
Abstract
Background
As much as “contempt for what is old” philosophy is detrimental, it may be a necessity to use old surgical techniques occasionally.
Purpose
To evaluate differences in surgical outcomes of wisdom tooth removal surgery between the lingual split chisel mallet technique (Group I) and the bur technique (Group II).
Study Design, Setting, and Sample
A randomized controlled non-inferiority trial was conducted at a tertiary care hospital in India, in an outpatient clinic. Patients aged 18-50 with impacted mandibular third molars (Pell and Gregory position A and B) without associated pathology were included (n = 40). Smokers, pregnant women, and those unable to follow-up were excluded.
Predictor Variables
Treatment assigned (Groups I and II).
Covariates
Age, gender, chief complaint, duration of complaint, side, Winter’s class, Pell and Gregory class and position, Pederson difficulty index, pre-existing temporomandibular dysfunction, and trismus.
Outcome Variables
Primary: Postoperative day 1 pain score. Secondary: Postoperative pain on days 3 and 7, trismus (mouth opening <30 mm), dry socket, paresthesia, infection, and dehiscence.
Analyzes
Categorical variables were analyzed by chi-square or Fisher’s exact test, and continuous variables by t-test and Wilcoxon rank sum test. The level of statistical significance was set at P value <.05, and the non-inferiority limit at δ of ±1 for the visual analogue scale (VAS) on day 1.
Results
Forty patients were eligible and included, 20 in each group. No statistical differences were found in demographics and preoperative variables. Mean pain-scores on day 1, 3, and 7 in Group I were 4.15 (±1.7), 2.5 (±1.9), and 1.05 (±1.2), respectively. The same in Group II were 4.3 (±1.9), 2.6 (±1.1), and 1.65 (±1.0). For the primary outcome variable, the P value was .94 [95% CI, (−0.82) −1.12]. Trismus by day 7 in Group I was 15% (n = 3) and in Group II was 45% (n = 9). Temporary sensory disturbance was noted in one patient in each group. There was no incidence of dry socket or infection.
Conclusion
Lingual split technique in third molar surgery gives comparable postoperative outcomes in terms of postoperative pain, trismus, infection, and paresthesia to the bur technique; however, the latter remains the gold standard.
Keywords
Introduction
Impaction of a tooth is a situation where a tooth fails to attain its normal functional position. Extraction of impacted molars remains one of the most commonly performed procedures in oral and maxillofacial surgery.
Archer 1 defined an impacted tooth as a tooth that is partially or completely unerupted and is positioned against another tooth, bone, or soft tissue so that its further eruption is unlikely. In comparison to other teeth in the dental arch, mandibular third molars are less likely to erupt and participate in food mastication, and are prone to getting affected by disease. The average worldwide rate of impaction is 24%. 2
The UK’s National Health Service (NHS), in the year 2000, introduced a protocol for the removal of third molars based on recommendations given by the National Institute for Clinical Evidence (NICE). 3 They recommended discontinue prophylactic removal of pathology-free impacted third molars and limit the removal to impacted third molars with evidence of pathology. Specific attention was drawn to plaque formation and pericoronitis, of which the first episode of pericoronitis, unless particularly severe, should not be considered an indication for surgery, whereas a second or subsequent episode should be considered an appropriate indication for surgery.
There are several techniques of bone removal during third molar surgery, such as the bur technique, piezoelectric technique, and chisel mallet technique, and each has its pros and cons. In 2019-2022, the world saw the COVID-19 pandemic, with lockdowns and hospitals running only emergency services apart from COVID care. Toothache, being one of the most severe painful ailments, required its removal without the use of rotary or piezoelectric armamentarium, as they caused more aerosol production and increased the risk of viral spread. The US Centres for Disease Control and Prevention 4 (CDC) has classified dental care-related aerosols or droplets as high risk. The usage of techniques that create less aerosol production (chisel and mallet) was thought to have the potential to be brought back into practice, if giving comparable surgical outcomes with the latest techniques for bone removal. Some of the scientific literature seems to support its use in terms of comparable complication rates, too.5, 6
Upon literature search, there are not many randomized controlled trials (RCTs) in the last 10 years that compare the intraoperative complications and postoperative outcomes in the extraction of mandibular third molars, using the lingual split technique with a chisel and mallet and using the rotary cutting instruments. We hypothesize that the lingual split chisel mallet technique is not inferior to the bur technique with regard to postoperative pain in mandibular third molar surgery.
