
Abstract
Background:
Hypertensive disorders of pregnancy (HDP), including gestational hypertension and preeclampsia, increase risk of acute complications, later development of hypertension and coronary artery disease and maternal mortality. Prenatal physical activity (PPA) reduces the risk of HDP development. Obstetric care providers (OCPs) are crucial in advising patients on safe PPA. Despite the belief among OCPs in other developed countries that PPA is beneficial, few are familiar with endorsed guidelines or discuss PPA with their patients.
Objectives:
This study aimed to explore what a subset of OCPs based in Southwestern Ontario believe, know and practice with respect to PPA and its endorsement for HDP prevention.
Design:
Virtual, qualitative interview-based study.
Methods:
Semi-structured virtual interviews were conducted with nurse practitioners (n = 2; 39.5 ± 4.9 (X ± SD) years of age) and midwives (n = 4; 39.5 ± 7.3 years of age) who were actively practising in Southwestern Ontario.
Results:
Four overarching themes were identified using reflexive thematic analysis: (1) Restricted Scope of PPA Practice for HDP, (2) PPA is Very Important for Health in and Beyond Pregnancy, (3) PPA is a Highly Individualized Patient Experience and (4) Lack of Training in PPA Among Providers. All participants strongly affirmed the benefits and importance of PPA in general, despite constraints imposed by referral protocols for those with HDP. This belief stemmed from experience, knowledge of Canadian PPA guidelines and evidence-based literature. PPA recommendations were individualized yet grounded in national guidelines. Participants identified a gap in PPA training and provided suggestions for improvement.
Conclusion:
PPA participation may assist in the prevention or management of HDP and promote comprehensive wellbeing for patients. Further exploration of OCP recommendation and patient uptake of PPA for HDP within a Southwestern Ontarian context and beyond is warranted.
Keywords
Introduction
Affecting nearly 7% of pregnant women in Canada, hypertensive disorders of pregnancy (HDP) are associated with potentially severe, even fatal, complications for both mother and neonate.1–5 HDP such as gestational hypertension (GH) and preeclampsia (PE) have also been identified as a significant risk factor for the development of chronic hypertension and coronary artery disease later in life.6,7
Physical activity (PA) is recommended during pregnancy in most cases and reduces the risk of developing GH or PE by 40%–60%.8,9 The 2019 Canadian Guideline for Physical Activity Throughout Pregnancy (the Guideline) is the current gold standard for prenatal physical activity (PPA) recommendations across Canada. 10 The Guideline 10 recommends that pregnant women should remain active throughout their pregnancy if they are not experiencing medical contraindications. Specifically, to accumulate health benefits, pregnant women are encouraged to participate in at least 150 total minutes of moderate-intensity PPA per week across three or more days in bouts of ten minutes or greater. Optimal health benefits are incurred by incorporating both aerobic and resistance training into a PPA routine. The Guideline 10 currently lists GH as a relative contraindication to exercise, requiring regular monitoring by an obstetric care provider (OCP). In contrast, PE is listed as an absolute contraindication to exercise.
In the United States, current evidence shows that upwards of 90% of physicians believe that PPA is beneficial for pregnant women 11 ; however, it remains widely under-endorsed.11–13 This work indicated that nearly 75% of OCPs do not regularly discuss PPA with their pregnant patients, 13 and approximately half of physicians surveyed reported a lack of familiarity with United States PPA guidelines. 12 The knowledge, beliefs and endorsement of PPA within clinical practice by Canadian OCPs using the Guideline 10 is under-studied. Furthermore, much of the previous work has been conducted primarily with general practitioners (GPs). Nurse practitioners (NPs) and midwives are typically able to spend more time with patients than GPs,14,15 and as such may be more amenable to PA discussion and promotion. Therefore, the purpose of this work was to explore, within Southwestern Ontario, what OCPs believe, know and practice with respect to PPA and its endorsement within clinical practice.
Methods
This study, approved by the University of Windsor’s Research Ethics Board, was conducted as a master’s thesis project using a relativist approach, through a constructionist viewpoint by the primary investigator (L.C.). During study conduction, L.C. was a female master’s student with a bachelor of science in kinesiology who was trained in qualitative interviewing and data analysis. She has not had any experience with obstetric care. Her educational background is in kinesiology with a particular interest and focus on cardiovascular health.
A qualitative, virtual interview-based study using Microsoft Teams® video calls was conducted with a sample of OCPs. To be eligible, the inclusion criteria required participants to be certified GPs, NPs, midwives or physician’s assistants practising in Canada, who provided obstetric care. Exclusion criteria included any individual who was not a certified GP, NP, midwife or physician’s assistant, who did not practice in Canada, or who did not provide obstetric care. Recruitment efforts were conducted nationally whereby 149 clinics across Canada were contacted via email or telephone (if no email). The objectives of the study were outlined, and a request was made to distribute recruitment materials. Interested participants contacted investigators via email. Six interested and potentially eligible participants contacted the primary investigator. Eligibility was confirmed in all six participants, and they were emailed the Letter of Information, Audio/Video Consent Form and Project Consent Form.
Demographic and contact information were collected via an online survey tool (Qualtrics®) before the interview. Survey data were collected and stored on the Qualtrics® server, downloaded onto a Microsoft Excel® spreadsheet and the participant email was deleted. De-identified survey data were saved to a password-protected laboratory computer and external hard drive.
