
Abstract
Background:
Knowledge confined within academic or clinical silos has limited utility to influence policy. To bridge the gap between evidence and action, a participatory, co-creation workshop was convened of persons living with dementia, family carers, healthcare professionals, policy actors, spiritual or faith-based leaders, and community advocates in a collective process of dialogue, reflection, and solution design.
Objectives:
The research aimed to determine whether stakeholders’ knowledge and attitudes towards dementia improved following the workshop.
Methods:
Data were drawn from a multi-method assessment from a participatory research dissemination and co-creation workshop held in Kumasi, Ghana. A non-parametric Wilcoxon signed-rank test was selected as the primary analytical tool for the pre–post-test. A reflexive thematic analysis was implemented for the qualitative data.
Results:
Following the workshop, participants reported feeling significantly more informed about dementia prevalence in Ghana (Z = 2.510, p = 0.012), the challenges faced by family caregivers (Z = 3.030, p = 0.002), and common caregiver coping strategies (Z = 3.247, p = 0.001). Understanding of socioeconomic (Z = 2.525, p = 0.012) and gender-related (Z = 2.569, p = 0.010) influences on dementia risk, and caregiving also improved. Attitudinally, participants expressed stronger agreement that family caregivers deserve more support (Z = 2.828, p = 0.005), that dementia care should be a higher health system priority (Z = 2.445, p = 0.014), and that faith-based organisations have an important role (Z = 2.001, p = 0.045). Proposed solutions included policy advocacy and systems thinking, community- and home-based care, collaborative networks, caregiver support programmes, stigma reduction and cultural reorientation, and involvement of religious leaders.
Conclusion:
There is a need to formalise and resource a community of practice, thus ensuring sustained collaboration, structured knowledge exchange, collective action across sectors, whilst piloting a caregiver support programme and home-care model with rigorous monitoring and evaluation. It is time for policymakers to enact a comprehensive dementia care policy to guide and regulate all stakeholders in the continuum of dementia care.
Background
The world’s population is ageing. According to the World Health Organisation, 1 the proportion of people aged 60 years and older in 2020 was approximately 1 billion; it is projected that this population will double by 2050, with 80% of the population residing in low- and middle-income countries (LMICs). In Ghana, the population of older people (60 years and above) has increased almost 10-fold between 1960 (i.e., 213,477) and 2021 (1.9 million). 2 The Ghana Statistical Service 2 further reports that of the 1.9 million older people in Ghana, 341,960 live alone. This ageing trajectory, coupled with the high level of solitary living arrangements, raises concern about the mental and neurological health of older people in Ghana. One such concerns is dementia.
Dementia is a neurodegenerative disease that impairs cognitive functions and adversely affects social behaviour and emotional control. 3 In Ghana, a recent study estimated that 23.4% of middle-aged and older adults screened with the Rowland Universal Dementia Assessment Scale showed higher dementia symptoms, with a higher prevalence in women (24.6%) compared to men (21.3%). 4 Available evidence also documents the challenges faced by the carers of individuals living with dementia. These challenges include financial stress, emotional burnout, enduring societal stigma, lack of information, and self-sacrifices.5–7 Furthermore, Ghana, like other sub-Saharan African countries, remains ill-prepared in terms of infrastructure, training, and public awareness to address this challenge effectively. 8
Recognising that the ill-preparedness of Ghana to advance dementia care partly stems from the limited availability of empirical evidence, a research project was undertaken in 2023 to estimate the prevalence of dementia in Ghana, examine the associated factors, explore the lived experiences of family caregivers of individuals living with dementia, and document the coping strategies adopted by family carers.4,5,9 Whilst generating data is important, translating research into practice and policy requires inclusive dialogue and participatory engagement with affected communities and key stakeholders. Knowledge confined within academic or clinical silos has limited utility to influence policy. To bridge the gap between evidence and action, a participatory, co-creation workshop was convened, including persons living with dementia (PLWD), family caregivers, healthcare professionals, policy actors, spiritual or faith-based leaders, and community advocates in a collective process of dialogue, reflection, and solution design. The research aimed to determine whether stakeholders’ knowledge and attitudes towards dementia improved following the workshop. The study also presents co-produced innovative solutions for dementia care tailored to the Ghanaian context.
