
Abstract
Objective
Complicated crown fractures of anterior permanent teeth, typically caused by traumatic injuries, are commonly encountered and require focused treatment. Prioritizing the preservation of pulp vitality is crucial, with an emphasis on maintaining it rather than resorting to a pulpectomy after pulp exposure.
Case Report
Two patients presented to the department due to trauma, and examination revealed a complicated crown fracture in tooth #21 and tooth #11. A partial pulpotomy and pulp capping were conducted using two different bioceramic materials as the medicament, and 2.5% sodium hypochlorite was utilized for hemostasis. The tooth was subsequently restored with the separated tooth fragment using adhesive bonding, and follow-up appointments were scheduled at 3, 6, and 18 months.
Conclusion
Vital pulp therapy serves as a viable substitute for root canal treatment in traumatized anterior teeth with pulp exposure. Bioinert (bioceramic material) proves to be a suitable choice for pulpotomy, fostering the formation of a dentin bridge, thereby maintaining the vitality of the remaining pulp portions.
Clinical Significance
Preserving the vitality of teeth is of paramount importance, as the vital pulp not only nourishes dentin but also generates reparative dentin in response to stimuli. The use of biocompatible materials offers numerous advantages, including enhanced esthetics, preservation of vitality, regenerative potential, and easy handling—all notable features of these innovative bioinert materials.
Introduction
In young permanent teeth, the approach to treating crown fractures with pulp exposure is contingent upon factors such as the extent of pulp tissue involvement, the stage of root development, and notably, the time elapsed between the traumatic incident and examination. Preservation of the pulp is advocated for teeth with immature roots to facilitate root formation and overall tooth maturation, and for mature teeth for nourishment and defense. When the pulpal exposure is less than 1 mm 2 , pulp capping is recommended, with the stipulation that the duration of exposure at the time of treatment should not exceed a few hours. In cases where pulpal exposure exceeds 1 mm 2 and there is a significant time lapse between the incident and examination, Cvek pulpotomy, a partial pulpotomy technique, is considered the treatment of choice.
