
Abstract
Objective
To report a case of a palatal fistula caused by trauma from a removable maxillary denture with a suction cup, and to evaluate the effectiveness of Bardach’s two-layer palatal flap technique for its surgical repair.
Methods
Palatal fistulas are pathological communications between the oral and nasal cavities, often leading to nasal regurgitation, hypernasal speech, and psychological discomfort. They may result from congenital anomalies like cleft palate, infections such as osteomyelitis, or mechanical trauma, including long-term use of maxillary dentures with suction cups. Surgical repair is often challenging due to limited tissue availability and scar tissue from previous procedures, contributing to a recurrence rate of up to 25%. A case of a patient with a suction cup-induced palatal perforation was managed using Bardach’s two-layer palatal flap technique. This method involves creating bilateral mucoperiosteal flaps from the hard palate and repositioning them to achieve a tension-free, two-layer closure.
Results
The surgical repair using Bardach’s technique was successful, with the patient experiencing no major postoperative complications. The flap provided adequate coverage with good vascularity and healing, and no recurrence of the fistula was observed during follow-up.
Conclusion
Bardach’s two-layer palatal flap is a reliable and straightforward surgical approach for repairing small palatal fistulas, especially those caused by trauma. Its advantages include simplicity, a robust blood supply, and minimal donor site morbidity. This case supports the technique’s continued use in similar clinical scenarios to achieve effective and lasting closure of palatal defects.
Introduction
A palatal fistula is a disruption in the structural integrity of the palate, resulting in oronasal communication. This condition can be caused by genetic factors like cleft lip and palate, neoplasms, infections such as osteomyelitis, or any penetrating trauma. It can also be caused due to wearing a maxillary complete denture with a suction cup for a prolonged period of time. The continuous pressure from the suction cup on the palatal mucosa can lead to necrosis of both the mucosa and underlying bone, ultimately creating a communication between the oral and nasal cavities. 1
This fistula creates an abnormal communication between the oral and nasal cavities, which may lead to regurgitation of food and fluids through the nose, with subsequent chances of nasal infection and nasal discharge. It can also result in nasal phonation, causing air to escape through the nose during speech. Although a palatal fistula is not a visible defect for confronting people, it can still have emotional and psychological impacts, especially during speaking or eating. 2 Cohen et al. categorized fistulas based upon the size into small (1-2 mm), medium (3-5 mm), and large (>5 mm). 3
Surgical management of an oronasal fistula is a technically complex and cumbersome procedure due to the availability of insufficient tissue for closure and the presence of scar tissue from any previous surgery, which makes the procedure more challenging for the surgeons. In the literature, the recurrence rate of oronasal fistula is approximately 25%-34.2%.4, 5 The key surgical principle is to achieve a two-layer, tension-free closure. To meet this goal, various techniques have been developed, ranging from local flaps to free tissue transfer. 6 Local advancement flaps include palatal flaps, nasolabial flaps, tongue flaps, and buccal fat pads, whereas distant pedicle flaps include buccinator myomucosal flaps, forehead flaps, and temporoparietal fascial flaps. 1
We present a case of suction cup-induced palatal perforation/fistula, which was surgically managed using Bardach’s two-flap technique.
Case Report
A 62-year-old male patient reported to the Department of Oral and Maxillofacial Surgery with a chief complaint of a hole in the palate region, along with the escape of fluids through his right nostril and nasal phonation for 3 months. The patient gave a history of wearing a maxillary denture with a suction cup throughout the day and night, and removed it for cleaning once daily for the past 5 years. The patient initially noticed an erythematous patch on the palate, which later converted into an oronasal fistula within a period of 3 months.
