
Abstract
This randomized controlled trial investigated whether an internally validated animated video, added to standard consent, improves patient understanding and satisfaction before elective percutaneous coronary intervention. Adults scheduled for percutaneous coronary intervention were randomized to receive either standard consent or standard consent plus an internally validated, local language animated video. Patient understanding and satisfaction were assessed using validated questionnaires and a visual analog scale, respectively. The intervention group demonstrated significantly higher knowledge scores and satisfaction, with no significant influence from socio-economic or educational status. This study supports implementing animated videos to enhance patient comprehension, satisfaction, and bridging the health care gap.
Keywords
Introduction
Informed consent ensures that patients understand a medical procedure risks and benefits before voluntarily agreeing to it. This vital process empowers patients to make informed decisions about their own healthcare. 1 In cardiac procedures like percutaneous coronary intervention (PCI), patients often exhibit an incomplete understanding when providing consent due to various factors. 2 Discrepancies frequently exist between the information delivered and the patient’s actual level of understanding, highlighting the critical need for objective evaluation methods.3-5 This study aims to compare understanding and the level of satisfaction between groups receiving either standard or video-based consent before PCI.
Methods
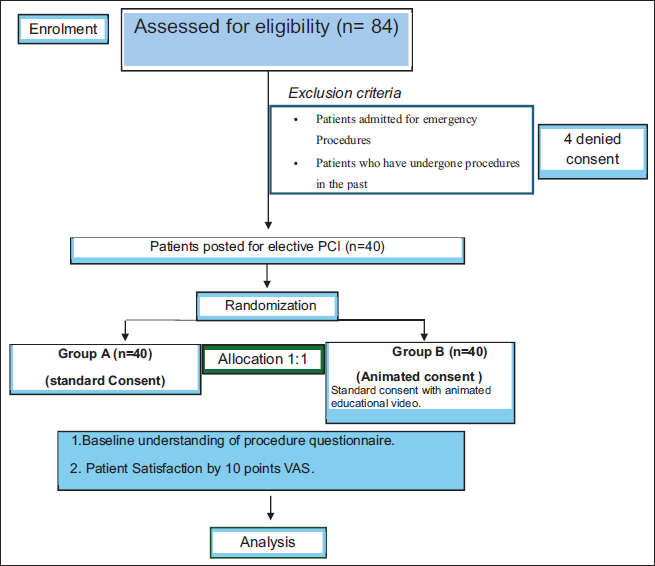
This was a single-center, parallel-group, randomized controlled trial comparing animation-based education with standard verbal consent for elective PCI patients (age ≥18). Participants were assigned 1:1 via block randomization with allotment concealment. Group 1 received standard written and verbal consent, while Group 2 received an internally validated animated video in their local language in addition. All discussions occurred in a private room with blinding of the principal investigator. The questionnaire was administered by a study investigator not involved in the consent process. Outcome assessment was performed by an independent investigator who was blinded to group allocation. Patients were instructed not to disclose their group allocation during assessment. The primary endpoint was the difference in dedicated information score measured by a dichotomous questionnaire, and the secondary endpoint was patient satisfaction assessed by a 10-point visual analog scale (VAS) (Figure 1).
CONSORT Flow Diagram Showing Patient Screening, Randomization, Allocation, and Final Analysis of the Study Population.
Tools
Patient understanding of the PCI procedure was assessed using a six-item dichotomous questionnaire addressing the core elements of informed consent: indication, purpose of the procedure, procedural steps, risks, benefits, and available alternatives. The questionnaire was adapted from a previously published study conducted in our department that evaluated patient understanding during informed consent for coronary angiography. 6 The tool was reviewed and refined by a multidisciplinary departmental committee consisting of interventional cardiologists, cardiology fellows, catheterization laboratory nurses, technicians, and a medical social worker to ensure clinical relevance and content validity for the PCI setting. Responses were recorded in a dichotomous format (Table 1).