Virtual interviews were then scheduled with the primary investigator and conducted from a university laboratory computer. All participants provided verbal informed consent at the start of the interview. No additional researchers or other individuals were present during the interviews. A semi-structured interview guide consisting of nine open-ended questions was used to facilitate the interviews and allow participants to lead the conversation as appropriate (Supplemental Appendix A).16,17 The interview guide was first reviewed by four third-party individuals to ensure completeness and clarity. A pilot interview was then conducted with a medical student at the University of Windsor to ensure the questions were understandable by someone in the medical field. No data were kept from this pilot interview. The interview guide was then finalized by the primary investigator in collaboration with two qualitative experts and one additional researcher at the University of Windsor.
At the beginning of the interview, verbal informed consent to participate in the study was attained by the primary investigator after reviewing study information and procedures with the participant and affording the participant an opportunity to ask questions. Participant identity was then confirmed by verifying their age, gender and province of practice provided in the Qualtrics® survey. Following identity confirmation, audio recording was initiated and three introductory questions were asked to help build rapport between the participant and the primary investigator. 16 For example: ‘Please tell me briefly about your experience with your academic and professional training background’. Participants were aware of the primary investigator’s name, educational institution and role as a student prior to their interview.
Next, participants were asked five main questions: two focusing on their beliefs, two on their knowledge and one on their practices regarding PPA. A final closing question was included to provide participants with an opportunity to ask questions or add additional information they felt was important. 16 Prompts and follow-up questions were used as needed by the primary investigator to elicit further detail or clarification in responses. 16 Interview duration ranged from 30 to 60 minutes, and all interviews were completed within a three week period. No repeat interviews were conducted. Participants were emailed a $20 e-Gift Card as remuneration for their time and effort.
Interview recordings were reviewed, manually transcribed, and de-identified by the primary investigator on Microsoft Word®.18,19 Given that the primary investigator’s lived experiences shape qualitative data interpretation, prioritizing reflexivity to ensure consistency and accountability was important in the research process.17,19–22 A reflexive journal which noted the primary investigator’s interpretations of interview data was kept and used during data analysis as appropriate.17,19–22 Participants were given the option of member checking to review their transcript and make any necessary changes within two weeks after their interview, thus adding another layer of reflexivity. 17 De-identified audio recordings were stored on the recording device in a locked laboratory for two weeks post-interview, then deleted. Following this, de-identified transcripts were analyzed. De-identified transcripts were saved to a password-protected laboratory computer and external hard drive.
Using Braun and Clarke’s reflexive thematic analysis (RTA) approach, de-identified transcripts were analyzed continuously by the primary investigator as data were collected.16,18,19 The RTA process was initiated for each transcript following completion (n = 4) or opt-out (n = 2) of the member-checking process.16–19 An inductive approach to RTA was utilized for all data, as recommended for qualitative research topics with limited prior exploration or evidence.17,18,23 Interpretive judgement regarding the exploratory nature of the study, depth and richness of data relevant to the research question and the ability of the data to form a clear and compelling story was used to gauge sufficient information power. Braun and Clarke do not recommend the use of theoretical data saturation for the RTA approach.24–26
Data were analyzed using a series of six phases beginning with generation of specific codes, and ending with broader, overarching themes. 19 In phase one, the primary investigator familiarized herself with the data by listening to and manually transcribing each interview recording on Microsoft Word®. This was followed by re-reading the completed transcript and noting initial thoughts which stood out in a reflexive journal kept in a separate Word® document.
For phase two, codes were generated by methodically reviewing each transcript line by line. Meaningful sets of words or sentences were condensed within the context of interview discussion. These were denoted as comments linked to the relevant line of the transcript on Word® to form a list of codes representing data which related to the research question.
In phase three, potential sub-themes were identified by first compiling the list of codes for the entire data set into the organizational qualitative data software Dedoose©. Related codes were moved dynamically within this application to compare, combine and categorize data into potential sub-themes which were finalized in phase four.
Overarching themes were produced in phase four through a fluid process in which sub-themes were continually revisited, compared with one another, and re-defined as necessary within Dedoose©, until all codes were organized into a set of coherent inter-related sub-themes. During this process, closely related sub-themes were collapsed until a clear pattern within the data was formed by the remaining nine sub-themes. The final four themes were produced from distinct meanings supported by the way in which the final set of nine sub-themes fit together to answer the research question by telling a comprehensive story through the data.
To define and name these four overarching themes within phase five, succinct descriptors were used for each overarching theme. The nine finalized sub-themes were moved from Dedoose© to Microsoft PowerPoint® and organized as a list. Using this list, closely related sub-themes were reviewed together in the context of interview discussion to create a name which encompassed their overall meaning and fit within the data set. Each name was refined to provide a brief descriptor of the core meaning of each theme, and to allow for a coherent flow between themes to present a snapshot into the flow of the story told by the data.
For the final phase, the report was produced to elaborate upon the story told by the data. Overarching themes were supported by participant quotations to provide a compelling picture of the story being told, as well as to relate themes back to the research question. Upon completion of data analysis, a reflexive conversation was held with a critical friend to challenge the primary investigator’s interpretations and descriptions of themes.16,17,19,22 The critical friend reviewed the overarching themes and how they were supported by related sub-themes and participant quotations. Using the code and sub-theme organization on the Word®, Dedoose© and PowerPoint® platforms as a foundation, the critical friend questioned the themes and sub-themes and sought clarification on their connection and justification as appropriate.
