HIV infection among Latinx individuals in the community and a need for developmentally and culturally responsive efforts to address these health disparities. The goals were to provide comprehensive, integrated implementation of prevention and testing strategies tailored for Latinx emerging adults in the university community. Program components included (a) increasing access to and utilization of on-campus HIV testing and (b) disseminating an environmental prevention campaign to spread prevention information, resources, brochures, flyers, newsletters, and so on across the college campus community.
The CBO that was the key service partner in this project was established in 1998 as a public health program designed to provide targeted HIV/AIDS prevention services to the highest risk populations throughout Miami-Dade County, Florida, specifically the Latinx community. Program materials and services offered by the organization were bilingual and were managed and administered by Latinx staff. Services and interventions provided included rapid HIV testing, linkage to care for those living with HIV, condom distribution, and comprehensive risk counseling services with a focus on adapting services for Latinx communities. The CBO received funding from several funding streams but was mainly dependent on funding sources through the state, primarily the Department of Health.
Project Methods
To achieve project goals, we employed a CBPR process that involved the team consisting of academic researchers, members of the CBO, media consultants, and student/community volunteers. Informed by the CBPR conceptual model developed by Wallerstein et al. (2020), we describe the intervention and research process that guided the success of the partnership, which included: (a) integrating community knowledge through formative research to understand needs and determine relevant risk factors, (b) empowering processes to build and maintain a highly collaborative relationship between a university and a community-based service provider, and (c) designing and implementing ongoing strategic environmental prevention activities through community-involved research. In this project, the community refers to the university student body that was 18 to 24 years old and identified as Latinx, which was the priority focus of the tailored program efforts. Table 1 provides an overview of the key phases and corresponding primary activities that are described below in further detail.
Overview of Intervention and Research Phases.
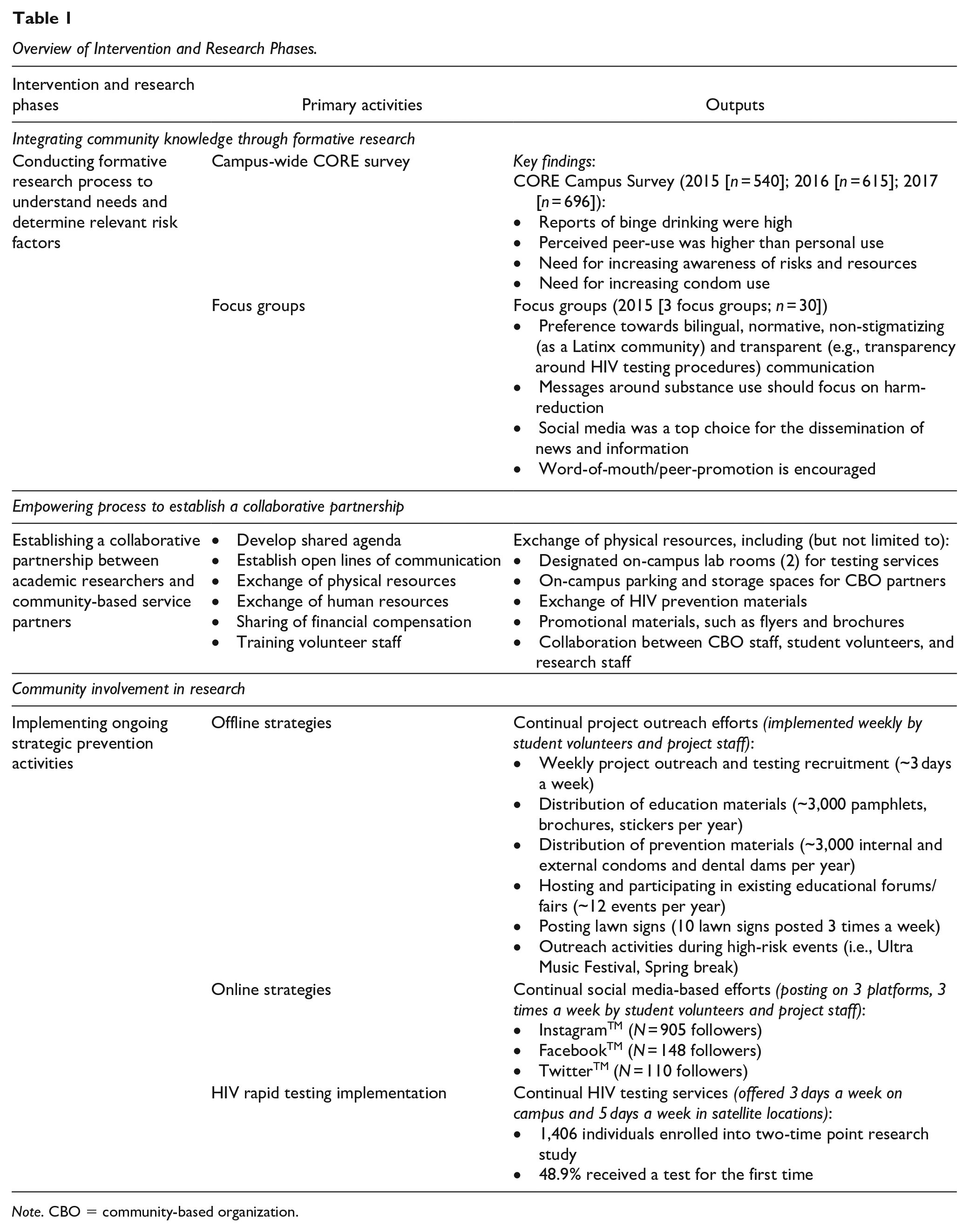
Note. CBO = community-based organization.
Integrating Community Knowledge Through Formative Research
