
Abstract
In this issue, we will present the original research abstracts submitted for the Best Research Paper at the 11th Annual CSI Conference, Telangana Chapter, held at Park Hyatt in Hyderabad on February 28 and March 1, 2026. The abstracts have been condensed into a single paragraph due to word limit restrictions.
Keywords
Aakanksha Pandey, Syed Imamuddin, Ravi Srinivas, KMK Reddy P.
Osmania Medical College, Hyderabad
Impaired right ventricular–pulmonary arterial (RV–PA) coupling is a key mechanism in right-sided heart failure and is associated with adverse clinical outcomes. Since invasive assessment of RV–PA coupling is not feasible in routine practice, echocardiographic surrogates such as the tricuspid annular plane systolic excursion to pulmonary artery systolic pressure ratio (TAPSE/PASP) and pulmonary pulse transit time (pPTT) have been proposed. While TAPSE/PASP has been validated in heart failure and pulmonary hypertension, comparative outcome-based data against established right ventricular functional markers remain limited. This study was conducted to evaluate the prognostic utility of these markers in patients with secondary tricuspid regurgitation. They were compared with an established marker of RV performance, fractional area change (FAC). The primary outcome was a composite of clinical worsening and death. At one year, of the 100 patients evaluated, 56% were clinically stable, improvement in clinical class was observed in 19%, and worsening of clinical class in 19%. Mortality occurred in 6%. When the composite endpoint was assessed, the TAPSE/PASP, RV FAC, and pPTT showed an AUC of 0.88, 0.75, and 0.60, respectively. A TAPSE/PASP cutoff of 0.30 identified patients at increased risk. To conclude, in patients with secondary tricuspid regurgitation, RV–PA coupling as assessed by TAPSE/PASP is a reliable, easy echocardiographic marker to estimate 1-year mortality compared to RVFAC and pPTT. Larger studies are needed to strengthen the clinical applicability of this echocardiographic surrogate of RV–PA coupling.
Vaasanthi Chintala, KMK Reddy P., Praveen Nagula
Osmania Medical College, Hyderabad
Left ventricular dysfunction, quantified through ejection fraction (LVEF) on echocardiography, is a significant prognostic factor in patients with coronary artery disease (CAD). However, the assessment of LVEF has limitations, primarily due to intra- and interobserver variability. Global longitudinal strain (GLS) has been shown to have greater prognostic significance but requires high-quality echocardiographic views for accurate evaluation. Recently, tissue motion annular displacement (TMAD) has emerged as a rapid and reliable alternative for assessing left ventricular systolic function. TMAD measures the longitudinal displacement of the mitral annulus and the left ventricular apex, and it requires less time and technical skill than GLS. This study aimed to evaluate the efficacy of TMAD as an alternative to GLS in predicting subclinical left ventricular dysfunction in patients with CAD. A total of 200 patients were assessed. The correlation between TMAD values and GLS was significant, with the strongest correlation observed with mean TMAD, followed by the TMAD 2C view and the TMAD 4C view (r = 0.84, 0.66, and 0.56, respectively). Due to its rapid assessment capabilities, TMAD proves to be an effective alternative to GLS in patients with CAD.
Aadil Rafeeq Shaher, Syed Imamuddin, Ravi Srinivas
Osmania Medical College, Hyderabad
Non-ST-segment elevation acute coronary syndrome (NSTE-ACS), which includes non-ST-elevation myocardial infarction (NSTEMI) and unstable angina (UA), is associated with diverse plaque pathology. Conventional coronary angiography offers limited insight into the mechanisms involved. Optical coherence tomography (OCT) allows for high-resolution, in vivo assessment of culprit lesion morphology and plaque vulnerability. This study aimed to characterize plaque morphology in these patients. A total of 100 patients were examined using OCT, comprising 70 patients with unstable angina and 30 patients with NSTEMI. The most common type of plaque observed was fibrous plaque in 40%, followed by lipid-rich plaque in 32% and calcific plaque in 28%. Plaque erosion was found in 48% of patients, while plaque rupture was seen in 38%. Intracoronary thrombus was present in 50% of the patients, and macrophage infiltration was noted in 18%. Thin cap fibroatheroma was more prevalent in NSTEMI patients compared to those with unstable angina (58.3% vs. 21.4%, P = .02). Plaque rupture was associated with NSTEMI, while plaque erosion was linked to unstable angina. Additionally, red thrombus was more frequently observed in NSTEMI patients.
