
Abstract
Background:
Women who have undergone mastectomy often report fatigue, shoulder dysfunction, and a diminished quality of life. Structured educational and supportive care programs have the potential to facilitate improved functional recovery and overall well-being post-surgery.
Aim:
This research aimed to evaluate the effect of the educational supportive care program on fatigue, shoulder functional ability, and quality of life among women after mastectomy.
Design and methods:
A quasi-experimental research design was conducted at Tanta Cancer Center, Gharbia Governorate, Egypt (affiliated with the Ministry of Health and Population). A purposive sample of 84 women undergoing mastectomy was included in the study (intervention group included 42 women, and control group included 42 women). Four tools were utilized (A demographic and cancer-related data sheet, cancer-related fatigue assessment (EORTC QLQ-FA12), shoulder pain and disability index (SPADI), and Functional Assessment of Cancer Therapy—general (FACT-G)). Means, standard deviations, frequencies, percentages, independent t test, and Chi-square test were used for statistical analysis.
Results:
The results of the present study showed that, during the first week post-mastectomy, no statistically significant difference was observed between the two groups toward fatigue level, shoulder pain and disability, and all quality-of-life domains. On the other hand, a highly statistically significant improvement was observed among the study group at 6 weeks and 3 months post the intervention, in which the study group showed significantly lower levels of fatigue, reduction in shoulder pain and shoulder-related disability, and quality-of-life scores increased in all domains. Additionally, there was a significant negative correlation between total quality-of-life scores and total fatigue, shoulder pain, and shoulder disability in both the study and control groups at all measurement times.
Conclusion:
The findings indicate that the educational supportive care program was associated with improvements in fatigue, shoulder functional ability, and quality of life among women after mastectomy. However, the quasi-experimental study may limit causal interference and the generalizability of the findings.
Recommendation:
In order to enhance women’s functional status and their quality-of-life post-mastectomy, educational supportive care should be integrated into routine care.
Plain language summary
Women who undergo mastectomy often experience physical difficulties, emotional stress, and reduced quality of life after surgery. Women who have had a mastectomy do not get help and information to deal with their daily life and new reality after losing their breasts. This study looked into whether a special care program that teaches and supports women can help those who have had a mastectomy in Egypt. Women who have experienced a mastectomy need this form of support to help them manage their lives. Women who have experienced a mastectomy often feel isolated in their challenges and need support on how to manage their daily activities post-surgery. This study aims to assess if supportive care impacts women who have had a mastectomy. The program helped women by teaching them things they could actually do giving them guidance and supporting them emotionally to heal physically take care of themselves and deal with situations. In this study the women who received educational programs were compared to the women who received the usual care. The women’s ability to function and their overall quality of life were checked before. After they went through the program. The results showed that the women who had been participants of the educational supportive care program had better daily functions than the women who did not. The results of the study show that the women are helped by the educational supportive care programs to recover from the mastectomy. This study shows the importance of ensuring that women are provided with educational and supportive care programs to enhance their recovery from the mastectomy.
Introduction
Breast cancer is a highly prevalent, aggressive, and fatal cancer in women worldwide, which may spread and metastasize extensively to adjacent tissues and organs. In 2021, GLOBOCAN statistics showed that it is among the most common cancers (11.7% of all new cases, 2,261,419 people) and the fifth leading cause of cancer mortality (6.9% of all cancer deaths, 684,996). 1 WHO predicts that the incidence of breast cancer will continue to rise by 2030 as a result of global lifestyle changes, highlighting the growing burden of this disease. 2
Breast cancer is treated with a combination of surgery, chemotherapy, and radiation therapies. Surgery often results in scarring and changes to the natural breast shape; therefore, women may have psychological issues regarding their appearance. Conversely, chemotherapy and radiotherapy come with several side effects, including fatigue, nausea, weight reduction, hair loss, and alterations in skin pigmentation. These alterations create unease for a young woman to experience, as they are typically associated with aging. Additionally, discomfort arises from hot flashes, muscle cramps, joint pain and stiffness, as well as a reduced sex drive, creating challenges for women to endure. 3
Mastectomy is a difficult decision that can significantly affect women in their daily routines, social activities, relationships, and overall health and well-being. Some women may experience pain, fatigue, sensory disorders, lymphedema, and functional limitations in the shoulder and upper limb, following surgery, which can negatively impact daily activities and overall quality of life.4,5 The decision to undergo a mastectomy is personal and influenced by various factors such as individual circumstances and preferences, cancer progression, tumor features, and genetic mutations. 6
According to Azim et al., 7 review of 13 studies in Egypt involving over 11,000 breast cancer patients, it’s estimated that about 85% of the time, the chosen treatment is a modified radical mastectomy. Jassim and Whitford 8 found that women who had a mastectomy reported a lower quality of life compared to those who underwent a lumpectomy. Similarly, research by Kamińska et al. 9 in 2015 and Enien et al. 10 in 2018 indicated that women undergoing breast conservation therapy generally experienced a higher quality of life than those who had a mastectomy.
Considering the variety of psychological, physical, and social challenges numerous women encounter after undergoing a mastectomy, it is clear that comprehensive, research-backed educational initiatives are essential. Educational supportive care is defined as a structured intervention combining patient education with psychological and physical support to improve coping strategies, functional ability, and overall quality of life during cancer treatment and recovery. 11
Post-mastectomy supportive training programs that cover physical activity, self-care, pain management, and psychosocial support assist women in developing adaptive skills and using proactive strategies that will enhance patient functional ability, decrease stress, and increase quality of life. Education can also be instrumental in minimizing psychological distress by enhancing self-esteem, body image, and social and family functioning, aligning the program with principles of supportive and palliative care. 12
Health care providers, particularly nurses need to acknowledge the alterations women go through following a mastectomy and offer tailored information, ongoing care, and emotional assistance. Postoperative nurses must demonstrate competencies in effective communication, the use of assistive technologies, family and patient-centered care, and the promotion of self-care to enhance patients’ quality of life. This involves adhering to evidence-based practices, collaborating with interdisciplinary teams and having the capability to enhance the quality of care. These skills are vital for improving secure and efficient care transitions through multiple care settings and help women develop coping skills and strategies, leading to a greater sense of fulfillment. 13
Significance of the study
In Egyptian women, Breast cancer (BC) is the most common cancer (34.9% of cancers diagnosed) and has an estimated age-standardized incidence rate of 55.4 per 100,000. BC rates are higher in females over 50 years of age, and it is likely to be a more aggressive disease in young women, particularly with certain clinicopathologic factors such as poorly differentiated. 14 Treatment of breast cancers relies on surgery, with mastectomy being the mainstay and crucial component of the treatment plan, and early mastectomy contributes to survival. 15
Women who undergo mastectomy often face a range of interrelated challenges that affect their physical, emotional, and social well-being. Physically, many patients report persistent fatigue, pain, lymphedema, limited shoulder movement, and changes in sexual function. Alongside these effects, psychological issues such as anxiety, fear of recurrence, depression, and reduced satisfaction with life are also common. Together, these experiences can substantially diminish overall health and quality of life. 16 Although pharmacological treatments are essential in cancer management, they do not reliably alleviate all cancer-related symptoms, especially emotional and psychosocial concerns, highlighting the importance of non-pharmacological approaches in supportive cancer care. Educational supportive care program in oncology are structured intervention that focus on managing and preventing adverse effects from cancer and its treatments, focusing on symptoms, psychosocial issues, and quality of life throughout the disease trajectory. 17
Therefore, the aim of this study was to evaluate the effect of the educational supportive care program on fatigue, shoulder functional ability, and quality of life among women after mastectomy.
