
Abstract
Background:
In recent years, several regions have evolved their own definitions of advance care planning (ACP). Country-specific characteristics may affect local definitions, goals, and quality assessment.
Objective:
To obtain collective views of key opinion leaders in Singapore regarding the target population, scope, and goals of ACP, and to propose a list of quality indicators that could be used to monitor and evaluate its progress and impact.
Design:
A World Café methodology was used to facilitate group discussions among participants involved in ACP-related work across a range of settings including acute hospitals, community hospitals, primary care clinics, nursing homes, community care organizations, nursing homes, and universities. To define the target population, scope, and goals of ACP, three distinct exercises were conducted within the World Café session, from which main insights were synthesized and reported.
Results:
A total of 34 ACP leaders, administrators, facilitators, and researchers representing 25 organizations participated. ACP was conceived to be an ongoing process of exploring an individual’s personal beliefs, values, and health care preferences in relation to current and future medical care, together with their families and loved ones. To balance respecting the voice of the individual a with operational efficiency, organizations can deploy structural and process quality indicators to guide goal achievement.
Conclusion:
We have established the intended target population, scope, and goals necessary to inform the implementation of ACP. Critical quality indicators were identified to support the monitoring and evaluation of the program’s progress across different implementation stages in Singapore.
Introduction
Singapore’s population is rapidly aging, with approximately one in four persons turning 65 years or older by 2030. 1 While medical technology continues to improve Singaporeans' care and possibilities for future therapies, it can complicate end-of-life care decisions. If individuals do not articulate their preferences, care providers and family members may be compelled to make decisions on their behalf upon the loss of mental capacity. Such uncertainties may cause misunderstanding and unwarranted stress among families and health care teams. Consequently, individuals may receive end-of-life care that contradicts their personal values and wishes.
In 2011, Singapore’s national advance care planning (ACP) program, “Living Matters,” was launched with support from the Ministry of Health. The Agency for Integrated Care, a central coordinating body for aged care services funded by the health ministry, was tasked to spearhead the implementation of the national program. A national ACP Steering Committee comprising senior clinicians, social workers, lawyers and ethicists was established to steer the national adoption of ACP and fostering a collaborative ecosystem among health care partners. 2 In the early years, the program focused on developing a supportive infrastructure, such as training hospital-based staff members to facilitate ACP discussions and establishing a national electronic ACP repository where completed ACP documents could be easily retrieved by health care professionals. Since then, the program has expanded to adopt strategies to enable more conversations in the community.
Modeled after the “Respecting Choices” program developed by the Gundersen Health System in Wisconsin, United States,3,4 ‘Living Matters’ aims to empower individuals to make informed health care decisions through open and ongoing conversations between individuals, their health care proxies, which could include their family and other loved ones, and health care professionals. The program targets populations comprising three major adult groups, including individuals suffering from life-limiting illnesses with a prognosis of less than 12 months, those with progressive and complex chronic organ-specific conditions, as well as healthy people and those with early chronic diseases. 2 ACP has been implemented across public health care organizations, community hospitals, and nursing homes. Furthermore, community care organizations operating Active Ageing Centers, which provide a variety of activities for older people to stay active and connected, also provide ACP facilitation services. As of July 2025, approximately 77,000 ACPs had been completed nationally. 5
The national ACP program has been evaluated twice since its inception. Despite strong recognition of its intrinsic value, the evaluations found a general lack of agreement around the objectives and expected benefits of ACP. The definition and role of ACP in relation to its specified goals have also been heavily debated in recent literature.6,7 In contrast to the Western perspective that focuses on self-determination, 8 the definition of ACP in Asia has evolved to emphasize a family-based approach. 9 There has also been more explicit delineation between current care and end-of-life decisions and whether ACP should cover both aspects. A 2024 consensus document on the definition of ACP for persons with dementia specified that ACP should apply to both current and future care. 10 Given these shifts, it is timely to assess how these wider environmental changes have influenced local perspectives.