Our study was conceptually informed by the Knowledge-to-Action (KTA) Framework and Communities of Practice.10,11 The KTA framework conceptualises knowledge translation as an iterative process that moves from knowledge generation and dissemination to contextual adaptation, implementation, evaluation, and sustainability. In parallel, Communities of Practice theory emphasises collective learning through sustained interaction among individuals who share a concern or domain of interest. These frameworks informed the structure of the dissemination workshop by emphasising stakeholder engagement, shared reflection, and collaborative solution development as mechanisms for advancing dementia care policy and practice in Ghana.
Methods
Study design
This multi-method study was conducted between 2 June 2025 and 31 July 2025. The rationale for adopting a multi-method approach, rather than a mixed-method design, was rooted in the distinct and non-integrative purposes of the individual components.12,13 That is, each component (quantitative survey and qualitative workshops) served distinct purposes that were not intended to be integrated analytically. The quantitative component aimed to quantify and assess short-term changes or improvements in stakeholders’ knowledge and attitudes towards dementia before and after the workshop. The qualitative component was designed to be participatory, through the facilitation of in-depth reflections, and the co-production of context-appropriate solutions to the challenges that impede dementia care in Ghana.
Sampling procedures
Participants were recruited using purposive sampling to ensure representation across key stakeholder groups relevant to dementia care and policy translation. Potential participants were identified through professional networks and institutional affiliations in the Ashanti region. Healthcare professionals, policy actors, spiritual or faith-based leaders, and community advocates were invited via email and telephone. Subsequently, text messages were sent to remind them of the day of the workshop. Family caregivers and PLWD were invited through referrals from collaborators involved in the parent study. 9 Individuals were eligible to participate in the workshop if they were aged 18 years or older and had professional, caregiving, advocacy, or lived experience related to dementia. PLWD who had severe symptoms that impaired speech and communication, or the ability to give consent, were excluded. It must also be noted that the study was designed as a stakeholder engagement workshop rather than a powered intervention trial. As such, no formal a priori power calculation was conducted for the pre–post survey component, as the quantitative assessment was exploratory.
Organisation of the workshop
To disseminate the findings of research conducted in 2023,4,5,9 a 1-day workshop was held at the IDL Conference Centre, located within the Kwame Nkrumah University of Science and Technology (KNUST), Kumasi, Ghana. The participants consisted of members from various stakeholder groups in the continuum of dementia care, including individuals living with dementia; family caregivers, healthcare professionals (nurses, medical officers, and psychiatrists), policymakers/implementers (directors from the Ghana Health Service), religious leaders, and members of the academic community (Provost and deans, researchers, and students).
The programme was organised in the following sequence: participants’ arrival, welcome message, pre-workshop survey, presentation of research findings, a diverse panel group discussion, a focused group discussion, post-workshop survey, and a plenary question-and-answer session. During the welcome message, participants were briefed about the workshop’s purpose. The presentation initially did not focus directly on the research findings; instead, it served as an opportunity to educate all stakeholders about dementia, misconceptions and myths, and how they can seek help. After this educational segment, the findings from the initial study (prevalence and associated factors of dementia) were presented, followed by the second (lived experience of caring for persons with dementia) and the third study (family caregivers’ coping strategies). The session lasted approximately 50 min.
The subsequent panel discussion, which lasted approximately 75 minutes, included representatives from the stakeholder groups: a caregiver/PLWD representative (n = 1), as well as representatives from the academic community (n = 2), healthcare professionals (n = 2), religious leaders (n = 2), and policymakers/implementers (n = 1). During this discussion, the panellists shared their perspectives and experiences about dementia caregiving in Ghana, the challenges encountered, and suggestions for areas of improvement. PLWD participation was supported through simplified explanations, allowance for caregiver accompaniment, and flexible discussion pacing. Where necessary, caregivers assisted with clarification.
Ethical considerations
Ethics approvals for the study were obtained from the School Research Ethics and Integrity Committee (SREIC), University of Huddersfield, UK [Approval ID: SREIC/2025/043], as well as the Committee on Human Research, Publication and Ethics (CHRPE), KNUST, Ghana [Approval ID: CHPRE/AP/561/25]. During the invitation to the workshop, participants were provided with a copy of the information sheet and an informed consent form to obtain their written informed permission to participate. The information sheet outlined the workshop’s objectives, the benefits, potential risks and discomfort, their rights, and our expectations of them. On the day of the workshop, the contents of the information sheet and informed consent form were reiterated to all the participants to secure their oral informed consent. All of the participants’ identities were anonymised to protect them.
Quantitative data collection
A computer-assisted personal interviewer known as KOBO Collect was used to administer the pre- and post-surveys. The survey comprised five sections (see Table 1). Participants responded to Sections A to D in the pre-workshop survey, and then responded to Sections A to E in the post-workshop survey. In all, there were 27 questions, with most questions being scored on a five-point Likert scale (Supplemental File 1).