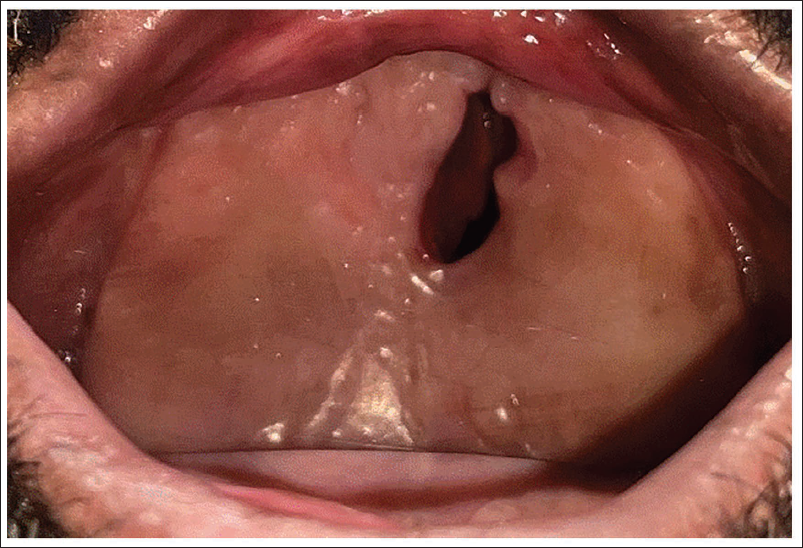
On intraoral examination, a palatal perforation measuring approximately 3 × 2 cm was present in the anterior palatal rugae region with inverted margins (Figure 1). All the surrounding tissues appeared normal in color and texture. On palpation, the margins were non-tender with no signs of any pus or fluid discharge.
Oronasal Fistula at Anterior Hard Palate Region.
The patient’s medical history was uneventful, and blood investigations were within normal limits.
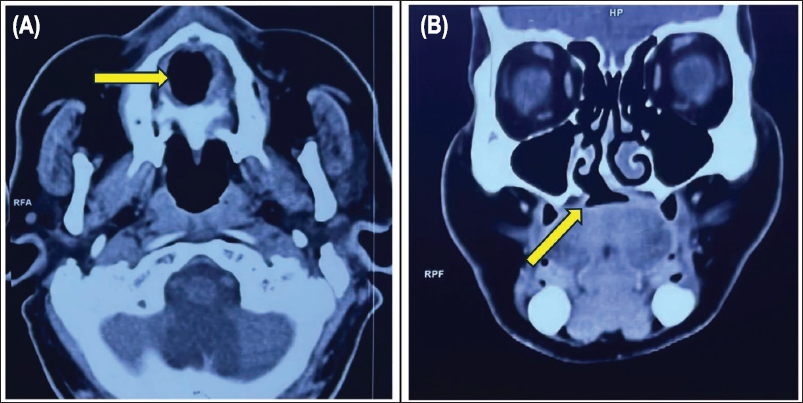
Contrast-enhanced computed tomography (CECT) face and neck showed a right paramidline defect at the anterior aspect of the hard palate with a fistulous communication between the oral and right nasal cavity (Figure 2).
(A) Axial and (B) Coronal Contrast-Enhanced Computed Tomography (CECT) Images of the Face and Neck Demonstrate a Right Paramidline Defect in the Anterior Aspect of the Hard Palate with a Fistulous Communication Between the Oral Cavity and the Right Nasal Cavity.
The surgery was planned for a two-layer closure of oronasal fistula using Bardach’s two-flap technique under general anesthesia.
Surgical Procedure
The patient was laid on the operation theater (OT) table in a supine position with an extended neck. Nasotracheal intubation was done under general anesthesia. Local infiltration was done using 2% lignocaine and 1:80,000 adrenaline to achieve adequate hemostasis.
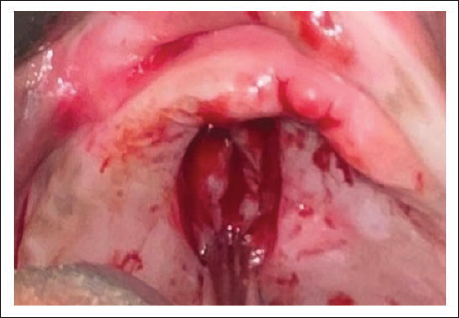
An incision was made with a no. 15 blade along the fistula edges, leaving a margin of approximately 2-3 mm. The oral mucosal flap was elevated towards the margin, turned down into the defect, and approximated in the midline for nasal layer closure using resorbable sutures (Figure 3).