Aim of the study
The study aimed to evaluate the effect of the educational supportive care program on fatigue, shoulder functional ability and quality of life among women after mastectomy.
Research hypotheses
Subjects and methods
Research design
A quasi-experimental two group pretest–post-test design was used to examine the effect of the educational supportive care program on fatigue, shoulder functional ability, and quality of life among women after mastectomy. The experimental group received the educational program along with the routine care, while the control group received only routine care. Pre and post-assessment were conducted to compare changes between the two groups.
Setting
This study was conducted at Tanta Cancer Center, Gharbia Governorate (affiliated with the Ministry of Health and Population), and data were collected from December 2024 to August 2025.
Sample type and size
A purposive sample of women who underwent mastectomy and met the inclusion criteria was recruited for the study. Sample size calculation using G*Power software version 3.1 (Heinrich Heine University Düsseldorf, Germany) for an independent t test assuming a medium effect size (Cohen’s d = 0.5), a significant level of 0.05, and statistical power of 0.8. Based on this calculation, 42 participants were required in each group, resulting in a total of 84 participants. The study group received an educational supportive program in addition to the routine hospital care, while the control group received only the routine hospital care. Participants weren’t selected randomly; recruitment was done sequentially: women meeting the inclusion and exclusion criteria were assigned to the study group for 1 week, and the control group the following week, continuing in this alternating manner until the target sample size was reached. Replacement of dropped-out subjects will occur through recruiting sufficient numbers to maintain the original sample size.
Inclusion criteria
Women must have had a mastectomy (modified radical mastectomy) and be 20 years of age or older; they must also be able to communicate and comprehend the instructional materials relative to the study, and provide informed consent to participate in an educational program for breast cancer rehabilitation.
Tools for data collection
Tool I: A demographic and cancer-related data sheet to record women’s age, marital status, education, occupation, residence, type of breast cancer, stage of cancer, duration of cancer since diagnosis, side of surgery, treatment, and family history.
Tool II: Cancer-Related Fatigue Assessment (EORTC QLQ-FA12)
The EORTC QLQ-FA12 is a self-administered questionnaire developed to assess fatigue in cancer patients. It evaluates physical, emotional, and cognitive aspects of fatigue, along with its impact on daily and social activities. This tool was designed by the European Organization for Research and Treatment of Cancer (EORTC) as a supplementary module to the QLQ-C30 and is widely used in clinical research to track fatigue over time. 18 Each item is rated on a 4-point scale from 1 (not at all) to 4 (very much). Multi-item scales are averaged to produce a raw score, while single-item measures use the individual item score directly. Raw scores are transformed to a 0–100 scale, with higher scores indicating a greater fatigue or more interference with daily life.
Tool III: Shoulder pain and disability index
The tool developed by Roach et al. 19 in 1991 and composed of two domains that assess both shoulder pain severity and functional limitation in daily activities. The tool contains 13 items, 5 measuring pain and 8 evaluating disability. Each item was rated on an 11-point numeric scale ranging from 0 “no pain or difficulty” to 10 “worst pain or inability to perform the task.” For scoring, the values of each domain were summed, divided by the maximum possible score for that domain, and then multiplied by 100 to obtain a percentage. Separate scores can be repeated for the pain and disability subscales, or the mean of both can be used to represent the overall shoulder pain and disability index (SPADI) score. The total score ranges from 0 to 130 where higher scores denote greater pain intensity and more pronounced functional limitation.
Tool IV: Functional assessment of cancer therapy—general
The questionnaire was originally developed by Cella et al. 20 in 1993. It is a self-administered tool designed to evaluate the overall quality of life in people living with cancer, regardless of their diagnosis or treatment stage. Functional Assessment of Cancer Therapy—General (FACT-G) contains 27 items divided into four main areas: physical, social /family, emotional, and functional well-being. The questions target concerns that may come up as a result of cancer, cancer treatment (such as pain, fatigue, emotional woes, social support, and performing daily living activities). By evaluating the multiple dimensions of a person’s life, FACT-G allows physicians and researchers to pinpoint specific issues as well as measure any changes to these areas over time. Each of 27 items in the FACT-G is related to a 5-point Likert scale ranging from 0 (“not at all”) to 4 (“very much”). Scores for negatively worded items were reversed so that higher scores consistently represent a better quality of life. Subscale scores are obtained by summing the responses within each of the four domains: physical, social/family, emotional, and functional well-being. The total FACT-G score is then calculated by combining all subscale scores, with higher overall scores indicating better perceived quality of life.
Tools’ validity
To ensure the validity of study tools, each instrument was assessed by a panel of five experts in the field of obstetrics and gynecology nursing, psychiatric nursing, and medical surgical nursing at the Faculty of Nursing, Tanta University. The experts assessed the clarity, relevance, comprehensiveness, and appropriateness of the items in relation to the study objectives and the target group of women after mastectomy. Based on their feedback minor refinements were made to enhance the understanding and ensure cultural suitability.
Tools’ reliability
The reliability of the study tools was ensured through the use of a well-validated instrument. The EORTC QLQ-FA12 demonstrated a high internal consistency in international validation studies with Cronbach’s alpha values ranging from 0.79 to 0.90 indicating reliable measurement of cancer-related fatigue. 18 The SPADI also showed excellent reliability with a Cronbach’s alpha of “0.90 or higher,” confirming its stability in assessing shoulder pain and function. 19 The FACT-G revealed a strong consistency across studies with an overall alpha of around 0.88 and subscales between 0.71 and 0.83 reflecting dependable assessment of quality of life among cancer patients.20,21 This research involved translating the tools from their source language (English) into an Arabic version by the researchers, which was done according to standard translation protocols, with subsequent implementation of the translated tools with participants. In the current study, the EORTC QLQ-FA12 demonstrated acceptable levels of reliability as indicated by a Cronbach’s alpha between “0.81 and 0.91,” while the SPADI had a score of 0.92 and FACT-G had a score of 0.87 with subscales ranging from “0.75 and 0.86.” The values supported the suitability of the tools for assessing fatigue, shoulder disability, and quality of life among women undergoing mastectomy.
