
Abstract
In acute spinal cord injury (SCI) patients who had lumbar intrathecal catheters inserted for cerebrospinal fluid (CSF) drainage and augmentation of spinal cord perfusion pressure (SCPP), we sought to characterize how neurologic recovery was related to aspects of this hemodynamic management approach. This prospective multi-center nonrandomized interventional clinical trial was conducted at eight level-1 trauma centers in North America with specialized units for SCI care. Twenty-seven patients presenting with motor-sensory complete SCI (AIS grade A) had catheters inserted for up to 7-days post-injury for CSF drainage and SCPP augmentation. Mean arterial pressure, intrathecal pressure (ITP), SCPP, ITP waveform morphology, and CSF drainage volume were collected hourly. Neurologic assessments were repeated at 6-months post-injury to determine if AIS grade conversion/improvement had occurred. Hemodynamic measures associated with the outcome of being an AIS grade “converter” or “non-converter” were compared. Of the 27 AIS A participants at baseline, 8 experienced neurologic recovery reflected by AIS grade conversion at 6-month follow-up (converters); 19 remained AIS A (non-converters). Converters were characterized by a higher ITP, lower SCPP, greater CSF drainage volume, and a more pulsatile ITP waveform morphology than nonconverters. In patients with AIS A SCI, AIS grade conversion at 6 months was associated with a specific pattern of hemodynamic measures that we hypothesize reflect a complete decompression and restoration of CSF flow in the subarachnoid space at the injury site. These metrics may provide guidance and/or targets for future studies on the management of acute SCI.
Introduction
The management of patients with traumatic spinal cord injury (SCI) during the acute and early sub-acute phases aims to limit secondary injury 1 and enhance long-term recovery potential of motor and/or sensory function.2,3 Timely surgical decompression and aggressive hemodynamic management within the first week post-injury are the primary treatment modalities in acute SCI. 4 Despite clinical practice guidelines indicating augmentation of mean arterial pressure (MAP) for 3–7 days post-injury, the evidence for the relationship between hemodynamic management and neurologic outcome is generally weak.5,6 Hence, identifying characteristics of the hemodynamic management in individuals who experience neurological recovery following acute traumatic SCI may help in identifying specific approaches that can direct early care and improve outcomes.
We previously reported that spinal cord perfusion pressure (SCPP), calculated as the difference between MAP and the pressure within the intrathecal space (i.e., intrathecal pressure [ITP]), may be a better predictor of American Spinal Injury Association Impairment Scale (AIS) grade conversion than established MAP targets 7 as SCPP theoretically better reflects perfusion and oxygen delivery to the cord than MAP. SCPP may be increased by elevating MAP or reducing ITP. 8 The reduction of ITP via drainage of cerebrospinal fluid (CSF) through an indwelling lumbar intrathecal catheter is a common neuroprotective strategy in thoraco-abdominal aortic aneurysm repair surgery to reduce the risk of ischemic paraplegia. 9 To date, there are three studies that have evaluated CSF drainage in the setting of traumatic SCI, although conclusions regarding its effect on neurologic outcomes are difficult given their small sample sizes.10–12
With a lumbar intrathecal catheter in place, one can both monitor ITP and drain CSF to lower ITP. Additionally, the ITP waveform morphology may be observed, which may be “flat” or varying degrees of “pulsatile.” There are two schools of thought on the cause of the pulsatility in the ITP waveform; one being that the waveform primarily reflects pulsations of the spinal arteries,13,14 the other that the waveform represents intracranial arterial pulsations that are transmitted through the CSF within the subarachnoid space (SAS).15,16 Our own observations support the latter theory, as we have previously noted the association between a compressed/occluded SAS at the injury site with a flat ITP waveform, and a decompressed/patent SAS at the injury site with a pulsatile ITP waveform. 10 These observations suggest that the pulsatility of the waveform may be used as a biomarker of SAS patency and the extent to which the spinal cord has been decompressed at the injury site.
