
Abstract
Background
The disease burden of malignant brain tumours poses significant challenges to both patients and their family caregivers. Even years post-bereavement, neuro-oncology caregivers can suffer serious and long-lasting adverse outcomes. A previous quantitative survey (reported separately) highlighted significant challenges experienced by bereaved neuro-oncology caregivers. This current work explored these issues further through focus groups.
Objective
To identify opportunities to enhance support, we investigated caregiver experiences during the patient’s end-of-life phase, the dying process, and post-bereavement outcomes.
Design
Focus groups as a component of a sequential mixed-methods study designed together with bereaved caregivers.
Methods
We performed online focus groups covering the end-of-life phase, the period surrounding the patient’s death, and their post-bereavement outcomes. Sampled from survey respondents, caregivers who were ≥6 months post-bereavement were invited to take part in online focus groups. Following audio transcription, data were analysed using reflexive thematic analysis.
Results
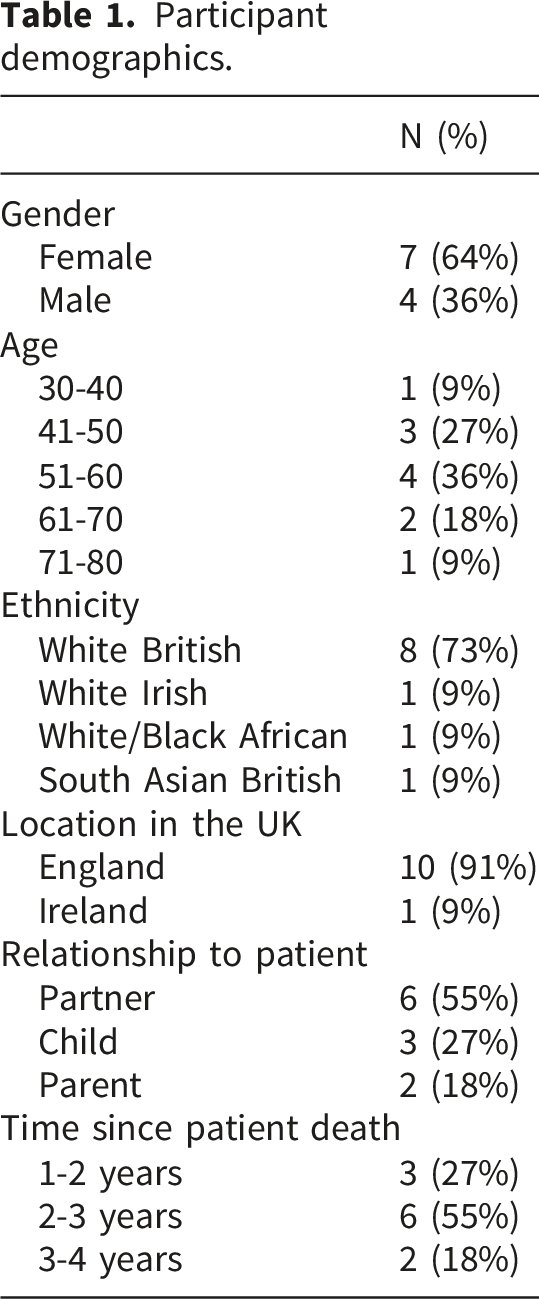
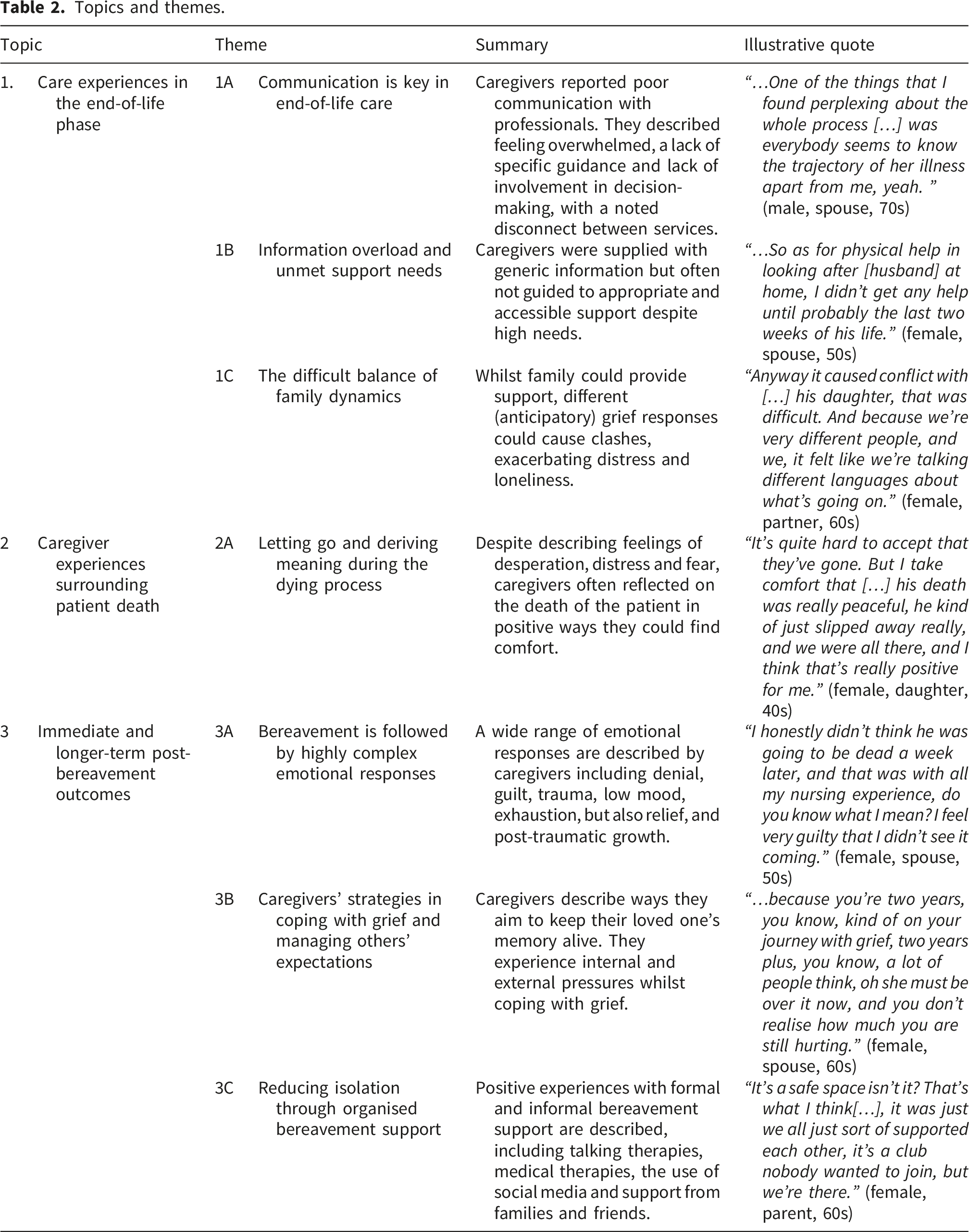
In three groups, 7 female (64%) and 4 male (36%) caregivers (55% partners of patients) of deceased patients diagnosed with glioblastoma were interviewed. Themes covered 1) care experiences in the end-of-life phase (covering communication, information, support needs, and balancing family dynamics), 2) caregiver experiences surrounding patient death, and 3) immediate and longer-term post-bereavement outcomes (covering complex and conflicting emotional responses, expectations and strategies to cope with grief, and the value of formal and informal support).
Conclusions
Findings highlight ongoing significant and unmet emotional support needs of bereaved neuro-oncology caregivers. Caregivers want and deserve to be proactively offered adequate and timely support which could limit the long-lasting adverse impact of providing care.
