
Abstract
Introduction:
Cardiovascular disease (CVD) is the leading cause of death in the United States, and women Veterans (WVs) face elevated risk due to traditional factors (hypertension (HTN), hyperlipidemia (HLD), obesity, diabetes, and smoking) and nontraditional factors (depression and post-traumatic stress disorder [PTSD]). Racial and ethnic disparities further affect their cardiovascular health. This study describes CVD prevalence, risk factors, and health behaviors among WVs to inform interventions.
Methods:
A cross-sectional survey was sent to 1,909 WVs receiving care at a VA Medical Center in California. Participants self-reported health behaviors, CVD diagnoses, and risk factors. The study was approved by the university and VA IRBs (IRB #24-42014).
Results:
Among 380 respondents (20% response rate; mean age 53), 58% were non-Hispanic White, 20% non-Hispanic Black, and 14% Hispanic. Common CVD risk factors were HLD (38%), obesity (36%), HTN (33%), smoking (13%), and diabetes (10%). Physical activity was low (vigorous activity 1.9 days/week) and diet suboptimal (score 6.1). Hazardous alcohol use was reported by 45.5%. Mean Patient Health Questionnaire 8-Item Scale and PC-PTSD-5 scores indicated moderate depression (8.7) and mild PTSD (2.9). Risk factors and mental health conditions were higher among WVs aged 18–44; nearly 70% reported ≥1 CVD risk factor. CVD prevalence peaked among those aged 65+.
Conclusions:
WVs in this sample demonstrated concerning CVD risk profiles, alongside a high prevalence of mental health conditions and hazardous alcohol use. Future research should examine social and environmental determinants and link survey data with clinical records to clarify behavior-disease relationships. Addressing both mental health and lifestyle factors is essential to reduce CVD risk and improve long-term health outcomes in WVs.
Introduction
Cardiovascular disease (CVD) has been the leading cause of death in the United States for over a century, 1 and women who have served in the military are at an increased risk. 2 Women Veterans (WVs) demonstrate a distinct cardiovascular profile compared with non-Veteran women. This elevated risk is due in part to a high prevalence of both traditional and non-traditional risk factors. 3 Hypertension (HTN), hyperlipidemia (HLD), tobacco use (e.g., cigarette smoking), obesity, and diabetes are well-established traditional risk factors for CVD. 4 Perhaps more concerning in this population is the prevalence of non-traditional risk factors, such as depression and post-traumatic stress disorder (PTSD). Compared to civilian women, WVs have higher rates of PTSD (7.7% vs. 13.4%) and depression (21.6% vs. 25.1%).5,6 Both PTSD and depression have been recognized as independent risk factors for CVD.7,8
Individual lifestyle and health behaviors can also contribute to CVD outcomes. Behaviors such as alcohol use and abuse, cigarette smoking, poor diet, and inadequate physical activity can impact cardiovascular health. 9 Further, Veterans have been known to demonstrate unhealthy behaviors at rates greater than their civilian counterparts. 10
Cigarette smoking and alcohol use
Cigarette smoking and excess alcohol consumption have both been linked to increased CVD risk and CVD outcomes. 11 Smoking and alcohol use are commonly reported among all Veterans and are often investigated side by side due to the co-occurrence of the two behaviors. 12 Both male Veterans and WVs have been shown to exhibit higher rates of alcohol abuse and cigarette smoking compared to civilians; however, estimates vary between these groups.13,14 One article that compared alcohol abuse and smoking in Veteran and non-Veteran men and women found that the overall estimated prevalence of alcohol use disorder among both WVs and civilian women was 4.8% (6.5% in male Veterans). 15 The same article reported that current smoking prevalence was 21.0% in WVs and 14.4% in civilian women (p < 0.0001) (16.4% in male Veterans). 15
Diet and physical activity
Diet and physical activity are linked to CVD outcomes directly and through confounders or modifiers such as obesity and HTN.9,16 Less than 1 in 4 American adults reportedly participate in adequate physical activity, and less than 10% meet daily guidelines for whole grain, fruit, and vegetable consumption. 17 Although physical fitness requirements exist for all military members, Veterans often experience significant declines in physical fitness after military service. 18 One study found similar rates of inactivity among WVs (26.3%) and civilian women (26.8%). 13 Another study reported diet quality among Veterans, using the Starting the Conversation survey tool. 19 Overall scores among men and WVs were similar (6.6 vs. 6.2, higher scores indicating worse diet), and factors such as worse depression symptom severity, lack of social support/someone to share meals with, and limited access to low-fat foods were all associated with worse diet. 20
Depression and post-traumatic stress disorder
Mental health factors are not only independent risk factors for CVD but may also lead to unhealthy behavior patterns.21,22 Both PTSD and depression are estimated to be more prevalent among WVs than civilian women.5,6 Depression is the most commonly diagnosed health condition among WVs aged 18–44 receiving care at Veterans Affairs clinics and medical centers (VA), 23 and has increasingly been linked to CVD, especially among young women. 22 Depression and PTSD have been linked to poor health behaviors, such as alcohol use, diet, physical activity, and tobacco use, 9 further contributing to CVD outcomes. Additionally, treatment for both PTSD and depression have been shown to improve morbidity and mortality in patients with established CVD.24,25
Though several studies have described the CVD risk profile of WVs, none have simultaneously characterized traditional CVD risk factors alongside health behaviors and mental health conditions within the same sample. As a result, important contextual factors that may shape the CVD health profile of WVs remain incompletely described. This study aims to address this gap by providing a comprehensive overview of cardiovascular health, the prevalence of associated CVD risk factors, and health behaviors among WVs.