Structure of survey questionnaire.

Statistical analyses
A total of 71 stakeholders participated in the test; however, only 22 completed both the pre-test and post-test. As such, the data analysis was limited to the 22 paired data. The lower number of paired responses was not due to participant drop-out from the workshop, but primarily to incomplete survey submission at the post-test stage. Nonetheless, differential completion may reflect varying levels of engagement or availability, introducing potential response bias. Data analysis was performed in STATA version 14 (StataCorp, College Station, TX, USA). Cronbach’s alpha test was performed on the combined pre-and-post test data to assess the reliability of the items measured. Descriptive analysis, including the estimation of the mean responses, was done. Due to the ordinal nature of the Likert-scale data and the paired, repeated-measures design, the non-parametric Wilcoxon signed-rank test was selected as the primary analytical tool. This test was used to compare the pre- and post-workshop scores for each knowledge and attitude item to determine whether there was a statistically significant change following the intervention. Effect sizes were calculated for each test using the formula
Qualitative data collection and analysis
Four focus group discussions (FGD) were organised. The group was composed of 12–15 participants (n = 69). The largest stakeholder group was healthcare professionals, which was divided into two. This increased the total number of groups to four: two groups of healthcare professionals (n = 30), one group of academics and policymakers (n = 12), one group of family caregivers and PLWD (n = 15), and one of religious leaders and community advocates (n = 12). The discussions during the FGD focused on participants’ reflections on the workshop and research findings, perceived institutional relevance and potential for implementation, and the future direction for dementia care in Ghana (Supplemental File 2). All discussions were audio-recorded and transcribed verbatim. On average, it took 60 min to complete each FGD. The FGDs were conducted in both English and Twi. All Twi transcripts were translated into English and then back-translated to ensure accuracy and preserve meaning before data analysis.
It is important to note that the FGDs were conducted within the context of a participatory dissemination and co-creation workshop rather than a stand-alone qualitative inquiry aimed at exhaustive theory development. Therefore, the study did not seek to achieve data saturation in the traditional sense. Instead, the objective was to capture a breadth of stakeholder perspectives across predefined groups within a structured engagement event. The adequacy of the qualitative data was determined by the diversity of stakeholder representation and the richness of discussion generated during the workshop.
The research team comprised public health researchers and clinicians with prior experience in dementia research, caregiving studies, and health systems strengthening in Ghana and the United Kingdom. This professional background meant that the researchers approached the workshop with a strong orientation towards knowledge translation and policy relevance. While this may have shaped attention towards implementation-focused themes, efforts were made to ensure that analysis remained grounded in participants’ narratives rather than researchers’ assumptions.
A reflexive thematic analytical approach proposed by Braun and Clarke 15 to analyse the data. The analysis was performed in NVivo-14. The transcripts were read several times to help the researchers become familiar with the data and inform the subsequent stage of the analysis. The next phase involved inductive coding, whereby there was no predefined coding scheme; codes were allowed to emerge naturally from the data. The codes were validated across all transcripts to identify patterns, which were then grouped into themes (action domains in this context). The action domains were continuously refined through constant comparison across transcripts, including different stakeholder roles (family caregivers, professionals, religious leaders) and perspectives (problem statements versus solution suggestions). P.A.D. and J.O. performed the initial analysis. The codes and themes were discussed among the larger team. Disagreements were resolved through team discussions until we reached a consensus.
Results
Demographic characteristics
Of the 22 participants with complete pre–post data, 55% were female, and 45% were male. The majority of participants with complete pre-post data were health professionals (86%), with smaller proportions being academic/researchers (9%) and family (5%) (see Figure 1).
