
Abstract
Background:
Over one million Americans develop menopausal symptoms annually. There is limited information regarding the population-level management of women who develop these symptoms. We described provider characteristics and clinical and demographic characteristics of females newly diagnosed with perimenopausal or menopause symptoms in the United States.
Methods:
We performed a retrospective cohort study using Optum Clinformatics data between January 1, 2012, and December 31, 2024. Eligible female patients between the ages of 40 and 65 years of age were identified by their first claim with a diagnosis code indicating menopause or perimenopausal or menopausal symptoms between 2013 and 2024. We categorized the diagnosing health care providers and tabulated the demographic and clinical characteristics of these patients, along with treatments that were prescribed and dispensed. We stratified the population into three age groups to observe potential differences based on age of onset of menopause symptoms.
Results:
There were 297,928 eligible female patients initially diagnosed with symptoms during the study period, diagnosed by 95,178 unique health care providers. Providers in the areas of family practice, internal medicine, and obstetrics and gynecology were the most common to diagnose these initial symptoms. Most of the women (69%) did not receive medications for treatment.
Conclusion:
Symptomatic perimenopause and menopause are natural reproductive phases for all women, and some treatments have been proven to cause harm. Women experiencing problematic vasomotor symptoms and sleep problems in perimenopause and menopause likely need treatment. We found that prescription pharmacologic treatment for symptoms was initiated in 31% of women.
Background
In the United States alone, approximately 1.3 million women per year begin to experience menopause symptoms.1–3 Approximately $3 billion dollars per year is spent managing menopause symptoms in the United States. 4 Perimenopause refers to the time when women experience physical and psychological changes associated with the transition from their reproductive years to menopause, while still having regular menstrual cycles. The age of onset of perimenopause varies, and every woman’s passage is unique, with reproductive hormone fluctuations commonly contributing as the underlying cause of common symptoms.3,5,6 The menopausal transition is defined after one year without menstrual flow.
One major symptom of perimenopause and menopause includes vasomotor symptoms (VMS) such as hot flashes.7,8 In the United States, the Study of Women’s Health Across the Nation’s national estimates for VMS show between 60% and 80% of women experience VMS during the menopausal transition. 9 Among women with moderate to severe symptoms, the prevalence of VMS during the early perimenopause to late perimenopause phase ranges from about 25% to 50%, with a recent estimate by Nappi et al. at 34%. 10 Of the costs attributed to VMS, approximately $1,350 per patient per year is spent managing these specific symptoms in the United States in direct health care costs, with another almost $800 in indirect costs. 4 Variation in VMS prevalence and duration is at least in part driven by differences seen across racial/ethnic groups. Among women reporting 6 or more days of VMS, a measure representing moderate to severe symptomatology, the prevalence of VMS during the early perimenopause to late perimenopause phase was highest and duration longest among African American and Hispanic women compared with white non-Hispanic, Japanese, and Chinese women. 11
Hormonal therapies are often used as first-line to treat menopausal symptoms, primarily VMS, but increased risk of venous thromboembolism, myocardial infarction, stroke, and hormone-dependent cancers, such as breast cancer, have raised concerns about their safety and limited their applicability.12–14 Furthermore, MHT has not been shown to be effective for perimenopausal VMS and sleep; currently oral micronized progesterone is the only documented effective and safe therapy. 15 Nonhormonal therapies such as selective serotonin reuptake inhibitors (SSRIs), gabapentin, and clonidine have limited efficacy and can have adverse effects such as sedation and nausea. 13 Despite the majority of women experiencing these symptoms, many never receive treatment, and 20% of internal, family, and obstetrics medicine reported receiving no teaching on menopause during residency. 14
There is a paucity of published data regarding the population-level management of the diagnosis and care of women who develop initial menopausal symptoms, such as VMS. Because these symptoms may present in various ways, we postulated that the diagnosis of menopausal symptoms is happening in many areas of the health care system. Additionally, we hypothesized that understanding where these encounters occur may inform more efficient patient management and care pathways. Therefore, we sought to describe provider characteristics and the clinical and demographic characteristics of females newly diagnosed with perimenopausal or menopause symptoms in the United States, along with the treatments prescribed after diagnosis.
