
Abstract
Background
Carers are individuals who provide unpaid care to family members and friends with disabilities, medical conditions, mental illness, or who are frail and aged. The contribution of carers to the Australian health, aged care, disability, and social care systems is significant. However, they face high levels of emotional, social, physical, and financial burdens. The Australian Government has recently introduced policy reforms to improve recognition of carers. However, there is limited evidence on research priorities to facilitate the translation of policies into practice.
Objective
To involve Australian stakeholders to a) identify evidence gaps and research needs; and b) set research priorities for carers within the context of ageing, palliative care and end of life.
Design
Stakeholder consultation study for research priority setting.
Methods
Australian stakeholders with expertise in areas related to carers, aged care, and palliative care were engaged through an online survey, a research roundtable and a focus group to discuss research priorities for carers. The survey qualitative responses, notes from the roundtable, and focus group transcript have been summarised and analysed thematically, using NVivo 14 qualitative software.
Results
Two main considerations as found from the study are ‘what to research’ and ‘how to research’ to improve recognition and support of carers in Australia. Research priorities identified include recognition and early identification of carers, timely and equitable access to support services, helping carers navigate services, support during the transition of care, post caring, including grief and bereavement support, evaluation of existing services, and carer self-care and wellbeing. Participants commented on the importance of research that engages carers meaningfully, respectfully, and in a timely and flexible manner to ensure maximum impact.
Conclusion
This study guides the design of carer-centred research to facilitate the translation of carer policies into practice. It also assists in evaluating the effectiveness, cost-effectiveness and sustainability of existing and new support services.
Plain language summary
Unpaid carers are individuals who help a family member or friend with a disability, medical condition, including terminal or chronic illness, mental illness, or are frail and aged. In Australia, carers play a critical role in providing care, and they make significant contributions to health, care and social care services. There are many programs to support carers, but carers still have problems accessing the right support services at the right time. They also lack the support they need to maintain their own health and wellbeing. To improve carer policy, it is important to look at research that helps put policy into practice in real-life situations. This study, aimed to give participants, including carers, a voice to help identify and shape future research that could make a difference in the lives of carers. The main areas of research priorities identified in the study are recognition and early identification of carers, timely and equal access to support services, helping carers to navigate support services, carer support during the transition of care, post caring, including grief and bereavement support, evaluation of existing support services, and carer self-care and wellbeing. Carers are diverse, and it is important that support services are culturally sensitive and support the cultural and individual needs of carers. It is also important that carers are involved in research design, implementation and evaluation. The study will inform future research and strengthen research that impacts carers.
Keywords
Background
‘Carer’ is an umbrella term used for individuals who provide unpaid care and support to family members and friends who have a disability, medical condition, including terminal or chronic illness, mental illness, or are frail and aged. 1 Unpaid carers are distinguished from paid care workers who are trained direct support staff with employment contracts, and unpaid volunteers who provide unpaid support through formal community or charitable organisations with activities structured within the organisational framework, and do not have a personal relationship with the recipient of care. 1 The terms “unpaid” or “informal carer” are commonly used in Australia. However, other terms such as caregiver, primary carer, family carer are also used in different settings. In this paper, the term ‘carer’ refers to an unpaid carer within a care relationship, such as a family member or friend, who provides regular, ongoing care and support to someone who needs help with daily living. 1
In Australia, carers make up nearly 12% of the population (3 million), with females more likely to be carers than males (12.8% vs 11.1%) and an average age of 50 years for a carer. 2 The contribution of carers to health, aged and social care systems is substantial. An examination of the economic value of carers in 2020 demonstrated that, based on average hourly replacement cost, the total cost of replacing all informal care provided by carers in Australia was almost $78 billion. 3 While communities and systems benefit from their contribution, carers face high levels of emotional, social, physical, and financial burdens. 4 According to the 2025 Carer Wellbeing Survey in Australia, over 60% of carers reported low wellbeing, over one third experienced high psychosocial distress, and 1 in 3 former carers reported that they would have been able to continue their caring role if more formal support was available to them. 5 Carers report their ability to work may be limited due to caring responsibilities, and feel emotionally overwhelmed and often unprepared for end-of-life care. 4 These pressures are intensified in regional areas where support services are less accessible. 6 Furthermore, carers of older adults, individuals in need of palliative care, and those nearing the end of life may encounter additional, role-specific challenges due to the prospect of facing the death of the person they care for.