Among the different treatment options available for coronal tooth fractures involving esthetics, such as laminated veneers or full crowns, as well as composite restorations, reattachment of fractured tooth fragments aims to replicate the natural esthetics and functionality of teeth, eliciting a positive psychological response from the patient. In 1964, Chosak and Eidelman pioneered the publication of this groundbreaking technique.
There is a lack of case reports demonstrating pulpotomy as an effective treatment for fragment attachment. Moreover, the use of bioceramic materials as a pulp sealing agent has become a crucial factor in enhancing success rates. This approach not only helps preserve pulp vitality but also significantly contributes to restoring esthetic outcomes.
Case 1
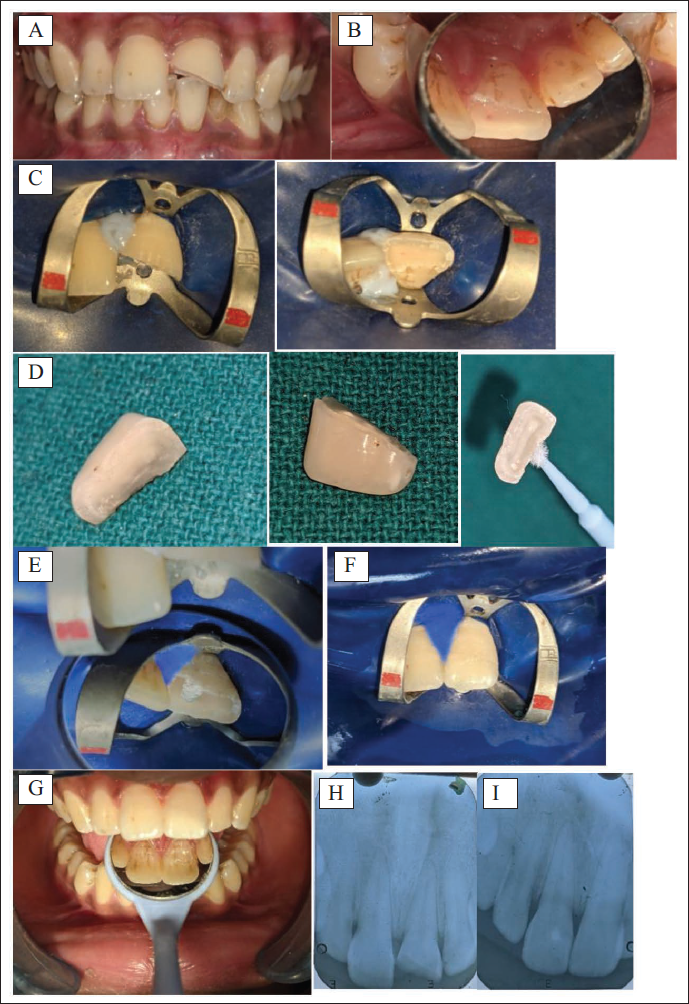
A 24-year-old male patient presented with the chief complaint of a broken upper front tooth within 30 min of trauma. Clinical examination revealed a fracture involving the middle third of #21 with a single separated fragment and pinpoint pulpal exposure on the mesial aspect. Bleeding was noted with a change in gingival contour (Figures 1A and 1B). Intraoral periapical radiograph (IOPA) revealed a fracture involving the mesial pulp horn. Radiographic and clinical findings showed pulpal involvement. According to the new traumatic classification, the diagnosis was a complicated crown fracture NAOD.03. A treatment plan using Biodentine as a pulp capping agent followed by fragment attachment was designed.
(A) Pre-op Clinical Photograph; (B) Palatal View; (C) Rubber Dam Isolation with Pulp Exposure; (D) Separated Fragment; (E) Biodentine Placed; (F) Fragment Attached; (G) Post-op Clinical Photograph; (H) Pre-op Radiograph; (I) Post-op Immediate.
Case 2
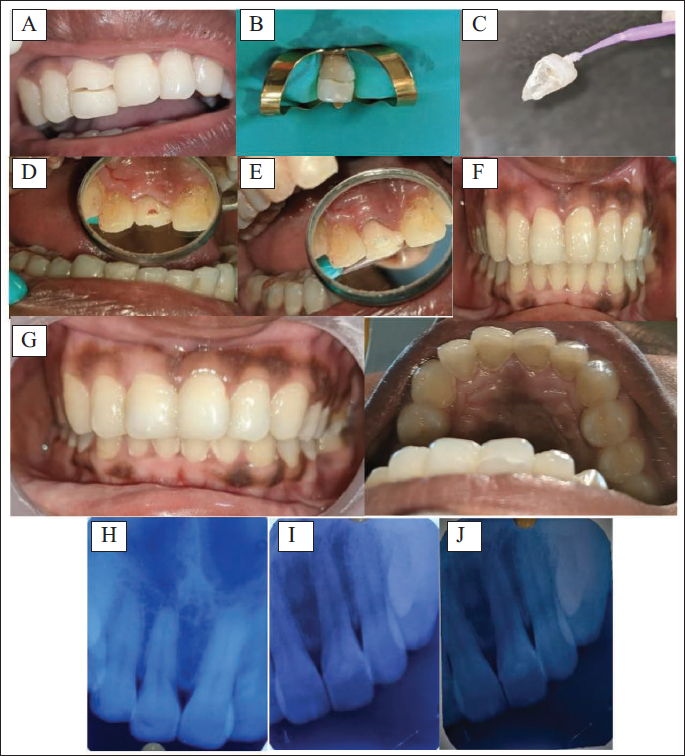
A 24-year-old male patient presented with the chief complaint of a broken upper front tooth within 1 day of trauma. Clinical examination revealed a fracture in the middle third of #11 on the labial aspect and the cervical third on the palatal aspect of the coronal tooth structure. The fractured segment remained attached to the tooth (Figures 2A and 2B). Gingival bleeding with inflammation was noted with a change in contour on the palatal aspect (Figure 2D). IOPA revealed a fracture involving the roof of the pulp chamber. Radiographic and clinical findings showed pulpal involvement. According to the new traumatic classification, the diagnosis of a complicated crown fracture NAOD.04 was made. The treatment plan included Cvek’s pulpotomy sealed with bioceramic material (iRoot BP Plus), beveling the labial side of the tooth, followed by fragment attachment.