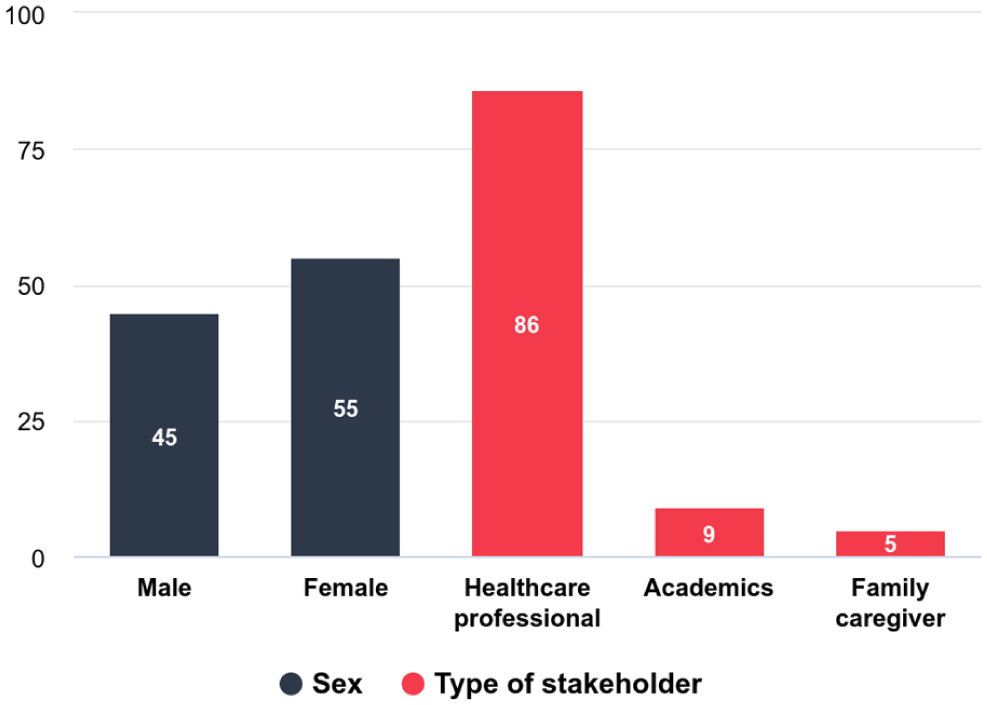
Demographic characteristics of participants with completed pre–post data.
Knowledge of dementia and caregiving
Following the workshop, participants reported feeling significantly more informed about the prevalence of dementia in Ghana (Z = 2.510, p = 0.012) and demonstrated a greater understanding of the challenges faced by family caregivers (Z = 3.030, p = 0.002) (Table 2). There was a significant increase in awareness of common coping strategies used by family caregivers (Z = 3.247, p = 0.001). Participants also showed a significantly improved understanding of the impact of socioeconomic factors (Z = 2.525, p = 0.012) and gender differences (Z = 2.569, p = 0.010) on dementia risk and caregiving. Most of the effect sizes were significantly high, suggesting that the intervention had a substantial short-term impact on participants’ knowledge and awareness across all domains.
Changes in knowledge of dementia and caregiving (pre- and post-workshop).

Cronbach’s alpha reliability coefficient: 0.86.
Attitudes towards PLWD and family caregivers
Post-workshop participants expressed significantly stronger agreement that family caregivers deserve more support (Z = 2.828, p = 0.005) and that faith-based organisations can play an important role in supporting families affected by dementia (Z = 2.001, p = 0.045). Similarly, there was a significant increase in the belief that improving dementia care should be a higher priority for health services in Ghana (Z = 2.445, p = 0.014). There were no statistically significant differences in agreement that PLWD should be involved in decisions about their care (Z = 1.134, p = 0.257), in perceptions of community stigma (Z = 1.524, p = 0.128), or in beliefs rejecting witchcraft and curses as causes of dementia (Z = 0.522, p = 0.602) (Table 3).
Changes in attitudes towards persons living with dementia and family caregivers.

Cronbach’s alpha reliability coefficient: 0.84; Bold: statistically significant.
Support needs to translate the dissemination into action
When participants were asked about the kind of support that must be available to translate the co-designed solutions into actionable projects, many participants highlighted financial support as the most needed resource (27.6%). A proportion (24.1%) of participants focused on greater public education, whilst other participants (17.2%) highlighted continued engagement and networking. A further 17.2% discussed capacity building for healthcare professionals, whilst 6.9% focused on the development of protocols and guidelines for dementia care/referrals, and access to the workshop materials (see Figure 2).

Support needs.
Findings from the FGD
From the thematic analysis, six action domains emerged as co-creation processes. The participants proposed the following as solutions to enhance dementia caregiving in Ghana: policy advocacy and systems thinking, community-based and home-based care services, building a collaborative and support networks, developing a caregiver support programme, stigma reduction and cultural orientation, and involvement of religious leaders. Although there was convergence across stakeholder groups regarding the need for improved awareness and system coordination, healthcare professionals and family caregivers emphasised clinical capacity gaps, caregivers highlighted stigma and caregiving burden, whereas policymakers focused on financing and integration into national strategies. Religious and community leaders highlighted more of the role of faith-based engagement in awareness creation.