Materials and Methods
To address the research purpose, we conducted a randomized controlled non-inferiority trial. The Institute Ethical Committee approved the present study (approval no. IECPG-577/28.10.2021, RT-29/25.11.2021), and the study was done in accordance with the Helsinki Declaration. Forty patients were enrolled with impacted mandibular third molars and were divided into two groups: Group I lingual split chisel malate technique (n = 20), and Group II bur technique (n = 20). The non-inferiority margin was taken as 1 (δ = 1), an α error of 0.05, a power of the study of 80%, and a confidence level of 95% were considered.
We included patients aged 18-50 with unilateral/bilateral impacted mandibular third molars planned for extraction and excluded them as study subjects if they had any systemic disease/condition that impaired healing, if they were physically/mentally challenged individuals, smokers, or pregnant women. Teeth involved in cyst/tumor, Pell and Gregory position C impactions, and patients who were unable to attend follow-up appointments were also excluded. Patients were followed up for 7 days. All included patients provided written informed consent.
Randomization was done by a computer-generated random table using software IBM Statistical Package for the Social Sciences (SPSS) (IBM Corp. Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.) and was then divided into two groups. Impacted molar removal with chisel mallet lingual bone split technique (Group I) and impacted molar removal with bur technique (Group II). Chits with labeling in accordance with the randomization list were placed in envelopes numbered in numerical order. After inclusion in the study, the envelopes were opened, and the patient was enrolled in one of the two groups. No blinding was done during the study.
Preoperatively, an orthopantomogram (OPG) was used. Baseline variables included age in years, gender, Winter 7 classification, Pell and Gregory 8 classification, Pedersen 9 difficulty index, mouth opening in mm, and proximity to the inferior alveolar nerve (IAN) on preoperative radiographs (noted as yes/no), which were recorded prior to the procedure.
The primary objective of this study was to compare differences in pain scores as per the visual analogue scale (VAS) (0 being no pain and 10 being the worst imaginable pain). This was assessed subjectively by direct questioning of the patient on postoperative day 1, day 3, and day 7. Secondary objectives were to compare the duration of surgery (in minutes) from exposure to removal of the mandibular third molar, intraoperative and postoperative complications like excessive bleeding requiring measures other than usual surgical steps, tooth/root piece slippage into the lingual pouch, mandibular fracture, trismus (mouth opening measured between upper and lower central incisal edges being <30 mm), dry socket, infection defined as purulent discharge from the surgical site with or without systemic complaints like fever or lymphadenopathy, and nerve paresthesia as assessed subjectively by direct questioning of the patient concerning any tingling or numbness of the tongue or lip, and also as confirmed objectively by the presence or absence of sensory alteration in response to cotton fibrils by the two-point discrimination test. Dehiscence and need for rescue pain medication were evaluated on postoperative days 1, 3, and 7 between the lingual split/chisel mallet technique and bur technique groups.