Ethical consideration
Before starting the study, ethical considerations were carefully looked into. The Scientific Research Ethical Committee at Tanta University’s Faculty of Nursing gave the study approval for its completion (854-12-2025), and the places where the research would happen also gave their okay. To make sure participants felt comfortable and trustworthy, the researchers explained what the study was about and why it was important before using any tools. Everyone involved had the chance to give their informed written consent after being told that what they said would be kept private. The research presented no danger to anyone’s mental, social, or physical health. Following data processing, the tools utilized for data collection were eliminated to safeguard individuals’ privacy. The whole research was conducted meticulously to guarantee that no disrespectful comments occurred and that individuals’ rights were honored. Participants had the liberty to exit the study whenever they wished.
Pilot Study
In a brief trial, nine women representing 10% of the participants had previously had a mastectomy. We aimed to evaluate the tools’ impartiality, clarity, usefulness, and significance. Furthermore, we sought to identify any problems with the wording or sequence of the questions that could hinder data collection. The researchers also calculated the time required to collect the data. They tweaked the tools based on what they learned from this test, and to make sure the main group wasn’t influenced, the people from the test group didn’t take part in the main study.
Field work
Preparatory phase
This phase represented the initial step of the study. The researchers obtained formal approval from Tanta—Faculty of Nursing and hospital administration to conduct the research in the oncology surgery department and the outpatient clinic. A thorough review of related literature was carried out to define the study problem and identify the suitable method and tools for data collection. Based on the review, the researcher prepared four tools to evaluate demographic data, cancer-related fatigue, shoulder disability, and quality of life. These tools were examined by experts in nursing. After that, a pilot study was conducted on a small group of women to test the feasibility of the instruments and the necessary modifications.
Interviewing and assessment phase
After obtaining the official approval, the researcher met eligible women who had undergone a mastectomy and explained the aim and the procedure of the study. Each woman was assured that participation was voluntary and confidentiality would be maintained. Informed consent was obtained prior to data collection. During this phase, demographic and cancer-related data were collected before the educational program was introduced. The questionnaire took about 10–15 min on average. Telephone numbers were collected to facilitate follow-up and reminders throughout the study.
Planning phase
Based on the information obtained in the assessment phase, the researchers developed an educational supportive care program designed to meet the physical and psychological needs of women after mastectomy. The program’s main objectives were to reduce fatigue, shoulder disability, and improve quality of life. The educational content was organized into sessions supported by simple visual materials and printed guidelines written in Arabic. The plan specified several sessions, duration, and methods of teaching such as discussions, demonstrations, and feedback to ensure effective understanding and participation.
Implementation phase
This program was only applied to the study group, whereas the control group received the standard hospital care without the intervention. The intervention consisted of several educational and practical sessions spread over several weeks, each lasting 45–60 min, with twice-weekly small group sessions to allow for active involvement and comfort, with the use of visual materials, such as presentations, videos, and simplified booklet in Arabic, to help the women understand and be able to practice independently, and the sessions were completed 2 weeks before surgery and after reviewing initial assessment data to determine the challenges the women faced.
The opening session introduced the goals of the program and provided an overview of mastectomy, including its purpose, different types, possible complications, and the effects on physical and emotional health. Women were encouraged to share their emotions and worries, creating a setting that fostered motivation and involvement. Other sessions included practical skills training: the second session focused on exercises in the very early postoperative period (1–7 days) to avoid shoulder stiffness and promote blood circulation without affecting the wound (such as hand, finger, wrist, and elbow movements) and to prevent respiratory complications (such as breathing exercises), while the third session concentrated on the early postoperative phase (7–10 days after drain removal) to gradually restore the normal range of motion of the shoulder through appropriate exercise in this stage (such as shoulder pendulum exercises, wall climbing exercises, and using a stick exercise to move the arms together). The fourth session aimed to restore muscle strength and improve shoulder function by training participants in a specific set of exercises after 6 weeks to 3 months. Permitted exercise during this period included light stretch exercises, simple resistance band, posture correction exercises, and a gradual return to daily activities (such as dressing and lifting light objects). The suggested exercises will be performed by participants for 15–20 min two times daily. The last session’s topics were proper nutrition, wound care, sleep patterns, and emotional distress, allowing the women to talk about their own experiences with each of these topics to strengthen their bond as peers and support each other regarding their body image and relationship issues. Every meeting ended with a summary of the main ideas and a question-and-answer period, tasks were given out and in later sessions, adherence was monitored. The instructional booklet was given at the first session and served as a continuous source of information. Follow-up visits and phone calls by the researcher were used to encourage continued engagement and address any difficulties.
A summary of educational sessions including content, duration, objectives, standardized versus individualized components, and adherence monitoring was presented in Table 1.
Summary of educational sessions including content, duration, objectives, standardized versus individualized components, and adherence monitoring.

Evaluation phase
This phase was conducted to assess the results of the educational suppurative care program at various points following a mastectomy. The first evaluation occurred during the early postoperative periods specifically between the third and seventh postoperative days, when the women came back to the hospital to have their drains removed. At this stage baseline information was collected about fatigue, shoulder pain and disability, and overall well-being before beginning the instructional program. Six weeks following a mastectomy, a second assessment was conducted to evaluate the program’s initial impact on quality of life and functional recovery. Three months post-mastectomy, the third evaluation was conducted to gauge the program’s long-term impact. To ensure consistency and accuracy when comparing the results across the three phases, all assessments used the same instruments.
Statistical analysis
The data received initial validation prior to being input into the computer system. The organized collected data were given codes and were statistically analyzed by applying appropriate methods and tests, and through the use of the Statistical Package for Social Sciences (SPSS version 25.0) (IBM Corp., Armonk, NY, USA). The following descriptive statistical analyses were conducted: means, standard deviations, frequencies, percentages, and other relevant calculations. For inferential statistical analyses, inferential statistics were performed in accordance with the outcomes anticipated from the study. The mean scores for the baseline (continuous) variables between the study and control groups were compared using an independent t test, while the Chi-square test was used for categorical variables.
To assess changes over time and differences between the study and control groups across repeated measurements (first week post-surgery, 6 weeks, and 3 months), Repeated-Measures Analysis of Variance was performed. This test was selected as it is appropriate for evaluating within-subject changes over time as well as between group differences, given the study design, which involved repeated measurements of the same participants at multiple time points. Effect size was calculated using Partial Eta Squared (η2) to determine the magnitude of the intervention effect. In addition, 95% confidence intervals (CIs) were reported for mean differences. Person correlation coefficient was used to examine the relationships between total quality-of-life scores and fatigue, shoulder pain, and shoulder disability scores. A p value ⩽0.05 was considered statistically significant, while a p value of 0.001 was considered highly statistically significant.