Bhavya K., Bhargavi, Nageshwar Rao K., Swetha Bhakru
Rainbow Children’s Heart Institute, Banjara Hills, Hyderabad
Patent ductus arteriosus (PDA) in preterm neonates is a major cause of prolonged hospital stay and a significant contributor to failure to extubate. Traditionally, these infants were referred for surgery due to the need for large sheaths and the risk of left pulmonary artery (LPA) stenosis and coarctation associated with the Amplatzer duct occluder-1 (ADO1). This study aims to evaluate the effectiveness and feasibility of transcatheter PDA device closure using the Amplatzer Piccolo device in ventilator-dependent preterm neonates, as well as to monitor improvements in their hemodynamic status. A total of 33 ventilator-dependent preterm neonates who underwent transcatheter PDA device closure with Amplatzer Piccolo device under fluoroscopic and echocardiographic guidance were studied. The infants were electively intubated and transported in incubators from their respective neonatal intensive care units (NICU). None of the babies received heparin during the procedure. Following device deployment, echocardiography was conducted to assess blood flow in the descending aorta and the left pulmonary artery. The median birth weight of the neonates was 1 kg, and the median weight at the time of the procedure was 1.2 kg. The mean age at the time of intervention was 26 days, with a 5/2 Piccolo device used in 50% of the cases. Successful device placement was achieved in all patients. Follow-up echocardiography confirmed stable device positioning without evidence of coarctation or LPA stenosis. The findings in this study suggest that transcatheter PDA device closure using the Piccolo device is a safe and effective procedure for preterm neonates, facilitating earlier weaning from ventilators and reducing hospital stays when performed by experienced teams.
Supreet Rao Patil, KMK Reddy P., Praveen Nagula
Osmania Medical College, Hyderabad
Acute coronary syndrome (ACS) occurs due to the sudden disruption of atherosclerotic plaques accompanied by thrombosis. Pathological studies have identified two main causes of ACS: plaque rupture and plaque erosion. Optical coherence tomography (OCT) allows for near-histological, in vivo evaluation of the morphology of these culprit plaques. This study aimed to assess plaque morphology in patients with ACS. A total of 30 consecutive patients who underwent OCT before stent deployment were analyzed. The average age of the participants was 52.2 ± 10.7 years, with 66.7% being male. ST-Elevation Myocardial Infarction (STEMI) accounted for 50% of the presentations. Overall, plaque rupture and erosion were observed in 53.3% and 33.3% of patients, respectively. Plaque rupture was significantly more common in those with STEMI (93.3% vs. 13.3%, P < .0001), while plaque erosion was more frequently seen in patients with non-ST-Elevation ACS (NSTE-ACS) (60% vs. 6.7%, P = .005). Red thrombus was predominantly found in STEMI cases, whereas white thrombus was more common in NSTE-ACS patients. These findings indicate that OCT can reveal distinct plaque morphologies in patients with ACS. STEMI is primarily associated with plaque rupture, while NSTE-ACS is often linked to plaque erosion, which supports the use of OCT-guided management strategies for these patients.
Likitha M., Suneetha K., Harish T.