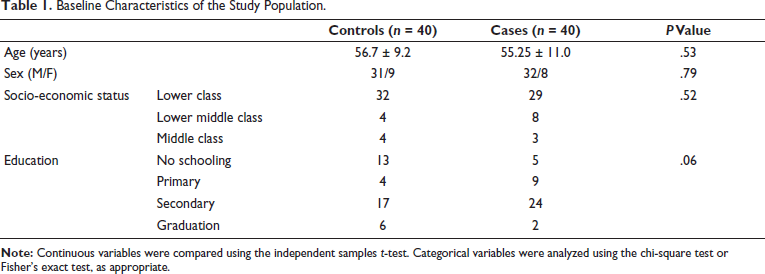
Baseline Characteristics of the Study Population.
Patient satisfaction regarding the information provided was assessed by a 10-point VAS. 7
Animated Video
The animated educational video was the core intervention, designed to clearly explain the indications, procedural steps, expected benefits, and risks of PCI. It integrated videos from the catheterization laboratory with 3D animations sourced from publicly available sources. Video content was validated by a departmental committee comprising five senior cardiologists, three senior nurses, five technicians, and a medical social worker.
Statistical Analysis
Data analysis was done using both descriptive and inferential statistics, strictly following the intention-to-treat principle. For continuous variables (e.g., knowledge scores and VAS scores), normality of distribution was assessed using the Shapiro–Wilk test. Data were expressed as mean ± standard deviation, where normally distributed. Between-group comparisons were performed using the independent samples t-test for normally distributed data; otherwise, appropriate non-parametric tests were considered. For categorical variables (e.g., responses to the six-item questionnaire), chi-square tests were used. All tests were two-tailed, and a P value < .05 was considered statistically significant. Assumptions of independence of observations and appropriate sample size for each test were also ensured. The sample size was calculated to detect a 10%-point difference in knowledge scores, requiring 36 participants per group based on 80% power and α = 0.05. Adjusting for a 10% attrition rate, the final sample size was 40 participants per group. 6 A total of 84 patients were assessed for eligibility, of whom four were excluded based on predefined criteria (as shown in the Consolidated Standards of Reporting Trials diagram), resulting in 80 participants who were randomized equally into two groups.
Results
Baseline characteristics confirmed successful randomization, and both the control and intervention arms were statistically comparable in age (control: 56.7 ± 9.2 years; intervention: 55.25 ± 11 years), gender distribution, socio-economic class, and education level (Table 1).
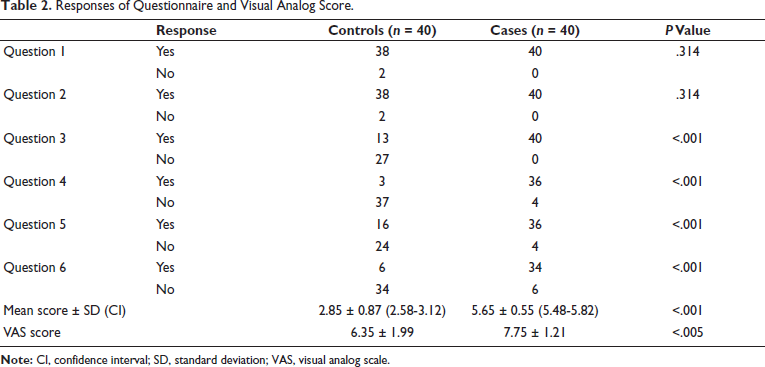
Animated consent significantly improved patient understanding of key procedural aspects compared with standard consent. The intervention group demonstrated a significantly higher understanding across all six core procedural elements tested, as evidenced by markedly greater rates of correct responses. The intervention group also showed markedly higher correct responses on challenging questions (5 and 6). Patient satisfaction scores were also higher in the animated education arm (Table 2). The mean knowledge score was significantly higher in the intervention group compared to the control group (5.65 ± 0.55 vs. 2.85 ± 0.87; mean difference 2.80, P < .001). Association of all responses to questionnaires with education and socio-economic status was compared; however, no significant association was found.
Responses of Questionnaire and Visual Analog Score.