Results
Table 2 summarizes the demographic characteristics of both groups. No statistically significant differences were observed between the study and the control groups (p > 0.05), indicating that both groups were comparable at baseline.
Distribution of both groups according to demographic data (n = 84).
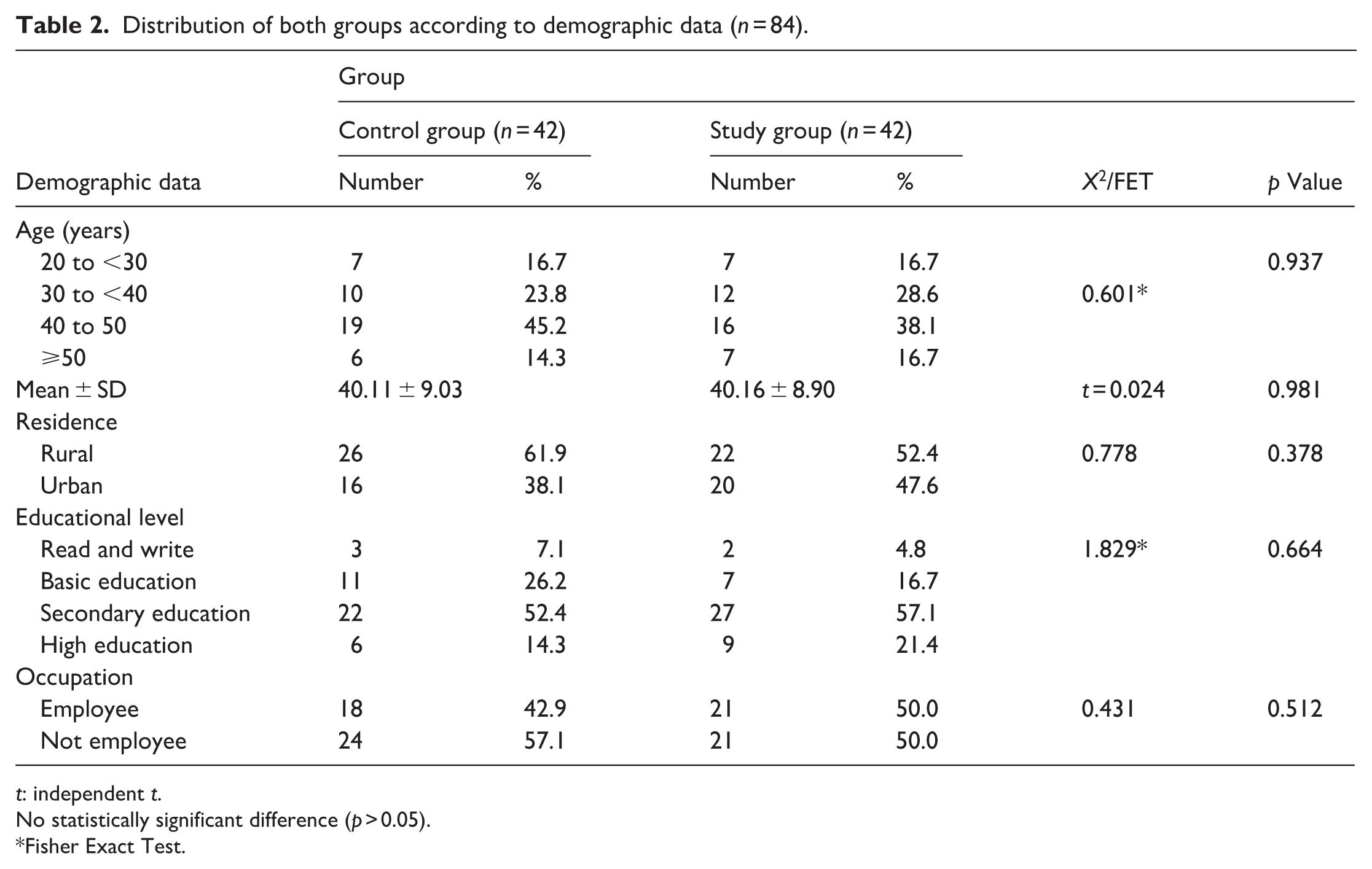
t: independent t.
No statistically significant difference (p > 0.05).
Fisher Exact Test.
Table 3 summarizes cancer-related characteristics for both groups. No statistically significant differences were observed between the study and the control groups (p > 0.05), indicating a comparable baseline cancer-related profile.
Distribution of both groups according to cancer-related data (n = 84).
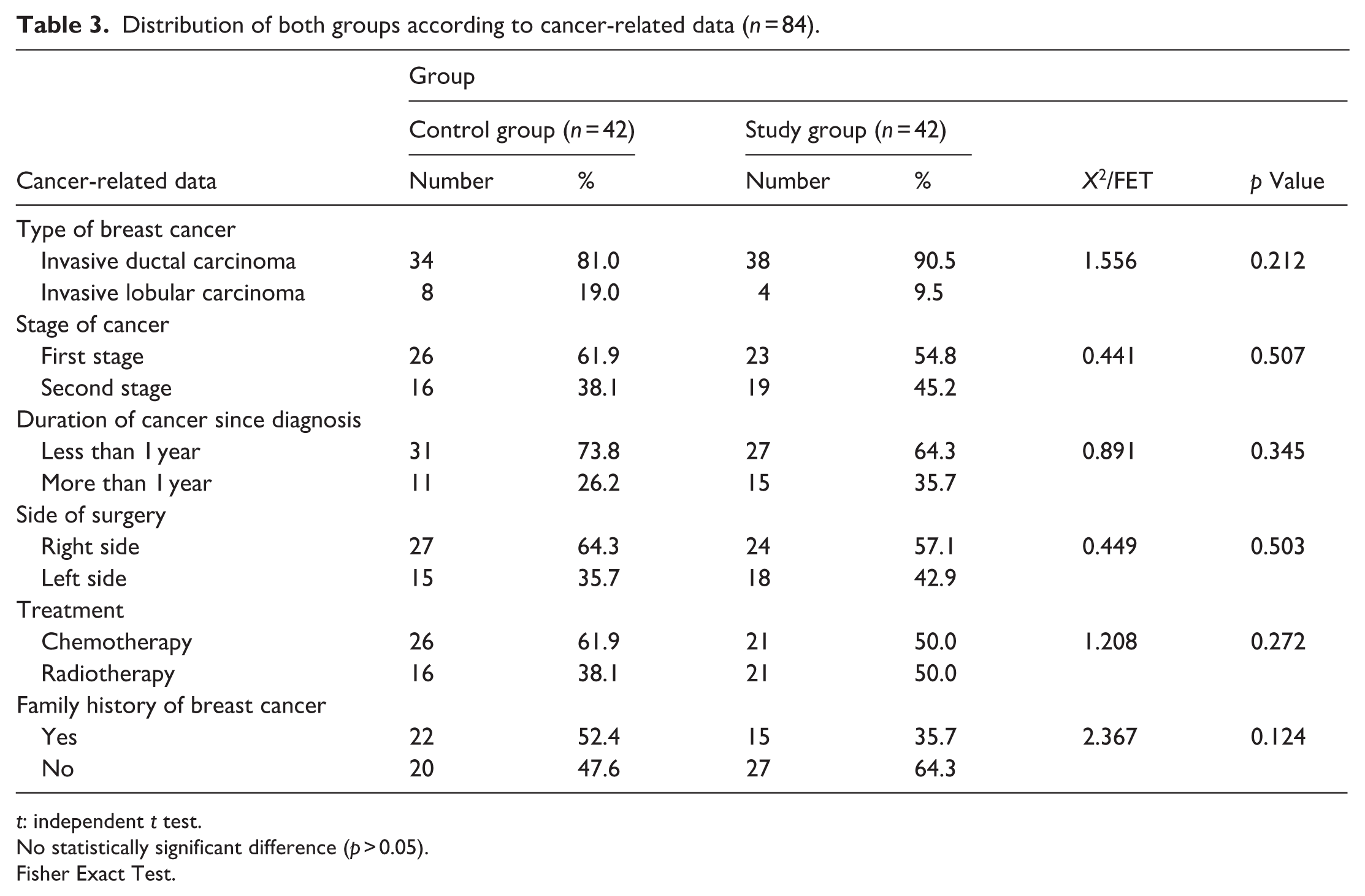
t: independent t test.