Surgical Procedure
Lingual Bone Split Technique 10
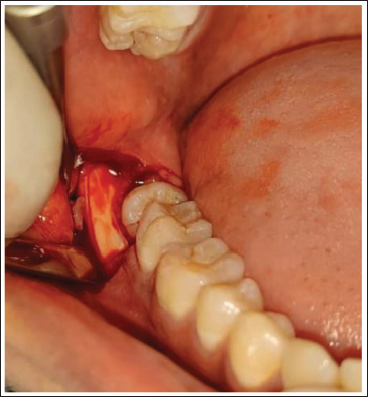
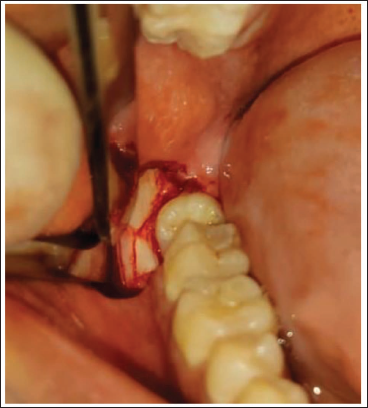
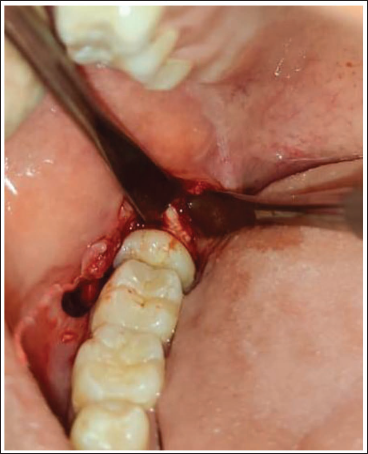
Painting and draping of the surgical area with 5% povidone iodine solution were done. Inferior alveolar, lingual, and long buccal nerve block on the side of third molar removal was given using 4-5 mL of 2% lignocaine hydrochloride with adrenaline 1:200,000 concentration. After 5 min, the incision was started using a number 15 blade. Ward 11 incision was placed by starting an anterior releasing incision, which was made from the distobuccal corner of the crown of the second molar and ended alongside the mesiobuccal cusp of that tooth. Incision is made through the mucoperiosteum and down to the bone with firm pressure. The incision is then extended distally in level with the buccal side of the tooth (in crevicular fashion if it is partially erupted) to the external oblique ridge. The posterior part of the incision is made to slope outwards as well as backwards towards the ascending ramus. Subperiosteal flaps were then reflected buccally and lingually, and the crown of the impacted third molar and the bone of the retromolar trigone region were exposed. The blunt end of the periosteal elevator was used to raise the lingual flap and was kept in situ to protect the lingual nerve. A 5 mm chisel was used to make a vertical stop cut on the buccal bone distal to the second molar, with the bevel placed distally, and the bone was to be sacrificed. By obliquely angling the chisel’s bevel towards the distobuccal bone over the impacted third molar, a second osteotomy cut was made from the lower end of the vertical stop cut. The triangular piece of buccal cortex adjacent to the buccal surface of the crown was removed next. The bone distolingual to the third molar was then split by using a 5 mm chisel placed distal to the third molar, with the bevel facing upward and lingually and directing towards the opposite side premolar. The cutting-edge of the chisel was kept parallel to the external oblique ridge. The angle of the chisel was held at 45° to the occlusal plane, depending on the amount of lingual bone that will be removed. The chisel was then driven by firm taps with the mallet into the bone to fracture the lingual plate. The fractured lingual plate, if attached to the periosteum, was left in situ. The elevator was then applied mesiobuccally, and the tooth was delivered in a distolingual direction. In vertical and distoangular impactions, the elevator was applied buccally at the bifurcation, or the distobuccal line angle, respectively and the tooth was delivered in a lingual direction. After removal of the tooth, any sharp lingual bony ridge was smoothened, the socket cavity was irrigated with saline, and hemostasis was achieved. The flaps were approximated and closed with simple interrupted sutures using 3-0 Vicryl/silk, and the anterior releasing incision was not sutured. Representative cases are shown in Figures 1–4.
Intraoperative Vertical Stop Cut Placement.
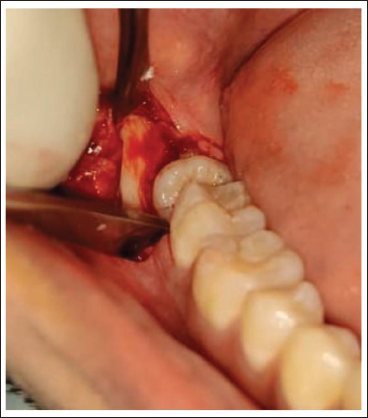
Vertical Stop Cut Placed.
Horizontal Cut Placed.
Splitting Lingual Cortical Plate.