To assess and integrate community knowledge into the project efforts, the research team conducted a two-part formative research process to better understand needs and determine relevant risk factors among the population of interest. First, researchers conducted a campus-wide needs assessment using the Core Institute Campus Norms Survey of alcohol and other drug use norms (Presley et al., 1994), which was used to assess a range of health behaviors including participants’ (mis)use of drugs and alcohol, HIV testing and prevention awareness, sexual risk behaviors, and media uses and preferences for health communication. The needs assessment survey was distributed electronically to all Latinx students aged 18 to 24 during the first year of the project (2015) and was disseminated in the same semester for the subsequent 2 years of the project to the eligible student body (Year 1: n = 540, Mage = 21.2, SDage = 1.9, 66.3% female; Year 2: n = 615, Mage = 21.2, SDage = 3.0, 69.6% female; Year 3: n = 696, Mage = 20.8, SDage = 2.8; 63.9% female). Results from this needs assessment identified main areas of focus in Year 1 of the project that would drive the direction of program development and served to evaluate continued needs in the subsequent 2 years among the student body.
Second, as a part of the formative research process, researchers conducted four focus groups with students from the population of interest in Year 1 of the project (n = 30, Mage = 21.2, SDage = 1.9, 63.3% female). The purpose of conducting the focus groups was to gain insight into the unique perceptions of the population of interest regarding their identified needs and preferences, namely around prevention testing and service implementation. Focus groups were used as a tool to explore and understand cultural assumptions, assess and prioritize areas of greatest perceived need, tailor education and outreach materials to the key values and beliefs of the population of focus, and to understand and capitalize on favored communication to reach project goals (see Fernandez et al., 2018, for full details on focus groups implementation).
The formative research process, which included both the campus needs assessment and the focus groups, highlighted salient risk factors among the Latinx emerging adult population of focus, and findings were used to directly involve the priority population’s knowledge in the tailoring and development of prevention programming. Results from the campus norms survey and focus groups indicated the need for increasing accessibility to free and convenient HIV testing (e.g., quick results, easy to access), increasing awareness of risks and resources, increasing condom use, and decreasing binge drinking and drug use while having sex (i.e., adopt a focus on harm reduction; Marlatt et al., 2011). Results also indicated that students viewed social media as the top choice for the dissemination of news and information, and students preferred bilingual, normative, non-stigmatizing (as a Latinx community) and transparent (e.g., transparency around HIV testing procedures) communication around HIV prevention services (Fernandez et al., 2018). The prevention strategies over the course of the 3-year project were designed and implemented to directly address the risk factors identified in the formative research process and incorporated both online and offline strategies to implement strategic prevention efforts.