In response to a growing understanding of the contributions made by, and issues being faced by carers, the Australian Government has recently introduced major policy reforms. In 2023, the Australian House of Representatives carried out an inquiry into the recognition of carers. The National Carer Recognition Act 2010 underwent a review through a consultative process that included 143 submissions from various organisations and individuals, as well as eight public hearings. The final report of the Act review was published in 2024. It contained 22 recommendations, including improved recognition and support for carers, community and health system awareness, and professional training. 1 The inquiry report is in the process of being tabled for House of Representatives. The Australian National Carer Strategy 2024-2034, and the Action Plans 2024-2027 were subsequently released, outlining key priority areas, action plans, and gaps in knowledge and evidence.7,8 The first action plan will be evaluated and followed by a second 3-year action plan throughout the timeframe of the Strategy. The Strategy and Action Plans include and prioritise recommendations from the Act review. Furthermore, some Australian jurisdictions have also undergone a similar process of reviewing their carer policies and strategic plans.9–12 For example, the South Australian Carers Recognition Act 2025, which is passed by both Houses of Parliament in November 2025, expanded the definition of carer to reflect the evolving nature of care and the diversity of carers, and explicitly acknowledged the different caring relationships. It has also been recognised that the nature of caring roles may or may not be ongoing, and the continued role of carers when the older people they support move into residential aged care. 13
These policy and legislative reforms call for greater focus on supporting carers, yet the evidence is limited on what works well to support them and why. Knowledge gaps in areas related to the recognition and support of carers can limit the translation of policy into action. In particular, these gaps affect the ability to: • design evidence-based interventions and support services • engage with carers to codesign support services • demonstrate the effectiveness of support services and their value for money • assess sustainability, scalability, and adaptability to meet the needs of a diverse group of carers in Australia.14,15
To address knowledge gaps and generate evidence that facilitates the translation of policy into practice, this project aimed to involve stakeholders and experts in Australia to a) identify areas of evidence gaps and research needs; and b) set research priorities for carers within the context of ageing, palliative care and end of life. This is a very timely opportunity for collaborative research that focuses on implementation, knowledge translation, and policy alignment to inform plans to improve the recognition and support of carers in Australia. Through stakeholder involvement, particularly carers and carer advocacy organisations, the study aims to develop research questions and identify priorities that are more relevant to carers. This will promote early engagement, foster relationships that support ongoing collaboration in future stages, such as research design and implementation, ensures that future research reflects the real-world needs of carers, and create transparency and consistency in carer involvement in research. 16 It will also inform researchers, research funders, and the government to fund, design and implement research that facilitates the translation of policy priorities into practice.
Methods
This study employed a stakeholder consultation process to identify research priorities most important to unpaid carers in Australia. A consultative process was designed and conducted to engage Australian stakeholders with expertise in areas related to carers in the context of aged care, and palliative care and end of life. Given the focus of study, we excluded stakeholders with expertise in broader carers groups such as disability. The project was auspiced by the Research Centre for Palliative Care, Death and Dying, Flinders University consisting of a team of experienced palliative and social care researchers, facilitating the identification and engagement of a diverse group of stakeholders from across Australia. Participants included researchers (n=28), representatives from carer advocacy organisations and peak bodies (n=11), experts in policy and planning (n=6), two of whom were carers, and carers, either former or current (n=6). We used purposeful sampling strategy to identify key stakeholders and experts in Australia. These included a comprehensive search of the lead researchers and research projects funded by the two major Australian research funding bodies (National Health and Medical Research Council and Australian Research Council) in the past 10 years, academic publications, carer advocacy organisations and carer peak bodies in Australia, advisory group members of the national and jurisdictional carers policy development committees, and consumers/carers advisory committees. The authors’ professional networks were also utilised to identify experts. This resulted in a list of 51 individuals with expertise in areas of caring, carer advocacy and policy, ageing, and palliative care. Identified experts were invited in the following stakeholders’ engagement activities:
Online survey
An online survey was designed by the first and last authors using the Qualtrics survey platform (March 2025), and the survey link was emailed to 51 identified experts. The survey broadly followed the principles of the James Lind Alliance (JLA) priority setting activity. 17 Participants were asked to reflect on their personal and professional experiences to propose research questions that can address 1) recognition and identification of carers; 2) support systems and services for carers and issues around system navigation and 3) physical and mental health and wellbeing of carers. These comments were provided through open-ended questions. The survey included two quantitative questions asking participants to rate eight broad areas, as identified in the Australian National Carers Strategy and National Carer Recognition Act 2010 review report, 1 for further development and research, and to rank their top 3 areas of research interest. Lastly, participants were asked to comment on how the research community can best engage meaningfully with carers in setting priorities and implementing research.