Bur Technique 10
Similar preparation and exposure were done, like the lingual split technique. A 703 number bur was used with a straight handpiece at 20,000 rpm, having an irrigation port to create a “gutter” along the buccal side and distal surface of the tooth. A complete bur depth was used to create the “gutter” while keeping the direction of the bur tip towards the tooth to be removed (Figure 5).
Intraoperative Exposure and Guttering Using 703 Bur.

A mesial purchase point was then created with a bur for application of a straight elevator, and the tooth was delivered out. In case difficulty was experienced during the delivery, additional sectioning 12 was done to facilitate easy removal in segments. After removal of the tooth, any sharp bony ridge was smoothed, the socket cavity was irrigated with saline, hemostasis was achieved, and the flaps were approximated and closed with simple interrupted sutures using 3-0 Vicryl/silk.
In both the operative groups, postoperative care and oral hygiene instructions were given along with antibiotics and analgesics, that is, Tablet Amoxicillin 500 mg + Clavulanic acid 125 mg TDS × 3 days, Tablet Aceclofenac 100 mg TDS × 3 days, Tablet Pantoprazole 40 mg OD × 3 days. Chlorhexidine 0.12% mouth rinse was also advised BD × 10 days, in addition to instructions on mechanical cleansing.
Statistical Tests Used
Categorical variables were analyzed by χ2 test or Fisher’s exact test, and continuous variables were compared using the t-test and Wilcoxon rank sum test. Software used: IBM SPSS (IBM Corp., Released 2011. IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.).
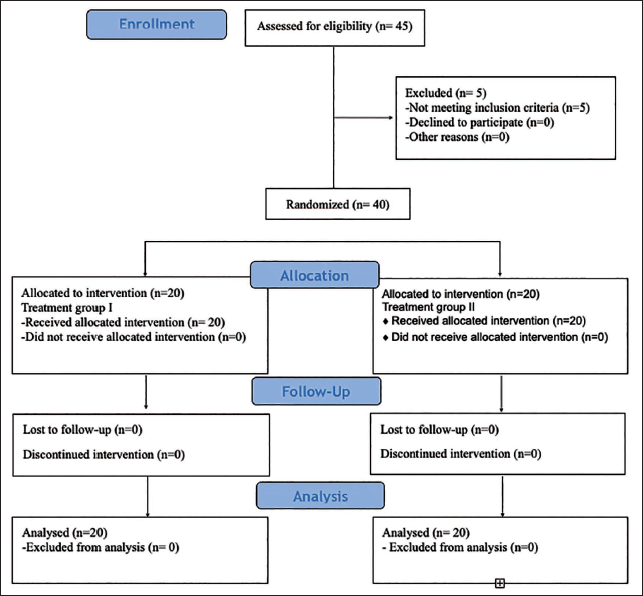
The Consolidated Standards of Reporting Trials (CONSORT) flow diagram for the present study is shown in Figure 6.
Consolidated Standards of Reporting Trials (CONSORT) Flow Diagram.
Results
Demographic Data
Comparison of all preoperative variables is summarized in Table 1. The mean (±standard deviation (SD)) age was 26.2 years (±4.4) for Group I and 27.9 years (±5.9) for Group II. Pericoronitis was the primary cause for extraction, with 14 patients (70%) in Group I and 12 patients (60%) in Group II. Caries as a cause for extraction was equally distributed between both groups, with four patients each (20%). One patient (5%) was referred from orthodontics for extraction in Group I, and four patients (20%) were referred from orthodontics in Group II. One patient in Group I (5%) had prophylactic removal.
Preoperative Variables in Both the Treatment Groups Included in the Study.