Empowering Processes to Build Highly Collaborative Relationships
To accomplish project goals through a collaborative relationship among the project team members, consistent meetings were held to build a shared agenda that incorporated the vision and values of all entities. During early stages of the project, meetings were held biweekly and were explorative in nature. Initial meetings were run with broad agendas to facilitate idea sharing and encourage open communication. While all entities were committed to addressing the project goals from the advent of the project, the different entities involved initially had distinct ideas about how to accomplish the study’s goals. While media consultants were more comfortable with provocative messages and avenues (including the incorporation of Miss Universe pageant contestants as spokespersons for HIV testing), academic researchers tended to have difficulty with the creativity needed to engage an emerging adult audience in sexual health promotion topics. This posed challenges for collaborative efforts, and numerous discussions were necessary to reach consensus regarding the tone, images, style, and content of campaign messages, as well as an understanding of the context and systems in which each entity operates. Significant time and energy were dedicated to understanding value systems of all those involved through continued and highly engaged meetings where all entities were needed to contribute to dialogue and discussion of the project vision. This development stage was critical to merge different ideas into a larger vision giving testimony to all entities’ expertise and perspectives, while also considering the findings from the needs assessments and focus groups. Ultimately, final campaign decisions were guided by feedback from the population of interest, whose preferences were prioritized in terms of developmental, cultural, and linguistic appeal of messaging, in line with contemporary CBPR models (Wallerstein et al., 2018).
Consistent in-person meetings were essential in the development and establishment phase of the project, and it was also critical for team members to maintain open lines of communication throughout the 3-year project implementation. Formal meetings were held monthly from the second year on. Consistent and open lines of communication (via email, telephone, and/or in-person meetings) allowed the team to handle implementation challenges in a united and efficient manner, and systematized monthly meetings allowed for a consistent in-person platform for discussion and problem solving.
An integral part of the process to build the collaborative relationship included an established exchange of resources between entities. This included sharing physical lab testing space, human resources and staff, expert knowledge from academics and providers alike, and prevention materials, such as educational materials and condoms. University partners worked diligently with the university administration to secure clinical lab testing rooms on campus for service providers to utilize for on-campus testing. Conversely, the service providers shared acquired prevention materials (i.e., internal and external condoms, educational resources, and pamphlets) with the student volunteers to disseminate to the population of interest. This sharing of resources contributed greatly to the successful collaboration between partners by establishing an infrastructure to provide HIV testing and prevention materials in a convenient manner and provided access to resources for the population of interest.
Another important aspect of building a truly collaborative relationship was sharing financial resources, particularly grant dollars. As primary investigators, the academic institution applied for, secured, and managed budgetary aspects through the support of their university’s budget administration. But, importantly, the CBO staff and leadership were not only substantially involved in decision making and project activities but were also financially compensated through grant funding for their involvement and efforts. Although the CBO did not receive any indirect costs and were not paid for the use of their facilities, there was a sharing in both funding support and spaces where the project activities (i.e., HIV testing) took place (i.e., at the university clinical lab rooms).