We recently conducted a prospective multicenter nonrandomized interventional clinical trial to investigate the influence of CSF drainage on SCPP and neurological recovery in the first seven days following SCI (the Canadian-American Spinal Cord Perfusion Pressure and Biomarker Study [CASPER], ClinicalTrials.gov ID: NCT03911492). 17 In doing so, we found that the hemodynamic management protocol was influenced by surgical management (specifically, the extent of decompression and ability to restore CSF flow around the injured cord) and made a number of qualitative observations regarding the associations between the ITP waveform morphology, ITP, SCPP, CSF drainage, and neurological recovery. The purpose of the present study was to (1) further explore these observations by quantitatively examining differences between participants who experienced positive AIS grade conversion and those who did not, and (2) describe patterns of positive AIS grade conversion in participants with acute, motor and sensory complete, traumatic SCI at admission.
Methods
Overview
The CASPER trial was a multi-center interventional clinical trial conducted at 8 North American sites: The University of British Columbia (Vancouver), University of Toronto (Toronto), University of Montreal (Montreal), and Dalhousie University (Halifax), University of Pittsburgh (Pittsburgh), University of Nebraska (Omaha), University of California, San Francisco (San Francisco), and University of New Mexico (Albuquerque). Multicenter recruitment for the CASPER trial occurred between August 2017 and March 2024.
The larger study aimed to manage patients with acute traumatic SCI for up to seven days post-SCI with a target SCPP of ≥ 65 mmHg through a combination of (a) MAP augmentation and (b) CSF drainage to reduce ITP. 17 The protocol followed by critical care bedside nurses indicated that if the patient was normotensive but their SCPP < 65 mmHg nurses were to examine their ITP and ITP waveform morphology. As described above, the ITP waveform was monitored and interpreted as a proxy measure of the patency of the SAS, whereby a flat waveform was deemed to reflect occlusion of the space at the injury site. A waveform with some degree of pulsatility was deemed to reflect enough patency of the SAS to transmit waveforms across the injury site to the lumbar catheter. When SCPP < 65 mmHg and ITP > 15 mmHg with a fully or dampened pulsatile waveform, CSF was to be drained to lower ITP to 15 mmHg. CSF was drained by bedside nurses via an indwelling lumbar intrathecal catheter levelled at the phlebostatic axis. If ITP was < 15 mmHg, then MAP was augmented to achieve a SCPP ≥ 65 mmHg. If the ITP waveform was flat, then the hemodynamic management reverted to conventional MAP augmentation. Ultimately, appropriate hemodynamic management was a clinical decision and could be altered at the discretion of the clinical team to achieve a SCPP ≥ 65 mmHg.
Because spontaneous recovery is more variable in incomplete injuries, 18 to address the objectives of the present study, we included a subset of participants who presented with motor and sensory complete SCI (AIS A) at enrolment and in whom an International Standards for the Neurological Classification of Spinal Cord Injury (ISNCSCI) exam was performed at 6-month follow-up. All study procedures were approved by the Institutional Clinical Research Ethics Boards, all participants provided informed consent, and the associated larger trial was registered at ClinicalTrials.gov.
Neurological examination
The motor and sensory function of individuals with SCI was assessed by the ISNCSCI exam. 19 Injuries were graded on a scale from AIS “A” to “E,” where AIS A represents a motor and sensory complete injury, AIS B represents a motor complete and sensory incomplete injury, AIS C and D represent varying degrees of motor and sensory incomplete injuries, and AIS E represents normal motor and sensory function. 19 Neurological recovery may occur in many ways, but operationally can be measured by improvements in motor or sensory scores, or improvement in the AIS grade. On the day of admission (or the following day if unable to do so at admission), the ISNCSCI exam was used to determine the neurological level and completeness of injury. 19 All participants were admitted within 24 h of their injury. A follow-up ISNCSCI exam was performed 6-months post-SCI. A follow-up window of 1 month past the due date was allowable. Neurological recovery was defined as a positive AIS grade conversion.