Plain Language Summary
Brain tumours place a heavy emotional and practical burden on family caregivers. Many caregivers experience lasting difficulties that can continue after the patient’s death. This study explored caregivers’ experiences during the patient’s end of life phase, the dying process, and life after bereavement, with the aim of identifying opportunities to improve support. We did online focus groups following a survey (reported elsewhere). Caregivers who were at least six months post‑bereavement were invited to participate. In total, 11 caregivers took part across three focus groups; most were women, and over half were partners of the patient. All had cared for someone diagnosed with glioblastoma. Discussions were audiorecorded, transcribed, and analysed using thematic analysis. Three main themes were identified. First, caregivers described their experiences during the end of life phase, highlighting challenges related to communication, access to information, unmet support needs, and managing family relationships alongside caregiving responsibilities. Second, caregivers shared their experiences surrounding the patient’s death, which was often described as intense and emotionally challenging. Third, caregivers reflected on their immediate and longer term bereavement experiences, including complex and sometimes conflicting emotions, expectations around grief, personal coping strategies, and the perceived value of both formal and informal support. Overall, the findings demonstrate substantial and ongoing emotional support needs among bereaved neurooncology caregivers. Caregivers emphasised the importance of being proactively offered timely and appropriate support, which may help reduce the long term negative effects associated with caring for someone with a brain tumour.