Strategic Prevention Through Community Involvement in Research
Strategic prevention activities included offline and online HIV prevention messaging as well as HIV testing services provided on campus. Project materials, which were launched at the culmination of the formative research period, included creation of a project campaign that focused on “hump day” testing (testing originally occurred on Wednesdays and later expanded to 3 times a week) and disseminating normative, harm reduction messaging called, “Tips for a smarter turn up” (colloquial slogan coined by student team members). Over the course of 3 years, a team of over 30 student volunteers were trained to assist in the implementation of project outreach and awareness activities. The student outreach team gave life to the project in the form of community member representation and interaction with the community of interest through outreach, tabling, attendance of events, and collaboration with other campus organizations. In-depth and in-person trainings occurred each semester throughout the course of the project to train and involve student volunteers in project tasks. While the training typically began with extensive information on the department, community partners, and study information, the goal of the trainings was to emphasize cultural responsiveness and youth empowerment, two values that were central to the daily decision making within the project team, as well as normalizing positive preventive behaviors (e.g., HIV testing and condom use). Training topics for student volunteers addressed multiple implementation domains, including recruitment, informed consent for testing, testing procedures, social media dissemination, and communication strategies. Trainings helped prepare dedicated student volunteers to assist in project implementation, increasing community involvement in the research process. The trainings were led by experienced senior staff with Dissemination & Implementation and clinical expertise. Ultimately, the student volunteers were prepared to utilize several multimedia and multiplatform prevention strategies yielding both offline and online methods of implementation.
Implementation Activities
Offline Strategies
The main offline strategies utilized included project outreach, distribution of educational and prevention materials during event-specific targeted events, and participation in educational forums/fairs that were led by student volunteers. Project outreach, in the form of presentations and distribution of educational materials, took place at both on- and off-campus locations to increase capacity to reach the population of focus. Student volunteers led efforts in identifying creative and relevant events/locations of outreach and scheduled events around the clock (both day and night) to reach a wide audience. Promotional and education materials were distributed at selected high-foot traffic areas on campus including, but not limited to, the student center, library, student health services clinic, campus restaurants, game rooms, parking garages, health fairs, and campus building breezeways. Large lawn signs were placed around the campus to notify students of testing and provide information specifying the established on-campus testing site location. Regular team meetings were used to consistently adapt to the most effective locations and outreach strategies, speaking to the dynamic nature of the implementation process.
The project team also identified and attended events that posed a risk for elevated drinking (Neighbors et al., 2011), with the help of the student volunteers, to implement event-specific outreach for risk reduction and resource awareness. The team was particularly active during identified events associated with elevated drinking and risky behaviors among college students, including during orientation and beginning-of-the-school year events, homecoming, spring break, Cinco de Mayo, New Year’s Eve, and tailgating events. For example, during the week prior to spring break, leaders of fraternities and sororities were invited to participate in a risk-reduction educational event. The session was designed to offer resources and tips for staying safe to influential members of the university’s Greek community.
Last, educational forums, fairs, and presentations occurred 2 to 4 times each semester and were designed to be both informal and interactive. Interactive activities included board games, a spinning-a-wheel game, walking the line with impairment goggles (to mimic the effects of alcohol intoxication), and practicing internal and external condom use on plastic models. Giveaways included HIV prevention materials (e.g., condoms, information resources from the community partner) and promotional materials (e.g., candy, stickers, and campaign branded sunglasses). Educational forums were ongoing and included activities hosted by the project team as well as attending existing activities across campus where the project team provided materials and presented program information.
Online Strategies
In addition to offline efforts, the project incorporated online efforts to cast a larger net of reach than would have been possible through offline efforts alone. The team disseminated online messaging tailored for specific events and utilized strategically timed messages with information intended to reduce the likelihood of problematic drinking, drug use, and unprotected sex by providing tips for harm reduction behaviors (see example of online posts in Supplemental Materials). The project staff actively posted and promoted the online social media campaign through weekly posts (three posts per week) on FacebookTM, InstagramTM, and Twitter TM. Social media messages centered on empowering students to get educated about prevention behaviors and to know their HIV status. These messages also provided facts about alcohol and drug misuse and quick educational tips for risk reduction. The posts were organized to cover four main content categories, in line with online communication best practices: (a) campaign promotion (promoting the campaign’s outreach and social media platforms); (b) cross promotion (promotion of on-campus services for health and mental health services); (c) health education news (promotion of healthy behaviors, particularly regarding substance use and sexual behavior); and (d) human interest (holidays, stories of individuals, etc.; Ramanadhan et al., 2013). The project’s social media platforms were used as an additional avenue to promote engagement and discussion with the population of focus. Benefits of online strategies included private, targeted, and timely response to questions and delivery of available service information, as well as an additional avenue for dynamic engagement with health information (see Fernandez et al., 2019, for details of social media-based messaging efforts).