The critical friend was a woman who had experienced pregnancy, exercised throughout pregnancy and suffered pregnancy-related complications. Her academic expertise was in cardiovascular health, disease and exercise physiology. She has had no experience working in obstetric care or caring for pregnant patients. The need to consider alternate interpretations and thought processes put forward by the critical friend was essential to enhance the primary investigator’s understanding of the data.16–19,22 Upon study completion, results were posted to a university-based website provided to participants. Subsequent feedback was not received from participants. This study was conducted and reported in accordance with the COREQ statement, and was completed from March 2024 to October 2024. 27
Results
Six Southwestern Ontario-based OCPs (two NPs and four midwives) participated. There were no dropouts or refusal to participate. All participants were female and completed their education in Canada. The average age was 39.5 years for both NPs and midwives with standard deviations of 4.9 and 7.3 years, respectively. None of the participants had received formal exercise education. All but one participant indicated that they care or have cared for pregnant women with GH or PE. Participants’ scope of care for pregnant women ranged from prenatal interactions through postnatal care. Please see Table 1 for additional participant demographics, Table 2 for personal PA characteristics and Table 3 for contextualization of participant characteristics.
Participant demographic characteristics.

HDP, hypertensive disorders of pregnancy.
Participant personal PA characteristics.
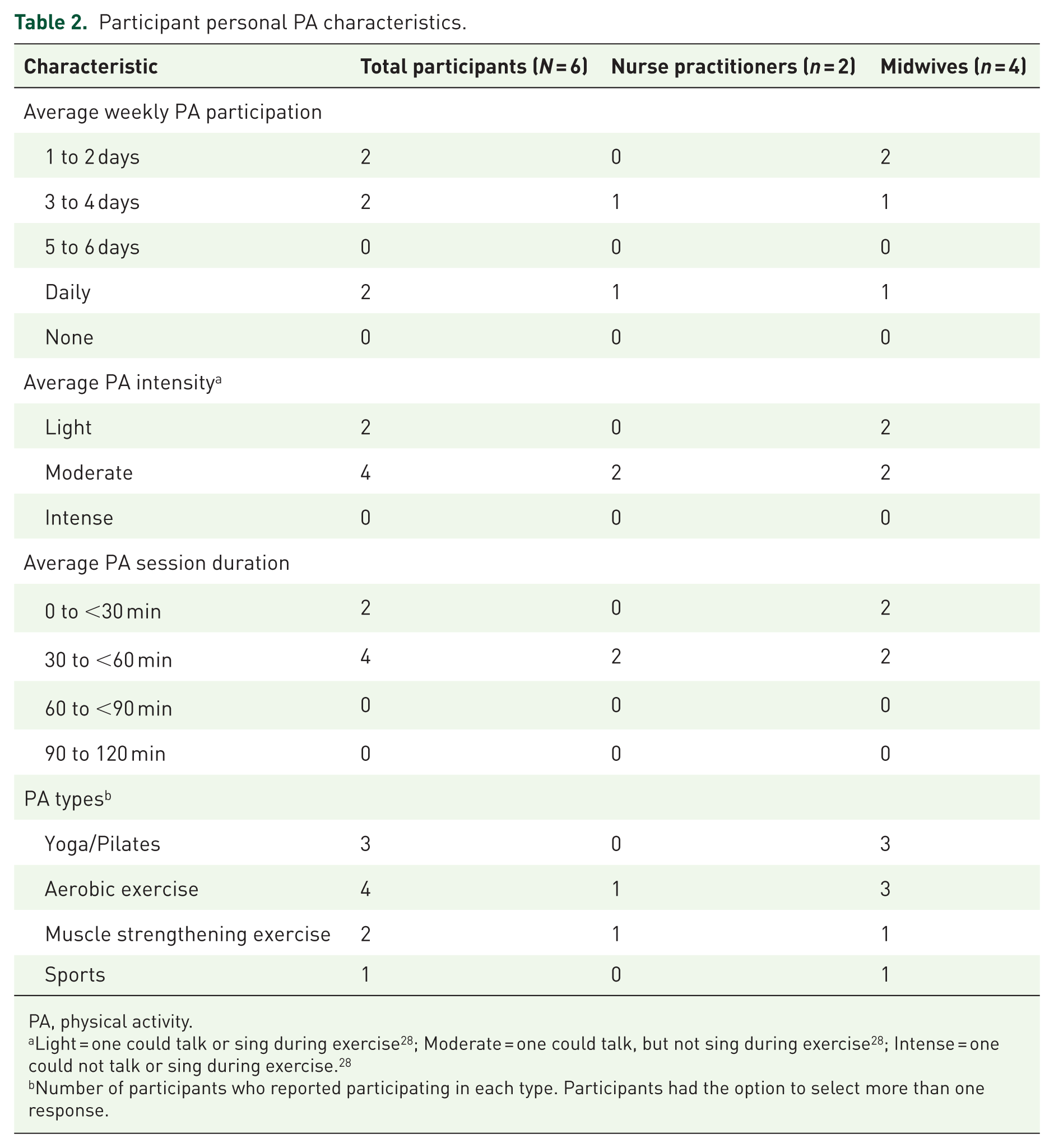
PA, physical activity.
Light = one could talk or sing during exercise 28 ; Moderate = one could talk, but not sing during exercise 28 ; Intense = one could not talk or sing during exercise. 28
Number of participants who reported participating in each type. Participants had the option to select more than one response.
Contextualization of participant characteristics.

Through rich, elaborative discussions with participants regarding their beliefs, knowledge and PPA practices, four overarching themes were generated. A visual representation of these themes and relationships between their sub-themes (depicted with arrows) is provided in Figure 1, with detailed findings outlined below. Participant quotes supporting each theme are provided in Table 4.

Flowchart of overarching themes and sub-themes.
Supporting quotes by theme and sub-theme.

HDP, hypertensive disorders of pregnancy; PPA, prenatal physical activity.