Introduction
The end-of-life phase, commonly defined as the last three months of life, is extremely burdensome in patients with primary brain tumours.1,2 The often-short disease course, rapid progression, and combination of oncological and neurological symptom burden3–5 cause significant distress. As the tumour progresses, patients and their caregivers (family members or friends who provide practical and emotional support) often increasingly attribute greater value to quality, rather than quantity of life. 6 Qualitative studies have described an increasing burden on caregivers, which can at times become overwhelming and unmanageable. 7 This was confirmed in our recent survey completed by 105 bereaved neuro-oncology caregivers, which also identified marked disruption to family life, compounded by often unsatisfactory information provision and support. 8
Importantly, caregivers’ struggles do not end after the patient dies. Difficult feelings of relief, and complicated grief-responses have been described.3,7 Depressive symptoms and fatigue are common post-bereavement, impacting on work- and social outcomes. 3 Indeed, our survey revealed notable rates of depression, anxiety, disruption to family life, low levels of resilience and symptoms compatible with post-traumatic stress disorder and prolonged grief disorder. 8 While other caregiver populations demonstrate similar responses,9–12 the prevalence of issues was higher in our sample of bereaved neuro-oncology caregivers.
To investigate these issues further, a nested sample of survey respondents took part in qualitative focus groups. With these focus groups we aimed to gain important contextual data and describe caregiver experiences during the patient’s end-of-life phase, the dying process, and beyond. This work will help understand caregivers’ struggles and identify opportunities to enhance support to ultimately limit the long-lasting adverse impact of a brain tumour diagnosis on families.
Methods
Focus groups were performed as part of a sequential explanatory mixed-methods study, co-designed and co-delivered by bereaved caregivers (PB and RM). The initial part of the study comprised a quantitative online survey. 8 A nested sample of survey participants contributed to the focus groups. The University of Leeds School of Medicine Research Ethics Committee provided approval (MREC 23-002).
Participants and procedures
For the overall study, caregivers were recruited from a closed Facebook group (‘Bereaved by a brain tumour’) which at the time of recruitment had approximately 1500 members. We also recruited through charities (brainstrust and the Brain Tumour Charity) via their social media channels and/or newsletter email. Adult bereaved caregivers of patients diagnosed with a primary malignant brain tumour were eligible if they: had been bereaved for ≥6 months; lived in the United Kingdom; had sufficient mastery of English to complete study procedures; had access to the internet; were able to provide consent. Exclusion criteria: professional, paid caregivers were not eligible, as the focus of the investigation was on informal caregiver perspectives. There was no focus on a specific relationship to the patient, and it was not necessary for caregivers to have been a part of the patient’s household, but they had to have held a caring role for the patient in some capacity. This was done because primary brain tumours are not common, and this work was intended to be hypothesis-generating. Due to the nature of the study we could not perform eligibility checks, although any respondents who self-reported to be under 6 months post-bereavement were excluded.
Following survey completion, participants could leave their contact details (provided by 68/105 (64.8%)) if interested in taking part in an online focus group. We purposely sampled focus group participants to reflect a breadth of experiences (e.g., different ages, genders, relationship to the patient, time since bereavement, ethnicity). To allow participants to share their experiences as freely as possible, we were mindful of the differences in caring experiences depending on relationship to the patient. Guided by bereaved caregiver co-investigators (PB and RM), we organised one group for male caregivers, one for spouses, and one for parents/adult children of patients. This latter group was arranged such since there was low uptake to the invitations from other potential participants that were either a parent, or adult children caring for a parent. Grouping these participants together provided a sample that was a similar size to the other groups, and neither too small for a focus group.
Focus groups were expected to last approximately 90 minutes. All participants received written and verbal study information and provided verbal consent. Consent statements, which were provided alongside the participant information sheet, were read out and confirmed by each participant prior to data collection. Participants were offered a £10 voucher as a token of appreciation. Focus groups were audio recorded, and reflexive notes were made after focus groups.
Focus groups
All focus groups were facilitated by an experienced qualitative researcher (SM, PhD, female research assistant), and experts-by-experience (PB, RM) co-facilitated one group each. Following team discussions, focus groups were deemed the most appropriate data collection method as it would allow us to provide a more supportive environment within which participants could share their experiences. The experts-by-experience (PB, RM) felt sharing similar experiences in a small group setting would be more appropriate than individual interviews, where participants may experience a sense of pressure from having a sole focus on them particularly when feeling overwhelmed.
Supervision was provided by the study chief investigator (FB) so that any issues arising after the focus groups could be discussed and reflected upon. A distress protocol was in place, which included addressing emotion reactions verbally, holding space for emotions, offering breaks or skipping questions or stopping groups if participants would prefer. For unexpectedly severe distress, the researcher would encourage caregivers to contact their general practitioner. These expectations were shared with participants in the study information materials. In practice, distress was manageable through light-touch strategies: no breaks, skipped questions, or referral to general practice were needed.