HIV Testing (Offline)
HIV rapid care testing, made available through the CBO, was offered 3 times a week on campus in a secured lab testing space. Testing included both on campus (university testing lab space) and off-campus locations (through mobile van testing and satellite locations in the downtown area of the city). Although the number of individuals tested prior to the project were not systematically captured, the project resulted in significant increases in both capacities to provide HIV testing and use of HIV testing on campus. Prior to this project, HIV testing on campus was limited to during medical health visits at the campus clinic. A total of 2,097 Latinx emerging adults between the ages of 18 to 24 were tested for HIV over the course of the study period, between June 2015 and September 2017. Moreover, as a part of the research process, the project team recruited a convenience subsample of 1,406 Latinx 18 to 24-year-olds who received an on-campus HIV test from 2015 to 2017 to participate in a two-time point research study after utilizing HIV testing services. To be eligible for this study portion, individuals needed to be: (a) between the ages of 18 to 24, (b) self-identify as Hispanic/Latinx, (c) receive an HIV test, and (d) agree to participate in the research project. The sample (n = 1,406) had a mean age of 20.4 years, was 50.7% female, 63% U.S. born, and predominantly identified as heterosexual (73.5%).
Participants completed an in-person baseline survey at their HIV testing session and completed a similar survey 1-month later via Qualtrics, an electronic survey platform. The survey instrument included questions about demographic characteristics (e.g., age, sex, country of birth), previous HIV testing, barriers to HIV testing, cues to action to receive HIV testing, and attitudes about condom use. Since our project involved a campaign to increase awareness and recruitment of testing, we were interested in understanding which components of the project prompted individuals to carry out the actual HIV test. To assess cues to action, respondents were asked what prompted them to be tested with the following response options: informational flyers or cards, lawn signs, friends, table event on campus, social media, jumbo screen messaging, and/or fraternity or sorority. To assess changes in attitudes about condom use, two questions were asked that were measured on a 4-point Likert scale. The first, “The advantages/benefits of using condoms during sexual intercourse are,” had response options ranging from “not at all important” = 1 to “very important” = 4. The second, “Indicate how confident you are that you could use a condom correctly during your next sexual intercourse act,” had response options from “not at all confident” = 1 to “very confident” = 4.
Descriptive analyses were conducted at baseline, and within subjects repeated measures ANOVA was used to examine changes in attitudes from baseline to 1-month follow-up. Key findings from this assessment identified that, among this subsample of individuals, 48.9% reported it was their first time getting tested for HIV. Surveillance testing rates among Latinx emerging adults varies, but this is higher than other estimates that indicate emerging Latinx adults have HIV testing prevalence rates as low as 26.8% and 46.5% among males and females, respectively (Van Handel et al., 2016). Our number of first-time testers was also just above the national estimates provided by CDC (2018, 2021) that reported 45.3% of Hispanic adults over 18 had ever been tested for HIV. Moreover, as a part of our study, there were small but significant gains from baseline to 1-month follow-up in perceived advantages of condom use, F (1, 632) = 4.96, p = .026, η2 = .01, and confidence in condom use, F (1, 631) = 3.97, p = .047, η2 = .01, though we cannot say for certain which elements of our program contributed to these improvements. Further details and limitations of this two-time point assessment are reported below and in Clarke et al. (2020).
