
Abstract
Zygomatic arch fracture is not uncommon, but due to being a closed fracture most of the time, it is often missed during initial clinical examination. Medially displaced zygomatic arch fractures, if left untreated, can lead to restricted mouth opening due to the impingement of the coronoid process, and this can lead to poor quality of life. In this report, we are going to discuss a case of restricted mouth opening due to a medially displaced, malunited zygomatic arch fracture, which was treated successfully by intraoral coronoidectomy.
Introduction
The zygomatic bone plays an important role in maintaining normal facial width and the projection of the midface. Among maxillofacial fractures, zygoma fracture is one of the most common fractures,1-3 due to its prominence, but it is often overlooked during the initial clinical examinations. Medially displaced zygomatic arch fracture, if left untreated, can significantly lead to functional problems in the form of restricted mouth opening due to impingement of the coronoid process. 4 If such a displaced zygomatic arch fracture is identified immediately after trauma and managed properly, then the outcome will be achieved optimally, but if zygomatic arch fractures are ignored or missed during the initial clinical examinations, then it can lead to malunion, which in turn leads to trismus and cosmetic deformity. Here we are presenting a rare case of trismus secondary to a medially displaced malunited comminuted zygomatic arch fracture treated successfully.
Case Report
A 23-year-old male reported to the Oral and Maxillofacial Surgery Unit, Department of Dentistry, at a Government Medical Institute with the chief complaint of reduced mouth opening for the past 6 months. The patient gave a history of assault in which he was hit by a rod on the left side of his face 6 months ago. At that time, he reported to some nearby hospital where he was managed by antibiotics and analgesics only to relieve his facial pain and swelling. His swelling and pain subsided after a few days, but later on, he felt a gradual restriction in mouth opening, which reduced up to one finger width within a few months, and then he reported to us. On clinical examination, it was found that his mouth opening was limited to 10 mm only, measuring in the maxillary to mandibular central incisor region (Figure 1). There was also a minor malar flattening noticed on the left side of the face (Figure 1). Based on clinical examination, a provisional diagnosis of an old zygomatic arch fracture was made. To confirm the diagnosis, non-contrast computed tomography (NCCT) face was done, which revealed a medially displaced, malunited left zygoma fracture leading to coronoid impingement (Figure 2). In order to achieve optimal mouth opening, an intraoral left coronoidectomy was planned under general anesthesia. Nasotracheal intubation was done, and the incision was carried out in the left posterior buccal vestibule, along the external oblique ridge, and extended toward the anterior border of the ramus. A full thickness periosteal flap was elevated, and the insertion of the temporalis attachment was identified, and after that, the ramus retractor was placed along the ascending ramus to expose the coronoid process. Left coronoidectomy was performed using a surgical bur under copious saline irrigation. After coronoidectomy, immediate postoperative active 40 mm mouth opening was achieved (Figure 3). One week postoperatively, active mouth opening exercise was initiated with Heister’s mouth gag, and the patient was asked to continue mouth opening exercises for 3 months. The patient was kept on regular follow-up at an interval of 1 month, and after 6 months, at follow-up, the patient was doing fine, and his passive mouth opening was satisfactory (Figure 4).
10 mm Mouth Opening Due to Malunited Left Zygomatic Arch Fracture.

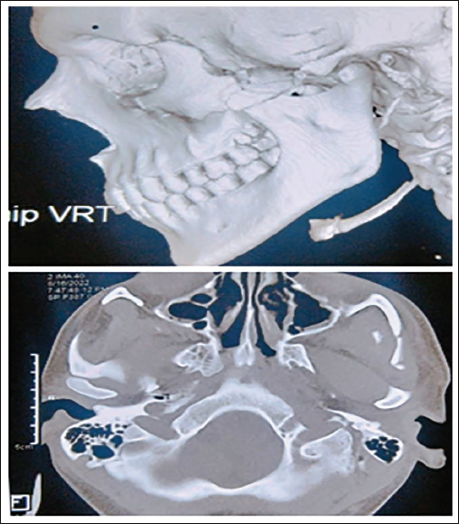
Non-contrast Computed Tomography (NCCT) Face Showing Medially Displaced Malunited Left Zygomatic Arch Fracture Leading to Coronoid Process Impingement.
Photographs Showing Left Coronoidectomy and 40 mm of Immediate Intraoperative Mouth Opening.