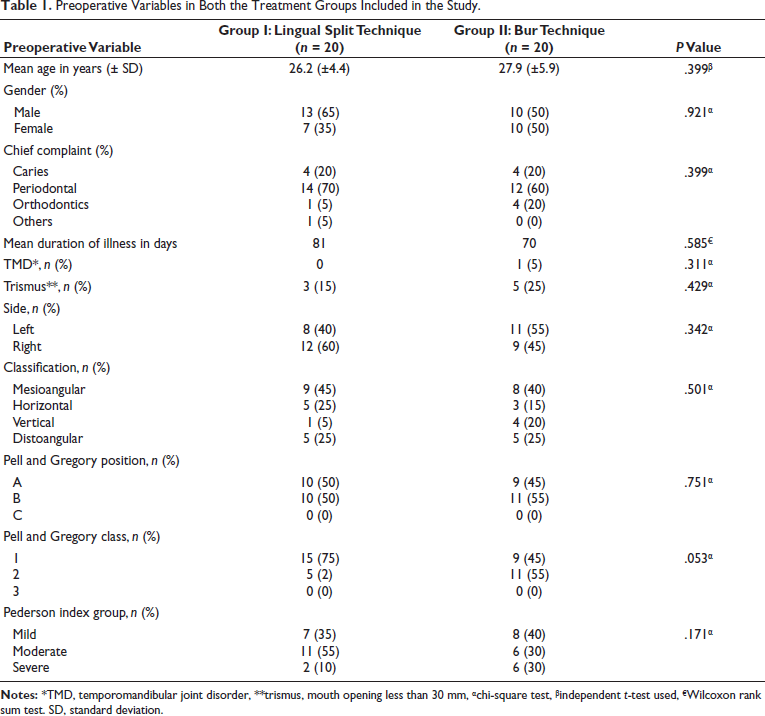
The mean duration of illness was 81 days for Group I and 70 days for Group II. No case in Group I had pre-existing temporomandibular joint (TMD), whereas in Group II, one patient (5%) had anterior disc displacement with reduction of the right TMD. Trismus was seen in three patients in Group I (15%) and five patients in Group II (25%). The most common type of impaction observed was mesioangular, which was in nine patients (45%) in Group I and in eight patients (40%) in Group II. Horizontal impaction was observed in five patients (25%) in Group I and in three patients (15%) in Group II. Distoangular impaction was observed in five patients (25%) in both groups. The least commonly seen impaction was vertical, which was observed in one patient (5%) in Group I and four patients (20%) in Group II.
Pell and Gregory position A was observed in 10 patients (50%) in Group I and in 9 patients (45%) in Group II. Position B was observed in 10 patients (50%) in Group I and in 11 patients (55%) in Group II. Pell and Gregory Class 1 was observed in 15 patients (75%) in Group I and in 9 patients (45%) in Group II. Class 2 was observed in 5 patients (25%) in Group I and in 11 patients (55%) in Group II.
Pederson’s difficulty index score 3-4 was observed in seven patients (35%) in Group I and in eight patients (40%) in Group II. A moderately difficult index (score: 5-6) was observed in 11 patients (55%) in Group I and in 6 patients (30%) in Group II. Difficult gradation (score: 7-10) was observed in two patients (10%) in Group I and in six patients (30%) in Group II. The average time duration from incision to removal of the third molar measured using a stopwatch was 17 (± 1.0) min in Group I and 18 (±1.9) min in Group II. The preoperative variables showed no statistically significant differences.
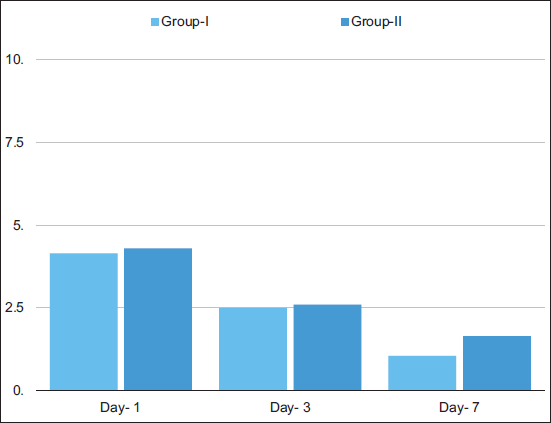
There were no major adverse events in the perioperative and postoperative periods in either group. Distribution of postoperative parameters in both groups is summarized in Table 2. Mean postoperative day 1 pain score (VAS) was 4.15 (±1.7) in Group I and 4.3 (±1.9) in Group II (P = .94). On postoperative day 3, mean pain score was 2.5 (±1.9) in Group I and 2.6 (±1.1) in Group II (P = .28). On postoperative day 7, it reduced to 1.05 (±1.2) in Group I and 1.65 (±1.0) in Group II (P = .06) (Graph 1).