Action domain 1: Policy-driven advocacy and systems thinking
One of the actions proposed by the participants was a need to champion policy-driven advocacy and challenge the current system. During the FGDs, the participants asserted that Ghana currently lacks a clear policy, protocol, or guidelines for dementia care. This policy vacuum led to fragmented services, underfunding, weak referral systems, and a lack of institutional accountability. The presentation of research findings on policy gaps helped participants to connect their day-to-day struggles to the need for structural reform: Our policy is silent on protocols. . . if not for this workshop, I wouldn’t have known this. (Participant 4, FGD HCP1)
The analysis revealed that in the absence of a clear national policy on dementia care, the most passionate healthcare professionals would struggle to coordinate activities for the good of the PLWD and their family caregivers. One of the participants stated: We should push for a national policy. Without guidelines, we are not coordinated. Everyone is doing their own thing. (Participant 2, FGD HCP1)
This need for a policy on dementia was further epitomised in the participants’ suggestion to form a policy advisory group from among the workshop participants to engage directly with the Ministry of Health and the Department of Social Welfare: We can’t just wait. A group of us here should draft something and present it formally to the health ministry. (Participant 7, FGD Religious leaders)
The participants asserted that a policy or guideline on dementia care must be one that will effectively regulate spiritual and traditional healer services to prevent exploitation and ensure collaboration with biomedical services. This was a significant step, given that many participants had initially hesitated to critique spiritual practices due to cultural sensitivities: The two potential solutions are implementing a national dementia policy and regulating spiritual practices. Otherwise, people will keep suffering in silence. (Participant 5, FGD Caregivers/Patients)
As a matter of policy, the participants proposed integrating dementia in professional training curricula for all cadres of healthcare professionals. They noted that many healthcare workers graduate without ever learning about dementia in detail, which contributes to misdiagnosis and mistreatment: We should be taught this in nursing school. . . not find out only when we meet a patient. Dementia deserves its own module. (Participant 3, FGD HCP2)
Action domain 2: Community-based and home care services
Another proposed action that emerged from the co-creation process was community-based and home care models. A common theme among the different stakeholders who participated in the workshop was that healthcare professionals cannot do everything, especially when hospital infrastructure is stretched, specialised personnel are limited, and families remain the primary caregivers: If relatives are educated to care for them at home, it improves their quality of life and reduces costs. The hospital cannot do everything. (Participant 4, FGD Caregivers/PLWD)
As such, the participants called for the adoption of home-care or community-based care models of care. Caregivers, in particular, voiced a preference for keeping loved ones at home, provided that they were equipped with adequate training, emotional support, and intermittent professional assistance. Healthcare workers echoed this view, arguing that regular hospital attendance is impractical for many families, describing home-based care as a cost-effective and culturally aligned alternative that could be strengthened with technical support: We said we can create home-like homes. . . even starting with just 16 regional homes where permanent workers can care for dementia patients. (Participant 3, FGD HCP2)
In terms of the practical implementation, the participants proposed that community volunteers, as well as graduate nurses who are yet to be posted to health facilities as full employees of the Ministry of Health, could be trained and prepared to provide home and community-based dementia care services: Most home care nurses are those who have finished school and have not been posted. . . they can be trained to provide long-term care in communities. (Participant 6, FGD HCP2)
Participants also advocated for the use of existing community institutions, such as religious centres, as platforms for dementia education and care coordination: The church is part of the community. We can create dementia-friendly spaces in our churches, train our ushers to assist. (Participant 7, FGD Religious leaders)
Action domain 3: Building sustainable, collaborative, and support networks
The participatory process revealed that although many individuals were already working in dementia-related roles, they had been doing so in isolation, without access to shared resources, peer consultation, or coordinated strategy. For that reason, the participants proposed establishing a sustainable collaboration network to continue advocating and pushing an organised dementia care regime in Ghana. Among the ways of establishing this network was the proposal to use digital platforms like WhatsApp and Zoom: We can’t go back to working alone. Let’s create a WhatsApp group so we can continue educating each other and share challenges from our facilities. (Participant 2, FGD HCP1)
Others recommended quarterly in-person meetings, mentorship pairings between experienced and new caregivers, and regional stakeholder forums facilitated by rotating institutions: There is a possibility of forming a network with religious leaders and researchers to assist in regular sensitisation and community action. (Participant 6, FGD Religious leaders) I believe the more we keep in touch, the more we can coordinate on awareness creation, policy, and how to train others. (Participant 4, FGD HCP1)
The participants also demonstrated a sense of sustainability. They proposed that in the long run, any dementia collaboration network would require some financial contribution from members to reduce donor dependency and enhance the sustainability prospects: We can start free, but maybe in the future we can contribute something small to sustain it. Just so we don’t always depend on donors. (Participant 3, FGD HCP1)