Case Management
The patient received an explanation of the pulpotomy procedure, and informed consent was obtained. Subsequently, the relevant tooth was anesthetized through local infiltration of 0.6 mL lignocaine (1:200,000 adrenaline). Chlorhexidine was used to disinfect the teeth. Under rubber dam isolation, the sharp fractured margins were smoothed, and both the exposed pulp and the surrounding dentin were thoroughly rinsed with an isotonic saline solution. Subsequently, freshly mixed Biodentine™ (Saint-Maur-des-Fossés, France) was promptly applied over the exposed pulp, and the setting process was allowed to proceed for 20 min (Figures 1C to 1E). The exposed dentin and Biodentine were bonded with the separated fragment using composite (Esthet X-Dentsply Caulk, Milford, DE) during the same appointment (Figures 1F and 1G).
In the second case, the subgingivally attached fragment was removed with minimal trauma and placed in Han’s balanced salt solution. A high-speed small round diamond bur #2 was employed with a gentle touch and water coolant to excise the superficial layer of the exposed pulp and surrounding tissue to a depth of 2 mm. The presence of associated bleeding from the radicular pulp indicated a healthy status of the pulp. The exposed pulp surface was irrigated with isotonic saline, and small sterile cotton pellets were gently applied for 5 min to control the bleeding. Following this, iRoot BP Plus was placed into the exposed area and restored with light-curing GIC (Fusion Pro) and composite (Esthet X-Dentsply Caulk, Milford, DE) (Figures 2E to 2H).
Follow-up
Periodic follow-ups were conducted at intervals of 24 h, 3 months, as well as at 6, 12, and 18 months, and the following parameters were assessed:
The teeth subjected to pulpotomy remained asymptomatic and showed no tenderness to percussion. At the 18-month follow-up, electric pulp testing revealed a vital response in the teeth treated with bioceramic pulpotomy and Biodentine pulp capping.
Radiographic assessment demonstrated the absence of periapical lesions and periodontal ligament (PDL) widening. In Case 1, a distinct radiopaque layer was observed on the pulpal aspect adjacent to the layer of Biodentine, indicating the formation of a calcific barrier (Figures 1H and 1I).
While distinct barrier formation was not evident in Case 2, there was an observed increase in radio-opacity in the radicular pulp adjacent to the layer of bioceramic material (iRoot BP Plus) (Figures 2I and 2J).
(A) Pre-op Clinical Photograph; (B) Rubber Dam Isolation; (C) Separated Fragment; (D) Palatal View with Pulp Exposure; (E) iRoot BP Plus Placed; (F) Fragment Attached; (G) Post-op Clinical Photograph; (H) Pre-op Radiograph, (I) Post-op Immediate; (J) Follow-up After 18 Months.
Discussion
Achieving a positive outcome necessitates comprehensive diagnosis, effective treatment planning, and diligent follow-up. Tooth trauma initiates pulpal hyperemia, leading to alterations in blood flow and may eventually lead to necrosis if left untreated. The observation suggested that, in the short term, pulpotomy presents a viable alternative to root canal treatment for teeth with vital pulps. 1 Nevertheless, there is insufficient clinical evidence to advocate for the application of this technique in the treatment of a permanent tooth.