Methods
Design
This study employed a descriptive cross-sectional design. An electronic survey was emailed to a convenience sample of WVs who were currently receiving or had previously received care at a single VA health care system. Self-reported data were collected on health behaviors (e.g., smoking, alcohol use, diet, and physical activity), CVD diagnoses, and CVD risk factors such as HTN, HLD, and diabetes. The survey also included items assessing depression, PTSD, and demographic characteristics.
Ethical consideration
The study received approval from both the university (IRB #24-42014) and VA institutional review boards prior to data collection. All participants were informed about the purpose of the study, the risks and benefits of participation, the voluntary nature of their participation, their right to decline participation, compensation, and the measures taken to protect their personal information.
Sample and setting
Study participants were identified using a secure patient tracking tool maintained by the local clinic, which tracks patient engagement. This VA health care system includes an urban academic medical center and community-based outpatient clinics (CBOC), which serve urban and rural Veterans. Eligible participants included WVs aged 18 and older who were assigned to this VA health care system. WVs without a listed email address were excluded from the study.
Procedure
Encrypted survey invitations were emailed to eligible individuals using REDCap electronic data capture tools hosted at the VA during January 2025. Access to contact information was granted in accordance with VA institutional data security protocols. Participants provided informed consent before beginning the survey. To maximize response rates, two reminder emails were sent at weekly intervals. Participants were compensated with $15 gift cards for the return of completed surveys.
A total of 1,909 WVs were identified and sent survey invitations, resulting in 412 returned surveys (response rate: 22%). Among the 412, three were excluded due to substantial missing data (e.g., >50% incomplete responses). In order to maintain consistency with the study’s objectives, 32 survey responses from transgender and nonbinary Veterans were excluded from the analysis. Thus, the final sample size is 380 cisgender WVs.
Measures
The survey questionnaire consisted of a total of 72 items covering health behaviors, health status, and demographic characteristics.
Health behaviors
Alcohol use
Alcohol use was measured using the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C). 26 This 3-item tool, which is adapted from the 10-item AUDIT, is used to measure severity of alcohol intake, with possible scores ranging from 0 to 12. The AUDIT was initially introduced by the World Health Organization and later adapted by researchers at the VA to create the AUDIT-C. 26 The AUDIT-C has shown excellent discrimination at distinguishing between individuals with and without hazardous drinking (AUC, 0.891, 95% CI, 0.877–0.904). 26 Higher scores indicate greater alcohol misuse severity. The standard female-specific cutoff of 3 or greater was applied to identify individuals at risk for hazardous drinking. 27
Cigarette smoking
Participants were asked, “Do you currently smoke cigarettes or use any tobacco-containing products?” to assess smoking status. Responses of “some days” and “everyday” were grouped into a single yes/no variable to indicate current cigarette use.
Diet
The 8-item Starting the Conversation screening tool was used to assess overall diet quality from the previous “few” months. 19 This tool has shown good accuracy in differentiating between healthy and unhealthy eating patterns. 19 Possible scores range from 0 to 16, with higher scores indicating a lower-quality diet. Two questions from the survey were extrapolated and reported independently regarding daily fruit and vegetable consumption. Participants responded by selecting 5 or more servings per day (0 points), 3–4 servings per day (1 point), or 2 or less servings per day (2 points).
Physical activity
Participants were asked about how many days in the past week they engaged in: at least 20 minutes of vigorous physical activity (e.g., aerobic activities, fast bicycling), at least 20 minutes of moderate activity (e.g., tennis, regular bicycling), or at least 10 minutes of walking activity and daily sedentary time (in minutes). These questions were adapted from the International Physical Activity Questionnaire (IPAQ), 28 a widely utilized tool for assessing physical activity levels.