Osmania Medical College, Hyderabad
The evidence regarding the relationship between the estradiol/testosterone (E2/T) ratio and the severity of disease burden in postmenopausal women with acute coronary syndrome (ACS) is still limited, especially in the South Asian population. This study aimed to assess this relationship in this specific group. A total of 100 postmenopausal women were studied. Patients with a history of myocardial infarction, those undergoing hormonal therapy, individuals with a history of malignancy, or those with valvular heart disease were excluded from the study. The E2/T ratio was calculated at the time of presentation, and the severity of coronary artery disease (CAD) was evaluated using the modified Gensini score (mGS), which categorized the disease as mild, moderate, or severe. The findings revealed a strong inverse correlation between the E2/T ratio and the mGS (ρ = –0.910, P < .001). The median E2/T ratio decreased as the severity of CAD increased, with values of 1.7 for mild disease, 0.65 for moderate disease, and 0.33 for severe disease (P < .001). In a multivariable linear regression analysis, the E2/T ratio remained independently associated with the increasing mGS, even after adjusting for factors such as age, hypertension, diabetes mellitus, dyslipidemia, and obesity (β = –61.79; 95% CI –68.28 to –55.30; P < .001). In contrast, traditional cardiovascular risk factors did not show an independent link to the angiographic severity of the disease. In conclusion, a lower E2/T ratio is strongly and independently associated with the angiographic severity of CAD in postmenopausal women with ACS. This suggests that an imbalance between endogenous sex hormones significantly contributes to the development of coronary atherosclerosis.
Faraaz Ahmed, Syed Imamuddin, Harish T.
Osmania Medical College, Hyderabad
Plaque rupture and plaque erosion are the principal mechanisms underlying acute coronary syndromes (ACS). Optical coherence tomography (OCT) allows high-resolution, in vivo visualization of culprit lesion morphology and may support morphology-guided reperfusion strategies. Data from South Asian STEMI cohorts remain limited. To compare the clinical and angiographic characteristics of ST-segment elevation myocardial infarction (STEMI) patients with OCT-defined plaque erosion versus plaque rupture, 30 consecutive STEMI patients undergoing primary percutaneous coronary intervention (PPCI) underwent pre-intervention OCT assessment. Culprit lesions were classified as plaque erosion or plaque rupture based on established morphological criteria. Demographic variables, cardiovascular risk factors, and angiographic patterns were compared between groups. Plaque erosion was identified in 16/30 patients (53.3%) and plaque rupture in 14/30 (46.7%). Patients with erosion were more frequently younger (<40 years; 50 years: 68.7% vs 35.7%). Smoking was more prevalent among erosion cases (62.5% vs. 42.9%). Prior statin therapy was also higher in erosion (56.2% vs. 28.6%). Single-vessel disease predominated in erosion (56.2%), whereas multivessel disease was more commonly seen in rupture (64.2%). The left anterior descending artery (LAD) was the most frequent culprit vessel in both groups. STEMI related to plaque erosion is characterized by younger age, smoking history, and more localized coronary involvement, whereas plaque rupture is associated with older age and diffuse disease. OCT-guided identification of lesion morphology may refine individualized PCI strategies.
Caroline Sarayu, Tripti Deb
Apollo Hospitals, Jubilee Hills, Hyderabad
Cardiogenic shock complicating ST-elevation myocardial infarction (STEMI) continues to be associated with high mortality. While extensive data are available from developed countries, information from low- and middle-income countries like India remains limited. Differences in epidemiological profile, access to timely revascularization, availability of mechanical circulatory support, and long-term outcomes make the application of global guidelines challenging in resource-limited settings. This study aimed to evaluate the profile of patients with cardiogenic shock admitted to Apollo Hospitals, Jubilee Hills, between January 2023 and July 2025. A total of 120 patients aged >18 years of both sexes with STEMI, elevated lactate, and hypotension within 48 h of symptom onset were included. Primary endpoints were overall survival, mortality, and functional status improvement. Secondary endpoints included length of hospital stay, vascular complications, renal replacement therapy, and sepsis. Among 120 patients, 80% were male with a mean age of 61.6 years. Diabetes (41.7%) and hypertension (39.2%) were common comorbidities. Cardiac arrest occurred in 33.3%, and mechanical ventilation was required in 70.8%. Reduced ejection fraction (≤30%) was seen in 53.3%. PCI was performed in 84.2%, with culprit-only PCI in 70.9%. MCS was used in 47.5%, mainly IABP. In-hospital mortality was 53.3%. Multivariate analysis identified cardiac arrest, renal failure, mechanical ventilation, advanced SCAI stage, shorter hospital stay, and triple vessel disease as significant predictors. Cardiogenic shock complicating STEMI remains associated with high in-hospital mortality despite advances in therapy. Early identification and aggressive management of high-risk patients are essential to improve outcomes.