Action domain 4: Developing caregiver support programmes
Throughout the workshop, the physical, emotional, and financial stress that family caregivers endure resonated with all stakeholders. Caregivers described feelings of loneliness, despair, frustration, and, in some cases, hopelessness. Several participants admitted to emotional breakdowns, and even recounted a case of suicidal ideation on the part of caregivers: The caregiver was in a lot of distress . . . he even attempted to [harm himself] . . . dealing with such a patient is a whole lot of stress. (Participant 6, FGD HCP2) Taking care of someone. . . you get tired. . . the stress is real. You cry but you have to hide your tears. (Participant 2, FGD Religious leaders)
Healthcare professionals acknowledged the ordeals of family caregivers: We need to start treating caregivers as clients too—not just as people who accompany the patient. They also need care. (Participant 6, FGD Caregivers/PLWD)
Recognising these challenges, the participants proposed the establishment of a national caregiver support programme. They emphasised that this support programme should not only be about educating the family caregiver. It must also support them psychologically: We should have regular caregiver meetings . . . not just for education, but for support. Let’s let them cry, talk, share, and be human. (Participant 7, FGD Religious leaders)
Another participant proposed monthly meetings for family caregivers: I suggest a programme where caregivers meet monthly to share their challenges, learn from each other, and get professional advice. (Participant 6, FGD Religious leaders)
Action domain 5: Stigma reduction and cultural reorientation
A pervasive issue identified throughout the workshop was the stigma surrounding dementia, deeply rooted in spiritual, superstitious, and cultural narratives that mischaracterise the condition. Stigma was discussed as both interpersonal and institutional. Families hide relatives living with dementia, family caregivers are blamed or pitied, and PLWD are labelled as “mad,” “possessed,” or “bewitched.” These beliefs lead to delayed health-seeking, abandonment, and maltreatment: Most mad people we see outside. . . it’s actually dementia. But because people think it’s spiritual, they are left to roam or are hidden at home. (Participant 7, FGD Religious leaders) Caregivers are stigmatised too. People in the neighbourhood stop visiting your house. They think your relative is cursed and you’re contaminated. (Participant 5, FGD Caregivers/PLWD)
Healthcare professionals also acknowledged their own biases. Some admitted that before the workshop, they viewed dementia as either a natural part of ageing or a condition requiring only spiritual intervention. This honest introspection signalled a deeper cultural issue: Even as a nurse, I used to think it was spiritual. We weren’t taught much about it. This workshop is the first time I’m seeing dementia broken down like this. (Participant 3, FGD HCP1)
Against this background, the participants asserted that stigma must be addressed through compassionate narrative change that resonates culturally. They proposed mass media campaigns that use relatable language and culturally respected figures (e.g., pastors, chiefs, radio hosts) to reshape public perceptions: We need to create a jingle or drama on the radio, something simple but powerful, that tells people this is a disease, not a curse. (Participant 4, FGD Religious leaders)
The participants highlighted the importance of intergenerational education in changing long-standing beliefs. They recommended integrating dementia education into schools, community centres, and youth clubs, arguing that shifting perspectives must begin early to avoid replicating harmful narratives in future generations: Young people need to learn about dementia now. If they grow up thinking it’s witchcraft, the cycle will continue. (Participant 2, FGD HCP1)
Action domain 6: Involvement of religious leaders
Participants also highlighted that integrating dementia care within faith-based settings can be beneficial for improving dementia care. Religious leaders proposed the establishment of formal roles for pastors and Imams at hospitals to assist in the triage and spiritual support of PLWD while also advocating for their referral to medical care: Stationing spiritual leaders at hospitals will help. . . they will assess people and if it’s not spiritual, they will refer them to healthcare professionals. (Participant 1, FGD Religious leaders)
Religious leaders offered their platforms as a conduit to spread awareness messages, correct myths, and frame caregiving as a spiritual act of service. They also committed to referring cases that show signs of dementia to hospitals rather than relying solely on prayer: We should help people know when something is spiritual and when it is not. In church, we can explain dementia and encourage families to go to the hospital. (Participant 6, FGD Religious leaders)
Discussion
This paper examined whether stakeholders’ knowledge and attitudes towards dementia caregiving improved following a research dissemination workshop. The findings revealed significant improvements in the knowledge and attitudes of participants in relation to dementia caregiving. Specifically, participants reported improved understanding of dementia prevalence, caregiver challenges, caregiver coping strategies, and the roles of socioeconomic status and gender in dementia risk and caregiving. In terms of attitudes, there were significant post-workshop increases in agreement that family caregivers deserve more support, that faith-based organisations can play a role in supporting families affected by dementia, and that improving dementia care should be a higher priority for Ghanaian health services. This observation aligns with previous studies conducted in Burkina Faso 16 and the United States 17 that have highlighted the significance of research dissemination workshops as catalysts for knowledge transfer.