No statistically significant difference (p > 0.05).
Fisher Exact Test.
Table 4 illustrates that, during the first week post-surgery, no significant differences were observed between the two groups in any fatigue domain, indicating comparable fatigue levels immediately after mastectomy (all p > 0.05). However, at 6 weeks and 3 months after the intervention, the study group showed significantly lower mean scores in all fatigue domains compared with the control group. The total mean fatigue score was 37.97 ± 5.92 and 39.80 ± 3.12 in the study and control groups, respectively, during the first week (F = 7.793, p = 0.003*, Partial η² = 0.087, 95% CI [−3.33, −0.67]). 29.61 ± 6.07 and 32.83 ± 3.68 after 6 weeks (95% CI [−6.24, −2.35]), and 22.95 ± 2.73 and 25.80 ± 4.83 after 3 months (95% CI [−5.30, −2.46]). The findings indicate a marked and sustained reduction in fatigue levels among women in the study group following the intervention, reflecting its positive effect in alleviating post-mastectomy fatigue.
Comparison of the total mean score of fatigue among women undergoing mastectomy at all measurement times (n = 84).

F: F value from repeated-measures ANOVA; Partial η²: Partial Eta Squared (effect size); 95% CI: 95% confidence interval of the mean difference between groups.
Statistically significant difference (p ⩽ 0.05).
Table 5 presents changes in shoulder pain and disability across three assessment periods for both groups. In the first week after surgery, the two groups show very similar scores. Shoulder pain averaged 40.61 ± 3.03 in the study group and 41.14 ± 3.60 in the control group. While disability scores are 67.66 ± 2.09 in the study group and 68.40 ± 2.55 in the control group. At this stage, no significant differences are noted. By 6 weeks, the study group demonstrates clearer improvement, with pain level decreasing to 34.47 ± 1.51 compared with 35.88 ± 2.80 in the control group, and disability drops to 52.54 ± 6.90 versus 55.83 ± 6.23. These results indicate the presence of significant differences favoring the study group. At 3 months follow-up, the pattern continues. Shoulder pain further declines to 25.11 ± 2.16 in the study group compared with 27.35 ± 5.01 in the control group, and disability becomes 37.76 ± 3.72 versus 41.92 ± 6.00. Significant differences remain evident at this stage as well.
Comparison of the total mean scores of shoulder pain and disability among women undergoing mastectomy at all measurement times (n = 84).

F: F value from repeated-measures ANOVA; Partial η²: Partial Eta Squared (effect size); 95% CI: 95% confidence interval of the mean difference between groups.
Statistically significant difference (p ⩽ 0.05).
Table 6 shows a consistent pattern of improvement in quality-of-life domains among women in the study group compared with those in the control group across all follow-up points. Although they started with very similar scores in the first postoperative week, notable differences emerged as time progressed. By 6 weeks and continuing to the 3-month assessment, the study group reported higher levels of physical, social, emotional, and functional well-being. These differences were statistically significant in most domains, indicating a meaningful advantage for the women who received the intervention. Similar trends appear in the overall quality-of-life score, while the two groups had comparable levels during the first week, the study group showed greater improvement at both 6 weeks and 3 months. At the final follow-up, the total quality of life reached 72.50 ± 5.50 in the study group compared with 65.88 ± 4.83 in the control group, reflecting a clear improvement over time.
Comparison of the total mean score of quality of life among women undergoing mastectomy at all measurement times (n = 84).

F: F value from repeated-measures ANOVA; Partial η²: Partial Eta Squared (effect size); 95% CI: 95% confidence interval of the mean difference between groups.
Statistically significant difference (p ⩽ 0.05).
A highly statistically significant difference (p ⩽ 0.001).
Table 7 shows a significant negative correlation between total quality-of-life scores and total fatigue, shoulder pain, and shoulder disability in both the study and control groups at all measurement times. This means that as fatigue, shoulder pain, and shoulder disability decrease, the overall quality of life improves. The study group showed an incremental increase in the strength of the negative correlation between the two groups over time, particularly at the three-month marker; this result demonstrates the positive impact of the educational support program on reducing symptoms and improving quality of life. While the control group also demonstrated significant correlations over time, they were less pronounced than those observed in the study group. Overall, these results highlight the strong relationship between physical recovery and quality of life among women undergoing mastectomy.
Correlation between total quality-of-life score and total fatigue, total shoulder pain as well as total shoulder disability scores among women undergoing mastectomy at all measurement times (n = 84).

A high statistically significant difference (p ⩽ 0.001).