Postoperative Variables in Both the Treatment Groups Included in the Study.
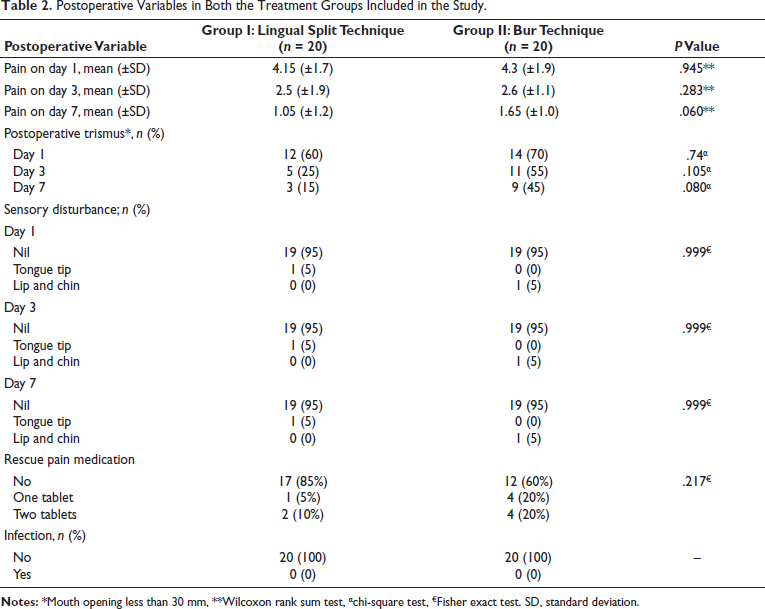
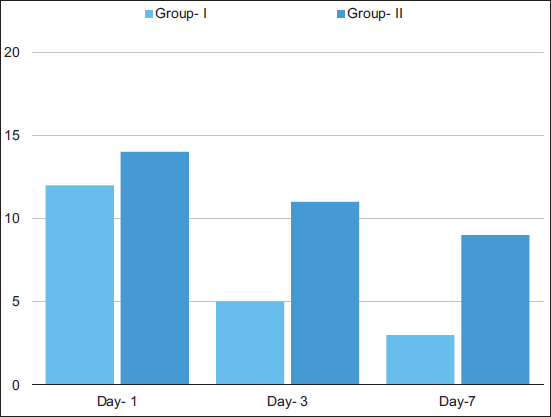
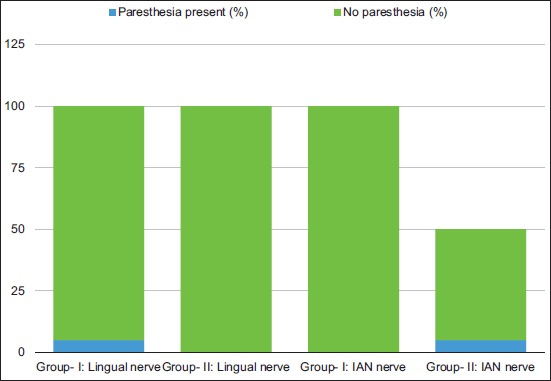
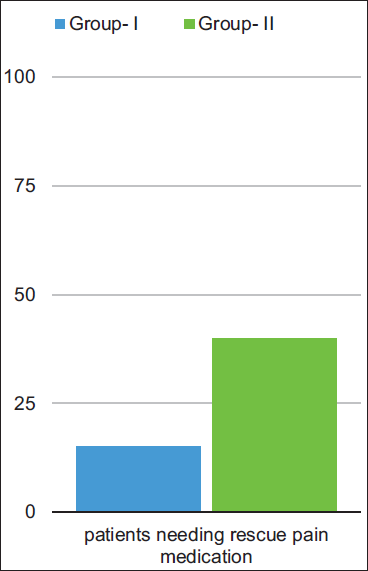
Trismus (<30 mm mouth opening) on postoperative day 1 was observed in 12 patients (60%) in Group I and in 14 patients (70%) in Group II. On postoperative day 3, trismus was observed in 5 patients (25%) in Group I and in 11 patients (55%) in Group II. On postoperative day 7, trismus was observed in three patients (15%) in Group I and nine patients in Group II (45%). The difference in the number of patients having trismus at various postoperative stages in both groups is depicted in Graph 2. Sensory disturbance was seen in one patient (5%) each in both the treatment groups from postoperative day 1 to day 7; however, the nerve afflicted in Group I was the lingual nerve, and in Group II was the IAN (Graph 3). This sensory loss was temporary, and sensation was regained by the end of the second week in Group I and by the fourth week in Group II. Rescue pain medication was not taken by 17 patients (85%) in Group I and 12 patients (60%) in Group II (Graph 4). Infection was not seen in either group. The differences in clinical outcomes were not statistically significant for any of the parameters taken for study between the treatment groups.