Theme 1: Restricted scope of PPA practice for HDP
This sample of OCPs displayed a restricted scope of PPA practice for patients with HDP. Protocols required referring patients to an obstetrician/gynecologist (OBGYN) for a higher level of care if they exhibited signs or symptoms of an HDP. This theme was described and supported by two sub-themes, the first of which focused on participants’ beliefs surrounding PPA for those with an HDP. Due to the nature of referral protocols, participant responses were varied when discussing these beliefs. For example, to illustrate their scope of practice, Participant 6 summarized, ‘We’re still involved, but once things become high risk, they’re out of the scope of midwifery and they’re on to specialized care with OBGYNs’. NPs expressed the same general practice. Participants further described what their own practice looks like when involving patients with an HDP (Q2, Table 4).
A positive viewpoint on the health benefits of PPA was still demonstrated in discussion particularly for patients with milder cases and with regard to cardiovascular disease (CVD) risk reduction later in life. Although referral protocols for high-risk cases limited their ability to prescribe PPA for patients experiencing HDP, the beliefs and knowledge of OCPs interviewed endorsed PPA for healthy individuals and those with mild symptoms (Q3, Table 4).
The second identified sub-theme considers participants’ general beliefs surrounding HDP. These OCPs commonly reported a gradient of beliefs regarding HDP, dependent upon their knowledge of the scale of disease severity. This was particularly evident in discussion of differences in beliefs surrounding GH and PE as separate entities. Regarding GH, Participant 5 reflected upon the difference she sees between GH and PE, and her belief on how PPA may still be beneficial to patients with GH (Q4, Table 4).
Concern was primarily expressed regarding PE which was believed by all participants to be significantly more severe than GH as a prenatal condition. When facing increasing PE severity, Participant 5 outlined her belief that these patients should not be exercising at all, ‘Preeclampsia is when you’re starting to have organ involvement, but if you’re at the upper end of that it can potentially get to have a seizure or stroke. . . I wouldn’t want those people exercising, so again it’s very individual’.
In addition to discussing severity, participants demonstrated an understanding of the physiology of HDP. Participant 6 noted that HDP function differently within the body than non-pregnancy related hypertension, and as such, she believed PPA was unlikely to be useful as a treatment adjunct (Q6, Table 4).
To summarize Theme 1, discussion with the OCPs sampled illustrated their limited scope of practice for patients with HDP. These conditions were usually considered higher risk and as such, primary care was transitioned to OBGYNs. The participants, however, displayed a strong level of knowledge and understanding of HDP. This knowledge is what informed their beliefs specifically regarding PPA in patients with an HDP, as well as their beliefs surrounding the conditions themselves.
Theme 2: PPA is very important for health in and beyond pregnancy
In contrast to discussion on HDP and PPA, the importance of PPA in general for health in and beyond pregnancy was very highly regarded among all participants. This theme was described and supported by two sub-themes, the first of which being participants’ general beliefs and knowledge surrounding PPA. The most common reason why participants believe that PPA is important to discuss with patients was summarized by Participant 2, ‘I include some discussion on physical activity in pretty much every single one of my appointments because it plays a role in absolutely everything from sleep to mental health to cardiovascular disease, to just health and development’.
Participants expressed that throughout the field it is common knowledge that regular PA confers great health benefits, including risk reduction for both mental and physical conditions. While these domains are not specific to pregnancy, the knowledge they displayed regarding the effects of PPA on health illustrated why participants believed and advocated strongly for its use. However, these OCPs noted that within their practice, patients are not always certain what kinds of PPA they are capable of or should be doing. As such, participants expressed the belief that their discussions with patients are the first step towards such improvements (Q8, Table 4).
Participants’ knowledge of the health benefits of PPA led to very little resistance against its use among pregnant women. Aside from extreme circumstances or high-risk conditions such as placenta previa or severe PE, every OCP interviewed was comfortable with recommending PPA in their practice. Simply put by Participant 6, ‘In a low-risk healthy pregnancy, there’s no reason why you can’t be exercising’.
The second sub-theme identified elaborates on participants’ beliefs and knowledge, specifically regarding health benefits of PPA. It became evident through discussion that all OCPs in the study possessed a strong belief in PPA as a healthy lifestyle modification for pregnant individuals. The primary reason for this belief was participant knowledge on the variety of benefits conferred on patients, the developing fetus and the friends and family of the patients. Significant emphasis was most often placed on direct benefits to the patient (Q10, Table 4).
Collectively, participants were knowledgeable about the positive effects PPA has upon physical and mental health, as well as risk-reduction, as evidenced in the literature. Physical health benefits cited by participants included increased energy, a reduction in musculoskeletal (MSK) aches and pains and improved mobility. Mental health benefits included decreases in anxious and depressive thoughts and feelings particularly with outdoor PPA. Pregnancy-related benefits included improved labour efficiency and a reduced risk of developing HDP and gestational diabetes, as well as CVD later in life. Their knowledge on the reduced risk of pregnancy complications led participants to express the belief that PPA also provides advantages to the developing fetus with respect to safety and efficiency during labour and birth. Much of this benefit was believed to be related to fetal positioning (Q11, Table 4).
Better coping was also suggested as a mental health benefit of PPA for the patient (Q11, Table 4). While no specific examples were given, Participant 5 described how physically active individuals were overall better able to cope with the stress, exhaustion and increased demands of labour and childbirth. In addition, Participant 3 shared a detailed perspective on how PPA benefits extended to friends and family of the active individual (Q12, Table 4).