The provision of goal-concordant care remains a central tenet and foundational goal for ACP. 8 Emerging research has, however, highlighted significant challenges in achieving goal-concordant care, as there are significant gaps between hypothetical scenarios and the decision-making process in clinical practice settings. 7 In reality, a myriad of scenarios may arise, and ACP conversations can facilitate discussions among stakeholders to explore and understand values and beliefs that could guide the care preferences of the individual while allowing for preferences to evolve. Instead of using singular output or outcome measures, we need to first articulate the key goals of ACP and its underlying processes before establishing a robust set of quality indicators to support the systematic collection of performance data to monitor the progress and achievement of the objectives of ACP.
In this article, we aim to present a case study describing the process through which we sought to obtain collective views among key opinion leaders in Singapore regarding the definition the scope of ACP process and quality indicators that should be used to monitor and evaluate its progress and impact.
Methods
Study design
In this study, we engaged multiple stakeholders in an open conversation using the World Café approach. 11 The process integrates several design principles, including clarification of the context, creating a hospitable space, encouraging everyone’s contribution, connecting diverse perspectives, listening together for patterns and insights, and sharing collective insights. 12 Several key studies8–10,13 eliciting definitions of ACP had used the Delphi technique to derive consensus. While anonymity can encourage discussions and provide equal weightage to each participant’s views, we might potentially miss nuances that could arise in a face-to-face discussion.
The study team was drawn from a 21-member national Quality Implementation Workgroup established to lead the development of a set of guidelines to support the implementation of ACP in Singapore. 14 This team comprised the chairperson of the workgroup, health services researchers, as well as representatives from the Agency for Integrated Care, a governmental agency charged by the Ministry of Health to oversee national ACP implementation.
Study participants
We sought to elicit a wide range of perspectives from those involved in leading, facilitating, and conducting research on ACP. Invitations were sent out to 40 persons considered to be key opinion leaders of ACP in Singapore. They are involved in ACP-related work in public acute and specialist hospitals, community hospitals, public primary care clinics, nursing homes, community care organizations, nursing homes, and universities (with backgrounds in law, bioethics, public health, and health services research). Among the participants were also members of the ACP National Steering Committee who are involved in shaping the national ACP agenda.
The World Café event was organized on 28 June 2023 and held in a seminar room in the Agency for Integrated Care corporate office. The participants were grouped into five groups with mixed professional backgrounds and practice settings. Three different exercises during the event were conducted, and the members of the core team were assigned to each subgroup during the exercises to facilitate discussions (Fig. 1).

Details of World Café Exercises. ACP, Advance Care Planning.
World café approach
The first exercise centered around a discussion on the definition of ACP in Singapore’s context using guided questions: Target population of ACP, process of ACP, scope of ACP discussion, goals of ACP process. Each group summarized their discussions on a flipchart and presented it to the group, where participants were free to provide comments on the definitions. We started the second exercise with a presentation of the scope of the ACP process and utilization of Mentimeter, 15 a web-based audience response system, to vote on the scope and flow of the ACP implementation in the practice settings.
The third and last exercise aimed to involve participants in the identification and prioritization of quality indicators that can support the monitoring of our health system’s progress toward achieving ACP goals. Five stations were organized to reflect steps of the implementation process: awareness and advocacy, identification, having the conversation, documenting the conversation, accessing and honoring the individual’s voice. Each of the five groups rotated through all stations. At each station, the groups brainstormed on the “who, what, when, why, and how” to measure relevant outcomes. They were also tasked to prioritize the top two outcomes for each stage of the implementation process. The content of the discussion was documented on flip charts available at each of the five stations. Facilitators shared the overall results. Participants were then asked to vote in a live digital poll on the ACP process that they viewed as having the greatest urgency to focus on.
The study team maintained a copy of the material written on the flip charts and the digital voting percentages and compiled summary notes from the group presentations. All data sources were anonymized. Quality indicators were categorized based on the three constructs (structure, process, and outcome) of Donabedian’s quality of care framework. 16 The team further deliberated on the findings and reached an agreed summarized version that was subsequently shared via email with all World Café participants, as well as invitees who were unable to attend. Feedback from both participants as well as non-participants mitigated researcher bias and addressed potential gaps in the interpretation of the findings.