Lessons Learned and Implications for Future Research
This paper outlines a project that was organized around a three-part, CBPR-informed process, where, through a formative research process to integrate community knowledge, an empowering process among collaborators, and community involvement in the research project, we were able to implement relevant and tailored intervention strategies, create partnership synergy, and implement systematic research designs to inform and guide project activities. The project partnership reflects the values of the CBPR intervention and research process and provides practical insights into a community-university’s program implementation. With the collaboration of dedicated and trained student volunteers as well as a grass-roots community-based organization, we were able to recruit and encourage thousands of Latinx emerging adults to engage in prevention services—about half for the first time—by normalizing testing, empowering emerging adults, increasing access and availability, and further attuning our strategies to their preferences and voices. There were a few key lessons learned to highlight.
Involving Members of Community in Research Teams
A key lesson from this project was the importance of involving members of the community in the research team from set-up of the project to end phases. Involving members of the community in the research team included meaningful participation in decision-making, daily tasks and roles, and leading project implementation efforts. For example, student volunteers (whose demographics represented the priority audience) led efforts to identify key events that would be high-risk and thus good targets for prevention efforts. They also led all outreach and recruitment efforts as well as educational forums and fairs that were a part of offline efforts. Moreover, student volunteers contributed to social media plans and used their personal accounts to draw attention to the project’s accounts. This helped increase the authenticity and reach of the online presence as well as normalized content by establishing a peer-led approach. Ultimately, this lesson learned speaks to the infrastructure the project built, which is inherently characterized by being community-informed such that it was by and for the community.
Mutual Support and Respect
Next, the level of collaboration and commitment between the university, CBO stakeholders, and community members was a key facilitator for success and was critical to establish mutual support and respect. Clear and open communication was essential among and across all entities involved. By serving as a university liaison, the student volunteers and project researchers were able to ensure that CBO staff could access and utilize the space to provide free testing to the student body. Showing continued and daily support of services and CBO staff allowed researchers to demonstrate that the project was not simply in the pursuit of scientific endeavors but also valued prevention and testing service provision. This relationship of mutual support and respect was critically important to cultivate. The synergistic union of practical “front line” experience with knowledge of theory and strategic implementation skills greatly improved both the quality of services delivered and the procedures utilized to guide project strategies (Harper & Salina, 2000).
Moreover, the success of HIV testing was dependent on a strong, trusting relationship between CBO staff and academic researchers, as well as between the CBO staff and student volunteers. The HIV testing was led by the CBO testing staff, while the recruitment and promotion of the testing was run by the student volunteers. Each volunteer was in charge of different weekly tasks ranging from recruiting individuals for testing, disseminating information about HIV testing, distributing free HIV prevention materials (e.g., internal and external condoms), and leading educational and outreach events. They were trained on ethical research implementation and included in brainstorming and planning meetings. Student volunteers were integral to deciding the locations and events of highest importance and gave life and voice to the messages of the project.
Aligning Project Voice
Despite the partnership’s success, aligning the project’s advocacy and awareness efforts within the university guidelines and community’s context was a challenge. Discrepancies arose between what entities perceived as appropriate for a sexual health promotion campaign as well as what was deemed creative enough to engage an emerging adult audience. This posed as a challenge for collaborative efforts, and numerous discussions were necessary to reach consensus regarding the tone, images, style, and content of campaign messages. The complex context in which HIV infection and treatment occurs requires not only biomedical and behavioral advances but is also highly dependable on social support and acceptance (Qiao et al., 2014; Turan et al., 2017). Ultimately, the lesson learned is that persistence and commitment in understanding value systems of those involved allowed for maximization of the expertise and contributions of each entity, while the involvement of the population of interest allowed for checking the cultural and developmental relevance.
This project employed multimedia, multi-channel strategies to increase the ability to reach the population of focus, a decision that was shaped by formative research phases and community input. This multi-channel approach contributed to the reach and success of our project efforts. Offline strategies such as distribution of educational and prevention materials during event-specific, targeted events and participation in educational forums and fairs offered diverse opportunities for the distribution of prevention resources. Online strategies included providing real-time updates, messaging with risk reduction tips, and linking students to available offline services. The concurrent use of both off- and online efforts increased our capacity and ability to reach our population of interest and provided ways to allow for private communication to protect confidentiality when desired by participants, an important consideration to reduce stigma and increase options of health information accessibility for Latinx emerging adults (Fernandez et al., 2018).