Cardiovascular health and demographic characteristics
Beyond health behaviors, participants were asked to rate their overall health and overall diet on a scale of 0–100 (0 being very poor, 100 being perfect). They were also asked about their CVD history and CVD risk factors. Individuals were considered to have a CVD if they responded “yes” to ever being told they had congestive heart failure, coronary artery disease, peripheral artery disease, or a history of heart attack, stroke, or irregular heart arrhythmias. 9 Traditional CVD risk factors—including HTN, HLD, and diabetes—were also self-reported. Height and weight were both self-reported and used to calculate individual body mass index (BMI). Participants reporting ‘yes’ to having HTN, HLD, diabetes, or current smoking or were categorized as obese (i.e., BMI >30) were considered to have at least one leading risk factor for CVD. Self-reported CVD data have been shown to be a valid method for identifying CVD and CVD-related conditions. 29
Mental health
Mental health conditions, specifically depression and PTSD, were assessed using two widely used and validated tools: the Patient Health Questionnaire 8-Item Scale (PHQ-8) and Primary Care PTSD Screen for DSM-5 (PC-PTSD-5). The PHQ-8 is an 8-item diagnostic tool that has demonstrated strong reliability and validity in assessing depression severity in Veterans. 30 Scores of 10 or greater (out of 27) are considered to be indicative of probable depression.
Post-traumatic stress disorder was screened using a VA-developed tool, the PC-PTSD-5. 31 Possible scores for this 5-item questionnaire range from 0 to 5, and scores of 4 or higher are considered positive for PTSD in women. Depression and PTSD have been reported as dichotomous outcomes (i.e., having PTSD or not having PTSD) and as overall score. Additionally, participants were asked on their military service (e.g., branch of service) and demographic information (e.g., race/ethnicity, income, and relationship status).
Statistical methods