Elevation of Flap for Closure of Nasal Layer.
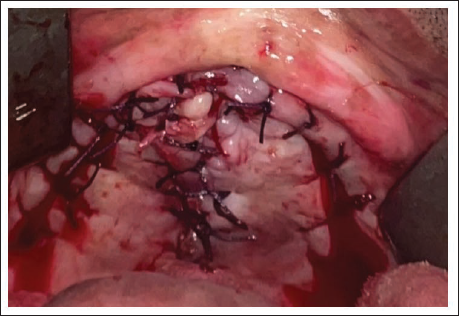
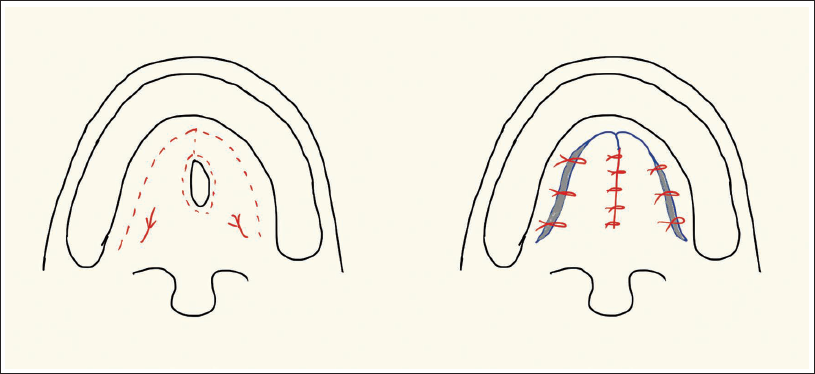
Then, a straight incision was given from the anterior edge of the fistula to the alveolar margin anteriorly, and this incision was extended bilaterally 5 mm palatally to the alveolar margin in a distant direction till the posterior border of the hard palate. Another incision was extended from the posterior end of the fistula to the posterior margins of the hard palate. A full-thickness mucoperiosteal flap was elevated up to the posterior border of the hard palate and was assessed for tension-free mobilization towards the midline. This flap was based upon the greater palatine vessels. Tension-free closure of the oral layer was done with mattress sutures using 3-0 Vicryl. A few stay sutures were placed along the lateral releasing incision (Figure 4). A schematic illustration of the incision and flap design is provided in (Figure 5). After completion of the procedure, reversal was given and the patient was extubated.
Closure of Mucosal Layer.
Incision and Flap Design.
Nasogastric tube (Ryle’s tube) was secured for postoperative feeding, and the patient was kept under antibiotic, anti-inflammatory, and analgesic coverage postoperatively for the next 7 days.
The patient was advised to follow postoperative nasal precautions, that is, to avoid vigorous sneezing and blowing of nose). The patient was reviewed on postoperative days 3rd, 7th, and 14th, as well as at the 1st and 2nd month intervals, and continues to be followed up. No postoperative complications were recorded in the subsequent follow-ups, with complete coverage of the defect (Figure 6).
Second Postoperative Month Follow-up.