It is plausible that the workshop format, which combined didactic presentation with interactive panel and group discussion, contributed to the observed short-term changes. However, given the small paired sample and absence of a comparison group, causal inferences should be made cautiously. Nonetheless, the findings can be interpreted through the lens of Wenger’s Communities of Practice framework, 11 which emphasises learning as a social process that occurs when individuals with shared concerns engage in sustained dialogue, knowledge exchange, and joint problem-solving. 18 The workshop may be interpreted as an exploratory step towards fostering elements consistent with a community of practice for dementia care in Ghana, particularly through shared dialogue and relationship building. This aligns with more reviews that highlight the utility of Communities of Practice in healthcare as mechanisms for knowledge translation, collaboration, and system strengthening.19,20
Although there were significant post-workshop attitude scores, more entrenched normative attitudes did not see any significant improvements. This means that while a short or 1-day workshop can improve knowledge, a continuous, long-term engagement is required to dismantle entrenched beliefs and attitudes about dementia caregiving. These findings can also be interpreted through the KTA Framework, 21 which conceptualises knowledge translation as a dynamic and iterative process. According to the KTA cycle, knowledge must move from synthesis and dissemination to adaptation within the local context, followed by implementation, evaluation, and sustainability. 21 Our participatory workshop aligns with early stages of this cycle by disseminating research evidence, engaging stakeholders in contextualising the knowledge, and co-creating potential solutions. However, later stages of the KTA cycle, such as pilot testing, monitoring, and embedding interventions within health and community systems, remain to be pursued.
The study also presented co-produced innovative solutions for dementia care tailored to the Ghanaian context. One of the major co-created solutions proposed was the need for policy-driven system thinking. The participants highlighted how dementia caregiving would be improved if there were clear guidelines or policies. This is congruent with published studies that document the absence of clear policies as a key barrier to dementia caregiving across LMICs, including Ghana and Nepal.22,23 A distinctive policy on dementia would spell out the diagnostic processes, referral pathways, and effectively regulate the role of spiritual healers and traditional medicine practitioners.
From the analysis, stakeholders acknowledged the current handicapped nature of Ghana’s healthcare facilities. As such, they proposed home-based and community-based services that use task-shifting and leverage community volunteers as a potential care module for delivering dementia care services. The stakeholders asserted that this can be done gradually by instituting residential home care facilities, one in each of the 16 administrative regions of Ghana. In such home care facilities, unposted nurses and community volunteers would then be trained to provide compassionate, person-centred services to PLWD. In addition, they proposed home-based services where family caregivers will be trained to understand the needs of the person living with dementia. The proposal for home-based dementia care alongside residential long-term care services aligns with Samus et al., 24 who assert that “home-based dementia care should be considered the nexus of new long term care models.”