Research roundtable
A research roundtable (April 2025) provided a focused opportunity to further investigate and challenge research priorities and key considerations in setting research priorities for carers. An invitation to participate was sent to the 51 identified stakeholders, and twenty-three people from different participant groups accepted to attend. The roundtable was organised in the format of panel discussions, small group conversations, and plenary question-and-answer sessions, offering participants opportunities to provide feedback, reflect on their experiences, share insights, and establish connections. Carers and representatives of carer advocacy organisations led the discussions in the panel, which was facilitated by author SJ. Holding the panel discussion at the beginning of the roundtable and discussing the importance of carers’ narratives and voices in research shaped further discussions at each table. At least one carer was assigned to each table to contribute to the small group discussions. We also shared with participants proposed or in progress work identified by the research team SJ, OO and JT. These include an environmental scan of carer initiatives in Australia, a review of Australian carer policies, and a scoping review of international literature on carer support programs.
Online focus group
Following the roundtable, we conducted an online focus group (June 2025) to engage with those who were unable to attend the research roundtable in person. Five people participated, including one carer, one researcher, one health practitioner, a representative from a carer advocacy organisation and a rural health expert. The focus group was facilitated in a similar but shorter format to the roundtable. Participants shared their visions and views on research priority areas and how collaborative research could be actioned.
Carers with lived experience were reimbursed for their time participating in the above activities.
Analysis
A descriptive analysis of survey questions on rating and ranking areas of priority action was conducted. Qualitative responses to the survey’s open-ended questions were transferred into NVivo 14 software, coded and analysed thematically to extract meaningful insights into stakeholders’ opinions about carer research (Supplement file). 18 Members of the research team took detailed notes on small group discussions during the roundtable, which were summarised and categorised by the first author for review and analysis. Online focus groups were recorded, transcribed and reviewed by the first author to identify priority areas as stated by participants. The initial draft of findings was shared with participants, and their feedback was incorporated. Many themes overlapped across the above methods, which are collated and presented below. Participants’ rating of the research priorities and policy alignment visualised, using a descriptive chart.
Reporting guideline for priority setting of health research (REPRISE) were followed to present the study. 19 We undertook several steps to ensure study rigour and trustworthiness, including developing the survey questions and roundtable discussion points based on a review of the most recent carer policies in Australia and discussion within the study team. Ethical considerations, including the ethics approval process, ensured the study’s credibility. We regularly discussed findings in internal team meetings and sought feedback from the study participants to confirm the accuracy of our interpretations.
Results
Of 51 experts invited, twenty-six (50%) completed the online survey, including 14 researchers, 4 representatives from carer advocacy organisations and peak bodies, 6 carers and 2 with policy expertise. Twenty-three individuals, including 4 carers, attended the research roundtable, and 5 individuals participated in the online focus group. Stakeholders commented on research priorities and policy alignment, and emphasised key considerations to ensure carer research is meaningful, participatory and impactful. Three carers, with one also representing a carer advocacy organisation (co-authors of this paper), assisted in interpreting the findings and recommendations.
Illustrative quotes for the key themes.
