
Abstract
Peripheral giant cell granuloma (PGCG) is a benign, reactive hyperplastic lesion of the oral cavity. Clinical diagnosis may be suggestive, but histopathology remains the gold standard for confirmation. This article reports a case of a male patient in his 50s with an aggressive growth in the posterior maxilla following extraction of the left first molar 3 months earlier. The lesion, which was associated with root stumps of the second molar, appeared as a sessile, lobulated, firm mass and was completely excised. Histopathological examination confirmed PGCG. Follow-up after 3 months showed satisfactory healing without recurrence.
Introduction
Peripheral giant cell granuloma (PGCG) is one of the most common giant cell lesions of the jaws, regarded not as a true neoplasm but as a reactive hyperplastic lesion. It appears as a soft tissue extra-osseous growth, often originating from the periosteum or periodontal ligament following local irritation or chronic trauma.1, 2 The inflammatory response results in granulation tissue composed of endothelial cells, fibroblasts, and chronic inflammatory infiltrates, presenting clinically as a purple-red gingival swelling. Histologically, multinucleated giant cells reflect osteoclastic-like activity.1, 3
Etiological factors include tooth extraction, over-contoured restorations, chronic trauma from poorly fitting dentures, and subgingival calculus. 3 PGCG has been described by multiple synonyms, such as peripheral giant cell tumor, osteoclastoma, giant cell epulis, and giant cell hyperplasia. 4 The term reparative giant cell granuloma is a misnomer, as reparative potential has not been established. 4 Histopathologically, PGCG closely resembles central giant cell granuloma (CGCG), and some authors consider it the soft tissue counterpart of CGCG. 5
Here, we present a rare case of PGCG in the posterior maxilla of an adult male, highlighting clinical features, histopathology, and outcome.
Case Report
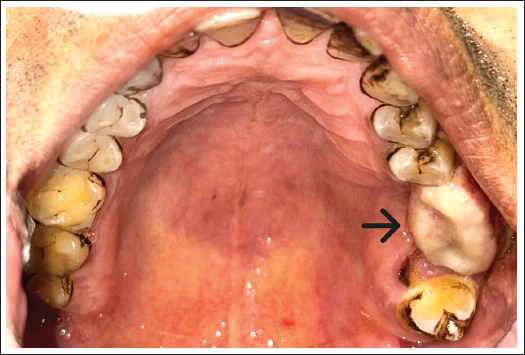
A male patient in his mid-50s reported with a swelling in the left upper jaw for three months. The swelling began as a small nodule that gradually increased in size, associated with intermittent pain but no systemic symptoms such as fever, weight loss, or appetite loss. The patient was moderately built, well-nourished, and systemically healthy. No family or personal history of similar conditions was noted. On extraoral examination, a diffuse swelling was observed over the left posterior maxilla. Intraoral examination revealed a 2 × 2 × 2 cm lobulated swelling extending from the distal surface of 25 to the mesial surface of 28, in relation to missing 26 (extracted 3 months earlier) and root stumps of 27 (Figure 1). The lesion was sessile, firm, purple in color, non-ulcerated, and attached to the periosteum.
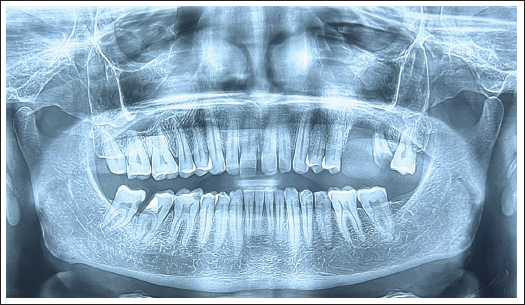
Radiographic examination (orthopantomogram [OPG]) showed no bone resorption or peripheral cuffing of bone (Figure 2). Routine blood investigations, including complete blood count (CBC), prothrombin time (PT), international normalized ratio (INR), activated partial thromboplastin time (APTT), random blood sugar (RBS), and viral markers, were within normal limits. Differential diagnoses considered included pyogenic granuloma, peripheral ossifying fibroma, and peripheral odontogenic fibroma. The lesion was excised under local anesthesia with blunt dissection, followed by extraction of 27 and aggressive curettage (Figure 3). Peripheral ostectomy was not performed as the lesion showed no bone resorption and peripheral cuffing of bone. Hemostasis was achieved by cautery, and the defect created post excision was managed by the primary closure with 3-0 silk sutures.