Methods
We performed a retrospective cohort study using administrative health claims data from Optum between January 1, 2012, and December 31, 2024. The Optum Clinformatics Data Mart™ (Optum, Eden Prairie, MN) is an administrative claims database composed of de-identified data of commercially- and Medicare Advantage-insured patients (United Healthcare Group). The database contains enrollee information (gender, age, race/ethnicity, US region of residence, and insurance plan type), medical service claims information (diagnosis and procedure codes), linked laboratory data, and pharmacy claims data for over 54 million members since 2006, and is fully compliant with the Health Insurance Portability and Accountability Act (HIPAA). The study team had direct access to claim-level data.
Eligible patients were categorized as female between age 40 and 65 years of age and identified between January 1, 2013, and December 31, 2024, at their first occurrence of a menopause diagnosis claim (index event) to allow for a 12-month baseline period of continuous health plan (insurance) enrollment. The first menopause diagnosis claim (international classification of diseases [ICD]-9/10-CM: 627.9, N95.1, N95.9) was captured from either the outpatient or inpatient care setting, excluding claims from the emergency department. People with a cancer diagnosis in the female genital organs or breasts (ICD-9/10-CM: 174.9, 180, 182–184, C50-C57) during the baseline period were excluded from the cohort. Additionally, due to their frequent use for symptom management, people with prescription records for a hormonal contraceptive, menopausal hormone therapy (MHT), antidepressant, or insomnia treatment for any diagnosis during the baseline period were also excluded from the study population. Because the primary objective of this analysis was to describe provider characteristics, we did not require a specific amount of patient follow-up time after the 12-month baseline period. Subjects were censored on the date their continuous health plan enrollment ended.
The diagnosing provider associated with the index claim of menopause symptoms for each patient was summarized by provider specialty, practice type, and region of the country. We grouped provider specialties into mutually exclusive categories that included addiction medicine, cardiology, nurse midwife, endocrinology, family practice, internal medicine, nurse practitioner, obstetrics/gynecology (OB/GYN), oncology, radiology, surgeon, or other. The same classification was applied to categorize the prescribers of treatments after diagnosis.