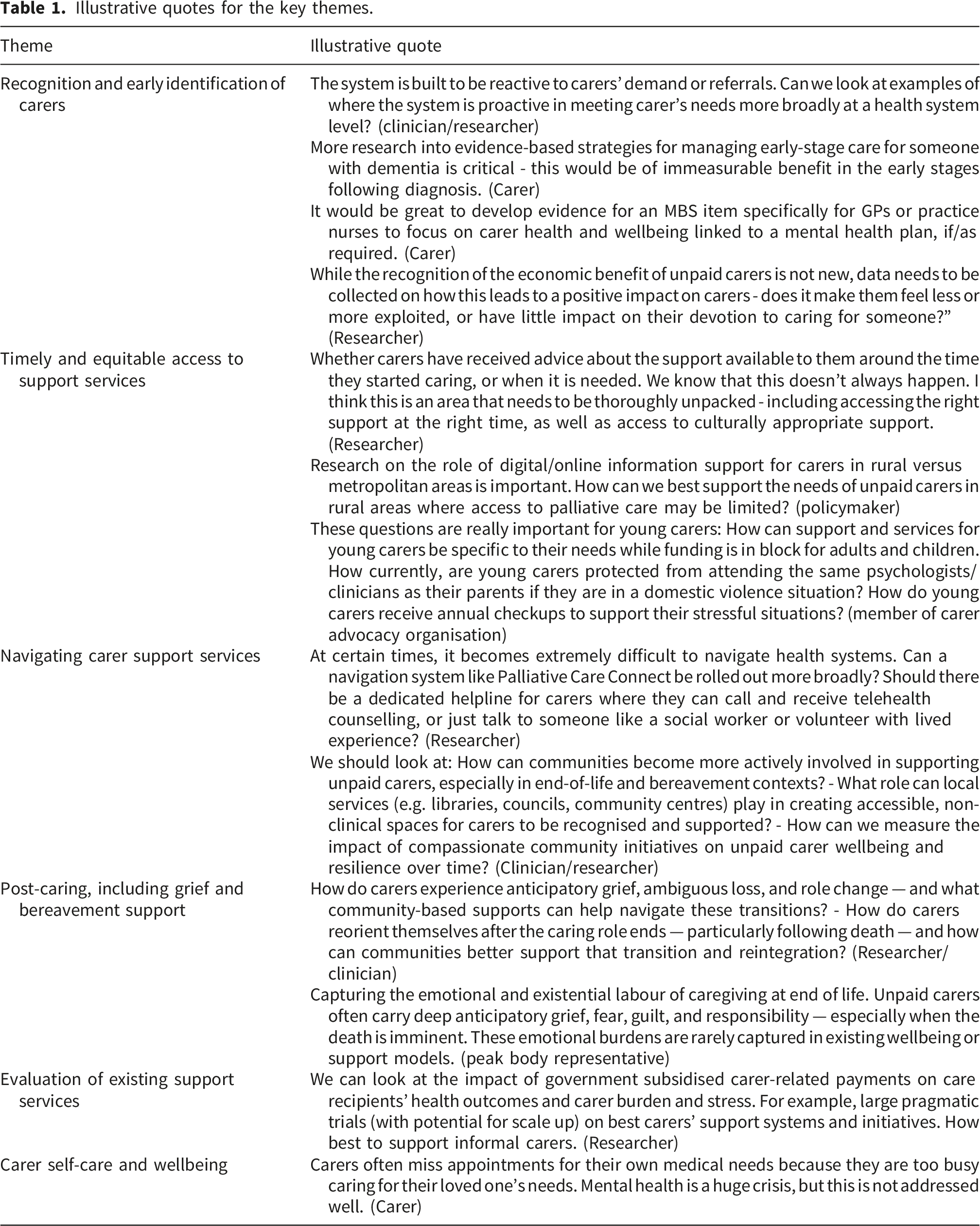
Recognition and early identification of carers
The importance of early identification of carers was frequently noted in both the survey and roundtable/focus group, which is a core element of the National Carer Strategy. 8 Given that carers often do not self-identify, especially when care is provided within a family relationship, systems and government agencies need to be more proactive in early assessment and identification of carers, and in providing timely support and referrals to prevent poor health, financial, and educational outcomes for different groups of carers.
Broader community awareness of the role and contribution of carers was also highlighted. Caring for people with dementia was particularly highlighted as challenging. In these situations, early identification is critical to ensure carers can access the available support services they need.