To summarize Theme 2, all participants demonstrated strong knowledge of PPA and endorsed its positive impact on maternal health. This belief also extended to the developing fetus and individuals close to the patient both during and post-pregnancy. While participants were familiar with evidence-based literature, their knowledge came primarily from experiences within their own practice. These experiences informed their beliefs and knowledge surrounding the safety and benefits of PPA.
Theme 3: PPA is a highly individualized patient experience
This sample of OCPs commonly believed that PPA should be tailored to the individual needs of each patient. This theme was described and supported by three sub-themes, the first being characteristics of participants’ PPA practices. Notably, participants did not like the use of specific language such as ‘prescription’ when referring to their practices. Due to the individualized nature of the patients as well as their experiences with pregnancy and general PA, ‘prescription’ was commonly replaced with ‘discussion’ and ‘recommendations’. When asked to elaborate upon how they might prescribe PPA, all participants responded similarly (Q13, Table 4).
While each OCP incorporated recommendations in their practice based on their knowledge of the Guideline, 10 none prescribed a specific PPA routine to follow. If a patient was already active, participants generally advised continuation of PA throughout pregnancy with few exceptions. As stated by Participant 2, ‘I usually start by asking them what they’ve currently been doing outside of pregnancy and then counsel them on continuing that activity with very few exceptions throughout the pregnancy, unless any risk factors develop’. Participants identified risk factors such as severe PE or placenta previa as justification for advising patients to reduce or discontinue PPA. PA with a high risk of fall or abdominal impact such as contact sports, extreme sports and martial arts, were also discouraged due to safety risks.
Although participants did not ‘prescribe’ specific PPA routines, recommendations discussed with patients in their practice were personally tailored. More commonly recommended PPA habits tended to be similar though not specific to Guideline 10 recommendations. For these OCPs, PPA is about frequent movement and a broad, inclusive plan rather than a regimen to be followed (Q15, Table 4).
The second sub-theme revolves around characteristics of the pregnant women themselves. Interestingly, the OCPs sampled described much of the patient population in their practice as already being fairly active, or at least interested in PPA, by the time they received care. As such, PPA discussions in participants’ practice were often patient-initiated and led (Q16, Table 4).
In some communities, familiarity with and interest in PPA in an OCP’s practice may have been impacted by the average socioeconomic status of the population (Q17, Table 4). However, sometimes patients still had concerns around PPA. Some of the most frequent concerns heard by participants stem from uncertainty around what types or how much PA is safe during pregnancy, and experience with patronizing commentary (Q18, Table 4).
This topic leads into the third sub-theme: Challenges or barriers which may preclude participation in PPA. Such challenges tended to span a wide variety and scale of obstacles which differ between patients and may change over the course of pregnancy. For individuals who have not previously been active, discontinue PPA, or are not interested at all, OCPs were of the belief that one or more of many factors could be involved (Q19, Table 4).
In some cases, participants believed that an inability to incorporate PPA into one’s lifestyle could be solely due to a lack of willingness to try or continue PPA. While these OCPs still expressed a strong belief in the importance of PPA conversations, they also understood when barriers existed to make this less feasible (Q20, Table 4). Though many challenges to PPA expressed by patients in participants’ practice could be mitigated. Most commonly, these concerns surrounded physical changes that tend to come with pregnancy itself regardless of health status. Thus, participants typically encouraged patients to practice small amounts of PPA whenever possible until their strength and energy improved (Q21, Table 4). This type of recommendation was a common thread in participants’ practice, focusing on breaking PPA into smaller, more manageable bouts. However, participants agreed that any activity which causes pain or discomfort should be discontinued or modified in collaboration with one’s OCP.
To summarize Theme 3, participants unanimously illustrated the belief that PPA is a highly individualized patient experience due to a variety of intertwining factors. This theme was supported by three sub-themes which described these OCPs’ experiences with patients in their practice. Characteristics of the PPA practices themselves were provided in conjunction with descriptions of the patient populations served and the challenges to patient participation in PPA.
Theme 4: Lack of training in PPA among providers
Most participants expressed concern over what was described as a lack of training surrounding PPA among OCPs. This concern was primarily expressed in discussion on how OCP knowledge and practices of PPA endorsement within clinical practice might be improved. This theme was described and supported by two sub-themes, the first of which involved improving PPA knowledge among OCPs. Improved training during school and continued professional education were the most commonly recommended strategies to improve knowledge (Q22, Table 4).
Aside from improving the education system, participants noted that in many cases, they expanded their knowledge on their own time. This was most often triggered by patients in their practice initiating a conversation, asking questions, or expressing concerns about topics with which these OCPs were not familiar. Participant 5 suggested improving OCP knowledge through information brought into their practice by patients, ‘Probably social media campaigns are the biggest or something that gets picked up by the news. Because if we haven’t heard of it, clients will have, and then they come in and they ask about it’.
However, one participant did not express dissatisfaction with the foundational knowledge among OCPs in her practice. Thus, it is equally important to note that while a need for knowledge improvements among OCPs appears to be necessary based on current evidence, there may not be a complete deficit across all practices (Q24, Table 4).
The second sub-theme expanded upon recommendations specific to informing current practices of PPA discussion and recommendation. Many participants believed that educational sessions from researchers knowledgeable on gold standard PPA practices and their impact on pregnancy would be extremely beneficial for informing and inspiring practice. Participant 6 expressed interest in this idea, ‘If you started just even a talk or a workshop or started the bare basics and educating them, people would definitely sign up and come and watch you. . . Every workshop or event that comes up I’m like oh, there’s a gap, let’s fill it’. Another strategy suggested by participants to inform current PPA practices involved distribution of this information directly to OCPs (Q26, Table 4).