Sachin Rahul, Karthik P. Jadhav
Apollo Hospitals, Hyderguda
Electrolyte imbalance is common in acute coronary syndrome (ACS) and contributes to electrical instability and early complications. Magnesium has membrane-stabilizing and anti-arrhythmic properties, but its impact on early outcomes in contemporary ACS practice remains uncertain. The association between intravenous magnesium administration and early mortality and arrhythmia incidence in patients with ACS was evaluated. A final cohort of 68 patients admitted in 2025 was studied. 31 received intravenous magnesium, and 37 did not at the time of presentation to the hospital immediately after diagnosis, along with loading doses of antiplatelets and statins, which are usually given in patients with ACS. Primary outcomes were any arrhythmia during admission and mortality at 48 h. Statistical comparisons were performed using Fisher’s exact test. No deaths occurred within the first 24 h. Overall, 48-h mortality was 4.4% (3/68). Mortality occurred in 1 patient (3.2%) in the magnesium group and 2 patients (5.4%) in the non-magnesium group (odds ratio 0.58, P = 1.00). Any arrhythmia occurred in 20 patients (29.4%): 14/31 (45.2%) in the magnesium group versus 6/37 (16.2%) in the non-magnesium group (odds ratio 4.25, P = .012). Bradyarrhythmias were more frequent in the magnesium group (35.5% vs. 8.1%, P = .008), while VT/VF rates were low and not significantly different between groups. Early mortality in this ACS cohort was low and not significantly different between groups. Arrhythmias were more frequent in patients receiving magnesium, likely reflecting treatment of higher-risk individuals. Larger prospective studies are needed to clarify the role of magnesium in ACS.
Ashwini, Soumen Devdutta
Apollo Hospitals, Jubilee Hills, Hyderabad
Acute pulmonary thromboembolism (PTE) is a cardiovascular emergency with substantial morbidity and mortality, though real-world Indian data on its presentation, management, and outcomes are limited. This prospective observational study at a tertiary cardiac center (May 2024-April 2025) enrolled 50 adults with CTPA-confirmed acute PTE to evaluate clinical profiles, risk stratification, treatment approaches, and short-term outcomes via 1-, 3-, and 6-month follow-ups. Patients (mean age 48.6 ± 12.3 years; 64% male) primarily presented with dyspnea (88%) and chest pain (56%), stratified as submassive (42%), low-risk (40%), and massive (18%); management included DOACs (40%), systemic thrombolysis (24%), LMWH (28%), UFH (12%), and catheter/surgical interventions (14%). In-hospital mortality was 8% and 4% had major bleeding, while 6-month follow-up showed residual pulmonary hypertension in 13.3%, post-PE syndrome in 22.2%, recurrence in 4.3%, and mortality in 2.2%, emphasizing that early recognition, risk-stratified therapy, and structured surveillance optimize outcomes and mitigate long-term sequelae.
Anthati Kirti, Rajeev Garg
Apollo Hospitals, Hyderguda
Lipoprotein(a) [Lp(a)], a genetically determined lipoprotein, serves as an independent risk factor for atherosclerotic cardiovascular disease (ASCVD), contributing to residual CV risk despite optimal LDL-C lowering and associating strongly with premature acute coronary syndrome (ACS) events. This retrospective observational analysis of a real-world Indian cohort with available Lp(a) measurements characterized its distribution, variability, prevalence of clinically elevated levels (≥50 mg/dL), and associations with traditional risk factors, including diabetes mellitus, hypertension, and smoking, alongside premature ACS history. Results revealed wide inter-individual Lp(a) variability with frequent elevations in both ACS patients and event-free individuals, often coexisting with modifiable risks, underscoring Lp(a) as a distinct marker of residual risk and highlighting the need for routine screening to enhance CV risk stratification in Indian clinical practice.