Pressure dynamics and vasopressor administration
MAP was measured by an arterial line and ITP by an indwelling lumbar intrathecal catheter. MAP, ITP, and SCPP were displayed on bedside monitors and reported each hour by critical care bedside nurses. Because previously established recommendations for the hemodynamic management of patients with acute SCI indicated maintaining MAP at 85 to 90 mmHg, 20 we calculated the percentage of all measures where MAP was between 85 and 90 mmHg as well as < 85 and > 90 mmHg. The percentage of MAP measures ≥ 85 mmHg was also calculated. As the goal of the larger study was to maintain SCPP ≥ 65 mmHg, the percentage of SCPP measures < 65 mmHg was calculated. The coefficient of variation (CV; i.e., standard deviation divided by mean multiplied by 100) of MAP was calculated as a measure of MAP variability. To quantify the exposure to low SCPP, the area under the curve (AUC) for SCPP measures < 65 mmHg was calculated as the sum of the extent to which measures were < 65 mmHg (e.g., a SCPP of 50 mmHg would be scored as 15) divided by the total number of SCPP measures (because not all participants were monitored for an equal length of time or had the same number of SCPP measures). Vasopressor administration was recorded hourly and the choice of vasopressor was made by individual institutions—for this reason, we only report whether a vasopressor was administered rather than the vasopressor dose.
ITP waveform morphology
Bedside nurses were trained on the interpretation of the ITP waveform morphology by a qualified research team member. Bedside nurses visually inspected the ITP waveform for ∼10 sec each hour, and based on their interpretation, recorded it as (a) flat, (b) dampened pulsatile, or (c) pulsatile. ITP waveform morphology is reported as the percentage of each morphology over the entire time that patients were monitored.
Statistical analyses
Differences in categorical variables related to demographics and injury characteristics at admission and 6-month follow-up between converters and non-converters were compared using Fisher’s exact test. Continuous data were first tested for normality using the Shapiro–Wilk test and non-normal data underwent square-root transformation. Differences in neurological outcomes, mean pressures, pressure distributions, vasopressor administration, total CSF drainage, and ITP waveform morphology between converters and non-converters were assessed by unpaired t-tests. Differences in pressures, and CSF drainage across the entire time participants were monitored were assessed using linear mixed-effects models with fixed effects for day post-injury, recovery parametrized as a two level-factor (converters and nonconverters), and recovery × day post-injury were performed to assess changes in outcome measures. Analyses were performed using IBM SPSS Statistics version 29 (IBM Corp., Armonk, NY, USA) and GraphPad Prism, version 9.1.0 (GraphPad Software, Inc., LaJolla, CA, USA). Group data are reported as the mean ± SD of individual participants mean ± SD data. Data are presented as mean ± SD unless noted otherwise and significance was set at p < 0.05.
Results
Participant demographics and neurological outcomes
Twenty-seven participants with acute, traumatic SCI determined to be AIS grade A at admission were included in the present analyses. All participants underwent surgical intervention with clinical decisions around surgical management made by the responsible clinical team. The lumbar intrathecal catheter remained in place for a median [IQR] of 152 [118–160] and 149 [90–160] h for converters and nonconverters, respectively. Not all participants were monitored for 7 days as—in some cases—the lumbar intrathecal drain was removed prematurely for clinical reasons; for example, if the participant was moved to a ward where lumbar drains could not be routinely managed.
Participant demographics and neurological outcomes at admission and 6-month follow-up are presented in Table 1 and Supplementary Table S1. There were no significant differences between groups at either time-point.