Each focus group started with general questions for the caregivers to introduce themselves. The second part involved retrospectively considering the period before the patient passed away, to the last three months of life. We then discussed the period surrounding the patient’s death and immediately post-bereavement, focusing on their own experiences and outcomes, to set the scene for further discussion on longer-term post-bereavement outcomes. The topic guide questions (see Supplementary Material 1) were developed based on our survey findings, 8 and in close collaboration with experts-by-experience (PB and RM). The topic guide was not formally pilot tested but refined through project team discussions ahead of the first focus group, with the reflexive thematic analysis approach allowing for changes during data collection.
Data analysis
Focus group data were analysed using reflexive thematic analysis,13,14 using NVivo, and following relevant reporting guidelines. 15 In line with qualitative research practice, we did not aim for a specific sample size but instead continued recruitment until data gathered were considered sufficiently rich to meet study aims. 16 Reflexive thematic analysis was considered appropriate since we approached analysis from the perspective of a paradigmatic framework of interpretivism and constructivism, assuming reality is subjective and socially constructed. This allowed the analysis to incorporate the subjectivity of the researcher, 17 and the experts-by-experience (RM,PB). The reflexive process began during data collection, as the researcher (SM) completed a brief reflexive diary after each focus group session. This allowed the ongoing data collection to be informed by the reflexive exercise and therefore additional questions were added when relevant. A qualitative researcher (SM) with a psychology background but new to the neuro-oncology care context lead analysis and read each transcript along with reflexive notes, enhancing familiarisation with the data. Reflexive notes allowed the researcher to consider several aspects that may impact data collection and interpretation. These are factors such as observations made during the focus groups for example of any group dynamics or times that certain participants did not contribute in the discussion.14,18 Transcripts were coded inductively to fully understand participant experiences and deductively to address research objectives. Codes were organised into subthemes and themes iteratively. The draft themes and subthemes were discussed and refined with experts-by-experience (PB and RM, supported by FB, an experienced qualitative researcher with neuro-oncology/family caregiving expertise) before finalising.
Results
Participants
Participant demographics.
Topics and themes
Topics and themes.
1. Care experiences in the end-of-life phase
1A. Communication is key in end-of-life care
Participants highlighted that a lack of clear communication between healthcare professionals and caregivers was at the heart of their issues.
Disease burden was invariably high and included a loss of independence, hallucinations, seizures, cognitive deficits, personality changes, a lack of insight, weight changes, communication difficulties, and patient’s mood issues, all profoundly impacting on caregivers.
Positive experiences with palliative and end-of-life care from hospices, district nurses, physiotherapists and occupational therapists were described as ‘very good’, ‘brilliant’, or ‘a wonderful help’. Negative experiences invoked strong emotional reactions including anger and frustration, as caregivers did not feel acknowledged or listened to. Some described feeling let down or patronised. For example, one participant indicated that there was no clear explanation of how their loved one would die and how devastating it may be to witness: “When people die of a brain tumour, […] people don’t understand how that person just gets slowly destroyed in front of you…” (female, daughter, 40s)
Stopping anti-tumour treatment could be emotionally difficult, with some caregivers expressing they felt decisions were made for them, rather than with them. This caregiver, who described his late wife as in good condition, was left feeling confused and shocked: “….and [hospital] made a very strange decision, in that they weren't going to treat her and that she was just suitable for palliative care. What then happened, when she came home, I had no realisation of what was going to happen. To me, the idea that she was going to die in a few weeks’ time was unbelievable in respect of her condition. ” (male, spouse, 70s)
Caregivers described the strangeness of being expected to speak to healthcare staff on behalf of the patient, without being involved as an active partner in decision-making: “And I don’t think they understand that, you know, on top of watching [partner’s] loss of dignity, and […] almost total loss of agency, […] if they asked me a question, I would turn my head to [partner], […] and I would repeat the question, and [partner] would answer the question. […] So they take his agency away, but they don’t give it to you as carer, you’re not allowed to make decisions.” (female, partner, 60s)
Several caregivers expressing misconceptions about the roles of the hospital and/or the hospice in providing end-of-life care. Whilst open and honest communication was highly valued, many caregivers highlighted that the hard, unpleasant truths were ‘skirted around’: “… Her oncologist wouldn’t make eye contact with her, and she asked how long she’d got, and he would not answer. […] All he told her was, she was about to buy a house with her partner and all he would say is, “Don’t sign a mortgage,” […]. I think we deserved, and she deserved a bit more than that.” (female, parent, 60s)
A disconnect between support services and healthcare professionals was described. Even within departments at the same hospital, it was noted: “no one speaks to one another” (female, daughter, 30s). At times, this could impact on the quality of care delivered, with e.g., medication not being organised in time. Caregivers indicated they were crying out for better information sharing and coordinated care: “…it's just unbelievable, […], there must be a better way of, within one hospital, with sharing information between the different doctors, […] it was almost like they have no contact with each other and no information sharing at all. ” (male, spouse, 40s)
1B. Information overload and unmet support needs
Caregivers were often directed to a lot of information (e.g., websites, leaflets) and therefore left feeling overwhelmed, but did not receive guidance as to what was specifically relevant to them, therefore not meeting their needs.