Discussion
While the core treatment for breast cancer, a mastectomy is a substantial surgical procedure that implies the partial or/whole removal of the breast tissue. A variety of mastectomy procedures, including basic mastectomy, modified radical mastectomy, or skin sparing besides nipple sparing treatments, can be taken out dangling on the severity as well as stage of the disease. Mastectomy is even a physically besides psychologically confronting treatment that has life-threatening postoperative outcomes, although developments in the surgical methods. Pain, diminished arm motion, postoperative fatigue, besides the likelihood of lymphedema are all outcomes of the surgery’s physiological interruption of the muscles, nerves, and lymphatic structures around the chest as well as the axilla. Mastectomy has a significant effect on women’s social and psychological well-being besides the physical challenges. Alterations in body image, depressed self-esteem, as well as rigorous anxiety can totally stem from breast loss. 22
These confronts display the necessity for all-inclusive supportive care programs. Because nurses have the longest and closest contact with patients during the perioperative period, supportive care is very important. They include information on coping mechanisms, emotional support, symptom management techniques, postoperative exercises, and advice on changing one’s lifestyle. To reduce problems and encourage a comprehensive recovery following a mastectomy, it is crucial to incorporate nurse supportive care programs into routine postoperative management. Therefore, this research aimed to evaluate the effect of the educational supportive care program on fatigue, shoulder functional ability, and quality of life among women after mastectomy. 23
Regarding participants’ demographic data, both groups had a similar age distribution, with the majority of participants falling in the 40–49 years category. This similarity indicates the groups were comparable at baseline. Women in this age range often carry significant family and social responsibilities, which may increase the psychological burden after mastectomy and affect their recovery and quality of life. In this context, a supportive educational program may help women better cope with these challenges and adjust to changes in their roles. Hashem et al. 24 in 2020 who reported a similar mean age among women undergoing mastectomy. It is well established that the risk of breast cancer increases with age, particularly after 40 years, which may be related to reproductive and lifestyle factors. However, other studies such as Natarajan et al. 25 in 2023 established that a higher proportion of mastectomy cases in their study were among women aged 55 years and older. These differences may be explained by variations in access to screening and early detection services across different settings.
Also, residence patterns in the current study are fairly balanced, with a slight predominance of rural participants in both groups. This is in accordance with Abdel-Wahab Afifi Araby et al. 26 in 2024 who found a higher proportion of rural women undergoing mastectomy. Conversely, Vangsness et al. 27 in 2025 found that most cases were from urban areas with better access to oncology services. Such differences may be related to variations in health care accessibility and regional population characteristics. The higher representation of rural participants in the current study may reflect the population served by the study setting.
Most participants in the current study had secondary education, and the proportion of participants with higher education is slightly higher in the study group. Higher educational attainment may facilitate understanding and application of educational materials, improving symptom management and self-care strategies, which are important for enhancing functional status and quality of life after mastectomy. This is similar to Abd El Rahman et al. 28 in 2024 who stated that women with secondary education represented the majority of mastectomy patients in their study. Education may influence how women perceive cancer and cope with physical, psychological, and social challenges. The distribution of employment status was similar between the groups, suggesting that occupational demands were unlikely to bias the results. Nonetheless, employed women may benefit more from supportive care interventions that promote energy conservation and gradually resumption of daily activities. These findings are consistent with Atya et al. 29 in 2020, who instituted no statistically significant difference reflecting group homogeneity between the two groups. Overall, the baseline comparability between the two groups suggests that the established supportive care program, rather than demographic differences, is more likely to be responsible for the observed post-intervention gains in functional status and quality of life.
Pertaining to participants’ cancer-related data, the existing research discovered that the majority of participants in both groups were diagnosed with invasive ductal carcinoma, while a small proportion of them had invasive lobular carcinoma. More than half of the participants in both groups were in the first stage, and the duration from the time of diagnosis was less than 1 year for the majority. Early-stage diagnosis is particularly relevant, as it is generally associated with better diagnosis and fewer physical complications, which may facilitate engagement in supportive educational interventions and promote faster recovery of functional abilities. However, women in the early adjustment phase may experience increased psychological distress and uncertainty, potentially affecting quality of life.
This finding matches a study by Hawash 30 in 2022, a study published at Alexandria University found that nearly half of the women examined had stage II breast cancer. While these results differ from those of Abd El Rahman et al. 28 in 2024 who showed that more than half of the post-mastectomy women had cancer for more than a year, and 25% of those women had third-stage breast cancer. These differences may stem from distinctions in the related diagnostic procedures and health care accessibility. Additionally, the cultural attributes between societies, altogether of which assert an influence on initial identification and the start of the treatment. Additionally, variations in the way supportive care is applied, for example, counseling, education, besides follow-up, could influence in what way involved patients are as well as results viewing.
Most surgeries in the current study were performed on the right breast, in addition to parallel proportions of contributors who received chemotherapy as well as radiotherapy, whereas a positive family history of breast cancer was reported in a noticeable portion. These treatments are often associated with discomfort, fatigue, as well as reduced physical functioning, underscoring the importance of supportive care in minimizing side effects and enhancing quality of life. The similarity in surgical site, treatment type, and family history between groups suggests that these factors were unlikely to influence the study outcomes. These results are in harmony with Abdallah Abdel-Mordy et al. 31 in 2021 who indicated that over half of the control group and around two-thirds of the women in the study group had breast cancer in the right breast. In addition, the study’s results support the declaration mentioned by Ahmed Ahmed et al. 32 in 2023 that above two-thirds of the contributors received chemotherapy as well as had a family history of breast cancer.
Pertaining to participants undergoing mastectomy, the current research illustrated that, fatigue levels were similar between the study and control groups during the first postoperative weeks, with no significant differences observed across all fatigue domains. This initial similarity can be reasonably attributed to the acute physiological impact of surgery, including tissue trauma, inflammatory responses, postoperative pain, and anesthesia-related effects, which usually dominate the early recovery phase and limit the immediate influence of educational or supportive interventions. Therefore, the absence of early differences should be interpreted cautiously and doesn’t necessarily indicate a lack of intervention effectiveness.
In contrast, at 6 weeks and 3 months after the intervention, participants in the study group demonstrated lower fatigue levels compared to those in the control group. This pattern suggests a delayed and cumulative effect of the supportive educational program, which may become more apparent as patients move beyond the acute postoperative stage. A possible explanation is that participants gradually adopt self-care practices, energy-conservative strategies, and coping mechanisms introduced during the intervention, alongside ongoing physical recovery and psychological adjustment. These changes may collectively contribute to the observed reduction in fatigue.
From a clinical perspective, reduced fatigue may be associated with improved functional capacity and greater participation in daily activities, which are essential components of recovery after mastectomy. However, this interpretation should be approached with caution, as fatigue is a multifactorial outcome that may also be influenced by factors such as adjuvant therapies, comorbid conditions, and individual psychosocial status, which weren’t fully controlled in the present study. Accordingly, causal inferences cannot be definitively established.