Healthcare professionals were found to be poorly supported and equipped with the necessary knowledge and tools to identify and recognise carers, which was noted as a major gap. It was identified that research with carers as co-investigators can help address this gap by co-designing evidence-based tools, resources, and training materials to assess carers’ needs and develop ways to address them. Diversity of carers means there is a need to assess and identify specific additional needs of disadvantaged carer groups specified in the National Carers Strategy, such as Veterans, young carers, culturally and linguistically diverse (CALD) carers, LGBTI+ and First Nations carers. Examples include language-accessible and culturally safe services for CALD and Aboriginal communities, transport and digital inclusion for carers living in rural and regional areas, flexible employment arrangements for working carers, and educational support for young carers.
Workplaces that employ working carers were highlighted as critical settings that require greater attention in identifying and recognising carers to ensure they receive the support they need. This includes transparent processes and human resource procedures (e.g., flexible work and leave arrangements). Furthermore, the impact of caring roles on carers’ employment, professional development and education, financial security, and their experience of workplace discrimination, particularly for carers working casually, who are more likely to be female, was raised as areas requiring further attention, evidence, and research.
Despite evidence on the economic and social value of carers, survey and roundtable participants stated that research on translating the evidence into practical strategies and mechanisms to impact carers’ lives is scarce. Research to demonstrate how specific interventions may save costs to individuals and the health or care systems can strengthen policy development and facilitate practice change to improve support for carers.
Timely and equitable access to support services
As with early identification, participants emphasised the importance of early access to services to support their own wellbeing and/or the person they care for. A range of factors affecting access and utilisation of support services was noted, including gender-related issues, culture, and location. Diversity of carers (e.g., those living in rural and regional areas, male carers, young carers, carers from culturally diverse communities, First Nation and LGBTI+ carers), nature of their caring roles (e.g., multiple carers caring for one individual or one carer providing care to multiple people and carers providing care for many years or throughout their life), as well as the needs of the person they care for means that support services must be adaptable to meet specific needs of carers across diverse support needs.
Research to examine caring journeys before and after the death of the person they care for was identified by participants as essential. Another important area was the role of non-clinical professionals, such as death doulas, in enhancing and complementing formal carer support systems, particularly through emotional and spiritual support.
Navigating carer support services
Challenges in navigating the complex support services across multiple sectors, e.g., health, aged care, disability, and the different funding and service models provided across federal and state/territory systems, were frequently identified as requiring further research. The navigation challenge is time-consuming and much more complex and prominent for end-of-life carers who are time-poor and highly distressed. Integration of current service navigation models, examination and comparison of different modes of communication (in-person versus online/digital platforms) and analysis of referral pathways and their benefits are examples of research suggested by participants.
Community support network models, such as compassionate communities, where communities are supported and mobilised to share responsibilities in supporting carers to navigate and access care systems 20 were suggested as an area requiring further research. This includes the involvement of the whole community and public health approaches to increase knowledge about carers, the caring relationship, and the contribution carers make to society, as well as ways community networks can enhance carer support during their caring roles, and support for grief and bereavement. Exploring the role that local services (e.g., libraries, local councils, community centres, schools) play in creating accessible, non-clinical spaces where carers can be recognised and supported is essential.
Carer support during the transition of care
Carers experience many transitions during their journey, e.g., from occasional to full-time, or vice versa, from being a partner to a carer, and whilst the person they care for is transferred from home to hospital to aged care, or, in the case of disability, from home to disability accommodation services. For many, these transitions that led them to become carers may be traumatic.
Small-group discussions during the roundtable particularly highlighted the importance of recognising and responding to carers’ needs at these points of transition. Research is scarce in identifying the range and nature of support offered to carers during and after care transitions. These may include effective strategies and mechanisms to support carers in managing their grief and emotional challenges during transition; carer-staff partnership; inclusion of carers in care planning and shared decision-making; and aged care staff knowledge and skills in communicating with and supporting carers.
Post-caring, including grief and bereavement support
Most support services for carers focus on current carers. Those providing care for older adults, people in need of palliative care and those nearing the end of life are more likely to experience the death of the person they care for. However, post-caring support, including grief and bereavement, is usually overlooked in information sharing, service provision and research. Research gaps, as highlighted by stakeholders, include: • an examination of the coping mechanisms of carers during grief and bereavement, • the psychological impact, • social support, • financial assistance, and • employment after the caring phase.
Research on death literacy was noted as particularly important for end-of-life carers, enabling them to navigate the complexities of death systems, understand the end-of-life options available, make informed decisions, and address the practicalities surrounding death and dying.