Caregivers reported trying to find answers to their questions online, or through social media: “…. I also tried to find out about death on the internet […] I wanted to know what the parameters of what can physically happen, what am I going to see, what am I going to experience, so that I was ready. But nobody told me the… they just didn’t, and that was really frustrating, I just, I needed to know…” (female, partner, 60s)
Although financial challenges were not uncommon, caregivers were often unaware of the benefits they were entitled to and some paid for additional (private) nurse support or equipment out-of-pocket: “…I’d taken my pension out so I could afford all stuff, like I could afford a car, and I got a bed, hospital bed in the bedroom, a big one, double.” (female, partner, 60s)
The need for professional support during the end-of-life phase varied. Some indicated that healthcare professionals seemed to understand their needs before they were even aware of them: “Even though you didn't ask for carers, they said, oh, maybe we can get some carers to come in to look after her. I said, okay, I was, you know, open to that, and they sort of almost knew what was going on.” (male, spouse, 50s)
Yet, even when support needs were identified, barriers to access included location (e.g., different availability of support in devolved nations), and age (funding for social services only available to people over 65). Informal support was described as invaluable when caregivers felt alone or overburdened, with one participant referring to her neighbour as ‘an angel’: “…She would pop in every couple of hours whilst I was at work, so we did it in shifts, […] if I needed a break when I was at home I would just go to hers, and watch the baby monitor at her house.” (female, daughter, 40s)
Support was often discussed in practical terms, whilst many caregivers also expressed a profound sense of loneliness, indicating an unmet need for emotional or social support.
1C. The difficult balance of family dynamics
Loneliness was exacerbated by the challenge of managing the expectations of the patient, and the wider family. At times this related to cultural backgrounds. Some participants described strong family support, allowing care tasks and responsibilities to be shared. Others talked about a new strain on family relationships, with relatives responding differently to the challenges of a brain tumour diagnosis. Moreover, patients did not always readily accept help from particular family members. One caregiver from a South Asian background explained: “…my dad would accept help from my brother and my mum, but he wouldn’t accept help from me, and I think that’s just, that was just how it was going to be, so I kind of had to accept that if he didn’t want my help in certain things…” (female, daughter, 40s)
Whilst at the time this had been difficult for this participant, she had come to understand that it was perhaps her father’s perception of maintaining his dignity at a time where he required help with personal care. This participant was able to find other ways to care for her father whilst respecting his wishes. Another described that the patient changed his mind about the role they wanted their adult child to fulfil in supporting them during the dying process: “…we talked about a certain care home, and I mentioned the name, and he looked at me with fear in his eyes, and he just said, “No, no, you, you, you,” and […] I think in all honesty it was fear, and maybe he had more trust in me than I ever thought he did.” (female, daughter, 40s)
This participant had no siblings to share the caring responsibilities with, which was described at burdensome at times. Still, the daughter was glad to have been able to care for her father in the way he wished. These examples illustrate that family dynamics can help or hinder provision of care, with different impact on caregiver burden, in the end-of-life phase.