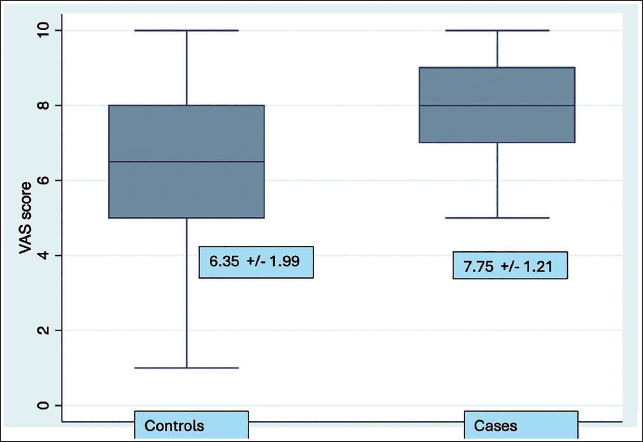
The success of the intervention was independent of demographic factors; VAS scores showed no statistical significance across different educational or socio-economic categories (P = .34 and P = .25, respectively) (Figure 2).
Box and Whisker Plot Diagram Showing Distribution of Visual Analog Score.
Discussion
To our knowledge, this study represents one of the first randomized studies to prospectively demonstrate the superiority of an internally validated educational animation model over standard consent protocols in an Indian context.
Primary End Point
Administration of an animated video in the patient’s own language convincingly demonstrated the feasibility of integration of this strategy in standard consent-taking protocols for PCI. The intervention group had a better understanding of all six core elements of the procedure (indication, purpose, protocol, risks, benefits, and alternatives), specifically in question number 3-6, suggesting that the standardized, visual, and language-flexible format of the video effectively overcomes communication barriers, disparity in literacy levels, and time constraints faced by the consent-takers. The development and expert validation of our animated video by a departmental committee ensured that the information delivered is reliable, compared to the risk of misinformation on unverified online sources and new artificial intelligence chat applications, which are available in the public domain.8, 9
Secondary End Points
Animated videos have demonstrated decreased anxiety and improved patient satisfaction in previous studies. In our study, the secondary objective was strongly supported, with the intervention group performing better in the satisfaction score measured by visual analog score (7.75 ± 1.21 vs. 6.35 ± 1.99, P < .005), pointing towards adequate clarity and sufficiency of the information provided.
Patients scheduled for PCI, particularly those who have not undergone the procedure previously, often exhibit anxiety and low levels of understanding. This becomes important, especially in the Indian context, where anxiety, depression, and low health literacy are understated.10, 11 Standard informed consent relies on the patient’s background knowledge of cardiac ailments and the consent taker’s communication style, making consistent information delivery and retention difficult. 12 The use of a validated, standardized animated video effectively mitigates these variables, and our study directly addresses this deficit comprehensively. A large proportion of our patients belonged to lower socio-economic groups, where health literacy and access to reliable information are often limited. A simple, language-based animated video can help overcome these barriers by providing clear and consistent information, which may explain the improved understanding and satisfaction seen in our study.
Western studies have also explored similar modalities, which showed that animations significantly improved reported understanding for urgent angiography patients. This study reiterates and extends this international data into the Indian context. 12 Visual add-ons in the form of movies and animations have shown to decrease anxiety, improve cooperation during the procedure, and also enhance recovery in the postoperative period.13, 14 The high patient satisfaction (measured by VAS) shows this method provides a patient-caring, compassionate environment, which fulfills both legal and ethical consent criteria. Moreover, there was no association between responses to the questionnaire and VAS with education and socio-economic status, indicating the effectiveness of this strategy across diverse patient backgrounds.
Limitations and Future Direction
We acknowledge that, while the questionnaire was grounded in a previously published institutional study, formal external validation was not performed in the department. The short-term impact of animated education on knowledge and satisfaction appears to be robust, but further research and multicenter validation studies are necessary to assess long-term retention and behavioral outcomes. This could enhance doctor–patient communication, enhance decision-making, and ultimately translate to better patient outcomes. Furthermore, this approach has the potential to be applied to other fields in medicine.
Conclusion
Inclusion of animated content in the consent is a powerful strategy to enhance comprehension, satisfaction, and mitigating the healthcare gap. It should be actively promoted as a promising strategy, potentially extending to other interventional specialties.
Footnotes
Data Availability Statement
The video is intended for non-commercial academic use, and we would be pleased to share it upon request. Interested individuals may contact the corresponding author, and a secure download link will be provided free of cost.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval was taken from instituite ethical committe before initiation of the study. Patient consent was taken before enrollment in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Appendix A. Participant’s Level of Understanding of Angioplasty Procedure.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.