Evaluation of existing support services
Research should include a realist evaluation of the impact, adoptability, acceptability and sustainability of existing support services. This will help to examine what works and what does not, what are the effects of support services (health and wellbeing outcomes for both carers and the person they care for), how the services can be adjusted to maximise impact, how the services should be tailored to meet the needs of different carer groups, and what factors influence the sustainability and scalability of the existing services. Developing monitoring and evaluation frameworks, including evidence-based quality indicators for measuring program outcomes felt to be essential. The inclusion of carers’ voices and perspectives in research design and service evaluation through the collection and analysis of carers’ narratives was noted as particularly important.
Carer self-care and wellbeing
Caring for those in need of palliative care and nearing the end of life can be overwhelming due to the intensity of care and time needed by carers, with a significant impact on their physical and mental health and wellbeing. 5 Furthermore, with population ageing, those who provide care to people with terminal illness and older adults are more likely to be ageing too. Furthermore, young carers supporting parents/grandparents across a wide range of caring needs face emotional and mental health issues over time. Carers’ self-care was a cross-cutting theme across all methods used in our research priority setting process. Participants emphasised the importance of research that focuses on improving carers’ physical and mental health and wellbeing. Examples include factors impacting carers’ self-care and help-seeking behaviour, as well as socio-cultural factors and perceived expectations that may hinder self-referral or limit acceptance of support. Research to better understand carers’ views on self-care was suggested, including co-designed research and the collection of carers’ stories.
Moreover, research on the short- and long-term impacts of carers’ ill health on their caring relationships, as well as the health outcomes of the person they care for, is scarce. There were also comments that caring can be rewarding, with some positive impacts on carers; nevertheless, this does not change their need for support and recognition. This area warrants further study and could be used to develop coping strategies and interventions to support carers.
The importance of non-clinical strategies to support carers’ health and wellbeing (e.g., through mindfulness, sound therapy, counselling) and ways to strengthen their roles was highlighted. Research on the impact of social networks, peer support and the support provided by non-clinical paid support workers was highly recommended.
Research-policy alignment
Survey participants were offered the opportunity to rate eight broad areas of priority for action that emerged from a review of recent Australian carer policies (Figure 1). All survey participants responded to this rating question. The three areas rated high in priority are: 1) improving carer psychological, physical and social wellbeing; 2) improving carer recognition, including their economic values, across departments and integrated across federal and state jurisdictions and in the general community; and 3) improving system navigation and timely access to carer support. Areas ranked high support areas of priority discussed in the roundtable and focus group that may benefit from research if policy priorities are to be translated into feasible, adoptable, and sustainable actions and practices. General areas of policy priority.
Consumer and carers’ engagement in research
In addition to research priorities, both roundtable/focus group and survey participants commented on the importance of, and enablers and barriers to, participatory research and carer-research partnership (online survey included one open-ended question on how best to engage carers in developing a research agenda – Supplementary file). Early and ongoing engagement with carers in the research process, allocating sufficient time to build relationships and trust, and engaging with community leaders, carer advocacy organisations, and carer peak bodies were particularly highlighted. Participants stressed the need for an appropriate mode of communication, including culturally sensitive and tailored communication appropriate to various cohorts of carers.
Participants noted the need for flexibility to allow carers to adjust the nature and level of their involvement as their circumstances change. Appropriate compensation and reimbursement for carers’ time and contribution to research were also emphasised.
There was a consensus that both researchers and carers require training to ensure meaningful dialogue and engagement. For carers, training should be provided in a format that is understandable and meets their needs, covering areas such as research processes, ethics, and co-authorship. Researchers must also possess effective human communication skills, cultural awareness, and the ability to navigate different perspectives and potential disputes between researchers and carers.
Discussion
To the authors’ knowledge, this is the first research priority-setting exercise in Australia concerning carers to have been conducted through multiple consultation processes, and in collaboration with stakeholders, including policymakers, carer advocacy organisations, carer peak bodies, researchers, and carers.
Two main considerations, as identified through our consultative approach, are ‘what to research’ and ‘how to research’ to improve carer recognition and support in Australia. The former was related to evidence gaps, research-policy alignment and areas of research importance suggested by stakeholders. The latter concerned the ways research should be conducted to engage carers meaningfully, respectfully, and in a timely and flexible manner, to achieve maximum impact. These findings are relevant to other countries with an interest in carer support.