Discussion
The present non-inferiority RCT was conducted to compare the lingual split technique using chisel-mallet and current day gold standard bur technique in disimpaction surgeries for mandibular third molars under local anesthesia. The study was conceived during the COVID-19 pandemic from 2019 to 2022. Switching over to a procedure involving less aerosol production could be of benefit in inhalation agent-related pandemic/epidemic scenarios, provided that the alternative technique yields comparable outcomes from a surgical point of view. 4
In this study, all the surgical extractions were done by a single operator after the learning curve was over for both techniques, and hence, there was no operator bias. The groups were comparable in terms of preoperative parameters. A statistical comparison of both techniques did not show any significant difference regarding operative time either; though the lingual split technique consumed less time by 1 min on average than the bur technique (17 vs. 18 min).
Post lower third molar surgery, some pain and trismus are expected in the initial days, regardless of the bone removal technique used. In our study, there was no statistically significant difference in the magnitude of pain scores at postoperative days 1, 3, and 7. This was in contrast to the study by Praveen et al. 13 (n = 90), who concluded that the lingual split technique was more painful than the other techniques. Our study holds similarity to the study by Mocan et al. 14 (n = 20) and Absi and Shepherd 15 (n = 52) who reported no statistically significant differences in pain scores at day 1, 2, and day 7 postoperatively. The patients in the bur technique group consumed more rescue pain medications (Tablet Ketorol DT) on postoperative day 1 when compared to the test group, though it was not statistically significant. Steel, 6 in a systematic review conducted in 2012, compared the lingual split with the bur technique and based on four component RCTs, concluded that there is no significant difference in postoperative pain between the two groups.
Potential causes for postoperative trismus are the presence of an infection that induces temporalis muscle spasm, overextension of the distal release incision, severing the thick temporalis tendon, primary closure without establishing hemostasis, and a traumatic surgical procedure. Increased age (>50 years) and surgical difficulty level can add to postoperative trismus. 16 Singh et al. 5 (n = 150) found higher trismus rates in the lingual split technique group, whereas Mocan et al. 14 (n = 20) found lesser trismus rates using the same technique, and their results were in alignment with the systematic review by Steel. 6 In contrast to the above studies, our study found no statistically significant trismus scores on postoperative day 1, 3, and 7. This variability in results among different studies may indicate sample size issues, variability in surgical technique, in postoperative care, and the importance of avoiding operator bias within a particular study. Measures that have been tried with variable success to reduce postoperative trismus, apart from standard surgical methods, include the use of platelet-rich fibrin (PRF), medications like bromelain, and the use of oral or intramuscular steroids.17–19
One patient complained of altered sensation over the tongue tip in the lingual split group (5%), which was consistent with Absi and Shepherd. 15 The patient regained sensation over 2 weeks. We suggest leaving the distolingual piece of split bone as advocated by Lewis 20 when using the lingual split technique as this makes it less traumatic, and usually the periosteum attachment of the split fragment to the underlying soft tissues ensures good healing. There was no lingual nerve injury among the bur technique group in our study, contradictory to Absi and Shepherd, 15 who reported 8% (n = 4) temporary lingual nerve injury.