Study patient demographics were summarized, including age at diagnosis, year of diagnosis, race, region, and health insurance type. The comorbid conditions and medications for each subject were tabulated from the baseline period. We also calculated each subject’s Quan–Charlson comorbidity index using claims from the baseline period. Study patients were categorized by age at index diagnosis into three groups (40–44, 45–50, and 51–65 years of age, respectively), and between-group comparisons were made for subject demographic and clinical characteristics. Lastly, we tabulated the prescription drug claims for each patient to capture the initial treatment decisions among women newly diagnosed with menopause (after study baseline). Menopause symptom treatments were grouped in four individual categories: MHT including estrogens and progestins, antidepressants (selective serotonin and selective serotonin–norepinephrine– reuptake inhibitors [SSRIs or SNRIs, respectively]), insomnia treatments (diazepam, lorazepam, temazepam, and z-drugs), and other symptom prescriptions (gabapentin, oxybutynin, and clonidine). Combination therapy was defined when multiple treatments were prescribed and dispensed within one month after the initiation of any treatment.
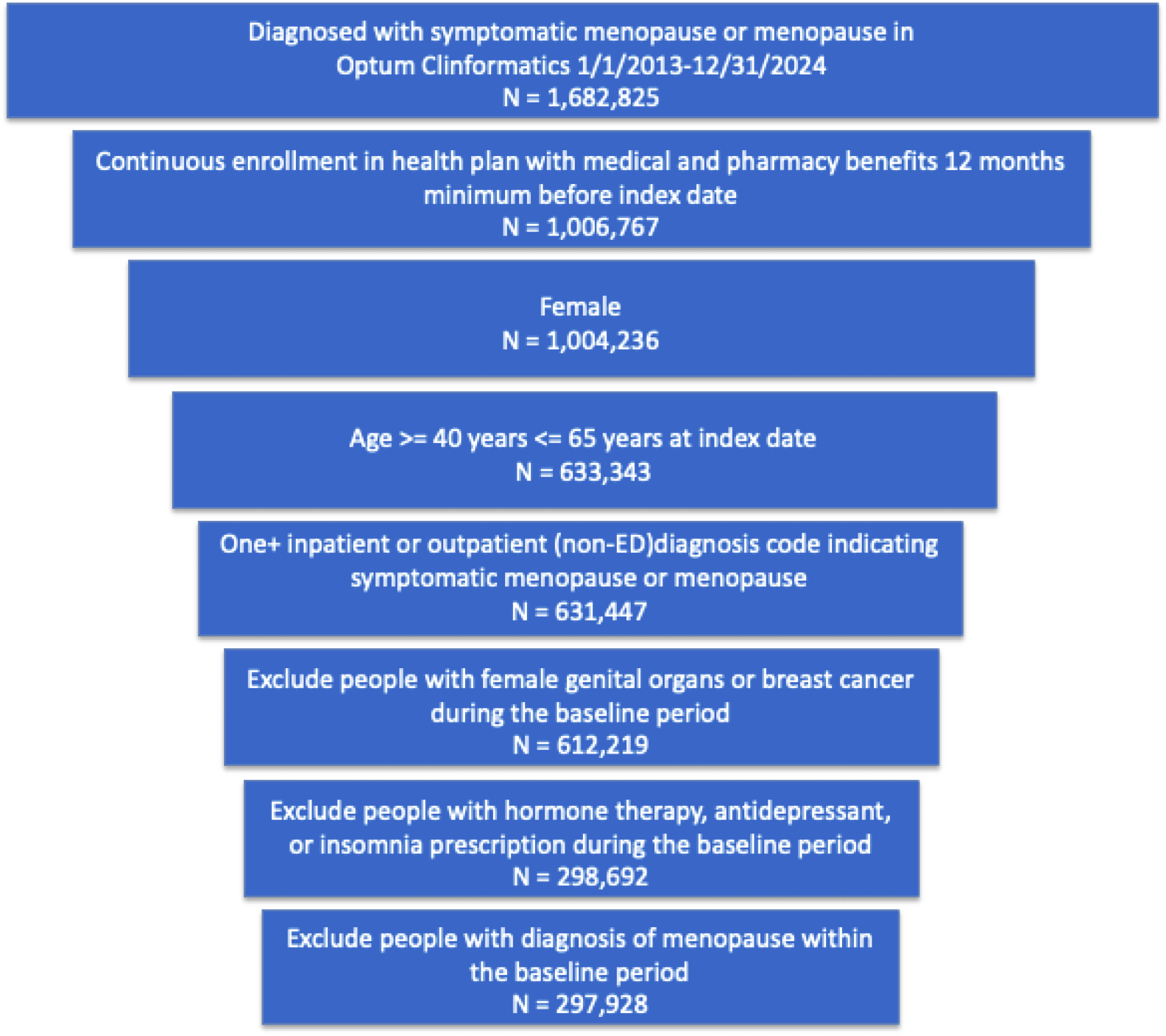
CONSORT Diagram of study. Index date defined as first date of claim with the diagnosis of menopausal symptoms or menopause baseline period defined as the continuous 12 months prior to the index date.
Statistical Analysis
We summarized diagnosing provider and patient characteristics as counts and percentages. We compared the demographic and clinical characteristics of patients within three age groups at diagnosis. Age was compared between groups using the Kruskal–Wallis test, the continuous Quan–Charlson comorbidity index using ANOVA, and categorical variables were compared using chi-square tests.
We utilized de-identified HIPAA-compliant claims data for the analyses reported herein; thus, the study was deemed nonhuman subjects research. This study was designed and implemented following the STROBE guidelines. 16 All analyses were performed using Statistical Analysis Software (SAS) Viya 4, LTS 2025.03 (SAS Institute Inc., Cary, NC, USA).