Means, standard deviations, and frequencies were calculated for all variables. Demographic characteristics were reported for the total sample and by age groups (18–44, 45–64, and 65+). These age groups were used based on previous reports of CVD and CVD risk factors in these age groups.8,23 All analysis was conducted using Stata version 17.0. 32
Results
Participants’ demographic and health characteristics
Table 1 provides the characteristics of the study participants. A total of 380 WVs completed surveys (20% response rate). Participants ranged in age from 23 to 82 years, with a mean age of 53 years. The majority were non-Hispanic White (58%), followed by non-Hispanic Black (20%), and Hispanic (14%). Over half of the participants reported having a bachelor’s degree, Master’s, or higher as their highest form of education. The largest Veteran group represented the Army (41%), followed by the Air Force (22%) and Navy (22%), with most participants reporting having served on active-duty (73%). Most participants reported either working full-time (35%) or being retired (29%).
Demographics Characteristics of Study Participants (N = 380)
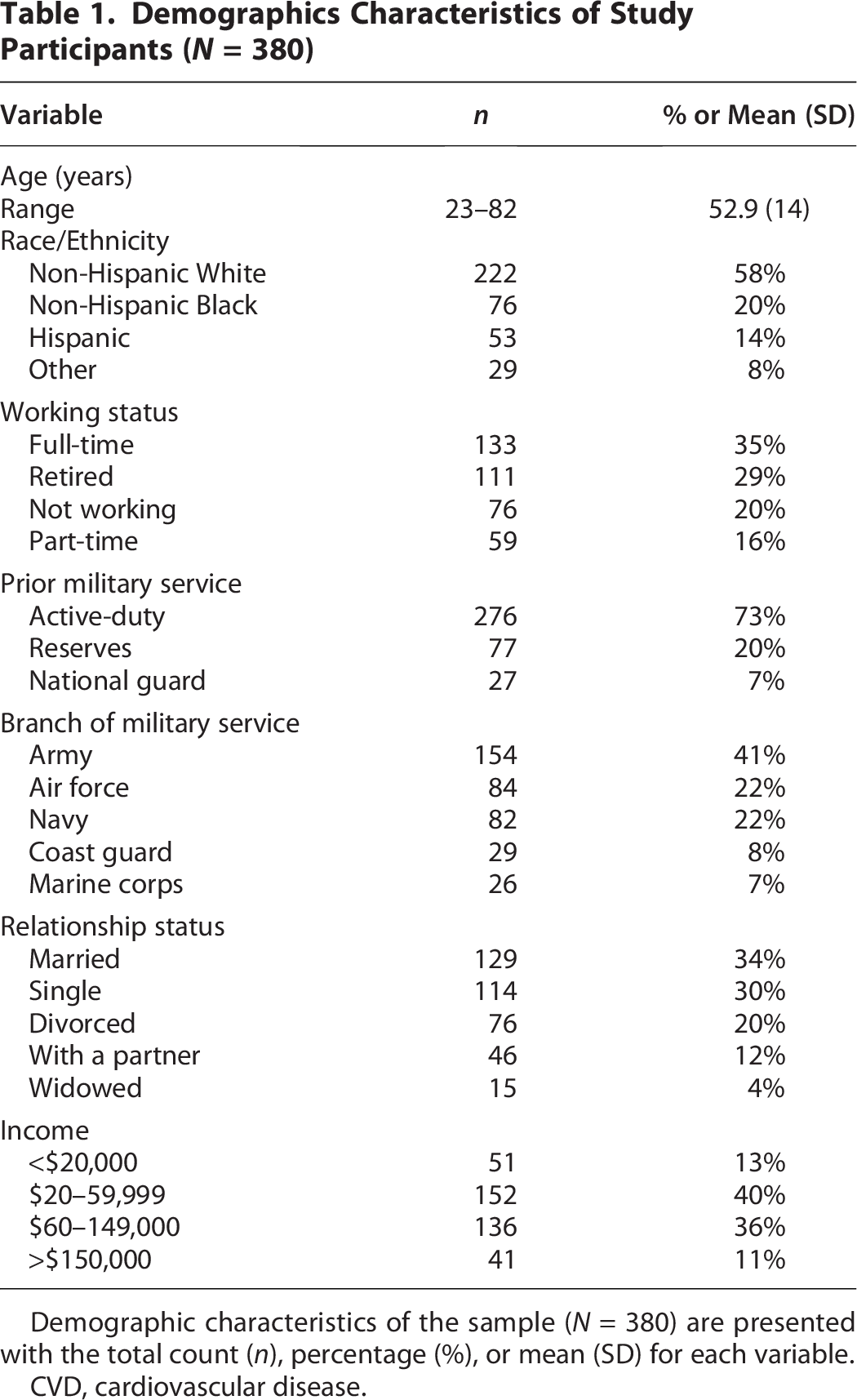
Demographic characteristics of the sample (N = 380) are presented with the total count (n), percentage (%), or mean (SD) for each variable.
CVD, cardiovascular disease.
Cardiovascular health and health behavior data are reported in Table 2. The mean overall health scores was 64.7 and mean overall diet score was 63.6. Of the traditional CVD risk factors, HLD was most prevalent (38%), followed by obesity (36%), HTN (33%), current smoking (13%), and diabetes (10%). Overall, 18% of participants had no traditional CVD risk factors, 32% had one, 43% had 2–3 risk factors, and 6% had 4 or more risk factors.
Cardiovascular Disease Risk Factors and Health Behaviors Among Study Participants (N = 380)
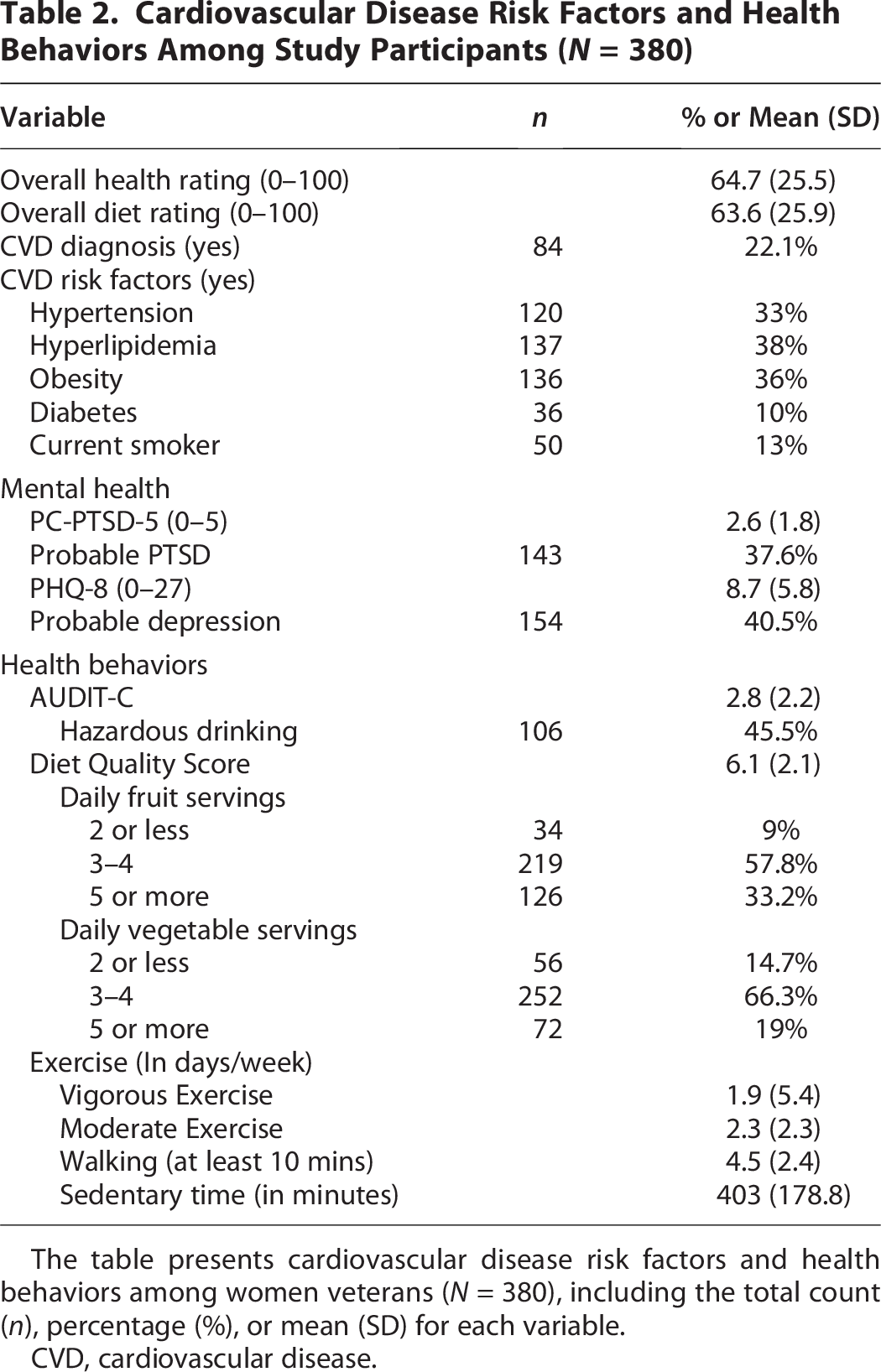