These findings can also be understood within the context of supportive and holistic nursing care approaches, with emphasizes patient empowerment through education, symptoms management, and psychological support across the recovery trajectory. Within this framework, the observed improvements in fatigue may reflect the cumulative benefit of addressing both physical and psychological needs rather than the effect of a single intervention component.
These outcomes are in proportion to research indicating that one of the greatest shared postoperative symptoms between mastectomy women is fatigue that mainly related to surgical trauma, sleep and psychological disorders, besides chemotherapy and radiation therapies.33,34 According to Wang et al. 35 in 2025 and John et al. 36 in 2025; symptom monitoring, psychological support, gradual physical activity, and concluded education, designed supportive care can lessen the strength of fatigue.
Several studies have shown similar tendencies of reducing fatigue over time after supportive interventions, which provides strong support for the current findings. Sharma et al. 37 in 2023 exhibited that planned sessions with stress on care of wound, exercise guidance, energy conservation, and mental guarantee were effective in fatigue reduction following mastectomy. As well, Prieto-Gómez et al. 38 in 2022 detected that prompt motion exercise in combination with educational maintenance significantly heightened physical conditioning as well as diminished the strength of fatigue.
The recent study’s strong correspondence with supporting care trials that comprehensive, nurse provided supportive care plays as a crucial component of postoperative treatment.39–41 Along with Wagner et al. 42 in 2025, and Lirola et al. 43 in 2025, the research group’s persistent reduction in fatigue scores highpoints the prominence of planned supportive care initiatives in enhancing healing, retrieval physical condition, as well as cumulative inclusive quality of life subsequent mastectomy.
The existing outcomes, though, are not constant with the outcomes of further studies. Marco et al. 44 in 2023, as well as Tait et al. 45 in 2018; revealed obstinately extraordinary levels of fatigue and related them to unmanaged shoulder discomfort besides limited arm motion. As these intervention trials were short, non-individualized, or deprived of follow-up support, the absence of planned/or ongoing supportive care can account for these contradictory outcomes. Fatigue trajectories can also be prejudiced by disparities in women’s variables including age, cancer stage, therapy kind, as well as emotional stress. Chemotherapy has been accompanied by insistent fatigue that could be responsible for the lower recovery seen in numerous researches.46,47
Relating to participants undergoing mastectomy, the current research illustrated that shoulder pain and disability levels were similar between the study and control groups during the first postoperative weeks, suggesting comparable early functional impairment. At this instant, pains as well as functional restriction are typically identified by the physical injury from surgery, tissue, and nerve irritation, besides postoperative immobility that is responsible for the absence of substantial group variances.44,48 This is frequently dominated throughout the initial stages of recovery as well as can be ambiguous at any instant, the benefits of instructive treatments.
Nevertheless, by 6 weeks postoperative surgery, the study group displayed stronger enhancement in total shoulder pain besides disability matched with the control group. This tendency was constant at the 3-month follow-up. This pattern suggests a progressive effect of the supportive care program that becomes more apparent over time. A plausible explanation is that participants increasingly adhered to the recommended exercises, activity modification strategies, and pain management techniques introduced during the intervention. In addition, gradual physical recovery combined with improved confidence in movement may have contributed to enhanced shoulder function and reduced discomfort.
From a clinical perspective, improvements in shoulder pain and function are likely to support greater independence and facilitate return to daily activities following mastectomy. However, this interpretation should be approached cautiously, as recovery trajectories may also be influenced by many factors such as, baseline functional status, variation in surgical technique, adjuvant therapies, and individual adherence to prescribed exercises, which weren’t fully controlled in the current study. Consequently, a direct causal relationship cannot be definitively established.
Aforementioned study showing that planned postoperative supportive intervention as exercise training, physical therapy, besides education delivered by nurses, can significantly augment upper limbs function after mastectomy, maintains our outcomes.49,50 From the investigators’ viewpoint, the study group’s superior enhancement can be likewise explicated by primary mobilization, advanced stretching, besides ergonomic physical activity that diminishes stiffness, lessens inflammation, and promotes neurological restoration as declared by Quintero et al. 51 Overall, the existing research highlights how imperative supportive care programs are for promoting recovery after mastectomy. As they combine education, personalized rehabilitation, pain controlling methods, besides enduring follow-up, nurse supportive interventions are predominantly fruitful in helping women recover shoulder movement, reduce pain, and improve functional individuality.52,53
This outcome has been related to Hussein et al. 54 in 2023 who verified a sturdy statistically significant correlation among the study group’s total score before shoulder exercises and their total score subsequent to the exercises as well as through follow-up. Moreover, Ahmed Ahmed et al. 32 in 2022 establish that a nurse-aided home shoulder exercise program effectively escalates shoulder motion besides diminishes discomfort in post-mastectomy women. Such interventions not only hasten physical restorative nonetheless also advance quality of life, lift women’s confidence, as well as diminish long-term handicap associated with post-mastectomy shoulder dysfunction, as verified by the consistent developments perceived at 6 weeks besides 3 months.
Alternatively, particular research has exposed that shoulder function progresses more sluggishly or/ not at altogether later mastectomy, predominantly in associates getting conventional postoperative treatment without modified guidance or planned follow-up.54,55 The variances across trials might be elucidated by variables similar to overdue beginning of physiotherapy, women’s adherence inconsistency, advanced standard pain, or related medication. Additionally, issued outcomes may possibly be wedged by disparities in valuation instruments, social norms adjacent postoperative activity, besides sample features.
Pertaining to participants undergoing mastectomy, the present study found that quality-of-life scores showed a consistent pattern of improvement in the study group across all follow-up periods compared to the control group. During the first postoperative week, both groups reported similar ratings in physical, emotional, social, and functional domains, indicating a comparable immediate impact of surgery. This early similarity can be attributed to the acute physical and psychological effects of mastectomy, including pain, fatigue, stress, and reduced mobility, which are likely to overshadow any short-term effects of supportive intervention. According to Chi et al. 56 in 2025 and Marco et al. 44 in 2023 all patients experience comparable immediate surgical side effects, such as pain, exhaustion, psychological stress, and reduced mobility.
However, women in the study group reported greater levels of functional, emotional, social, and physical health by 6 weeks and up to 3 months, with statistically significant differences in most domains. The educational supportive care program, which offered techniques for symptom management, energy conservation, guided exercise, emotional coping skills, and social support, can mechanistically explain this improvement. These elements probably improved functional independence, decreased shoulder pain and tiredness, and improved psychological adjustment, all of which resulted in better quality-of-life outcomes. These gains are in line with earlier studies showing that organized, supportive care programs improve recovery, lower postoperative complications, and improve several aspects of quality of life following mastectomy.57–59
In essence, from a theoretical standpoint, the findings corroborate the philosophy of support-based and holistic nursing; in that they support the implementation of holistic nursing philosophy for providing both the physical and emotional needs of patients during recovery. The observed improvements in quality of life are due to the cumulative benefit from combining all three elements of a structured nurse-leadership program providing patient education, self-management, and ongoing support; instead of treating each component as an individual entity.