Manas Gundala, Bharat Reddy K., Lakshmi Prasanna, Pankaj Jariwala
Yashoda Hospitals, Somajiguda
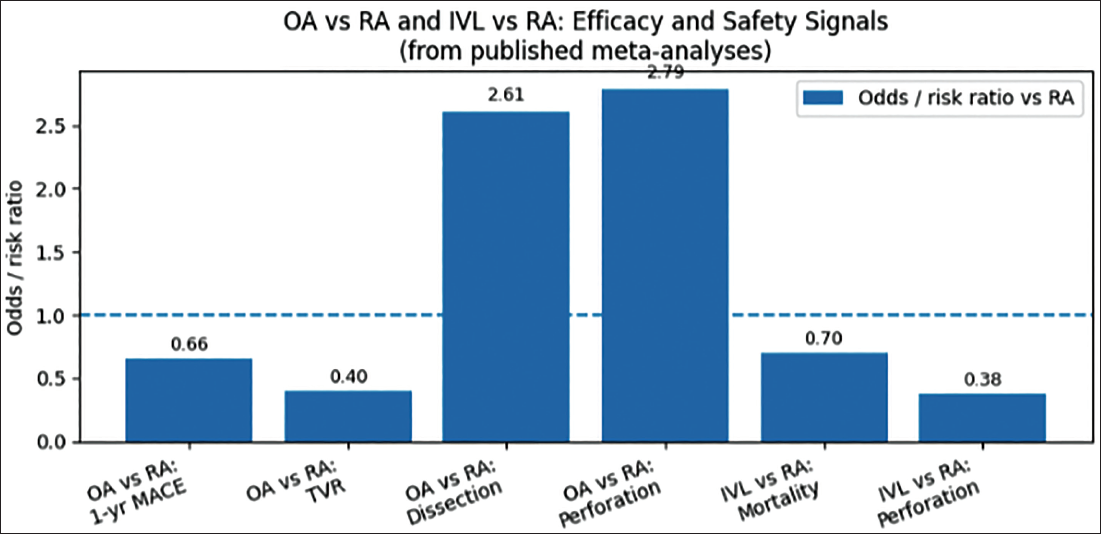
Severe coronary calcification remains a major challenge in percutaneous coronary intervention (PCI), predisposing to stent underexpansion and adverse outcomes. Rotational atherectomy (RA), orbital atherectomy (OA), and intravascular lithotripsy (IVL) are key calcium-modification strategies, but comparative long-term data are limited. We aim to systematically compare atherectomy (RA and/or OA) versus IVL in patients undergoing PCI for moderate-to-severe calcified coronary lesions, focusing on ≥12-month clinical outcomes and differences between RA and OA. A comprehensive search of major databases and trial registries up to December 2025, including randomized and comparative observational studies, with independent study selection, data extraction, and risk-of-bias assessment, was conducted. The primary endpoint was major adverse cardiovascular events (MACE), with secondary endpoints including mortality, target lesion/vessel revascularization, stent thrombosis, and procedural outcomes. Random-effects meta-analyses with subgroup and sensitivity analyses, and network meta-analyses where feasible, were performed. Existing evidence suggests higher long-term MACE and mortality with RA compared with non-RA PCI, while OA may reduce 1-year MACE and revascularization at the expense of higher procedural complications (Figure 1). IVL demonstrates higher procedural success and lower perforation risk compared with RA, with similar follow-up clinical outcomes. This study provided an integrated assessment of calcium-modification strategies to guide optimal device selection in complex calcified coronary lesions.
Odds/Risk Ratios for Key Efficacy (MACE, TVR) and Safety (Dissection, Perforation, Mortality) Outcomes Comparing Orbital Atherectomy and Intravascular Lithotripsy Versus Rotational Atherectomy, Based on Published Meta-Analyses.