2. Caregiver experiences surrounding patient death
2A. Letting go and deriving meaning during the dying process
The second topic covers the experiences immediately related to patient death. Participants spoke of acts they did to make sure that their loved one felt cared for, ensuring they were as comfortable as possible. For some, it meant that they too were able to heal rifts and feel the love reciprocated from their relative. “…I wish it hadn’t happened because he was dying, but it did, but it gave us the opportunity to, I understood fully that he did love me, and he knew just how much I loved him […].” (female, daughter, 30s)
Participants spoke about the way that their loved one had died, reflecting on their passing in ways that they could find comfort. They spoke about peaceful deaths or their loved one not knowing what had happened to them. Participants also indicated that it was important that they were able to be there with their loved one in their final moments. Some reflected on how letting go was, in retrospect, the best outcome. For example, when cardiopulmonary resuscitation was applied: “…Got her into hospital, and she had another massive seizure and her heart stopped, and they got her back seven times and then they said, “No.” And we fully agreed with them, we said, “No, there’s nothing you’re bringing her back for,”” (female, parent, 60s)
Depending on the relationship to the patient and their age at time of death, death could be viewed as a release from suffering or being spared further suffering: “I think for me the main relief was that [daughter] didn’t get to that point where she was in a hospital bed at home, […] Your relationship starts to change, you become a carer, and I didn’t want to become a carer, not a mum. And that didn’t happen, and that is a relief for me. And also that her relationship with her partner didn’t go through that awful change as well…” (female, parent, 60s)
Despite many positive experiences shared by participants, feelings of desperation, distress and fear were not uncommon: “I was so desperate, I just said to him, [cries], I just whispered in his ear, “Go to sleep my lovely.” […] And nobody had told me about the breathing, because I’d always wondered what a death rattle was, I thought it was something poetic and nice, but oh my good god it’s mechanical isn’t it, and loud” (female, partner, 60s)
3. Immediate and longer-term post-bereavement outcomes
3A. Bereavement is followed by highly complex emotional responses
After the patient died, several, mostly male caregivers expressed a sense of denial. Participants mentioned experiencing a dreamlike state during both the end-of-life phase and upon receiving the news of their loved one’s death: “…and you go home and you get that horrible call at four […]. But when you're told, it's just in a dream, you can't, you know, okay, well, I'll have another half an hour in bed and I'll go over there, but then you sort of snap out and think, hang on, I’ve got to get over there and sort it out…” (male, spouse, 50s)
Feelings of guilt were not unusual, sometimes linked to not having been able to respect the patient’s wishes, or feeling like they withheld information from them: “I feel a lot of guilt surrounding that [dying in hospice care], because [husband] wanted to be at home. […]. But he stayed up in his bed, and I ended up, I hurt myself […] I mean, I was kind of half holding him up whenever he was wanting to the toilet.” (female, spouse, 50s) “….when the clinical nurse specialist came in the last week of [patient’s] life, and she spoke to me in whispers and I didn’t know why she was speaking to me in whispers, and I couldn’t really make sense of what she was saying. […] And he said to me, “Was it positive what she said?” and I said to him, “Yes, it was.” Because I didn’t feel I could say anything else, and I feel really guilty about that, because that’s the only time I’ve ever lied to [husband].” (female, partner, 60s)
The experience was described as traumatic by some, both explicitly, or through speaking of nightmares, replaying the situation, or experiencing flashbacks: “…it took a long time for things to stop playing over in my head, the dreams, the nightmares, the feelings of guilt, there was things that I might have done wrong.” (female, daughter, 30s)
Many participants, particularly men, indicated that they were still struggling with low mood. Grief was described as exhausting. Death could be perceived as an escape from complex and unresolved feelings: “…I would say, I feel completely numb, I feel completely empty, yeah, I don't know what's happening tomorrow and in a way I don't care tomorrow. There are times when I could say, quite honestly, I don't want this life, this life I have, I don't actually want it. That doesn't mean to say I'm going to harm myself, it means that given a choice, I want to be anywhere else but where I am now, yeah.[…] And because I feel that all these thoughts are so complex and unresolved, I actually envy my wife, I actually envy my wife for not having to deal with all this.” (male, spouse, 70s)
Losing a partner or soulmate, was described as losing part of their own future: “…I suppose losing your soulmate is completely different. […] you lose your hopes and dreams.” (female, spouse, 50s).
Yet, some participants described aspects of post-traumatic growth, allowing them to focus on what is most important in life: “I think it’s made me not sweat the small stuff, and I think it’s allowed me to let joy into my life, in a funny way, you know? And yeah, just enjoy what I have, not to dwell on what I’ve lost, but to be thankful for what I have, which as I say was a lot, I’m very fortunate.” (female, parent, 60s)
3B. Caregivers’ strategies in coping with grief and managing others’ expectations
Various strategies to deal with the loss of their loved one were brought up. For some this was about the way they chose to live their life, for others it was in the way they chose to spread ashes of their loved one. Others mentioned fundraising for charities, pushing on with shared plans such as a house move, taking up the hobby that their loved one used to practice, or creating physical reminders: tattoos, jewellery, benches, and plaques. This was accepted by several participants as part of managing grief. “…I went through this phase of wanting to put [husband's] name on everything and I would see who I could pay. Can I have a bench, can I have this, can I put his name on that […]. I honour his memory now by just living and getting on and trying to get back to normal.” (male, spouse, 50s)
Many participants spoke about how it was important for them to mention their loved one in conversation. This allowed them to keep their memory alive and acknowledge their existence. Participants found it difficult, sometimes hurtful or annoying, when friends or family were hesitant to mention the patient’s name.