In general, the research priorities were broad, covering clinical assessment of carers’ health, transition points in carers’ journeys, post-caring, and more public health strategies to support carers. Carers move across various care settings, and therefore, research to inform policies and support services should consider the intersection between health, aged care, disability, and community care settings; however, they are largely under-represented in research, and in process and outcome evaluation measures. 21 Furthermore, carers require skills and support in their caring role, as well as personal skills to contribute to society, and support to maintain their own health and wellbeing.
Generating evidence and developing tools to improve health and care professionals’ knowledge and skills in early identification of carers and supporting them to navigate the system to fulfil their caring role is important. A more holistic approach should be taken to identify and address macro-level factors, with health and care systems focusing on patient-centred care and tending to overlook carers as partners in care. This can be due to time constraints, cost, and a system culture that discourages health and care professionals from recognising and supporting carers. Some tools have already been developed to support health professionals in recognising carers. These tools and frameworks can be reviewed and adapted for wider use in different settings. For example, the National Safety and Quality Health Service Standards promote carers’ inclusion by identifying carers, involving them in care planning and decision-making, and providing research to ensure carers’ needs are integrated into healthcare systems. 22 The South Australian Government has developed a Partnering with Carers Policy to set out mandatory requirements to support carers in public healthcare systems. 23 In Queensland, a tool has been developed to guide health professionals in working with carers, family and kin. 24 There is also a Carer Charter in South Australia that values carer choice, health and wellbeing and their right to be supported, enjoy life and contribute to society. 25
Our research priority setting exercise highlights the need to shift focus from research that solely examines carers’ problems and barriers to more participatory research projects that co-design, tailor, test, and evaluate carers’ support interventions and outcomes, and to those that focus on carers as the primary target population rather than secondary to the person that they care for. There is great potential to advance carer-centred research that requires stronger engagement with carers. This is also important as carers (especially those who care for an elderly spouse) are ageing themselves and face their own health challenges in addition to the person they care for, or young carers who are likely to face additional problems due to lost opportunities and continued poor mental health.
Carers are diverse, and this project focused on carers of older adults, those in need of palliative care or approaching the end of life, who are more likely to experience grief and bereavement prior to and following the death of the person they care for. Evidence suggests gaps in the factual and practical knowledge of carers around death and dying and their access to help. 26 Research to improve carers’ death literacy, as well as post-caring services, including psychological support for bereavement, return to employment, and social life, was identified as a priority. Given the recent carer policy reforms in Australia, there was a consensus that research should align with policy priorities and be conducted in partnership with policy stakeholders to facilitate the translation of policies into actionable strategies and initiatives.
This study reaffirms the importance of consumer and carer engagement in research, building their trust and confidence in research, and conducting research sensitively, safely, and flexibly to meet carers’ needs and preferences. This will help researchers to identify carer priorities and ensure the research outcomes are relevant and impactful. Increasingly, research funding bodies, government agencies and research institutions require carer involvement in research. 27 This requires researchers to develop a communication plan, consider support and training, and prepare budgets and processes to recognise carers’ contributions to research, provide payments, and ensure timely feedback and reporting.
Strengths and limitations
The priority setting process was guided by the James Lind Alliance to ensure research priorities are developed using a transparent process. 17 The process and findings were also informed by other preliminary works in progress by the first and last authors to ensure alignment with the Australian policy and practice context.
A wide range of stakeholders participated in various activities (an online survey, a research roundtable, and a focus group). This included carers whose insights were invaluable for a comprehensive understanding of ‘what’ and ‘how’ in designing and implementing research with carers. The process laid the groundwork for establishing a collaborative research team. 28
The study has some limitations. The online survey mainly included broad, open-ended questions about what is important in carers’ research, which were discussed within the internal team but were not pilot tested with an external sample. Considerations should be given to the representativeness of participants. Given the diversity and time constraints of current carers, the total number of 6 carers, of whom 5 have been past carers, may not represent the broader carer groups, for example, end-of-life carers, young carers, those from culturally and linguistically diverse backgrounds, and First Nation carers. This may affect the suggested research priorities. Nevertheless, other participants with research and clinical roles may have had experience as carers, but this has not been explored or recorded. Limited engagement with policymakers and research funders in the priority setting activities was another limitation. 29 Their engagement is pivotal in the priority setting process, along with future support and investment.