The table presents cardiovascular disease risk factors and health behaviors among women veterans (N = 380), including the total count (n), percentage (%), or mean (SD) for each variable.
CVD, cardiovascular disease.
Mental health and health behaviors
Participants had a mean PC-PTSD-5 severity score of 2.9 (SD, 1.8) and PHQ-8 scores had a mean of 8.7 (SD, 5.8). Due to incompleteness in survey data, the full IPAQ score was not reportable; therefore, we reported on days per week of moderate and vigorous activity, walking, and sedentary time (in minutes). The average reported days of vigorous activity was 1.9 (SD, 5.4) and the average reported days of moderate activity was 2.3 (SD, 2.3). Participants reported walking at least 10 minutes per day for 4.5 days, on average (SD, 2.4), with mean sedentary minutes per day of 403 (SD, 179). The mean diet quality score was 6.1 (SD, 2.1), a large majority of participants consuming three or more servings of fruits and vegetables per day. The mean AUDIT-C severity score was 2.8 (SD, 2.2). Using the established female cutoff (i.e., score of 3 or greater) measure for hazardous drinking, 26 nearly half of participants (45.5%) were considered to have hazardous drinking patterns.
Mental health, CVD, and CVD risk by age group
Figure 1 shows the prevalence of PTSD and depression (using dichotomous outcomes from the previously mentioned cut-points), CVD, and CVD risk factors (e.g., one or more of: smoking, diabetes, obesity, HTN, or HLD) by three age groups. Veteran groups have previously been described in the literature by a three-way divided categorization system consisting of younger (18–44), middle-aged (45–64), and older (65+) Veterans. 23 Depression and PTSD were most common among younger Veterans, with a high prevalence among middle-aged WVs, as well. As expected, trends in CVD and CVD risk factors increased by age group. CVD was highest among the 65+ group. Nearly 70% of the youngest WVs group had at least one leading CVD risk factors, and risk factor prevalence rose to 84% in middle-aged WVs and over 90% among WVs aged 65+.