This activity was conceived as a stakeholder dialogue session. As such, we did not collect any identifiable data. All written comments and notes were captured anonymously. Participants were informed at the start of the session that written records would be analyzed and used to create a final report.
Results
Participants
Out of 40 invitees, a total of 34 individuals attended the World Café session. These participants included ACP leaders, administrators, facilitators, and researchers representing 25 unique organizations, including acute care hospitals (n = 17), community hospitals (n = 3), polyclinics (n = 2), nursing homes (n = 3), community care organizations (n = 7), and universities (n = 2). These key opinion leaders were identified based on their clinical roles, ACP-related administrative roles, or through professional contacts. As the activity was designed to be a stakeholder dialogue, we did not collect additional information to profile the participants. However, we are aware that 82% of the participants were female, and all participants were English-speaking.
Target population, scope, and goals of ACP
There was overall agreement that the target population of ACP conversations should include persons aged 21 years old across all states of health who have the mental capacity for decision-making. Most participants emphasized the importance of explicitly considering the role of ACP for persons with cognitive impairment, children, or young persons with serious illness, alongside establishing safeguards for proxy involvement. Some participants expressed that ACP should exclude individuals without decision-making capacity and that a separate definition for conversations about care could be created for persons with special needs. One group suggested differentiating ACP based on whether it was completed by the individual or a proxy, and whether it pertained to code status or resuscitation decisions made by the health care team. Ultimately, no substantive conclusion was achieved during the World Café regarding the categorization of conversations by type.
Across the five World Café groups, ACP was viewed as an ongoing process of conversations that should be reviewed in accordance with changing life and health circumstances. The groups agreed that the discussion should include the individual, health care proxy, and other loved ones chosen by the individual, as well as a trained facilitator such as someone from the care team. The ACP discussion should cover the individual’s values and preferences as well as current goals of care, care plans, and preferences for future medical care. It is necessary to document the content of the discussion. In the event that the individual loses the capacity to make decisions, future care teams can access the ACP document and consult with the individual’s nominated health care proxies on his/her prior expressed preferences. Documented preferences should be reviewed in a timely manner and be updated with any changes that might have occurred.
Some participants shared that ACP should include preferences beyond medical priorities, but the majority thought the scope should be limited to treatment and care options to be coherent with the original objective of guiding medical decision-making should an individual loses capacity to do so. Some participants opined that the ACP process should focus on a conversation about one’s beliefs, values, and preferences but should not culminate in a decision about care, as the decision legally rests with the attending physician in the local context. This resulted in a broad agreement among the World Café participants to refrain from including the term “decisions” as part of the definition.
The World Café participants further agreed that the ACP process should aim to encourage conversations between individuals, their loved ones, and the health care team, promote person-centered care, build trust, and to respect the voice of the individual.
Process of ACP
The voting results from the Mentimeter (yes—21, 61%; somewhat—13, 39%) reflected strong agreement that the ACP lifecycle encompasses initial advocacy, facilitation and documentation, and finally, respecting the voice of the individual in clinical decisions (Fig. 2). The ACP process should encourage individuals, with the support of their health care proxies, to initiate ACP conversations and complete the documentation of their values and care priorities. This will allow the health care team to advocate for his or her preferences in the event that the individual is unable to make health care decisions in the future.