Despite several participants expressing they were not religious or practicing their religion, some did find comfort and solace in spiritual beliefs. “When he passed I was holding his hand, and I felt like I physically felt him leave, like he… and I think if I hadn’t been able to see him and feel him at that time, I would never have known that that was a feeling you could have. […]. And that helped me a lot, because […] everything that made up my dad was no longer there, but it didn’t feel like it had stopped, it felt like it had just left. So it didn’t feel as final I think as I expected it to. […] So yeah, so spiritually weirdly I’ve got a new appreciation for what I think may happen, you know, once people leave, which is comforting…” (female, daughter, 30s)
Getting back to a sense of normality after their loss, was expressed in different ways, for example returning to work or engaging in social activities, despite not feeling like it: “Although I’m not enjoying things, I’m still going through the motions, and that’s enough for now.” (female, spouse, 50s). For others, life only became more normal when the nightmares ended.
Participants reflected on the length of time they were grieving, with many being years post-bereavement and still describing their grief as coming in waves or cycles, with seemingly random everyday items or events triggering their feelings of loss. Some described they felt friends expected them to have moved on, while their grief was still overwhelming at times. Some were still finding it difficult to find enjoyment in life: “…because you’re two years, you know, kind of on your journey with grief, two years plus, you know, a lot of people think, oh she must be over it now, and you don’t realise how much you are still hurting.” (female, spouse, 60s)
3C. Reducing isolation through organised bereavement support
Articulating support needs could be difficult but those who accessed bereavement support services found these useful. Bereavement support was often provided through hospices (pro-actively offered) and charities (self-sought). “… I had some EMDR therapy [privately paid] which was really helpful, and we plugged into a bereavement charity for [my] children that really helped.” (female, daughter, 40s)
Peer support through social media was invaluable, a non-judgemental and safe space, or ‘a lifesaver’: “It’s a safe space isn’t it? That’s what I think[…], it was just we all just sort of supported each other, it’s a club nobody wanted to join, but we’re there.” (female, parent, 60s)
Family and friends, or face-to-face peer support, were also found helpful. Participants indicated that shared experiences could bring people together, reducing isolation: “… [Son’s] best friend also had a glioblastoma, he was diagnosed six months after [son], and he has subsequently died, […] and I’ve become very close to his parents. And so we’ve got quite a close-knit support group, that has developed around those, you know, the two boys…” (female, parent, 60s)
A participant indicated they benefitted from antidepressants, which they found upsetting, perhaps because it suggested to them that they were not coping as well as they thought: “I’m on antidepressants […] and I remember when I got them and I looked and I just cried, and thought, this is where I am now, but […] they’ve really helped me, for sure.” (male, spouse, 50s)
Although not intended to function as a peer support group, participants expressed they found taking part in the focus group cathartic and helpful. In the male group, in particular, there were expressions of how they would welcome regular sessions: “I do see a regular counsellor, but I think I personally would benefit from this kind of group on a regular basis, but it doesn't exist.” (male, spouse, 70s)
Discussion
Key findings
Throughout the end-of-life phase, caregivers spoke of difficulties navigating support services, with service providers often not communicating between themselves. The patient’s death itself was described as both a continuation of the difficult disease trajectory, and also a relief or a comfort. This was, understandably, and in line with existing literature,19,20 influenced by the nature of the relationship between caregiver and patient, as well as the patient’s age.
Experiences related to information and (practical) support provision varied. The good experiences were described in highly positive terms, the bad experiences made a profound and lasting negative impact. This is in line with existing literature.3,21,22 In addition to known changes in the patient-caregiver relationship, 23 our study illustrates how family function and dynamics can play a role. When a family came together to support each other this was extremely valuable, but the patient’s illness could also bring with it new family dynamics and conflicts, as people deal with loss and grief in different ways. Family-focused interventions could be beneficial, with good family functioning associated with a lower risk of adverse post-bereavement outcomes. 8
The processes of grief described by participants, to some extent match adaptive grief responses with e.g., continuing bonds through keeping memories alive, 24 finding meaning in the loss, and turning to religion or spirituality to make sense of death.25,26 Both cognitive and affective strategies in coping with the loss are described, and participants mentioned internal and external pressures to grieve in certain ways – many caregivers said they ‘should be over it now’. This is consistent with established bereavement models.27,28 Feelings of guilt described by our participants, are common in bereaved caregivers and thought to be linked to depression outcomes. 29 Yet, we also note precursors of complex grief issues, with caregivers describing trauma, flashbacks, and nightmares – symptoms of post-traumatic stress disorder; and a sense of disbelief or denial about death, intense emotional pain, difficulty with reintegration, emotional numbness, a loss of meaning in life, and loneliness – symptoms of prolonged grief disorder. Cutting across all themes was a profound sense of loneliness, with unmet emotional and social support needs. Clearly, carers’ support needs do not end after the patient dies.3,7,30,31 The focus group findings from this sequential mixed-methods study therefore contextualise the survey results which noted high rates of adverse mental health outcomes post-bereavement– with high rates of depression (35%), anxiety (61%), disruption to family life (53%), low levels of resilience, and indications of high risk for post-traumatic stress disorder (42%) and prolonged grief disorder (64%). 8
Our findings are sobering, especially since one of the first articles covering bereaved neuro-oncology caregiver experiences was published in 2004, 31 and the importance of supporting neuro-oncology caregivers in palliative care has since been highlighted. 32 Yet little seems to have improved in the United Kingdom.