Finally, the benefits of having access to multiple OCPs within the same practice were expressed as an advantage towards informing individual OCP’s practices. In this environment, knowledge is shared in discussion among several OCPs to fill in potential gaps in knowledge or practices. This was Participant 4’s experience, ‘We’ve also got a lot of healthcare providers in our practice. So, maybe the knowledge base here is a bit higher. . . So, it could be also just the place that I’m working in and the demographic of people that I work with’.
To summarize Theme 4, the majority of OCPs sampled experienced a lack of training surrounding PPA knowledge and practices. This was primarily apparent through their educational experiences prior to becoming OCPs. To mitigate or improve upon this identified gap in training, participants discussed strategies intended to enhance PPA knowledge, and practices of PPA discussion and recommendation. Resulting from these discussions was evidence of interest among participants in improving PPA knowledge and practices through one or more illustrated strategies.
Discussion
This work explored beliefs, knowledge and PPA endorsement practices among NPs and midwives to generate four overarching themes using RTA. With respect to the Restricted Scope of PPA Practice for HDP, these OCPs reported commonly referring patients with signs and symptoms of an HDP to a higher level of care with an OBGYN, as is common practice. 29 While participants are no longer the primary care provider for patients with an HDP, they are still involved in regular monitoring and follow-up. Thus, while final decisions regarding PPA would be made by an OBGYN, NPs and midwives may still discuss PPA with these patients albeit to a lesser degree. Since the care they provided was mostly follow-up, providing guidance on PPA for those with HDP was not common practice.
Additionally, beliefs among this sample of OCPs regarding the potential role of PPA as a treatment adjunct for HDP was varied based on perceived disease severity. The belief that PPA may still be beneficial for those with milder forms of HDP, and that PPA becomes contraindicated with greater disease severity aligns with Guideline 10 recommendations.
With a milder form of an HDP, particularly GH, participants were more inclined to continue encouraging them to remain active, though not at a high level of exertion. This is supported by Guideline 10 recommendations for GH. A recent systematic review by Meah et al. supports the use of PPA for health benefits in individuals with GH. 30 Evidence from this systematic review suggests that PPA recommended in the Guideline 10 confers health benefits to women experiencing GH, without incurring undue risk or contributing to pregnancy-related complications. 30 Taken together, this supports participants’ inclination to advise PPA for their patients with milder forms of HDP such as GH.
Historically, PPA minimization or bedrest have been recommended to preserve health when diagnosed with an HDP.30–33 Some evidence indicates that OCPs who are unfamiliar or uncomfortable with PPA are more likely to recommend restricted activity or not discuss PPA with these individuals.11–13,34 While the Guideline 10 recommends considerable caution and PPA modification in accordance with an OCP, current study responses reflect beliefs that depending on the clinical profile of the HDP, bedrest may not be necessary, or beneficial.30,32,33 Current evidence indicates that risks to maternal and fetal health associated with PPA increase concomitantly with the HDP severity, specifically PE.10,30,35 Knowledge of health risks in high-risk patients was reflected in concern displayed by participants regarding patients with severe PE participating in PPA. Thus, while these OCPs believe PPA should be performed by most pregnant women, this belief is highly dependent upon HDP severity.
Regarding PPA being Very Important for Health in and Beyond Pregnancy, findings of the current study reflect a high standard of belief in the ability of PPA to positively impact the health and wellness of the pregnant woman, fetus and others around them. These results support work exploring OCPs’ beliefs, knowledge and PPA practices in other developed countries such as the United States and Australia which found that most OCPs surveyed believed that PPA was beneficial for health and reducing complication risks in pregnancy.11–13,34
OCPs were familiar with evidence-based literature on the role of PPA in reducing the risk of HDP development. This knowledge of PPA-related reductions to the risk of pregnancy complications and development of CVD later in life was reflected in their beliefs in its long-term health benefits for those with or without HDP. Much of participants’ beliefs and knowledge on pregnancy and postpartum health benefits arose from professional experiences within their practice. All participants regularly incorporated PA into their personal lives as well, adding another layer of familiarity to the practice of PPA endorsement. Professionally, these discussions were supported by their general knowledge of academic literature reporting PPA-induced mental and physical health benefits.10,35–37 D’Angelo et al. acknowledge that provider advice reflects a combination of professional experience gained from previous patient encounters and evidence-based knowledge. 38
Several maternal health benefits of PPA reported by OCPs in this study mirrored findings from previous research. These included physical health benefits such as increased energy and stamina, a reduction in MSK aches and pains, improved strength and mobility and improved labour efficiency.10,35–37,39–41 Mental health benefits, particularly when exercising outdoors, included the decreased severity of anxious and depressive thoughts and feelings.10,37,42 Participants also described active patients as being better able to cope with labour and childbirth. In line with this, Barakat et al. found that women who participated in moderate PPA three days per week for the last two trimesters of pregnancy had shorter labours than those who received only standard care. 40 Moreover, Davenport et al. provide meta-analytic evidence that following PPA recommended by the Guideline 10 may reduce the incidence of forceps or vacuum use during delivery. 41
With respect to the fetus, positional adjustment was the most strongly observed direct benefit of PPA by participants. Optimal in-utero position prior to labour reduces the risk of complications from breech positioning or shoulder dystocia, thus promoting a safer, more efficient labour and birth.43,44 Though drawn from participants’ experiences, these findings are in accordance with previous studies investigating the effects of PPA on fetal health.35,36,43,44
Translation of PA through a patient’s circle of loved ones was a novel finding which represented a broader view of the health benefits of PPA. As discussed by one participant, if pregnant patients involve their children in PA, this may mitigate sedentary behaviour risks. Brown et al. reinforce this from a family-based exercise intervention perspective in that a significant proportion of examined literature demonstrated increases in PA levels among children when the family was more active. 45
PPA recommendations were highly integrated in practice because of participants’ strong beliefs and knowledge regarding health benefits. This represents a divergence from previous research, which has shown that as few as 53% of obstetric patients received PPA advice from their OCP. 34 In the present study, every participant reported discussing PPA and its health benefits with all, or almost all, of their patients at least once. The topic of PPA was re-visited throughout their patients’ pregnancies. As such, the OCPs in the present study discuss and advise on PPA more frequently than what has been seen in previous work.