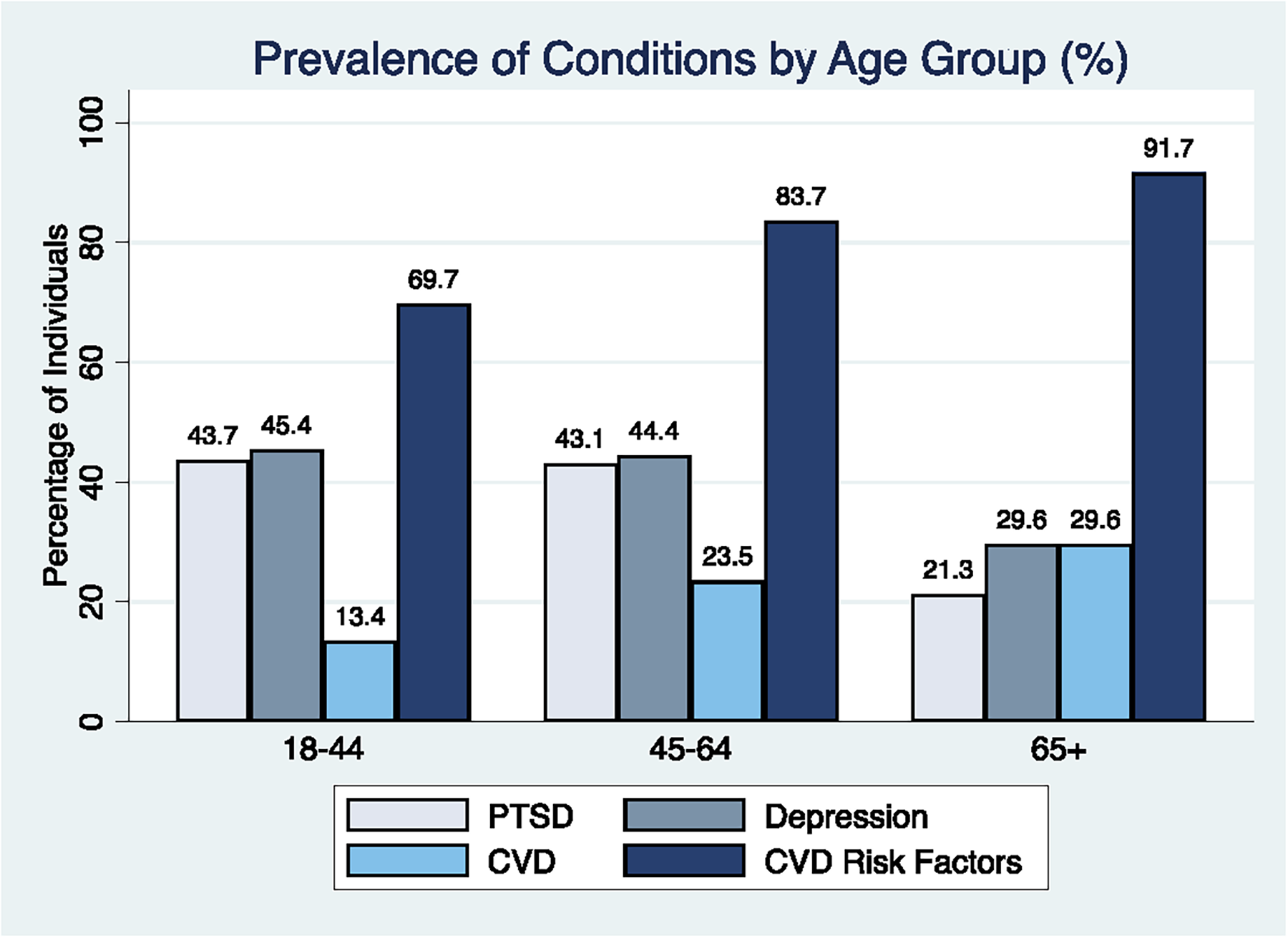
Mental Health, Cardiovascular Disease (CVD), and CVD Risk Factors by Age Group. Mental health, cardiovascular disease (CVD), and CVD risk factors by age group (18–44, 45–64, and 65+). The figure compares the prevalence of mental health conditions, CVD, and related risk factors across different age groups among women veterans.
Discussion
The objective of this study was to characterize cardiovascular health, traditional CVD risk factors, and health behaviors among WVs receiving care through one large VA medical center and surrounding CBOCs. Overall, we observed a high burden of traditional CVD risk factors alongside health behaviors and mental health conditions known to be relevant to CVD risk. These findings provide a contemporary descriptive profile of cardiovascular health among WVs and offer contextual evidence of potential areas for prevention and risk reduction efforts.