Participant Demographics and Neurological Outcomes
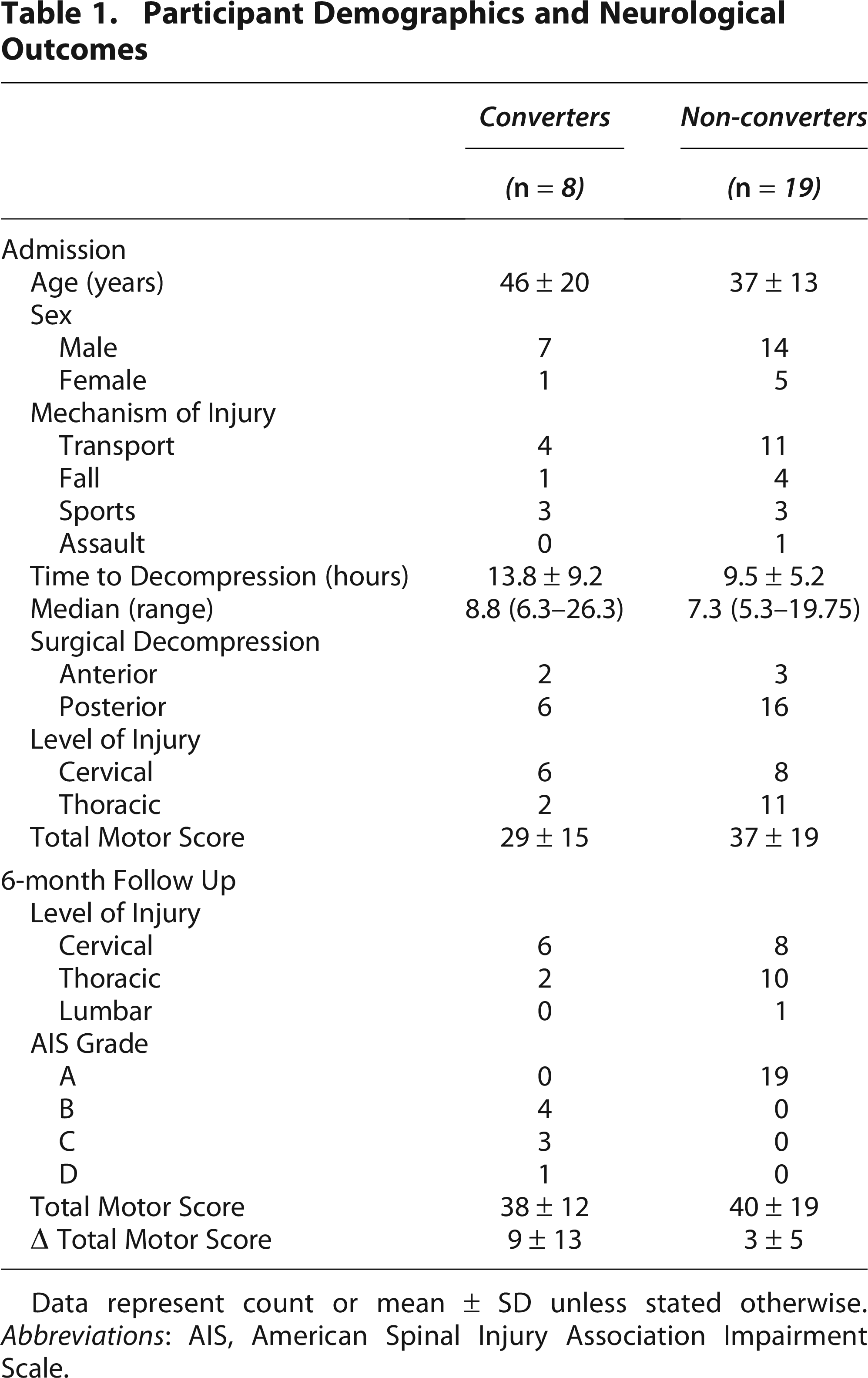
Data represent count or mean ± SD unless stated otherwise. Abbreviations: AIS, American Spinal Injury Association Impairment Scale.
Eight participants with complete SCI at admission experienced positive AIS grade conversion (46 ± 20 years, 7M/1F) at 6-month follow-up and 19 did not (37 ± 13 years, 14 M/5F). Among participants determined to be converters, four participants converted from AIS A to AIS B, three to AIS C, and one to AIS D.
Pressure dynamics and vasopressor administration
A summary of mean daily pressures is presented in Figure 1. There were no significant differences between converters and nonconverters mean MAP (90 ± 2 vs. 92 ± 5 mmHg, p = 0.268 [Fig. 1A]). Mean ITP was higher among converters than non-converters (17 ± 6 vs. 14 ± 4 mmHg, p = 0.160 (Fig. 1B)) resulting in mean SCPP being significantly lower in participants who experienced conversion (73 ± 6 vs. 79 ± 7 mmHg, p = 0.038 (Fig. 1C)).