This study supports previous research that supports a structured nurse-led supportive care program as beneficial to improving patient recovery and decreasing postoperative complications, as well as providing multiple aspects of improved quality of life among women who have undergone mastectomy. However, the sustainability of these benefits may also be influenced by individual patients’ factors, including baseline health status, adherence to recommended activities, and exposure to adjuvant therapies, which should be considered when interpreting the findings.
The findings are in agreement with Rastegar et al. 60 who found that the intervention group improved more than the controls both immediately and 3 weeks after counseling in terms of digestive health, physical, psychological, and mental health, skin health, self-care knowledge, sexual health, and general self-care dimensions. Women can regain functional independence, enhance social relationships, and restore emotional equilibrium with the help of individualized education, psychological support, physical rehabilitation supervision, and routine follow-up.52,53
Altogether, the contemporary results climax the serious role that supportive care programs play in promoting an inclusive recovery after mastectomy. These interventions that emphasize physical recovery, pain control, psychological support, besides self-management teaching, not merely hasten enhancements in quality of life but also allow women to realize the problems of postoperative recovery, evade long-term debility, as well as progress overall well-being.53,61
Conversely, certain studies have displayed that women’s quality of life develops more sluggishly after mastectomy.56,62,63 These discrepancies could stem from variants in the length, intensity, timing, besides devotion of the intervention. For instance, research on missing personalized direction, short-term or/ limited supportive interventions, or difficult follow-up often fails to deliver significant advances in the functional, emotional, or social domains. Quality-of-life outcomes are also influenced by patient-related characteristics, including age, comorbidities, type of adjuvant therapy, and baseline psychosocial support. 64 Measures of fatigue, shoulder discomfort, and shoulder impairment were found to be significantly correlated negatively with overall quality-of-life scores in both the study and control groups across all measurement points.
Relating to correlation among total quality-of-life score, total fatigue, total shoulder pain besides total shoulder disability scores between contributors undertaking mastectomy at all measurement times; the existing research displayed a substantial negative correlation among total quality-of-life scores as well as total fatigue, shoulder pain besides shoulder incapacity in both the study as well as control groups at all measurement times. This means that, besides reducing shoulder incapacity, shoulder pain improves the quality of life. In the study group, the forte of negative correlation somewhat amplified over time, particularly later 3 months, representing that the educational supportive program had a progressive influence on plummeting symptoms in addition enlightening quality of life. The control group also showed significant correlations, but the changes were less noticeable compared to the study group. Overall, these results highlight the strong relationship between physical recovery and quality of life among women undergoing mastectomy. These results highlight the crucial connection between holistic well-being and physical recuperation in women after mastectomy.
These findings are in line with numerous studies that highlight how improvements in the physical, emotional, and social aspects of quality of life are directly correlated with decreases in postoperative fatigue, pain, and functional impairment.35,53,65,66 Through hastening recovery, besides augmenting women’s apparent quality of life, educational and nurse-led supportive care initiatives fortify this negative correlation by contributing a planned direction for management, primary rehabilitation, as well as survival strategies.58,67
Overall, the outcomes display how imperative supportive care programs are for enlightening post-mastectomy quality of life as well as physical restoration. Supportive interventions aid women recuperate their individuality, heightening their psychological well-being, and advancing overall postoperative outcomes by tackling fatigue, pain, and functional debility through education, rehabilitation, and enduring follow-up.53,68 Furthermore, Adesina and Olajire 69 in 2020 indicated that exercise plus learning regarding the disease is a supplementary influence that might advance psychological well-being, which sequentially escalates life satisfaction and happiness as well as diminishes pain and fatigue.
Oppositely, certain research has established scarcer relations among physical grievances and quality of life, particularly in cohorts that didn’t obtain planned supportive care interventions.70,71 Dissimilarities in intervention design, such as the extent, strength, and customization of educational or/ rehabilitative programs, may be the reason for these discrepancies. The point at which physical symptoms and the whole quality of life are related can also be prejudiced by women’s individualities.72,73
Limitations
‑ The research was conducted on a slightly limited sample size (84 participants) that might restrict the applicability of the outcomes.
‑ The research was carried out in one health care facility that could restrict the generalizability of the results to women having mastectomies in other health care areas.
‑ Furthermore, participants were enrolled consecutively and allocated sequentially rather than through randomization. This may introduce selection and temporal bias besides, and it limits the ability to draw definitive causal conclusions regarding the efficiency of the intervention.
‑ The lack of blinding may have introduced measurement and performance bias.
‑ The relatively short follow-up period limits the assessment of long-term outcomes.
‑ Despite the positive outcomes of the supportive care program, the reliance on self-reported scales for fatigue and quality of life might introduce the risk of response bias and subjectivity. Finally, confounding factors such as the participants’ nutritional status, and psychological support from their families weren’t strictly controlled, which might have influenced the study outcomes.
Conclusion
The educational supportive care program was associated with positive outcomes in women who had undergone a mastectomy. Although both groups were comparable in the first week post-mastectomy, women in the intervention group experienced reductions in fatigue level, shoulder pain, and disability, and they also showed improvements in their quality of life at both 6 weeks and 3 months after receiving the intervention. A significant negative correlation was observed between total quality-of-life scores and total fatigue, shoulder pain, and shoulder disability, indicating that symptom reduction may be associated with better quality of life. These findings suggest that an educational supportive care program could be a beneficial component of post-mastectomy care, while further randomized studies are needed to confirm its effectiveness.
Recommendations
- In order to enhance women’s functional status and their quality-of-life post-mastectomy, educational supportive care should be integrated into routine care.
- Continuous educational sessions should be provided for women post-mastectomy, focusing on arm exercises, eating healthy, caring for wounds, sleeping habits, and managing emotional distress.
- It is important to provide psychological support and intervention activities to help women regain their strength and adapt well after a mastectomy.
- Repeating the study with a broader and more varied group of participants is intended to make the findings more widely applicable and enhance their relevance for a diverse population.
Footnotes
Ethical considerations
The Scientific and Ethical Research Committee at Tanta University, Faculty of Nursing, was addressed and approved. Procedures were strictly aligned with applicable standards and laws, including the Declaration of Helsinki.
Consent to participate
All women who participated in this study gave their written consent to participate in the study, and confidentiality was guaranteed. Procedures were strictly aligned with applicable standards and laws, including the Declaration of Helsinki.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current clinical trial are not publicly available as they have not been published, but can be gained from the corresponding author* upon reasonable request.