Alcohol use and cigarette smoking
In this sample, the prevalence of hazardous drinking among WVs was higher than what has been previously reported in prior WV samples.33,34 This may be related to factors specific to this population, for example, access to health care services and treatment limitations or military experiences and trauma exposure that could have an impact on hazardous drinking patterns. A recent study of 209 WVs conducted by Buckheit et al 33 reported a mean AUDIT-C score of 2.3, slightly lower than the mean score of 2.8 found in this study. Another systematic review of WVs’ literature published from 1980 to 2013 found a range of hazardous alcohol use of 12%–37% of WVs when using the cutoff of 3 or greater. 34 This study adds to previous literature by further highlighting concerning drinking patterns among WVs. 33 Heavy drinking patterns have also been noted among civilian women. One national study of U.S. women found that 40.3% reported heavy alcohol use and 19% reported binge drinking. 35
In contrast, smoking rates among this sample are lower than those previously reported. Tobacco use among WVs was reported in one 2012 article at 19.4%, 13 while our findings showed 13% of participants reported current cigarette smoking. Still, smoking rates among civilian women are lower with 10% of the general female population reporting daily cigarette use. 36 Prior research has documented declining rates of smoking and alcohol use among active-duty military personnel, 37 and findings from this sample of WVs are consistent with that trend.
Diet and physical activity
Observations from this study relating to diet, specifically daily fruit and vegetable consumption, are similar to those previously observed in WVs, 20 and daily reported fruit and vegetable consumption was much higher than the national average. According to a report from the CDC, U.S. adults consume one serving of fruit and 1.6 servings of vegetables per day, 38 compared to 85% of the current study sample reporting daily consumption of 3 or more servings of fruits and vegetables per day, indicating little concern over diet patterns among this sample.
Study participants reported spending 2 days, on average, doing both vigorous and moderate activities and more than 2 days per week walking. While WVs baseline engagement in physical fitness has been observed as being higher than in civilian women, longitudinal trends have shown a greater decline in physical activity, alongside an increase in sedentary time among WVs over time.39,40 Although the reported levels of physical activity in this study do not raise immediate concern, historical trends suggest a need for targeted interventions to prevent further declines and mitigate the risks associated with increased sedentary time.
Research on diet and physical fitness among WVs remains limited. While this study provides valuable insight into their dietary and fitness behaviors, further investigation is needed to fully understand these patterns. Given the high prevalence (36%) of obesity in this sample, a deeper understanding of diet quality and physical activity trends could inform the development of effective weight loss interventions.
Health characteristics
Prevalence of CVD risk factors has consistently grown among WVs. The most recent VA report on cardiovascular health in WVs found that for leading risk factors for CVD (e.g., diabetes, HTN, HLD, obesity, and smoking), 56% of WVs aged 18–44, 76% of WVs aged 45–64, and nearly 80% of WVs over the age of 65 had at least one CVD risk factor. 8 Data from this study show that CVD risk factor prevalence continues to increase, with the greatest jumps being among the youngest and oldest WVs. Overall prevalence of CVD among this group of WVs in California has also nearly doubled since a previous VA report. 8 With an increase in CVD risk factors, mental health, and some health behaviors, this trend in CVD growth may continue.
Findings from this study align with existing evidence of the growing prevalence of PTSD and depression among WVs, especially among the younger cohort. As the next wave of women transitions from activeduty to Veteran status, the VA should take steps to prepare for a cohort with similarly high rates of mental health by expanding access to trauma-informed, gender-sensitive mental health services. More already WVs utilize VA mental health services compared to male Veterans, 23 and treatment interventions such as cognitive behavioral therapy and interpersonal psychotherapy) have proven to be effective in reducing the severity of PTSD and depression. 41 Given the established link between mental health and CVD, addressing PTSD and depression may also contribute to reducing long-term CVD risk in WVs.
Strengths and limitations
This study is the first of its kind to report on overall prevalence of CVD, associated risk factors, and health behaviors among WVs. While several peer-reviewed VA reports8,23 have examined the health of WVs, including cardiovascular health, these publications often have limited audiences, as they are only accessible to VA employees through secure internal platforms. The study design is a strength due to its sample size and use of validated tools for self-reported data. Additionally, the inclusion of WVs receiving care across multiple community-based health centers provides a clear picture of present CVD health and health behaviors in this population.