In our study, one patient complained of altered sensation over the lip and chin on postoperative day 1 in the bur technique group (5%). The patient regained sensation over 4 weeks. Singh et al. 5 and Rood 21 have reported a high incidence of temporary inferior alveolar injury of 12.07%, whereas in our study, we did not have any incidence of IAN injury with the lingual split technique. According to Mocan et al. 14 and Praveen et al., 13 none of the patients had temporary or permanent inferior alveolar or lingual nerve sensory impairment with both the lingual split and bur technique. There was no permanent nerve injury that was noted during our study.
The frequency of dry socket ranges from 0.3% to 26%. 22 Postoperative infections after third molar removal have been reported to vary from 0.8% to 4.2%. 19 Birn 23 proposed that dry socket results from the release of tissue factors that activate plasminogen and cause the blood clot to fibrinolyze. This may also explain why dry socket seems to occur more frequently after undergoing traumatic or difficult surgery. Nitzan 24 proposed that a localized bacterial infection is the primary cause of dry socket. Increasing age, female gender, oral contraceptives, smoking, surgical trauma, and pericoronitis were all contributing risk factors. In order to lower the incidence of dry socket, the same author discovered that the majority of studies supported the use of copious intraoperative lavage, perioperative antiseptic mouthwash, intra-alveolar medications, and systemic antibiotics. 24 In separate studies, Blonde and Daniel 25 and Sun et al. 26 have drawn conclusions that associated dry socket with older age, female gender, and operating time >15 min, and pre-existing pericoronitis, respectively. Singh et al. 5 reported an overall incidence of dry socket of 12%. Absi and Shepherd 15 reported an overall incidence of infection of 11.5%. In our study, we did not encounter any dry socket or infected wound complications.
Chlorhexidine-containing mouthwash has shown type IV hypersensitivity. 27 One patient in our study reported multiple ulcers and generalized erythema in the oral cavity, mainly on the lips and soft palate, on postoperative day 2. We discontinued the mouth rinse and prescribed local anesthetic gel application for 1 week. On subsequent follow-up, the symptoms had resolved.
Displacement of the root piece into the sublingual pouch was found in one case in the bur technique group. The reason was probably the use of the Cryer elevator, which fractured the thin lingual cortex and led to slippage of the root piece. It was retrieved by placing the index finger at the junction of the lingual pouch and the floor of the mouth, and the root was slowly milked out. In an effort to guide the tooth back upwards on the lingual surface of the mandible, Pogrel 28 advised the operator to insert their thumb below the inferior border of the mandible. He suggested to reflect the lingual gingiva as far as the premolar region and to incise the mylohyoid muscle to access the submandibular space and to deliver the tooth. When doing this, care must be taken to prevent injury to the lingual nerve.
As observed in the results, none of the outcome parameters showed a statistically significant difference between the two groups. However, to prove non-inferiority, the confidence interval of both groups for the primary variable of pain on postoperative day-1 (POD-1) has to be checked.
Since the confidence interval limits cross the delta δ (defined as a VAS difference of ±1) (Figure 7), it can be postulated that if the study were repeated enough number of times, every time it may not yield a statistically insignificant difference, and it may go in favor of the bur technique.
Confidence Interval Limit Across Delta.
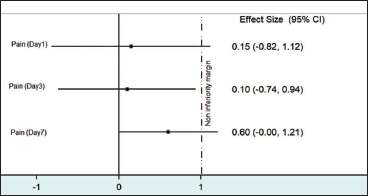
However, one has to look at statistics with a proper understanding of their clinical inference, and here the very tight limits of δ; with VAS differences of even one score as the defining factor of inferiority/non-inferiority may be the culprit in seemingly negative results by the lingual split technique. The other limitations of the study are less sample size and missing out on outcome variable of swelling.
Conclusion
Postoperative clinical outcomes of pain, trismus, infection, need for rescue pain medication, and nerve paresthesia using the lingual split chisel mallet technique in third molar surgery are comparable to those achieved by the gold standard—bur technique. The age-old technique thus yields satisfactory outcomes and is a useful skill tool in the surgeon’s hands.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent were received and obtained, respectively, before initiating the study from all participants.