There is also a limitation about the optimal consensus development methods used in this study. Among the three approaches to elicit stakeholders’ research priorities (identification, prioritisation, consensus finding), 29 our study mainly used identification (nominating research needs) and prioritisation approaches (rating and ranking priorities) rather than reaching a final agreement on the final set of research priorities. Deliberative approaches, such as stakeholder nomination and further discussion of their priorities, and other consensus-based methodologies, such as Delphi, should be considered to reach consensus on research priorities for carers.
The research priority setting exercise is an important first step that is strengthened by other preliminary studies being undertaken by our research team including an environmental scan of carer support initiatives in Australia, a review of carer policies and a review of international literature on carer support and services. Collectively, these activities will provide valuable insight into developing a collaborative research plan and co-designing tools and interventions to support the carer recognition and support agenda moving forward in Australia and other similar countries.
Conclusions
There is an urgent need to improve the recognition and support of carers at the policy and practice levels. Research provides evidence that informs and facilitates the translation of policies into practice. Researchers play a critical role in generating evidence and tools to support this translation and to evaluate the effectiveness, cost-effectiveness, and sustainability of such interventions. Given the increasing demand and reliance on carers to assist in care provision, and scarcity of resources, a systematic approach to identify research priorities and consider ways to involve and engage carers in the process is essential to enhance impact and efficiency. Addressing these research priorities will require a commitment from research funding bodies, federal and state governments, professional bodies, and carer advocacy organisations to invest in, implement, and monitor progress towards improved recognition and support for carers in Australia.
Supplemental material
Supplemental material - Research priority setting for unpaid carers of older adults, patients with palliative care needs and at the end of life in Australia
Supplemental material for Research priority setting for unpaid carers of older adults, patients with palliative care needs and at the end of life in Australia by Sara Javanparast, Philip Martin, Annie Dullow, Allison Willis, Oluwatomilayo Omoya, Jennifer Tieman in Palliative Care and Social Practice
Supplemental material
Supplemental material - Research priority setting for unpaid carers of older adults, patients with palliative care needs and at the end of life in Australia
Supplemental material for Research priority setting for unpaid carers of older adults, patients with palliative care needs and at the end of life in Australia by Sara Javanparast, Philip Martin, Annie Dullow, Allison Willis, Oluwatomilayo Omoya, Jennifer Tieman in Palliative Care and Social Practice
Supplemental material
Supplemental material - Research priority setting for unpaid carers of older adults, patients with palliative care needs and at the end of life in Australia
Supplemental material for Research priority setting for unpaid carers of older adults, patients with palliative care needs and at the end of life in Australia by Sara Javanparast, Philip Martin, Annie Dullow, Allison Willis, Oluwatomilayo Omoya, Jennifer Tieman in Palliative Care and Social Practice
Footnotes
Acknowledgements
We acknowledge participants who contributed to the consultation events, including the online survey, research roundtable and online focus group and shared their perspectives and experiences. We particularly acknowledge the contributions of carers who generously shared their stories and experiences with us, and their willingness to continue supporting the team in future research.
Ethical considerations
Ethics approval was granted by Flinders University Human Research Ethics Committee (ID 8296) for the engagement activities undertaken in this study. All participants, including carers, were provided with an information sheet detailing the activity, the benefits and potential risks of their involvement, the measures undertaken to protect the privacy and confidentiality of data, recognition of participants’ contributions, and their withdrawal rights. All activities were conducted in line with the ethical principles of the Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from participants prior to the roundtable and focus group. Survey participants were required to read the information and provide online consent (by checking the consent statement box) before proceeding to the survey questions.
Consent for publication
All participants were informed that the results of the research priority setting activities would be published. Data included in the manuscript is aggregated and deidentified, and written consent was not obtained from individual participants for publication.
Authors’ contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Research Centre for Palliative Care, Death and Dying.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data generated from this study (online survey data, notes from the roundtable, transcription of the focus group) are not publicly available but can be made available upon reasonable request to the first author (SJ).
Supplemental material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.