Stakeholders of this workshop underscored the need for continuous engagement; hence, they called for a sustained collaborative network and heavy investment in caregiver support programmes. The proposed caregiver support programme will transcend education to provide psychosocial and, in extreme cases, financial support to caregivers. This is an important solution proposed by the stakeholders, as there is evidence supporting the relevance of such caregiver support programmes.25,26 This finding is corroborated by Zebrak and Campione’s study, 25 which found that at least 4-h participation in a national caregiver support programme resulted in a significant decline in caregiver burden. Similar findings have been reported in Korea, 26 where an 8-week community-based support programme resulted in significant decreases in personal strain among the intervention group compared to caregivers in the control arm. The recommendation for a sustainable dementia network is based on the belief that communities of practice and academic-community partnerships can support implementation, maintain momentum after one-off events, and enable iterative learning. 27
The study revealed that financial support was the most important factor that stakeholders believe needs to be available to help in the implementation of the co-created solutions. This finding is not surprising because the co-created solutions (i.e., caregiver support programmes, community-based care models, and the creation of a sustained collaboration network) presuppose some form of financial input. For example, financial resources would be needed to facilitate the establishment of residential long-term care homes across the 16 administrative regions; also, such resources will be needed to organise the caregiver support programmes. Without dedicated financial allocation, these well-conceived programmatic solutions remain unfunded mandates, placing further strain on an already overburdened and under-resourced community health system. 28
Strengths and limitations
This study is arguably the first in Ghana to assess how research dissemination workshops influence knowledge and attitudes about dementia care. Also, the use of a paired pre- and post-workshop allowed us to measure the immediate impact of the workshop. However, a key limitation is the small sample size (22 paired responses), which limited statistical power and prevented subgroup analyses. Pursuing a subgroup analysis would have increased the risk of type I and type II errors. It is important to note that the improvements observed in knowledge and attitudes were short-term and do not reflect retention of knowledge or sustained attitude change. Therefore, it should be considered exploratory. Given that the researchers were available at the time of the pre-and-post tests, there is a possibility of social desirability bias. Future research should aim for a subgroup analysis with a larger sample size and a longitudinal design to evaluate the long-term impact of such workshops. It must also be noted that the questionnaire used has not been validated, nor was it piloted. As such, future studies may want to validate it for the Ghanaian or similar contexts.
Conclusion
The participatory dissemination workshop, combining evidence presentation with co-creation, resulted in immediate improvements in stakeholder knowledge and several caregiving-related attitudes to dementia care. Stakeholders converged on six priority areas that span policy reform, workforce training, community-based care, caregiver support, stigma reduction, and faith-based engagement. In line with the KTA Framework and Wenger’s Communities of Practice framework, it is concluded that the next step must be to formalise and resource a community of practice, ensuring sustained collaboration, structured knowledge exchange, and collective action across sectors while piloting a caregiver support programme and home-care model, and rigorously monitoring and evaluating their impact. Complimentarily, these actions would move dementia care in Ghana further along the KTA cycle from knowledge dissemination towards sustained implementation and system-level change. Now is the time for the Parliament of Ghana to enact a comprehensive dementia care policy to guide and regulate all stakeholders in the continuum of dementia care.
Supplemental Material
sj-pdf-1-pcr-10.1177_26323524261442208 – Supplemental material for Co-creating dementia knowledge and action in Ghana: Evidence from a participatory stakeholder workshop
Supplemental material, sj-pdf-1-pcr-10.1177_26323524261442208 for Co-creating dementia knowledge and action in Ghana: Evidence from a participatory stakeholder workshop by Precious Adade Duodu, Joshua Okyere, Dorothy Wilson, Abigail Kabukie Dosoo, Peter Boakye, Bibha Simkhada, Caroline Barker, Warren Gillibrand and Padam Simkhada in Palliative Care and Social Practice
Supplemental Material
sj-pdf-2-pcr-10.1177_26323524261442208 – Supplemental material for Co-creating dementia knowledge and action in Ghana: Evidence from a participatory stakeholder workshop
Supplemental material, sj-pdf-2-pcr-10.1177_26323524261442208 for Co-creating dementia knowledge and action in Ghana: Evidence from a participatory stakeholder workshop by Precious Adade Duodu, Joshua Okyere, Dorothy Wilson, Abigail Kabukie Dosoo, Peter Boakye, Bibha Simkhada, Caroline Barker, Warren Gillibrand and Padam Simkhada in Palliative Care and Social Practice
Footnotes
Acknowledgements
We thank Prof. Veronica Millicent Dzomeku, Dr. Nana K. Ayisi-Boateng, and Prof. Christian Agyare for supporting the implementation of the dissemination workshop. We also acknowledge the Ashanti Regional Director of the Ghana Health Service for adding a voice to the discussions at the dissemination workshop. Special thank you to all PLWD, family caregivers, healthcare professionals, religious leaders, and community leaders who participated in this study.
Ethical considerations
All methods in this study align with the Helsinki Declaration and Belmont Declaration. Ethics approvals for the study were obtained from the School Research Ethics and Integrity Committee (SREIC), University of Huddersfield, UK [Approval ID: SREIC/2025/043], as well as the Committee on Human Research, Publication and Ethics (CHRPE), KNUST, Ghana [Approval ID: CHPRE/AP/561/25].
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received the School Rapid Research Support Fund (Grant number: QRHH06). However, the content of this work is solely the responsibility of the authors and does not necessarily represent the official views of the University of Huddersfield.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All relevant data are within the paper. Any other data or material associated with this manuscript is available on request through the first author (PAD).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.