Navigating Internal Governmental Systems
Navigating the internal governmental system of one of the largest colleges in the United States was a challenge. Previous research on collaborative partnerships has found that differences in organizational culture contribute to delays in making joint decisions (Drahota et al., 2016). Partnership cohesion allowed the partnership to clear institutional hurdles in a united manner. Through the commitment and training of student volunteers as well as with support from higher level research-involved faculty (Zimmerman, 2019), we were able to host outreach events in most university locations with very few exceptions. Apart from persistence, clear communication and a trusting relationship between the CBO partner and academic partner were key in overcoming institutional barriers (Bernal et al., 2004). Finally, the research team’s cohesion, rapport, and trust ultimately benefitted the project significantly by allowing the research team to achieve goals in a united manner when facing challenges to project implementation. A strength of the CBPR approach is to develop program and interventions that are not only practically significant for community members but that also address politically and systematically rooted systems by involving larger systems (i.e., institutions) in partnership processes (Holliday et al., 2020).
Creating Mutual and Direct Benefits of Partnership
While the project success represents mutual benefits of reaching program goals to increase access and use of HIV testing services, it is also important to note the ways in which the CBO directly benefited from this project. First, the CBO was provided with the financial resources and physical space to carry out services, including funding for supplies, testing kits, and support for the personnel needed to carry out project activities. In line with the long-term nature of this project, the CBO was included as a subcontract in the partnership and was financially compensated over the course of the project, on a monthly basis to provide financial resources, continually. Second, as a part of the collaborative nature of this project, the CBO was supported with the research personnel to facilitate and manage the research components that were embedded within the project’s development and implementation, including recruitment into HIV testing services. Limited human resources and funding is often a challenge for CBOs, particularly around research activities, because priorities are often more aligned with service provision. Shared physical spaces (i.e., clinical lab spaces) and personnel (i.e., research study staff) were key components for partnership success. Furthermore, through this partnership, the CBO had direct access to provide services to the community of university students, which they would not have had otherwise without the partnership. A strength of this partnership was allowing each entity involved to contribute its resources and access to benefit the other entities. CBO HIV testers were able to bring their expertise of testing and counseling, while researchers were able to facilitate the strategic research process and were able to directly involve university students. These are important takeaways since the logistical benefits of an academic–community partnership from the CBOs perspective are often overlooked. Finally, an additional benefit was the recognition that the CBO received through their impact and service provision. Through this project, results were disseminated at several local and national conferences. Moreover, the chief executive office of the CBO was recognized by the local community and was awarded with recognition at an award ceremony for individuals whose work made significant impact on the public health and social welfare of the South Florida community.
In terms of direct benefits to community members or student volunteers, the majority of whom were from backgrounds underrepresented in health science, working on this project created opportunities for both personal health promotion as well as the development of team and leadership skills by working as a part of a large team. Many of the student volunteers have gone on to pursue degrees in medicine, social work, health promotion, and other applied health professions. Working on this project served as a tangible opportunity to increase skills, networks, and references to build their portfolios. Most importantly, the student volunteers learned hands-on CBPR skills, further building a future workforce that is able and willing to conduct proper CBPR. The project trained dozens of master’s in public health practicum students, many of whom have remained in the HIV field after graduating from the university.
Utilizing Networks to Enhance Sustainability
Israel et al. (2008) set forth guiding principles for successful CBPR with minority communities, which include balancing research and action for the mutual benefit of all partners, disseminating findings and knowledge gained to the community, and promoting a long-term commitment to sustainability. Importantly, the success of this partnership also resulted in continued federal and institutional support to continue offering these prevention efforts to our population of interest for a continued period. Per late 2020, we have provided these services for three additional years, and our reach and service availability have increased. With the support of federal funding, this project not only brought together the researchers, CBO staff, and student volunteers, but also brought together numerous departments within the university. Representatives from the university’s student affairs, counseling and psychological services center, the student health clinic, the university’s Alcohol & Other Drug Task Force, and academic health centers were actively involved in project development and implementation and helped us reach our goals. We learned that the involvement of many of the community’s established service providers benefits not only the community members of focus but all entities who seek to service those individuals.