Bharat Reddy K., Manas Gundala, Lakshmi Prasanna, Pankaj Jariwala
Yashoda Hospitals, Somajiguda, Hyderabad
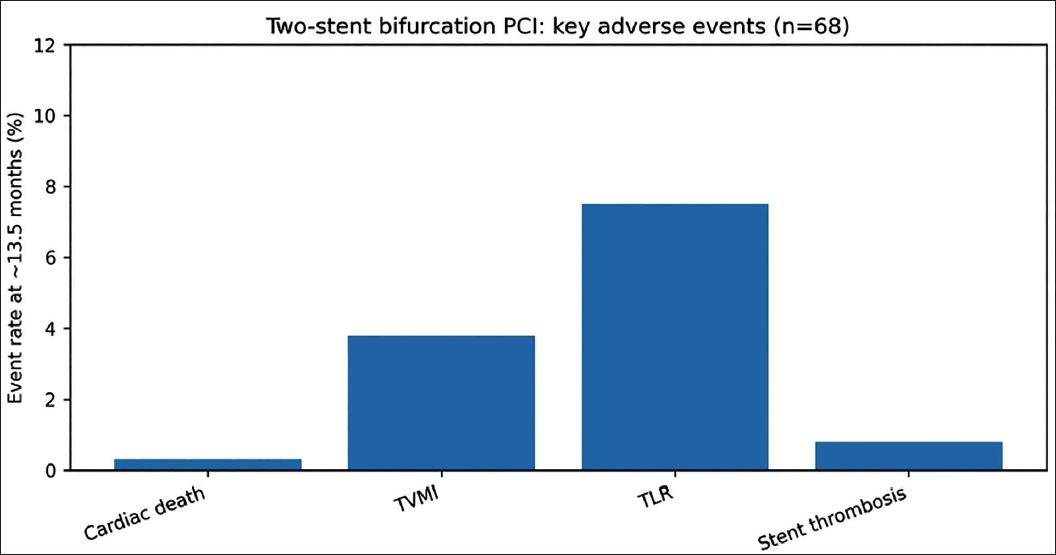
Two-stent bifurcation percutaneous coronary intervention (PCI) is typically reserved for complex anatomy and remains technically demanding; however, contemporary optimization strategies such as proximal optimization technique (POT) and final kissing balloon (FKB) may improve outcomes. We conducted a single-center retrospective registry of 68 consecutive patients undergoing planned two-stent PCI for coronary bifurcation lesions, predominantly in an elective setting, to evaluate mid-term outcomes and predictors of target lesion failure (TLF). The cohort had a mean age of 61.4 ± 11 years with male predominance, and T and protrusion (TAP) was the most frequently used technique (81.3%), followed by DK-crush, culotte, and mini-crush. Optimization rates were high (POT 96.5%, FKB 96.3%), with a procedural success of 100%. At a median follow-up of 13.5 months, TLF occurred in 6.8%, driven mainly by target lesion revascularization (7.5%) and target vessel myocardial infarction (3.8%), while cardiac death was rare (0.3%) (Figure 2). Definite or probable stent thrombosis occurred in 0.8%. Independent predictors of TLF included bifurcation angle >90°, side-branch reference diameter ≤2.5 mm, main-branch lesion length ≥25 mm, and presence of main-branch calcification. In this contemporary cohort with near-universal optimization, two-stent bifurcation PCI demonstrated high procedural success and low mid-term TLF, with anatomic complexity remaining the primary determinant of adverse outcomes.
Key Adverse Effects of Two Stent Bifurcation PCI.