Participants of the present study reported the belief that their professional interactions were more amenable to PPA discussions with their patients. This perspective is reflected in recent work exploring the provider–patient relationships in NP and midwifery care models.14,15 From a wider perspective, OCPs play an integral role in enhancing patients’ understanding of their health, risk factors and disease management strategies.46,47 PPA is included here as an endorsed strategy in clinical practice guidelines for pregnant individuals.10,46 Participants believed that they could increase uptake among pregnant patients by frequently discussing PPA. It is plausible that participants’ high reported frequency and depth of PPA discussion in their practice may help to overcome perceived barriers to PA in their patients. Knowing that provider advice strongly impacts patients’ health behaviour,46,47 this may have had an influence.
With respect to PPA being a Highly Individualized Patient Experience, discussion with OCPs illustrated a concordance in PPA recommendation strategies. Participants unanimously believed language such as ‘prescription’ was restrictive when referring to PPA practices. Thus, recommendations were individually tailored and discussed with patients as opposed to being prescribed. In line with previous work by Sparks et al. nearly all surveyed women who were pregnant or had given birth in the past two years expressed that they were more likely to be active during pregnancy with an individualized exercise plan endorsed by their OCP. 48
All OCPs expressed general knowledge of Guideline 10 recommendations, including relative and absolute contraindications to exercise. A reduction in intensity in addition to discussion and monitoring by obstetric and primary care providers was an important part of participants’ PPA discussions with all patients but was more prominent for those with GH compared to those with PE. Notably, participants unanimously agreed, citing the Guideline, 10 that any activity which causes pain or discomfort should be discontinued or modified in collaboration with one’s OCP.
Most participants expressed some difficulty recalling exact parameters of the Guideline. 10 However, their advice was similar to specified Guideline recommendations. 10 In general, participants advised maintaining a low-to-moderate intensity, progressing towards 30 minutes of activity per day, 3-5 times per week. All participants also reported advising pregnant women to remain active throughout pregnancy as appropriate.
It was very common in participants’ practice for new patients to initiate the conversation about PPA. These OCPs believed that high PA levels prior to pregnancy among their patients were responsible for the frequency of patient-led PPA discussion, which is also seen in work exploring the effects of exercise habit formation. Rebar et al. has described a positive association between habitual exercise performance and increased likelihood of continued PA participation. 49 This supports speculation by OCPs that active patients were more likely to inquire about continuing PA during pregnancy.
Participants commonly inquired about the current PA habits of their patients and advised continuing activities with modifications as appropriate, with exceptions in high-risk cases, which are also supported in the literature.8,10,30,35,41 Other recommendations included splitting PPA into smaller sessions. Walking, yoga and swimming were the most frequently mentioned methods and have been suggested to be beneficial and easy to modify.10,12,30 Recommendations often began conservatively with the goal of achieving Guideline 10 recommendation levels, in addition to being specific to patients’ interests and familiarity with PA. This strategy supports patient adherence to PA.14,15,50 Participants of the current study also believed that suggesting lower levels of PPA with the goal of working up to Guideline 10 recommendations is effective in helping patients overcome challenges associated with physical changes in pregnancy.46,47
Study participants viewed their interactions with patients positively, expressing their belief that patient-led discussions lessened concern surrounding conflicting messages regarding PPA in cultural, social and media-related contexts. This account of patient attitudes towards seeking knowledge from their OCP suggests that patients view OCPs as a trusted source of information, further supporting research indicating providers’ influence on their patients.46,47 By empowering patients to lead health discussions, providers may foster trust, allowing their patients to feel more comfortable and receptive to lifestyle advice. 15
With respect to the Lack of Training in PPA Among Providers, one participant expressed adequate training, while most considered themselves to be insufficiently trained in PPA counselling, which aligns with work from other developed countries.11–13,34 Participants recommended incorporating PPA-related learning in early stages of professional training, to increase knowledge and improve PPA endorsement. While there seems to be a paucity in current Canadian research, academic institutions in the United States have implemented courses in lifestyle medicine coaching. 51 Overall, this coaching has been well received by students and is associated with improvements in their knowledge, satisfaction, coaching skills and interprofessional skills. 51
Strategies to enhance knowledge and PPA practices of current OCPs were also discussed. As with current literature demonstrating improvement in knowledge,11–13,52 participants recommended implementing seminars or workshops led by researchers with expertise in PPA and pregnancy. To reach OCPs who may be too busy or uninterested in education sessions, some participants recommended national distribution of informational materials. One example of this strategy is provider newsletters, which have been studied by Hohmann et al. 53 Approximately 80% of providers sampled believed resources in the study newsletter were adequately accessible sources of information. 53 One participant suggested spreading positive, factual information about pregnancy and PPA on social media and/or public news media. This has been successfully demonstrated in similar populations. 54 Such strategies may have the potential to directly improve patients’ knowledge on the safety and health benefits of PPA.