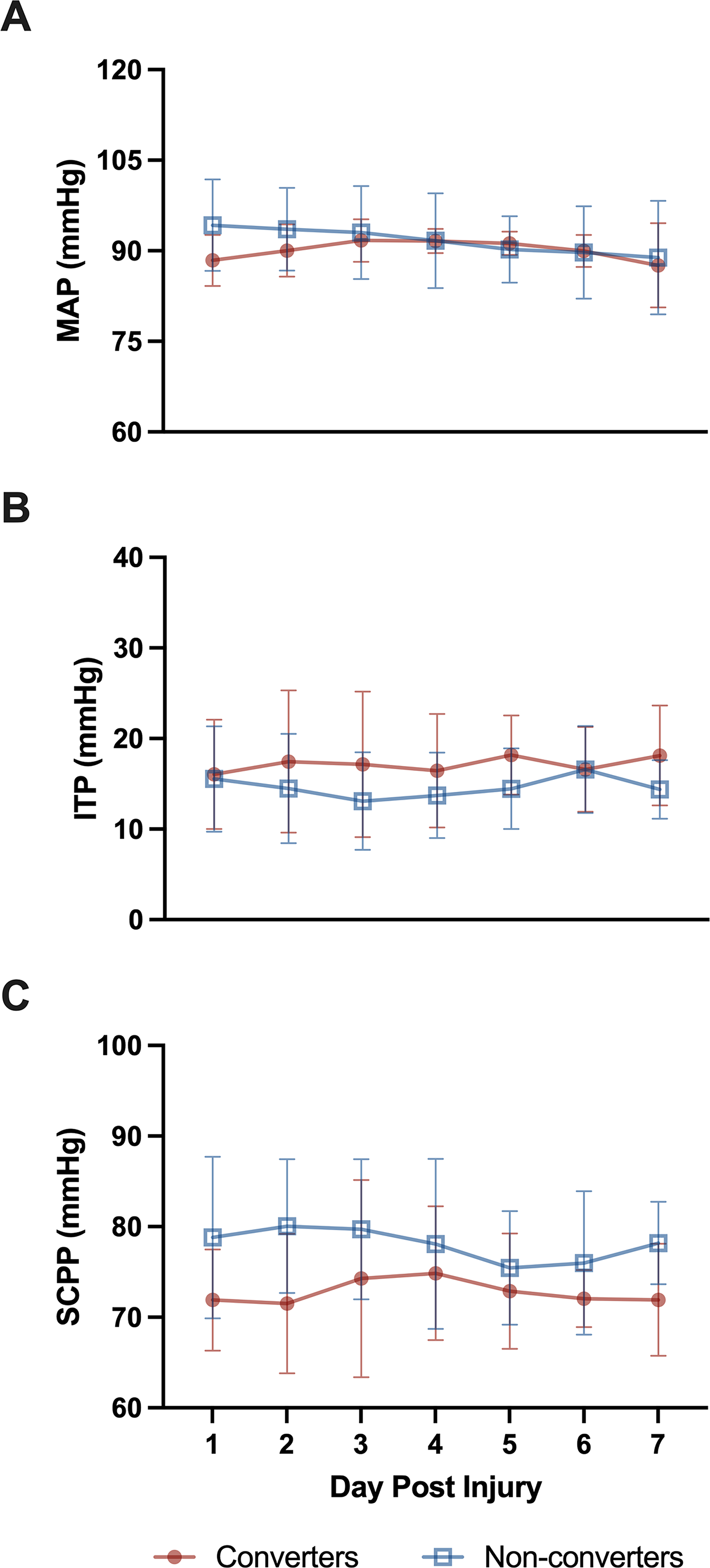
Summary of pressure dynamics. Data represent the daily mean ± SD
Specific pressure distributions, relevant to the objectives of the larger CASPER study are shown in Figure 1. Participants who experienced AIS grade conversion had a significantly greater percentage of MAP measurements in the range of 85 to 90 mmHg than non-converters (39 ± 14 vs. 24 ± 9%, p = 0.002 [Fig. 2A]). Converters had 16 ± 14% of MAP measures < 85 mmHg and 45 ± 12% of measures > 90 mmHg compared to 22 ± 12 and 54 ± 16%, respectively, in non-converters (both p > 0.164). The percentage of MAP measures ≥ 85 mmHg was not different between converters and non-converters (84 ± 14 vs. 78 ± 12%, p = 0.257 [Fig. 2B]). Participants who converted had less MAP variability (CV = 7 ± 3 vs. 11 ± 3, p = 0.006 [Fig. 2C]). Converters had a higher percentage of SCPP measures < 65 mmHg (16 ± 11 vs. 7 ± 6%, p = 0.015 [Fig. 3A]) and the exposure to SCPP < 65 mmHg (as reflected by the SCPP AUC) was greater in the converters than non-converters (0.8 ± 0.5 vs. 0.4 ± 0.4 mmHg/h, p = 0.022 [Fig. 3B]).