Bharat Reddy K., Manas Gundala, Lakshmi Prasanna, Pankaj Jariwala
Yashoda Hospitals, Somajiguda, Hyderabad
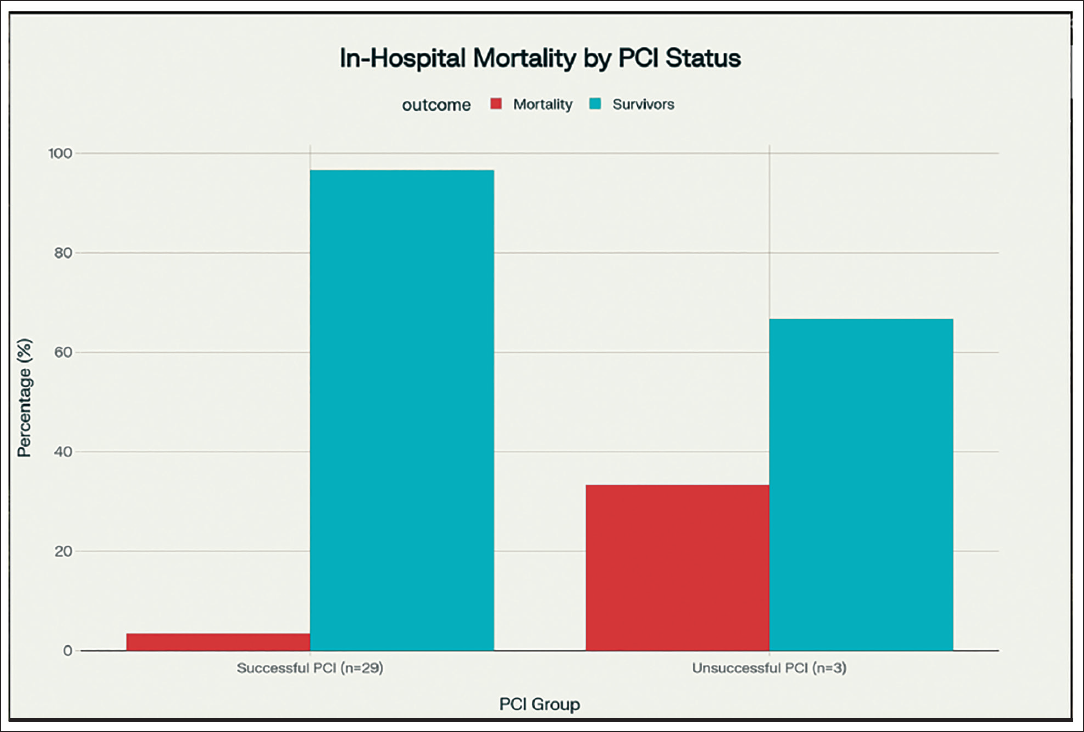
This retrospective study analyzed 32 post-CABG patients presenting with acute coronary syndrome (ACS) secondary to saphenous vein graft (SVG) occlusion to evaluate clinical outcomes and predictors of mortality. The cohort (mean age 66.7 ± 8.8 years; 84.4% male) presented primarily with NSTEMI (46.9%) and unstable angina (43.8%), with STEMI occurring in 9.4% of cases. Percutaneous coronary intervention (PCI) was successful in 90.6% of patients, resulting in an overall in-hospital mortality rate of 6.2%. Notably, unsuccessful PCI was significantly associated with a marked increase in in-hospital mortality compared to successful revascularization (33.3% vs. 3.4%, P < .05) (Figure 3). At 6-month follow-up, 6.7% of discharged patients experienced stent thrombosis. These findings underscore that successful PCI is a critical determinant of improved in-hospital outcomes in the high-risk SVG-ACS population, though larger studies are necessary to further elucidate risk variables and optimize therapeutic strategies.
Clinical Outcomes and 30-day Follow-Up in Post-CABG ACS Patients. This Multi-Panel Figure Illustrates the Key Clinical Outcomes of 32 Patients with Acute Coronary Syndrome After Coronary Artery Bypass Grafting (CABG). The Grouped Bar Chart Compares In-hospital Mortality Rates Between Patients Who Underwent Successful Percutaneous Coronary Intervention (PCI) (3.4%) and those Who Underwent Unsuccessful PCI (33.3%). The Sample Sizes are Indicated for Each Subgroup. Abbreviations: ACS, acute coronary syndrome; CABG, coronary artery bypass grafting; PCI, percutaneous coronary intervention.