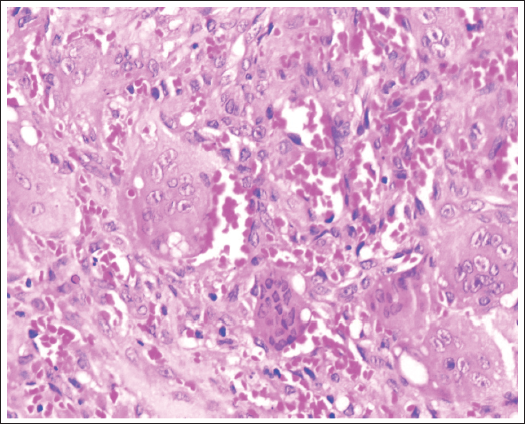
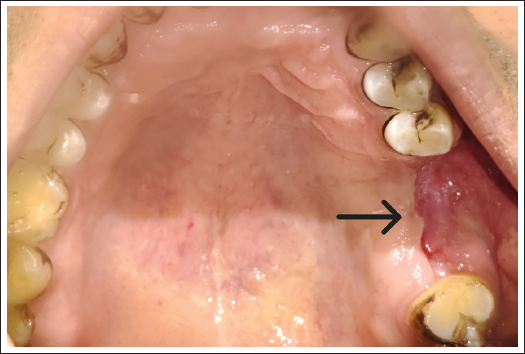
Histopathological evaluation revealed hyperplastic epithelium overlying connective tissue stroma, with multinucleated giant cells (8-15 nuclei) in a fibroblastic background, hemorrhagic areas, and chronic inflammatory cells. Numerous small blood vessels and predominantly chronic inflammatory cells in the form of lymphocytes and plasma cells are also seen (Figure 4). Follow-up at 1 week, 4 weeks, and 3 months (Figure 5) showed uneventful healing with no recurrence. The patient resumed routine activity within a day after surgery.
Intra-oral Examination Showing Lobulated Swelling Extending from the Distal Surface of 25 to the Mesial Surface of 28.
Orthopantomogram Showing No Bone Resorption and Peripheral Cuffing of Bone.
Excised Lesion.

Histopathological Examination Showing Multinucleated Giant Cells.
Follow-up at 3 Months Showing Uneventful Healing.
Discussion
PGCG is a benign lesion believed to arise from the periodontal ligament or mucoperiosteum. 6 The etiology of PGCG is unknown, although chronic irritation, calculus, residual root stumps, and trauma have all been implicated as potential triggers. 3 In the present case, the lesion was associated with root stumps of the maxillary second molar, which likely acted as a persistent source of irritation leading to the reactive overgrowth.
Histopathologically, PGCG is defined by multinucleated giant cells within a fibrovascular stroma. Several hypotheses have been proposed regarding their nature. Some investigators suggest that they represent osteoclasts remaining from physiological root resorption, while others believe they are a response to periosteal injury. 7 Evidence of calcitonin receptor expression further supports their osteoclastic lineage and ability to resorb bone in vitro.1, 7 In our case, abundant multinucleated giant cells confirmed this typical histological picture.
Epidemiological data suggest that PGCG has a female predilection, with reported male-to-female ratios ranging from 1:1.5 to 1:2.8, 9 However, Bhaskar et al. 10 and Zhang et al. 11 reported a slight male predominance. Regarding age, the lesion is most common in the 6- to 12-year range and in the third to fourth decades of life. 9 The present case, a male in his 50s lies outside the typical age groups, underscoring that PGCG can occur beyond expected demographic limits.
Anatomically, PGCG occurs more frequently in the mandible than the maxilla, with a reported ratio of 2.4:1. 12 While most cases occur anterior to the molar region, 13 Pindborg described a predilection for premolar and molar regions. 14 The posterior maxillary occurrence in this case is relatively uncommon.
Radiographically, PGCG is usually confined to soft tissues, but superficial alveolar bone resorption or “cuffing” of bone may sometimes be observed. 15 Differentiation from CGCG is important, especially when CGCG perforates cortical bone and extends into soft tissue. In our case, the absence of radiographic bone resorption favored the diagnosis of PGCG.
Clinically, PGCGs vary from sessile to pedunculated swellings, often reddish-purple in appearance. Our lesion was firm, sessile, and lobulated, without ulceration or bleeding. This is consistent with Regezi et al., 16 who observed that PGCG frequently presents as sessile growths. Firm consistency may indicate lesion maturation and collagenization.
The mainstay of treatment is complete surgical excision with aggressive curettage of underlying tissues. If excision is superficial, recurrence is common. Recurrence rates have been reported between 5% and 20%. 5 In this case, lesion excision with concurrent extraction of root stumps achieved uneventful healing without recurrence at 3 months.
Thus, this case illustrates several atypical features: occurrence in a male in the sixth decade of life, involvement of the posterior maxilla, and clear association with root stumps as an etiological factor. These findings highlight the need for careful differential diagnosis, elimination of irritants, and histopathological confirmation for the management of gingival swellings.
Conclusion
PGCG is a reactive lesion linked to chronic irritation. Although it shows a predilection for younger age groups, females, and mandibular sites, it may present in atypical demographics as in this case. Complete surgical excision, along with removal of local irritants, is crucial to minimize recurrence. Regular follow-up is advised.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent were received and obtained, respectively, before initiating the study from all participants.