Results
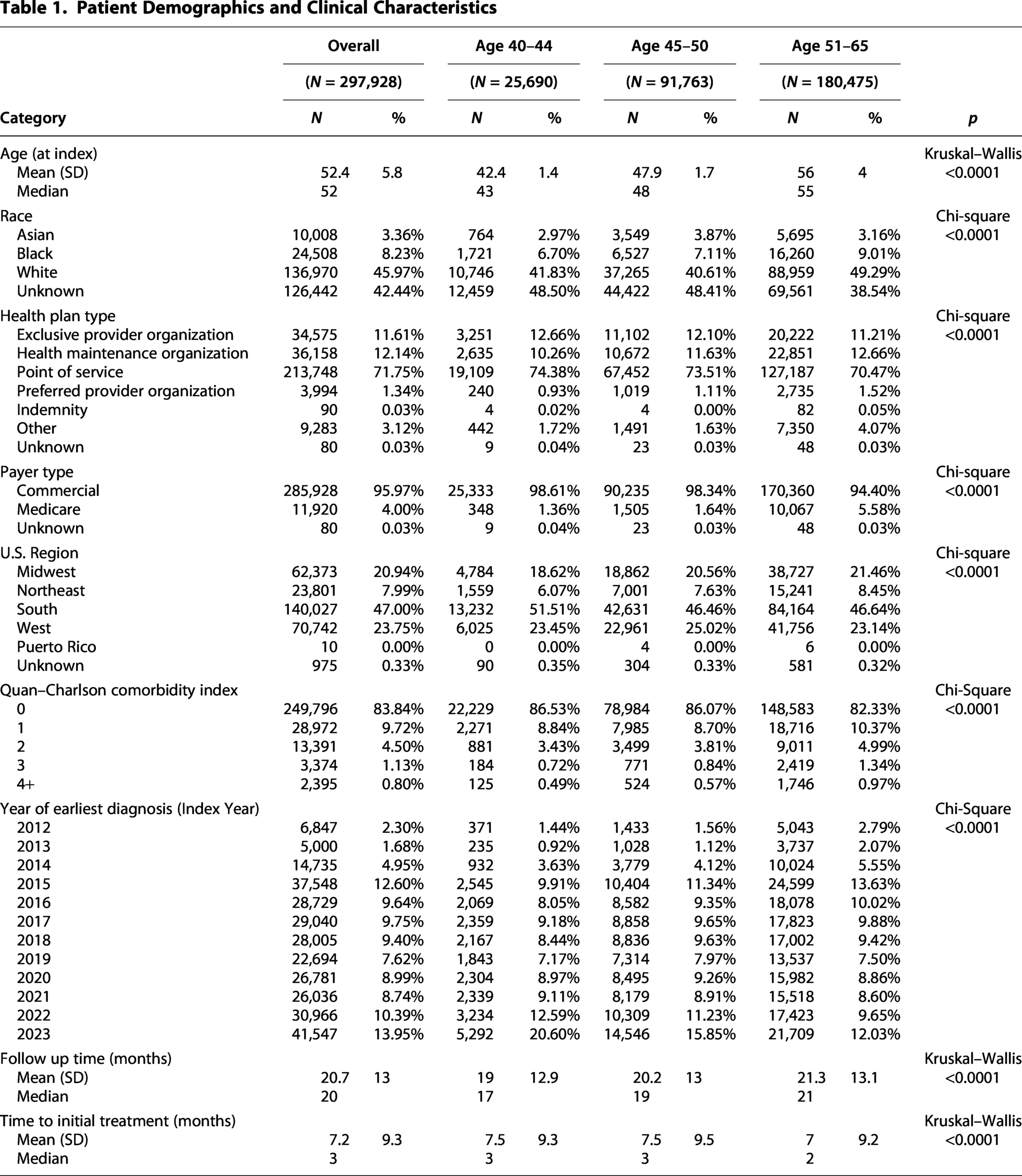
We identified 297,928 eligible female patients who were initially diagnosed with menopause symptoms during the study period from a pool of 1,682,825 people with at least one diagnosis (Fig. 1) between 2013 and 2024. The average age of the patient cohort was 52.4 years (standard deviation [SD]: 5.8). Race was unknown or missing for 42.4% of the cohort. White individuals represented 45.9% of the cohort. Most (96%) of the cohort were covered by commercial insurance plans, and the majority of patients were enrolled in a point of service plan (71.8%). The majority of patients (83.8%) had a zero score on the Quan–Charlson comorbidity index, though 5.6% of the cohort had a 2 or higher score (Table 1). The baseline comorbidities and medications for the patient cohort are displayed in Table 2. Importantly, these patients had a mean follow-up time (continuous insurance coverage where treatments may be observed before censoring) after index diagnosis of 20.7 months (SD: 13 and median: 20 months).
Patient Demographics and Clinical Characteristics
Baseline Comorbidities and Medications

GnRH, gonadotropin releasing hormone; Gyn, Gynecology.
This cohort of patients was diagnosed by 95,178 unique health care providers. The three most common diagnosing provider specialties were family practice (30.9%), OB/GYN (23.4%), and internal medicine (16.3%; Table 3). Treatment was observed to be initiated in 30.7% of women, with the use of MHT being most common (48.7%), followed by insomnia treatments (23.3%) and antidepressants (20.7%; Table 4). These observed treatments were initiated on average at 7.2 months after diagnosis (SD: 9.3, median: 3 months).