Manas Gundala, Bharat Reddy K., Lakshmi Prasabnna, Pankaj Jariwala
Yashoda Hospitals, Somajiguda, Hyderabad
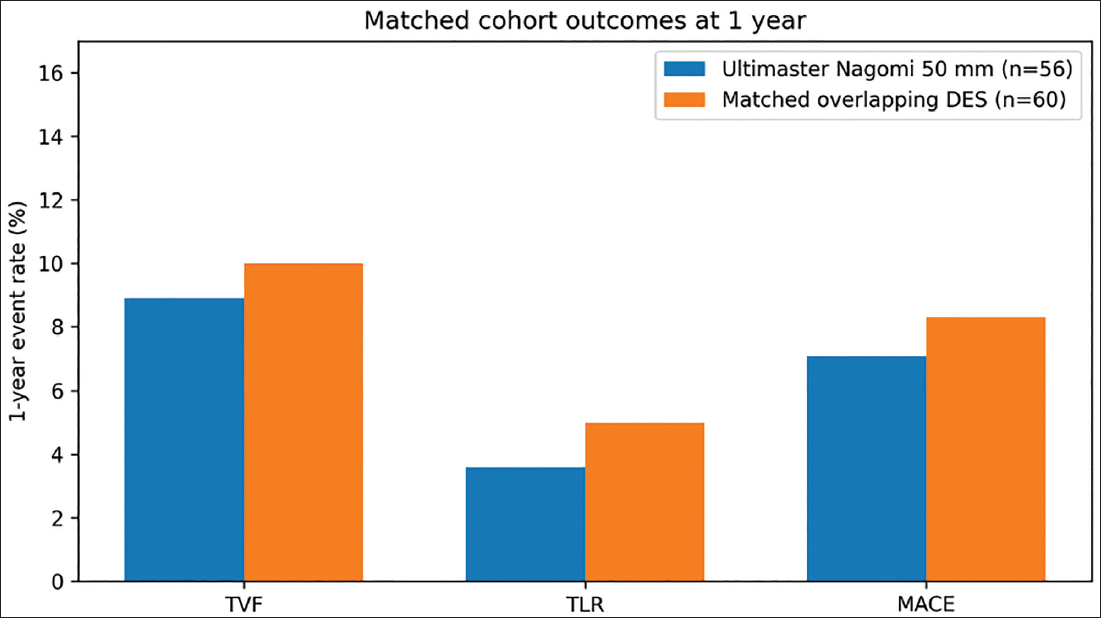
This study evaluated the 1-year clinical outcomes of a single 50-mm Ultimaster Nagomi drug-eluting stent (DES) compared to a propensity-matched cohort treated with overlapping contemporary DES for long, diffuse coronary lesions. Utilizing an all-comers registry between 2023 and 2024, the analysis compared 56 Nagomi cases against 60 matched controls treated predominantly with two or three overlapping stents (XIENCE, Onyx Frontier, or SYNERGY) in high-complexity scenarios, including STEMI (38.7%) and calcified lesions (33.6%). At 1-year follow-up, the primary endpoint of target-vessel failure (TVF) occurred in 8.9% of the Nagomi group versus 10.0% in the control group (OR 0.88, 95% CI 0.25-3.07; P = 1.00), successfully meeting the prespecified 10% non-inferiority margin with an absolute risk difference of −1.1%. Secondary endpoints, including target lesion revascularization (3.6% vs. 5.0%) and MACE (7.1% vs. 8.3%), further demonstrated clinical parity between the two strategies (Figure 4). These findings suggest that a single-stent strategy using the 50-mm Ultimaster Nagomi effectively simplifies long-lesion percutaneous coronary intervention (PCI) by reducing metal burden and procedural complexity without compromising safety or efficacy.
Matched Outcomes of the Cohort Comparing Ultimaster Nagomi 50 mm Stent and Matched Overlapping DES.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Not applicable.