Though the study design and overall reporting are notable strengths, several limitations should be acknowledged. The use of self-reported surveys introduces potential biases, such as selection bias and recall bias. Given reliance on self-reported data, the prevalence of certain CVD risk factors, such as HTN, may be underestimated, particularly among individuals with limited engagement in routine health care. Additionally, though PTSD was assessed using a validated instrument (i.e., PC-PTSD-5), this measurement is designed for screening rather than diagnostic confirmation and may be subject to reporting bias. The absence of a handwritten survey option may have limited older and less tech-savvy WVs’ participation. Although the study used validated self-report questionnaires, future research should incorporate clinical data in addition to self-report to ensure more robust findings. Missingness of data and a low response rate also present limitations to the survey data. Although surveys with >50% missing data were excluded from this study, a pattern emerged of several missing responses on certain areas of the survey (e.g., IPAQ), which limited the usability of this measure for physical fitness. Finally, survey invitations were sent to WVs receiving care through one VA medical center, limiting the generalizability of findings to the broader population of WVs. However, California has a large WV population, and we have not found any evidence to suggest that Veterans in this region differ in phenotype from those in other regions (e.g., this VA medical center serves both rural and urban Veterans). 23
Implications for practice
Veterans Affairs medical centers and clinics are well-equipped with programs and resources to promote health behaviors and treat CVD risk factors to help prevent future CVD diagnosis. Ongoing programs, such as smokefreeVET, substance abuse treatment, and MOVE!, are just a few examples that serve Veterans in an attempt to support Veterans in promoting their health and preventing chronic illness. Each VA health care system also has a designated Health Promotion and Disease Prevention Manager, responsible for integrating programs into clinical care for Veterans. Tailoring these existing programs may offer a practical approach to enhancing health behavior interventions to address the specific needs of WVs. CVD and CVD risk screening efforts should be expanded for both VA and non-VA clinicians. Asking questions, such as “Have you served?” in routine assessment, is an important factor in assessing individual CVD risk and should be included as a part of a comprehensive health profile. Finally, mental health integration with clinical and health behavior programs will be imperative in order to address the unique CVD profile of WVs. With a robust of program offerings and mental health services available to Veterans through the VA, future efforts to merge these existing programs may be a feasible and novel way to achieve CVD prevention aimed at WVs.
Implications for future research
Although these data provide a broad overview of cardiovascular health, CVD risk factors, and health behaviors, a more focused assessment of health behaviors, particularly physical fitness, could help enhance the CVD risk profile of WVs. Some survey responses lacked sufficient detail, making it challenging to quantify and fully assess physical fitness levels. Future research should incorporate more precise measures of health behavior, such as objective fitness assessments, or consider one-to-one interviews to improve accuracy and completeness. Factors such as social support, rurality, and access to healthy food have all been shown to influence health behaviors. Future research should explore how these social and environmental determinants interact with clinical factors and influence CVD risk. Further efforts are needed to better understand hazardous drinking patterns among WVs and to make sense of the high rates among this study sample. Future research aimed at assessing the associations between CVD risk factors and CVD diagnoses will be critical to contextualizing and building on these descriptive findings. While PTSD scales have been well-validated in the WV population, a more thorough characterization of trauma type and severity could also shed light on the important relationship between mental health and heart health. In addition, linking survey data to VA records (i.e., clinical markers and utilization patterns) could provide a more comprehensive understanding of how health behaviors correlate with disease outcomes and health care engagement. While the majority of WVs continue to opt to receive health care in the community, 23 the VA offers care to more WVs than any other health care organization. Therefore, the VA is a logical place to derive these data and focus CVD preventative efforts.
Conclusion
This study provides a comprehensive overview of the cardiovascular health, mental health, and health behaviors among WVs receiving care at a VA medical center in California. Findings indicate increasing rates of CVD and its risk factors among WVs, with a particularly high prevalence of PTSD and depression among younger and middle-aged WVs. Although smoking rates have declined, hazardous drinking remains a concern. These findings highlight the need for tailored CVD interventions that integrate mental and behavioral health factors alongside clinical care to improve health outcomes among WVs.
Authors’ Contributions
C.D.: Conceptualization (lead), writing—original draft (lead), data curation (lead), formal analysis (lead), visualization (lead), writing—review and editing (equal). L.G.P.: Writing—review and editing (equal), conceptualization (supporting). J.K.C.: Writing—review and editing (equal), conceptualization (supporting). O.S.H.: Supervision (lead), writing—review and editing (equal), project administration (supporting). All authors read and approved the final article.
Footnotes
Acknowledgments
The authors would like to acknowledge the survey data contributed by women Veterans, which made this study possible.
Prior Presentation
Data Availability
The data that support the findings of this study are available on request from the corresponding author.
Institutional Review Board (Human Subjects)
This study was approved by the UCSF and VA Medical Center Institutional Review Boards (IRB) (IRB #24-42014).
Institutional Clearance
Institutional approval granted by the University of California, San Francisco and the San Francisco VA Medical Center.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the NIOSH, the Department of VA, or the United States government.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the
This material is based upon work supported by the National Clinician Scholars Program, sponsored by the Department of Veterans Affairs Office of Academic Affiliations (OAA) and the University of California, San Francisco. This material was supported with the use of resources and facilities at the San Francisco VA Medical Center, San Francisco, CA.