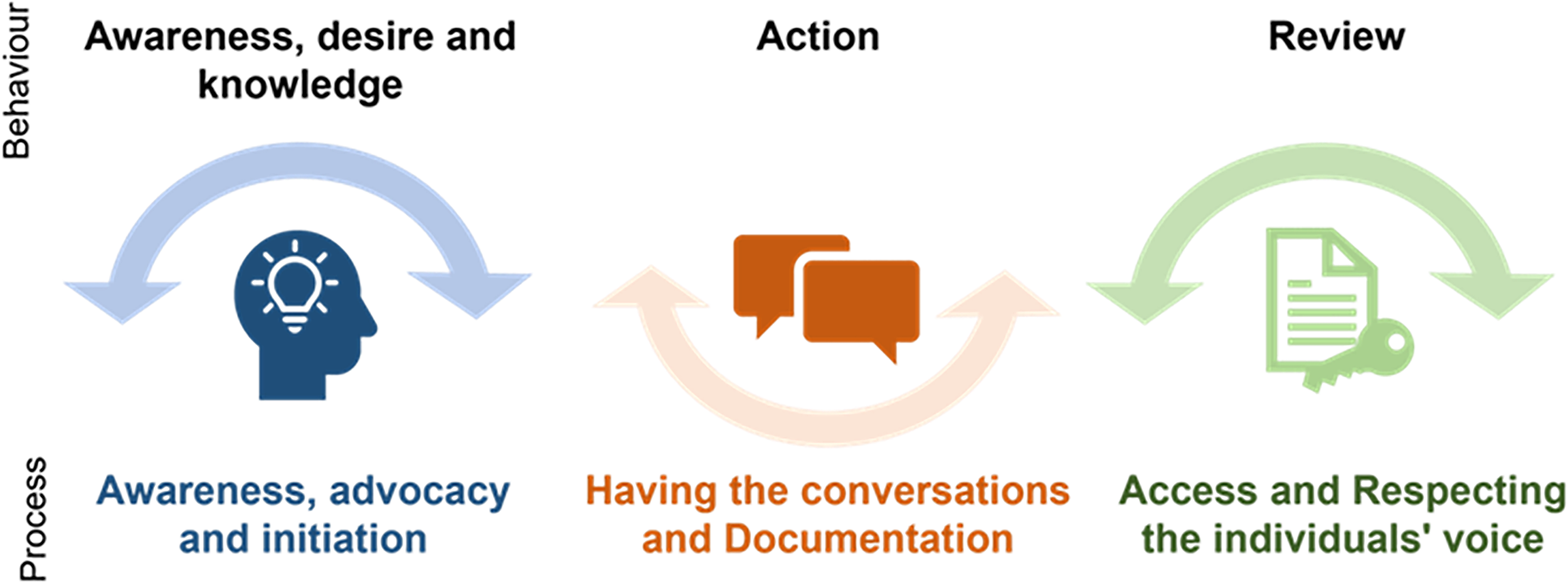
Intended behaviors and process of advance care planning.
Reflecting the level of perceived importance in addressing barriers to ACP implementation in Singapore, the voting results illustrated that 16 out of 34 participants (47%) perceived that we should urgently address low public receptivity to ACP by introducing strategies to enhance awareness, advocacy, and systematic implementation to normalize ACP as part of person-centered care. Participants also highlighted the importance of ensuring greater readiness in having the conversations (24%) and ensuring that discussions are documented and accessible across different care settings (27%).