Diagnosing Provider Characteristics

Treatments Observed During Follow-Up
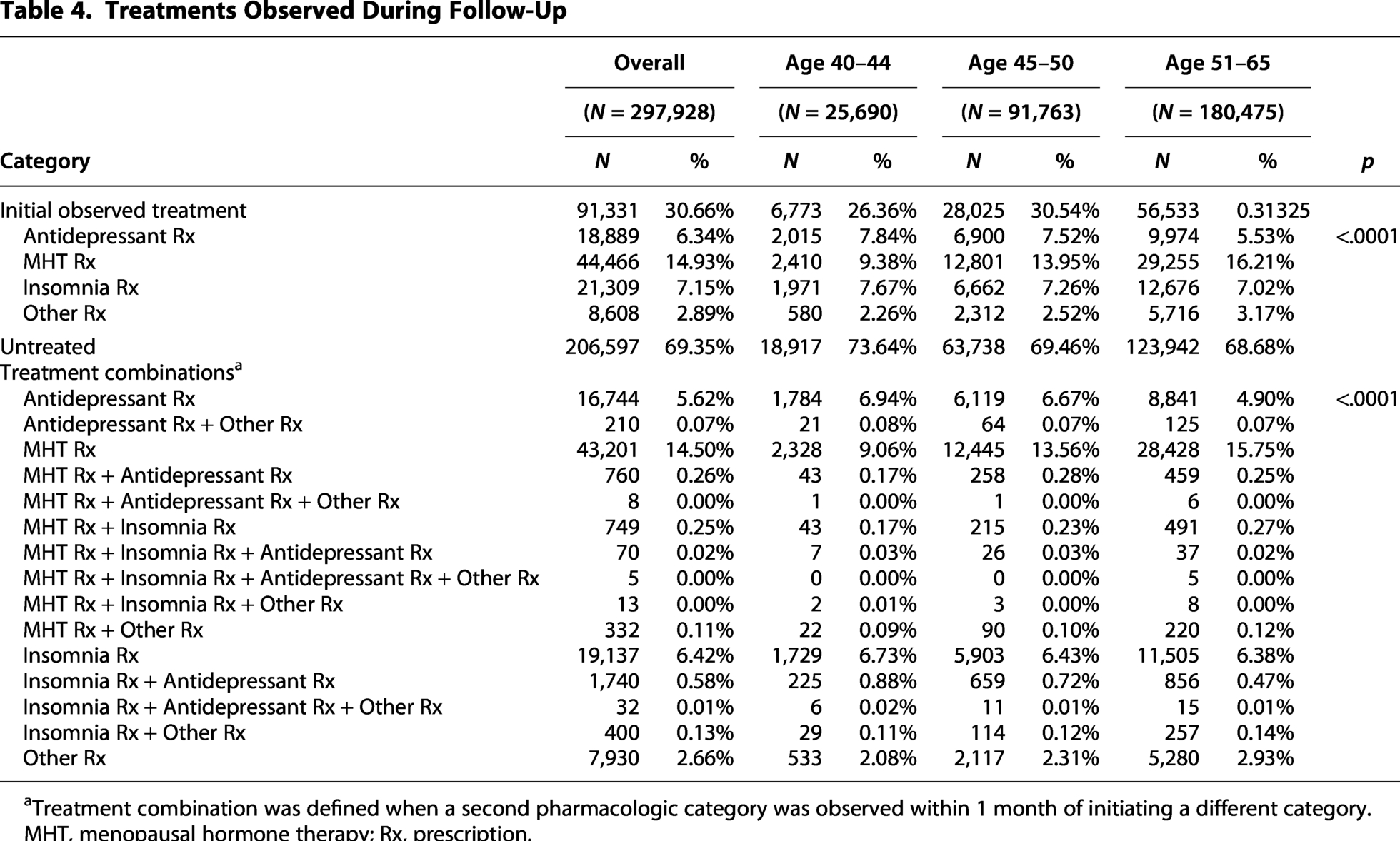
aTreatment combination was defined when a second pharmacologic category was observed within 1 month of initiating a different category.