Follow-up Photographs Showing Satisfactory Mouth Opening.

Discussion
The zygomatic bone is also called the cheekbone, which is articulated by four suture lines to the frontal, temporal, maxillary, and sphenoid bones, and plays an important role in creating facial width and projection. The zygomatic complex fracture is a tetrapod fracture in which the separation of all four sutures takes place. 1 Management of zygomatic arch fracture depends on its degree of displacement, and the main goal of treatment of zygoma fracture is to restore malar contour, orbital volume, and normal mandibular range of motion. Treatment of zygomatic arch fracture ranges from conservative management, closed reduction, and open reduction internal fixation, based on the level of comminution and degree of displacement of the fracture segment.
Undisplaced or minimally displaced zygomatic arch fractures are easily managed by non-operative interventions in which patients are kept on liquid diet, analgesia, and close follow-up care. But in case of displaced or comminuted zygomatic arch fracture, some kind of surgical intervention is necessary within 2 weeks in order to achieve the goals of zygomatic arch fracture management. In displaced zygomatic arch fracture, usually two- or three-point fixation is sufficient depending on the degree of displacement. Untreated displaced zygomatic arch fracture can lead to malunion of the displaced fracture segment, which in turn leads to cosmetic deformity and limited mouth opening due to the depressed zygoma impinging on the mandibular coronoid process.5, 6 It has been seen that after immediate trauma, due to the edema of the surrounding area, zygoma fractures are easy to go unnoticed if the clinical examination is not carried out in a proper way. So, in the presence of periorbital edema and ecchymosis, subconjunctival hemorrhage, infraorbital nerve paresthesia, and restricted mouth opening, zygomatic arch fracture should be suspected, and proper workup should be done so that such injuries cannot be missed. Radiographic evaluation must be done to confirm the zygomatic arch fracture.
Isolated zygomatic arch can be managed by either Keen’s intraoral approach 7 or Gille’s temporal approach, 8 in which the displaced zygomatic arch is reduced but fixation is not carried out. If there is a displaced comminuted zygomatic arch fracture, then hemicoronal incision should be planned to reduce and fix the arch to achieve facial projection and to avoid mechanical coronoid process impingement, which could lead to trismus. In case of a malunited zygomatic arch fracture, if the patient’s chief complaint is facial asymmetry and restricted mouth opening, then the treatment would be zygomatic osteotomy along with fixation of the displaced malunited segment, but if there is only a complaint of restricted mouth opening without significant facial asymmetry, then intraoral coronoidectomy is the treatment of choice.
In the present case, the chief complaint of the patient was restricted mouth opening, which gradually developed after the history of assault 6 months back. At that time, he was having a left zygomatic arch fracture, which was missed in the initial clinical examination in the hospital where he had reported at the time of assault. Had he been diagnosed with his zygomatic arch fracture at that time, he would not have this issue. At that time, he was managed with analgesics only and was not kept under any follow-up visits. Gradually his fracture zygomatic arch got malunited and he was having severe restricted mouth opening due to the impingement of the coronoid process over the depressed zygoma. In the present case, the cosmetic deformity was very minimal, and the patient’s concern was only restricted mouth opening, and he did not want any facial scar, so intraoral coronoidectomy was planned. Coronoidectomy is a simple surgical procedure, which has been the treatment of choice in restricted mouth opening cases. 9 In this patient, as a result of coronoidectomy, the impingement of the coronoid process was removed, due to which we achieved immediate optimum mouth opening of around 40 mm.
In conclusion, in case of restricted mouth opening due to the impingement of the coronoid process at a malunited zygomatic arch fracture, coronoidectomy is the treatment of choice.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent were obtained before initiating the study from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.