Discussion
Complete dentures can cause changes in both soft and hard tissues. Alveolar bone resorption can cause the denture to rock around the mid-palatal area, leading to excessive pressure despite good retention from a rubber disc. 7 This negative pressure can result in palatal bone loss, as seen in this case, potentially leading to a perforation if the prosthesis is not properly fabricated. Oronasal fistula leads to nasal regurgitation of food/fluids and hypernasal speech, which has an emotional and psychological impact on the patient. 8
Many clinical practitioners are still using suction cups in the maxillary denture as an additional retentive aid, even after knowing about its ill effects. So, practitioners should be well aware of the consequences of using a suction cup in a maxillary denture and should provide appropriate treatment to stop the progression of the existing pathology and provide an environment for the healing to take place. 9
Management of palatal perforation caused by a suction cup begins with educating the patient on the harmful effects of the prolonged use of maxillary dentures with a suction cup. Closure of palatal fistulas is difficult due to the rigidity of the palatal mucosa and is further complicated by the limited availability of tissue for tension-free closure. 10 There is no single procedure that is universally effective for all types of palatal fistulas. The choice of technique depends on factors such as the defect’s size, location, and the patient’s age. 11 Flap techniques are often more successful, as they reduce tension and provide better support for the repair. 12
An oronasal fistula is an epithelialized, pathological communication between the oral and nasal cavities. It can be categorized by size into small (1-2 mm), medium (3-5 mm), and large (greater than 5 mm). 3 The management of oronasal fistulas is determined by the site and size of the defect, with surgical intervention being the definitive approach. Numerous surgical techniques have been described in the literature, utilizing both local and regional flaps such as the palatal flap, buccal fat pad, buccinator myomucosal flap, tongue flap, and nasolabial flap. In addition, distant flaps like myofascial and forehead flaps may also be employed. Among these options, the tongue flap is effective, but it can cause functional problems such as impaired swallowing and speech due to temporary tongue immobility. 11 Also, buccal and tongue flaps involve two-stage surgical procedures, which are often associated with donor site morbidity.
Palatal flaps are advantageous for closing small palatal defects due to the hard palate’s thick mucoperiosteum and its reliable vascular supply from the greater palatine artery, which offers good vascularity, making them a favorable option. 9 But, it frequently results in a bulky tissue mass due to overlapping flaps. Also, these techniques generally rely on a single-layer closure, which is less reliable. Challenges associated with these methods include limited tissue availability, reduced vascularity, repair fragility, and a higher likelihood of failure. 13
These techniques offer benefits in specific cases, but many are cumbersome and associated with postoperative complications such as tissue loss, scar contracture, poor aesthetics, and a high recurrence rate, reaching up to 34.2%. 14 The buccal fat pad flap may provide bulk, but it is often insufficient when mobilized to the palate. Nasolabial flaps involve extraoral incisions and tunneling, resulting in visible scars. Distant flaps require complex techniques and have associated donor site morbidities, such as scarring.
In this study, palatal fistula was repaired using Bardach’s two-layered mucoperiosteal flap technique, which offers a two-layer, tension-free closure of the fistula, making it a reliable and well-established option.
It provides tissue that closely matches the defect site, eliminates the need for a second donor site, and has demonstrated consistent success. However, a drawback of this technique is the exposed bone lateral to the flap, which may lead to pain and discomfort. 13
The first layer was formed by bilateral hinge flaps from the mucoperiosteum surrounding the fistula, while the second layer was based on the greater palatine artery and was advanced for optimal closure. After the palatal cleft was fully closed, attention was given to any exposed bone areas lateral to the flaps. In most cases, gaps could be closed or approximated to promote healing. If full closure is not possible due to tension, loose sutures can be used to reduce the exposed bone area and encourage healing. 14
Anani and Aly 15 applied a similar approach and were successful in closing oronasal fistulas in eight patients, achieving a 100% success rate. Sadhu 4 recommended a two-layer closure technique involving a rotational mucoperiosteal flap from the opposite side of the palate to seal the oral surface, along with a turnover mucoperiosteal flap for the nasal layer.
In this case, Bardach’s flap was chosen based on the defect’s location and the flap’s ability to rotate without compromising its blood supply. The circular incision around the fistula was crucial for securing the flap, ensuring strong bony support, and preventing wound dehiscence. This technique offers several advantages as it is a straightforward, single-stage procedure with no need for any extra-oral incisions, free vascular flaps, or complex donor site management. The mucoperiosteum, being tough and resilient, is well-suited for lining the hard palate without affecting mouth opening, unlike other local or free flaps.16, 17
Conclusion
Successful repair of a palatal fistula requires a well-supported, airtight, and tension-free closure. The success of the procedure largely depends on the surgeon’s ability to achieve a tension-free closure. For small palatal perforations, Bardach’s two-flap technique, which utilizes bilateral mucosal tissues for effective defect closure, is a viable option. This technique offers benefits such as technical simplicity, good vascular supply, and minimal donor site morbidity.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Necessary ethical clearances were received and obtained respectively before initiating the study from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Written informed consent was obtained from the patient.