MHT, menopausal hormone therapy; Rx, prescription.
Age subgroups
The majority of the patient cohort were over 50 years of age (60.6%), with approximately 5.6% of the patients aged 51–65 years of age covered by Medicare compared with 1.5% in younger ages (Table 1). Not surprisingly, the older age group had overall higher comorbidity index distribution. We also note modest but statistically different distributions by geographic region between the age groups. Due primarily to large sample sizes, all between age group comparisons of demographic and clinical characteristics were statistically significant. However, provider type and treatment initiation were relatively similar overall (Tables 3 and 4).
Discussion
We described a cohort of almost 300,000 female patients in the United States. who were diagnosed with menopausal symptoms between 2013 and 2024 and the health care providers who diagnosed and made initial treatment decisions for this population. These women were diagnosed primarily by three types of health care providers: OB/GYN, family practice, and internal medicine. Less than one-third of diagnosed women filled a prescription for a pharmacotherapy during the observed follow-up after diagnosis. This may indicate that through shared decision-making, patients and providers are currently managing initial menopause symptoms using alternatives to prescription medication, including adjunctive therapies. 17
To our knowledge, this is the first study examining the incident diagnosis and initial treatment of women with menopausal symptoms in the United States focused on both patients and the type of health care providers seen. Prior work, for example, using the National Health and Nutrition Examination Survey, has shown that women with menopause have been using less hormone replacement therapy in recent decades across all age and race/ethnicity groups. 3 This is not surprising given the findings of the Women’s Health Initiative and subsequent clinical recommendations.18,19 Our study shows that not only is the use of hormonal and nonhormonal treatments low, but so are common treatments for other symptoms typically experienced by people entering menopause.
Limitations
Like any study, these results should be interpreted in the context of limitations of the study design and data source. The inclusion and exclusion criteria for the study were necessary to identify a population of women who could be assured to have new treatment initiated and associated with the onset of a provider visit for symptoms of menopause. Excluding women with a recent history of genital or breast cancer was necessary to ensure that the diagnosis was not biased by cancer treatment nor that symptoms of menopause were not induced by either a tumor or cancer treatment. This is an important subgroup of women aging into menopause but outside the scope of the current analysis. Excluding women with a history of medications for depression or insomnia may have excluded women with underlying conditions not associated with menopause and thus may not capture a subgroup of women who enter menopause with active depression or insomnia. Additionally, as with all observational studies, we must also acknowledge the limitations of retrospective analyses and the inherent limitations of utilizing claims data. Because this study was descriptive in nature, the primary limitation is of generalizability of the Optum patient population to the rest of the U.S. population of women experiencing menopausal symptoms at diagnosis. Because Optum is among the three largest health insurers in the country, collectively covering over 80% of commercially insured adults in the United States, we feel that the population is generalizable, with the exception of excluding the Medicaid and uninsured population. Furthermore, we designed this study with providers as the primary area of interest and thus did not restrict the patient population based on follow-up time, which could result in misclassification of treatment status based on inability to observe treatment in the available follow-up data. Based on the mean and median follow-up time of 20 months and observed time to treatment initiation of 7.3 months, the risk of misclassification for descriptive purposes is minimal. However, we also did not capture oral micronized progesterone, compounded hormone treatments, or over-the-counter supplements and medications, which are not cleanly reported in claims data or covered inconsistently by health insurers in the United States, or are simply missing from claims data due to lack of coverage, respectively. 17 This limitation regarding compounded prescriptions could bias our finding of the treated proportion toward the null.
Conclusions
Women experiencing symptoms of menopause in the United States are typically diagnosed by primary care and OB/GYN providers in the areas of family practice, internal medicine, and OB/GYN. In this large cohort study, we found that treatment for common symptoms was initiated in 31% of women using all available follow-up time. Some women might benefit from adding pharmacologic treatments. Because some clinicians may be uncomfortable with the use of hormones that may be helpful for some women, care should be taken to focus on training and implementation of care strategies among the providers most commonly caring for women developing these symptoms.
Footnotes
Author Disclosure Statement
A.P.S., J.H., K.R.B., Je C., A.L., and R.F. are employees of Bayer U.S. LLC. R.N.H. has received consulting fees from Bayer U.S. LLC. Ju C. and E.D. previously served as interns at Bayer U.S. LLC.
Funding Information
No funding was received for this article.