Quality indicators
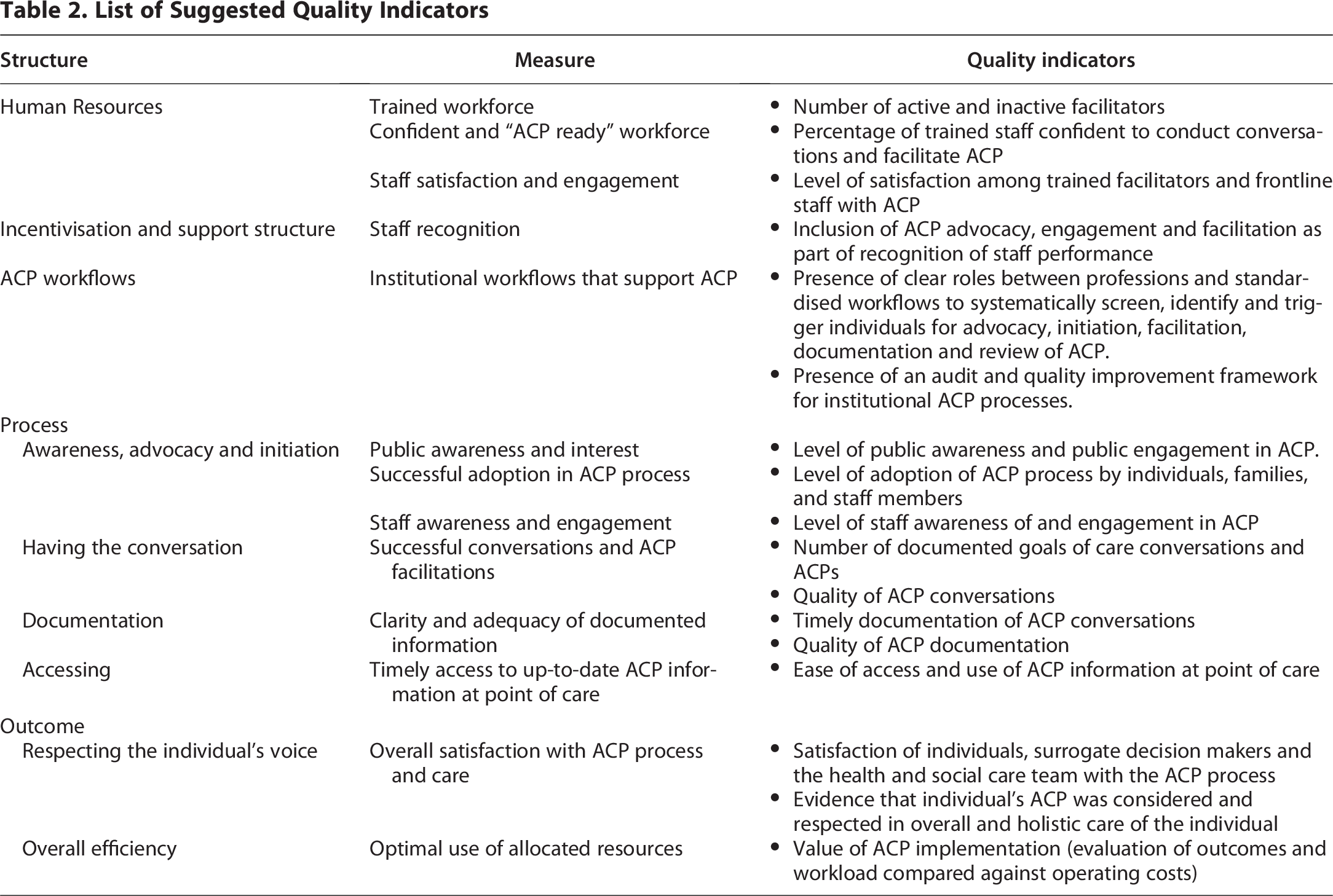
The World Café session yielded key quality indicators for measuring system readiness, implementation, and effectiveness. Successful implementation requires a comprehensive approach integrating human resource support, structured workflows, and person-centered care. Ensuring respect for individual voices while meeting efficiency metrics is a critical driver of organizational sustainability. We have organized the measures to aid the monitoring and evaluation of the quality of ACP implementation in terms of these three constructs: structure, process, and outcome. Structure refers to the organizational resources, facilities, and policies in place for ACP implementation. The process involves the activities and interventions carried out in relation to the phases of ACP implementation. Outcome indicators should reflect the results and effectiveness of ACP with reference to its intended goals. In line with the definition and scope of ACP (Table 1), the participants of the World Café did not include goal-concordance as an outcome.
Summary of World Café Discussion About Definition and Scope of ACP

Table 2 provides a list of quality indicators derived from the World Café discussion and agreed upon by its members. Organizations at different stages of ACP implementation may have different priorities and, therefore, establish varying short-, medium-, and long-term objectives. The indicators can be used to monitor the progress toward pre-specified targets.