To further address sustainability, we connected the CBO to other units on campus and trained the campus health clinic staff on culturally competent HIV testing and counseling procedures for Latinx populations. Moreover, as a part of sustainability plans, we transferred the program campaign (including the online social networking accounts) to the university health clinic to further embed the campaign into continued health efforts and interventions beyond the life of the federal funding of the project.
Limitations and Implications for Future Research
Because we were implementing a large, multi-component prevention program, it was difficult to ascertain which particular CBPR components resulted in the greatest impact. Environmental prevention components including online and offline strategies were often implemented simultaneously. Future studies may systematically track this, if it is not detrimental to service provision. Similar to other studies that used CBPR among racial and ethnic minority groups, we cannot claim any causal inference that links our CBPR methodology to specific outcomes in this current study (McFarlane et al., 2022). While this is a limitation, it is inherent to real-world, community-based studies. Next, the program development and progress were unique to the location, history, and positioning of the university and the CBO, providing unique insight into this population and community. Similarly, future projects may consider the implementation of similar programs in other university settings, which may vary depending on other factors such as makeup of the student body, institutional involvement, and so on. An additional point of improvement includes the sample used for the needs assessment (Core Institute Campus Survey), which was a relatively small sample, based on convenience sampling, and may, to some degree, lack comprehensive representation regarding the institution’s Latinx student body’s demographics. Similarly, the individuals enrolled in the research component after HIV testing were a convenience sample of 18 to 24-year-old Latinx individuals who opted for testing. Despite these limitations, we believe that our process can serve as a model and provides a comprehensive overview of our program and partnership.
Conclusions
This paper details the implementation of a health promotion and HIV prevention project that involved a community–university partnership that exceeded project goals in providing and increasing access to HIV prevention and testing services tailored for Latinx emerging adults at a minority-serving institution. This study furthers the literature on the development and implementation of health promotional practices by providing detailed strategies for implementing HIV prevention strategies for Latinx emerging adults in an educational setting and providing comprehensive program descriptions including details of needs assessment and intervention strategies for achieving health promotional goals. These key lessons learned included the factors contributing to the success of our community–university partnership, which was highly dependent on the level of collaboration, mutual support, and reciprocal respect among its members. We suggest that continued collaborations are needed as we move into the final decade towards ending the epidemic and recommend that community–university partnerships be used to tailor strategies to address relevant HIV-related barriers in order to effectively reduce health disparities among communities of focus. Our findings suggest that to strengthen the ability to reach health promotional goals when designing HIV testing programs for Latinx emerging adults, community–university partnerships will need to ensure attention to involving community members in research teams, aligning project voices, navigating internal governmental systems, creating mutual and direct benefits of partnership, and utilizing networks to enhance sustainability.
Supplemental Material
sj-docx-1-prv-10.1177_26320770231189182 – Supplemental material for Lessons Learned From a Community–University Partnership to Increase HIV Testing Services for Emerging Adults at a Minority-Serving Institution
Supplemental material, sj-docx-1-prv-10.1177_26320770231189182 for Lessons Learned From a Community–University Partnership to Increase HIV Testing Services for Emerging Adults at a Minority-Serving Institution by Sofia B. Fernandez, Rachel D. Clarke, Robbert J. Langwerden, Katherine R. Perez, Melissa Howard, Michelle M. Hospital, Staci Leon Morris and Eric F. Wagner in Journal of Prevention and Health Promotion
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge funding from the Substance Abuse and Mental Health Services Administration-sponsored FIU MSI CBO Grant Program (SP020653) for this work and support from the National Institute on Minority Health and Health Disparities Research-sponsored FIU Research Center in Minority Institutions Program (U54MD012393). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.