Abarajithan et al. 2 observed a favorable outcome in two cases of traumatic pulp exposures treated with pulpotomy using MTA, noting a normal response to electric pulp tests and a custom-made pulse oximeter, along with the absence of periapical pathology after a 2-year follow-up. However, the prolonged setting time, challenging handling characteristics, and high cost associated with MTA have prompted the exploration of a more suitable alternative material. In their study, Han and Okiji conducted a comparison between Biodentine and white ProRoot MTA regarding the uptake of Ca and Si by adjacent root canal dentin. They observed that, while both materials formed tag-like structures, Biodentine exhibited a more pronounced uptake of dentin elements compared to MTA. 3 Laurent et al. conducted a separate study, which revealed a significant enhancement in the secretion of transforming growth factor-beta 1 (TGF-β1) from pulp cells when treated with Biodentine. 4
In the treatment of a symptomatic immature second right mandibular premolar, Villat et al. conducted a partial pulpotomy using Biodentine. Their study demonstrated a rapid tissue response at both the pulpal and root dentin levels, resulting in the formation of a radio-opaque bridge within 3-6 months. 5 Hence, it is recommended to consider tricalcium silicate cement, such as Biodentine, as a conservative intervention in the management of symptomatic immature teeth and for mature vital teeth with minimal pulp exposure.
Second, the problem with the material is tooth discoloration. In a study by Awawdeh et al., 6 the MTA group exhibited signs of discoloration, while the Biodentine group remained unaffected. Additionally, in an in vitro study, Raskin et al. found that Biodentine demonstrated favorable performance as a dentin substitute without requiring any conditioning treatment. 7 Consequently, it is not advisable to etch Biodentine, as it can be directly bonded to resin composite materials.
Hashem et al. 8 examined the use of both self-etch and total-etch systems for bonding Biodentine to resin composites and found no significant difference between the two methods. As a result, they recommended using either self-etch or total-etch adhesives for this purpose. Consequently, the first case was treated with Biodentine (a dentin substitute), where the pulp exposure was minimal, involving only the mesial pulp horn, and a direct bonding technique was applied.
Bioceramic material was chosen due to the delayed reporting of the patient, and the fracture segment involved till the cervical third palatally, mainly due to its antibacterial activity. Recent evidence suggests that pulpotomy of immature permanent molars exhibiting irreversible pulpitis symptoms demonstrated promising outcomes with both MTA and bioceramic putty, establishing them as viable and acceptable conservative options. BC Putty shows a good response to partial pulpotomy in clinical cases, and it may be an effective sealing material for the pulpotomy of young permanent teeth after trauma.9, 10
Another new bioceramic material, iRoot BP Plus, has been chosen as it is reported to have good biocompatibility, sealing ability, and antibacterial activity. Recent investigation in immature permanent teeth with complicated fractures suggested iRoot BP Plus may be an effective capping material for partial pulpotomy. Another retrospective study showed that iRoot BP Plus is a suitable alternative to CH for use in the management of permanent incisors with complicated crown fractures treated by pulpotomy. Pulpotomy with iRoot BP Plus can be completed in a single visit and maintains pulp vitality without tooth discoloration.11, 12
iRoot BP Plus demonstrates remarkable biological characteristics and effective sealing capabilities while also promoting the generation of a substantial dentin bridge layer. In this case report, partial pulpotomy followed by placing the material resulted in the formation of a calcific barrier after 3 months in the second case, revealing its osteogenic potential. In vitro and in vivo investigations have also consistently validated the bioactive nature of this substance. It stimulated the proliferation of human dental pulp cells and facilitated the formation of hard tissue at locations where the pulp was exposed. These attributes potentially make iRoot BP Plus a superior material for pulpotomy treatment.11, 12
Conclusion
This case report inferred that vital pulp therapy (pulp capping and pulpotomy) serves as a viable substitute for root canal treatment in traumatized anterior teeth with pulp exposure, even when performed several days after the initial pulp exposure. Bioceramic material for pulpotomy facilitates dentin bridge formation and safeguards the vitality of the remaining pulp portions. Additional research and clinical trials are essential to formulate treatment protocols that can optimize clinical success.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Not applicable.