List of Suggested Quality Indicators
Discussion
In this study, ACP is conceived as an ongoing process of exploring an individual’s personal beliefs, values, and health care preferences in relation to current and future medical care, together with their families and loved ones. The World Café adopted an inclusive approach, advocating for the involvement of children, youths, and persons with cognitive impairment, provided safeguards are in place for these vulnerable populations. The resulting scope of ACP reflects the collectivist culture of the Singaporean society, where family members share the responsibility for each other’s well-being. To achieve the intended outcome of respecting the individual’s voice, organizations must systematically monitor specific structural and process factors due to their complex dependencies with organizational culture and the broader health care system.
Our definition of ACP aligns with the European as well as Asian consensus definitions.8,9,17 In Singapore and other East Asian jurisdictions such as Taiwan 18 and Japan, 13 the definition of ACP recognizes personal autonomy but also strongly reflects the collectivist culture of the Asian societies where collaborative decision-making13,19,20 is prevalent, and relational autonomy and familial harmony is a priority. 21 To be coherent with the realities of multicultural, family-centric communities, ACP in Singapore therefore needs to encompass and consider individuals’ familial networks, 22 and foster open communication and explore treatment options that respect the individual’s autonomy. Whereas in countries like Australia 23 and England, 24 ACP remains fundamentally built on principles of self-determination, placing significantly less emphasis on familial decision-making.
The World Café discussion highlighted the practical necessity of including children and youth with serious illnesses, as well as persons with cognitive impairment, in ACP conversations. This shift reflects an evolution in Singapore’s pediatric end-of-life care from a purely parent-led model to a collaborative approach that emphasizes the values, goals, and preferences of the child. 25 Simiarly, there is also growing recognition in Singapore 26 and internationally that the ACP process should be dynamically adapted to match the cognitive capacity of persons living with dementia. 10 To protect these populations from coerced or poorly understood decisions, specific clinical and ethical safeguards should be implemented.
Our findings indicate that facilitated and structured ACP sessions are preferred over self-directed methods because facilitators provide active support, which reduces uncertainty and fosters more informed decision-making. Evidence suggests that trained facilitators help patients and families navigate complex decisions by clarifying personal values, reducing uncertainty, and addressing specific queries. 27 Nonetheless, to empower generally healthy, digitally literate individuals to start planning independently, the Singapore Ministry of Health launched a digital ACP tool, myACP in July 2025. 5 While facilitated ACP sessions remain the gold standard for patients with complex or serious illnesses, this digital option offers a convenient, cost-free option for healthy individuals. Interpersonal interaction in a facilitated session offers comfort and support, while digital platforms offer convenience, flexibility, and personalized pacing. 28 Both approaches have their merits and can be used in conjunction with each other.
Legislative differences across jurisdictions have a bearing on which goals are realistically achievable. The World Café participants emphasized that an ACP should not culminate in a definitive decision about care. In Singapore, the attending doctor remains the legal decision-maker for patients lacking capacity in matters of life-sustaining treatment; however they must take all relevant circumstances into consideration including the persons’ past and present wishes, especially those documented while the person had mental capacity. Families and appointed legal representative should be consulted on the person’s likely choices for a comprehensive decision that is in the patient’s best interests. 29 Because concordance with documented care preferences is influenced by circumstances at the end-of-life, it should not serve as an indicator of ACP quality itself. Hence, goal concordance was excluded from the current list of recommended quality indicators, as it is recognized that multifaceted interventions 30 and a systems approach are required.31,32 Greater commitment to address systemic barriers in the future may shift our current views about the relevance of goal-concordant care as a primary outcome indicator. The selection of appropriate outcomes for ACP should cater to evolving empirical research, advances in measurement approaches, and shifting cultures of care. As a process, ACP as a process remains highly complex and multidimensional, with many interlinked factors and outcomes.