In summary, all OCPs strongly believed that PPA is very important for health during and beyond pregnancy, while taking HDP-related symptoms into consideration. They had in-depth discussions and recommended personally tailored PPA which was complimentary to the Guideline. 10 There was however a significant lack of PPA-related training across OCPs. Implementation of seminars, workshops, national resource distribution and sharing information through media channels may help to improve knowledge and inform PPA practice among OCPs in the future.
Strengths and limitations
The strengths of this study were its qualitative nature, and the data quality control. Using semi-structured interviews, participants were encouraged to share their beliefs, knowledge and experiences directly with the primary investigator. This strength of communication together with data being analyzed throughout the collection process, promoted acquisition of a rich data set and confidence in the acceptability of the final participant sample.16,17,19 Theoretical data saturation is not recommended for the RTA approach.24–26 As such, attainment of sufficient information power was considered using interpretive judgement with respect to the exploratory nature of the study, depth and richness of data relevant to the research question, and the ability of the data to form a clear and compelling story.24–26 With respect to data quality control, the reflexive approach to data analysis and the use of a critical friend to promote accountability are clear strengths of this work.17,19–21,22
Despite these strengths, there are limitations of this work. The virtual nature of interview conduction may have limited rapport-building and non-verbal cue recognition, potentially affecting the depth of data interpretation.16,17 We also acknowledge that selection bias and social desirability are fundamental limitations of this study. Despite national recruitment efforts, our response rate was very low. As such, those who did respond may have been more amenable to discussions around PA with their patients, a practice not reflective of broader patterns of poor familiarity and endorsement of clinical exercise guidelines. Generalizability of study findings is further limited by the inclusion of only two types of OCPs, NPs and midwives. The unequal distribution of OCP types also raises the possibility of sampling bias. This may have influenced captured perspectives, potentially skewing data toward views more commonly held by midwives. However, responses from both types of OCPs yielded similar results despite differing qualifications and responsibilities within their fields. This could be considered a strength; however, it is likely that only OCPs interested in PPA participated in this study, leading to the possibility of selection bias. Social desirability bias may also be present, with participants potentially overstating their support for or use of PPA in clinical practice. Furthermore, there was minimal variation among participants with respect to their demographic characteristics (i.e. all participants were female, physically active and practiced in Ontario) and thus, results may not be generalizable to NPs or midwives of other Canadian practices. Although we did not explore the socioeconomic backgrounds of our participants’ patients, data suggest that physicians are more likely to counsel patients to begin or continue with exercise the higher their income and current PA status, and if they are university graduates. 55 As it was noted within our participant sample that the patient population was ‘privileged’, it is plausible that our providers were more likely to endorse PA due to their demographic profile.
Future work should also expand the sample to encapsulate obstetric care across Canada by including OBGYNs, GPs and cardiologists, as well as physician’s assistants. It would also be important to note whether these OCPs have a foundational degree in kinesiology or exercise science to determine whether those with more PA education would be more familiar with PPA guidelines and/or more likely to recommend PPA. Evaluating the current educational curriculum and professional training opportunities for OCPs would also be an important consideration.
Conclusion
PPA participation may prevent or treat HDP and promote comprehensive well-being for patients. Further exploration of OCP recommendation and patient uptake of PPA for HDP within a Southwestern Ontarian context and beyond is warranted.
Supplemental Material
sj-docx-1-reh-10.1177_26334941261451342 – Supplemental material for Understanding providers’ beliefs, knowledge and practices of prenatal physical activity endorsement for the prevention and management of hypertensive disorders of pregnancy: a qualitative study
Supplemental material, sj-docx-1-reh-10.1177_26334941261451342 for Understanding providers’ beliefs, knowledge and practices of prenatal physical activity endorsement for the prevention and management of hypertensive disorders of pregnancy: a qualitative study by Lauren Ceman, Lana Milidrag, Cayla Brush, Kiara De Simone, Gabrielle Nguyen, Kendall Soucie, Todd Loughead and Cheri McGowan in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-2-reh-10.1177_26334941261451342 – Supplemental material for Understanding providers’ beliefs, knowledge and practices of prenatal physical activity endorsement for the prevention and management of hypertensive disorders of pregnancy: a qualitative study
Supplemental material, sj-docx-2-reh-10.1177_26334941261451342 for Understanding providers’ beliefs, knowledge and practices of prenatal physical activity endorsement for the prevention and management of hypertensive disorders of pregnancy: a qualitative study by Lauren Ceman, Lana Milidrag, Cayla Brush, Kiara De Simone, Gabrielle Nguyen, Kendall Soucie, Todd Loughead and Cheri McGowan in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-pdf-3-reh-10.1177_26334941261451342 – Supplemental material for Understanding providers’ beliefs, knowledge and practices of prenatal physical activity endorsement for the prevention and management of hypertensive disorders of pregnancy: a qualitative study
Supplemental material, sj-pdf-3-reh-10.1177_26334941261451342 for Understanding providers’ beliefs, knowledge and practices of prenatal physical activity endorsement for the prevention and management of hypertensive disorders of pregnancy: a qualitative study by Lauren Ceman, Lana Milidrag, Cayla Brush, Kiara De Simone, Gabrielle Nguyen, Kendall Soucie, Todd Loughead and Cheri McGowan in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
We would like to acknowledge the contributions of Arjuna Srikrishnaraj, Megan Bornais, Brooke Obermok, Anne McGowan, Alicia Dai and Regan Lane to this work. In addition, a special thanks to the participants who made this work possible.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.