Participants described some helpful strategies for coping with their experience, including formal (pharmacological and non-pharmacological) and informal support (from family, friends, or peers). DSM-V mental disorders, once manifested, require intensive intervention. Guidelines from NICE and the World Health Organisation exist for the management of post-traumatic stress disorder and prolonged grief disorder,33,34 but strategies for prevention are less well-established. The international neuro-oncology community calls for routine bereavement support.35,36 With recent systematic reviews not identifying any trials of interventions targeted at bereaved neuro-oncology carers,37–40 and systematic reviews critiquing the robustness of existing bereavement support studies in general,41–43 it is hard to push for service improvement without further work. We envision this includes the development, testing, and integration of a comprehensive neuro-oncology caregiver support programme. This should start early in the disease trajectory to better support caregivers in managing the acute and fast-changing patient needs, but also provide caregivers with guidance and support on managing their own mental and physical health needs as the disease progresses, through the end-of-life phase, and beyond to build resilience, strengthen social networks, and where possible, prevent the long-lasting adverse impact of a brain tumour bereavement.35,40,44
Strengths and limitations
This work was designed and delivered together with bereaved caregivers. It is noteworthy that the experts-by-experience (PB and RM) approached the lead researcher (FB) with the initial idea of setting up a study focusing on end-of-life and post-bereavement experiences, based on their observations among peers. Together, we have designed and delivered the project: defining project aims, methods, recruitment, focus group topics and delivery, analysis, and write-up. Particularly, their co-facilitation of focus groups supported and encouraged open and honest conversations about this highly emotive topic. Similarly, their input into the reflexive thematic analysis was invaluable. With an author team that represents doctors (LM), nurses (KP, RM), chaplains (CLS), palliative care (LZ), family caregiver (FB), and health research (SM) experts, and bereaved caregivers (RM, PB), the analytical process was enriched by our diverse backgrounds.
There is a potential sampling bias for the overall study in predominantly recruiting through social media. Despite careful purposive sampling, which ensured focus group input from caregivers of different genders, ages, and relationship to the patient, we were less successful in obtaining variation in cultural background. The requirement of speaking English enabled us to facilitate rich group discussions, but we acknowledge that there could be a bias in non-representation of experiences from non-English speaking caregivers. Due to our recruitment methods, we could not perform eligibility checks and relied on self-report.
Conclusions
Our work describes the experiences of neuro-oncology caregivers through the end-of-life phase into post-bereavement, highlighting ongoing significant and unmet emotional support needs. Neuro-oncology caregivers who are in the midst of what may be one of the most challenging periods in their life, may not be able to identify or articulate their support needs. Therefore, the neuro-oncology research and clinical community needs to find ways to identify those at highest risk and proactively offer timely and accessible support to limit the long-lasting adverse impact of providing care.35,45,46
Supplemental material
Supplemental material - “It’s a club nobody wanted to join, but we’re there”: Focus groups on end-of-life care experiences and long-term outcomes of bereaved neuro-oncology caregivers
Supplemental material for “It’s a club nobody wanted to join, but we’re there”: Focus groups on end-of-life care experiences and long-term outcomes of bereaved neuro-oncology caregivers by Shaista Meer, Rosanna Miller, Peter Buckle, Louise Murray, Catherine Lewis-Smith, Lucy Ziegler, Karin Piil, Florien Boele in Palliative Care and Social Practice
Footnotes
Acknowledgements
We would like to thank all participants for their time and effort. We also thank the Bereaved by a Brain Tumour Facebook group, brainstrust and the Brain Tumour Charity for supporting recruitment.
Ethical considerations
The University of Leeds School of Medicine Research Ethics Committee provided approval (MREC 23-002).
Consent to participate
All participants provided informed verbal consent.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by combined funding from a University of Leeds Academic Development Grant (to FB) and Yorkshire Cancer Research (L389FB to FB, L389LM to LM).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FB: speaker (Medscape, Medtalks, Servier, Angelini Pharma); KP: consultancy (Servier), speaker (Medscape). The other authors report no conflict of interest.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author (FB), upon reasonable request and following appropriate agreements.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.