Specifying the goals of ACP is crucial for determining the resources and processes necessary to achieve these intended objectives. 33 To this end, we must start by measuring and assessing the structural factors and processes. Past studies have emphasized the quality of the documentation process 34 or focused on establishing the range of outcomes to measure the success of ACP initiatives.33,35 However, few have called for a systematic collection of performance data to monitor whether organizational resources and policies as well as the process of initiating and facilitating ACP discussions are designed and resourced to respect the voice of the individual person. Framing the quality measures within a structure, process, and outcome framework supports a virtuous cycle of continuous quality improvement. This approach provides actionable information on implementation obstacles, informs the design of implementation strategies to overcome identified bottlenecks, facilitate learning, and enhances accountability for the use of public and organizational resources. 36 This list of indicators contributed toward the final list of indicators shared in the Guidelines for Quality Implementation of ACP, which was disseminated for use by health and social care providers implementing ACP in their settings in Singapore.
Study limitations
The findings of the study have to be interpreted in view of its limitations. First, we sought the views of key opinion leaders who were at the forefront of practice and research of ACP in Singapore. While a variety of perspectives were included, the specific views of our World Café participants cannot be generalizable to any larger populations. Second, individuals who attended the session may be more interested in having their views represented compared to those who did not or could not attend. We attempted to mitigate this by seeking the views of individuals who were invited but could not be present at the World Café session.
Conclusion
Findings from this study have helped anchor and articulate the intended target population, scope, and goals of ACP in Singapore. A definition that includes children, young persons, and older persons with progressive cognitive decline positions ACP as an ongoing, and person-centered communication process accessible to all people. The findings from this study supported development of the Guidelines for Quality Implementation of ACP, which was launched in May 2025. The guidelines served to recommend quality indicators and good practice principles to promote a consistent approach to ACP implementation across various health care settings. Such a process of stakeholder engagement and consensus building encourages organizations toward adopting robust and pragmatic ways to drive ACP implementation in Singapore.
Authors’ Contributions
The study was conceptualized by W.S.T., J.L., and R.N. J.L. and W.M.W. secured resources for the study. W.S.T., P.L., J.L., and R.N. contributed to the design of the study and facilitated the World Café. W.S.T. analyzed the data and wrote the first draft of the article. All authors interpreted the findings, reviewed and edited the article.
Footnotes
Acknowledgments
The authors would like to thank the World Café participants for their participation and contributions. In addition, they would thank Jane Lim and Priscilla Lim (Agency for Integrated Care, Singapore) and Chou Chuen Yu and Nongluck Pussayapibul (Geriatric Education and Research Institute, Singapore) for assisting in the facilitation of the World Café session; and Norhidayah Ishak and Charlotte Ong (Geriatric Education and Research Institute, Singapore) for providing administrative support. The authors acknowledge Phui Ching Lai (Agency for Integrated Care, Singapore) and Chetna Malhotra (Lien Center for Palliative Care, Duke-NUS Medical School, Singapore) for their contributions to the preliminary discussion of the results. The authors also sincerely thank the following members of the National Quality Implementation Workgroup for their contributions:
Lee Beng Ang, KK Women’s and Children’s Hospital, Singapore
Cindy Lau, National Heart Center, Singapore
Jamilah Jailani, National University Polyclinics, Singapore
Jamine Tan, Tan Tock Seng Hospital, Singapore
Koh Lip Hoe, Changi General Hospital, Singapore
Lee Guo Zhang, Singapore General Hospital, Singapore
Shi Jin, Sengkang General Hospital, Singapore
Shirlyn Neo, National Cancer Center, Singapore
Shirlynn Ho, National Cancer Center, Singapore
Sim Lai Kiow, Khoo Teck Puat Hospital, Singapore
Sim Siew Ting, Ng Teng Fong Hospital, Singapore
Teng Sook Fong, Alexandra Hospital, Singapore
Yeo Hui Nan, National University Polyclinics, Singapore
Wong Wei Teen, SingHealth Polyclinics, Singapore
Author Disclosure Statement
The authors declare that the study was conducted in the absence any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This project was co-funded by the Geriatric Education and Research Institute [BRF-2023-006], and the Agency for Integrated Care.