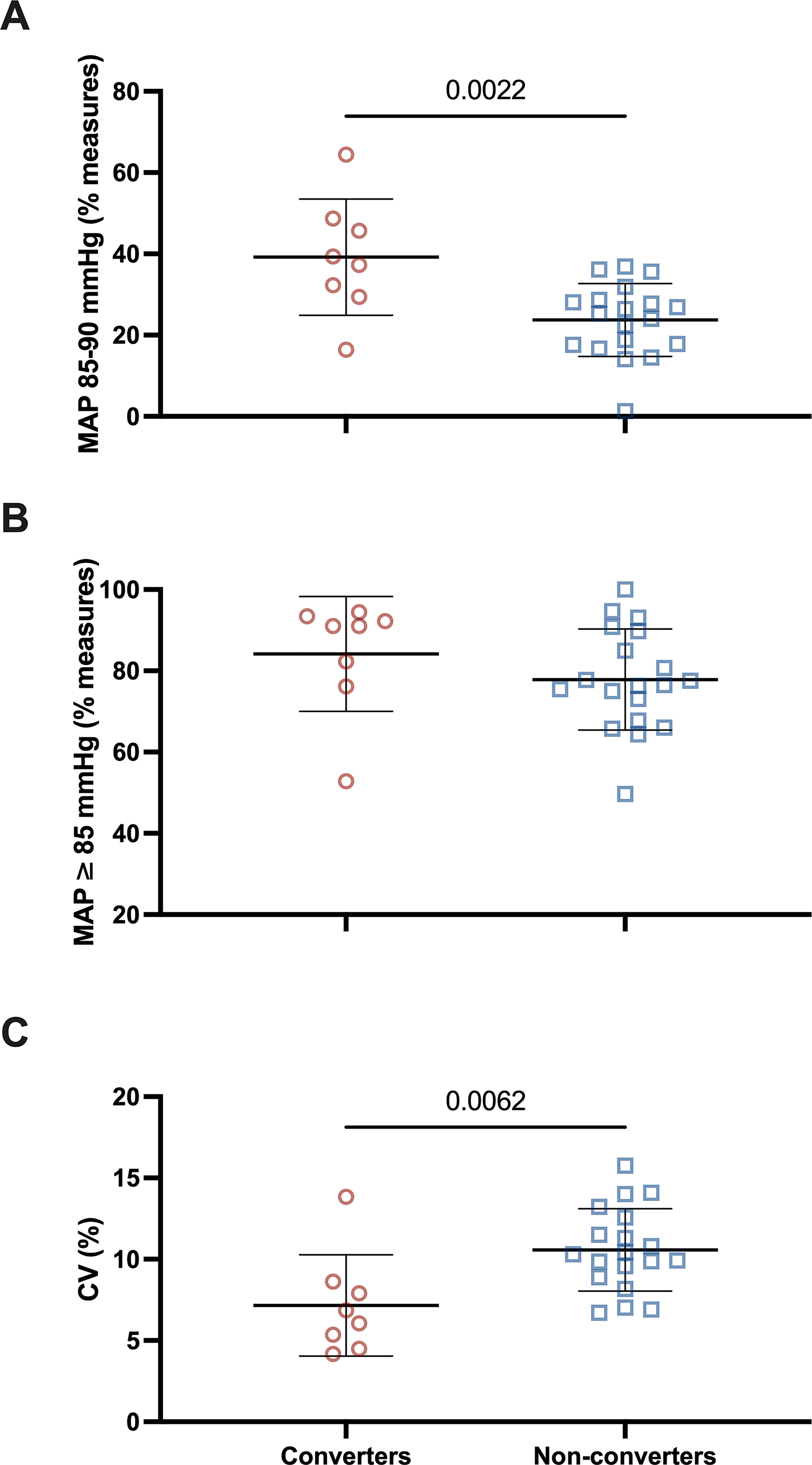
Distributions of mean arterial pressure. Each data point represent the mean value of one participant across 7 days of monitoring for
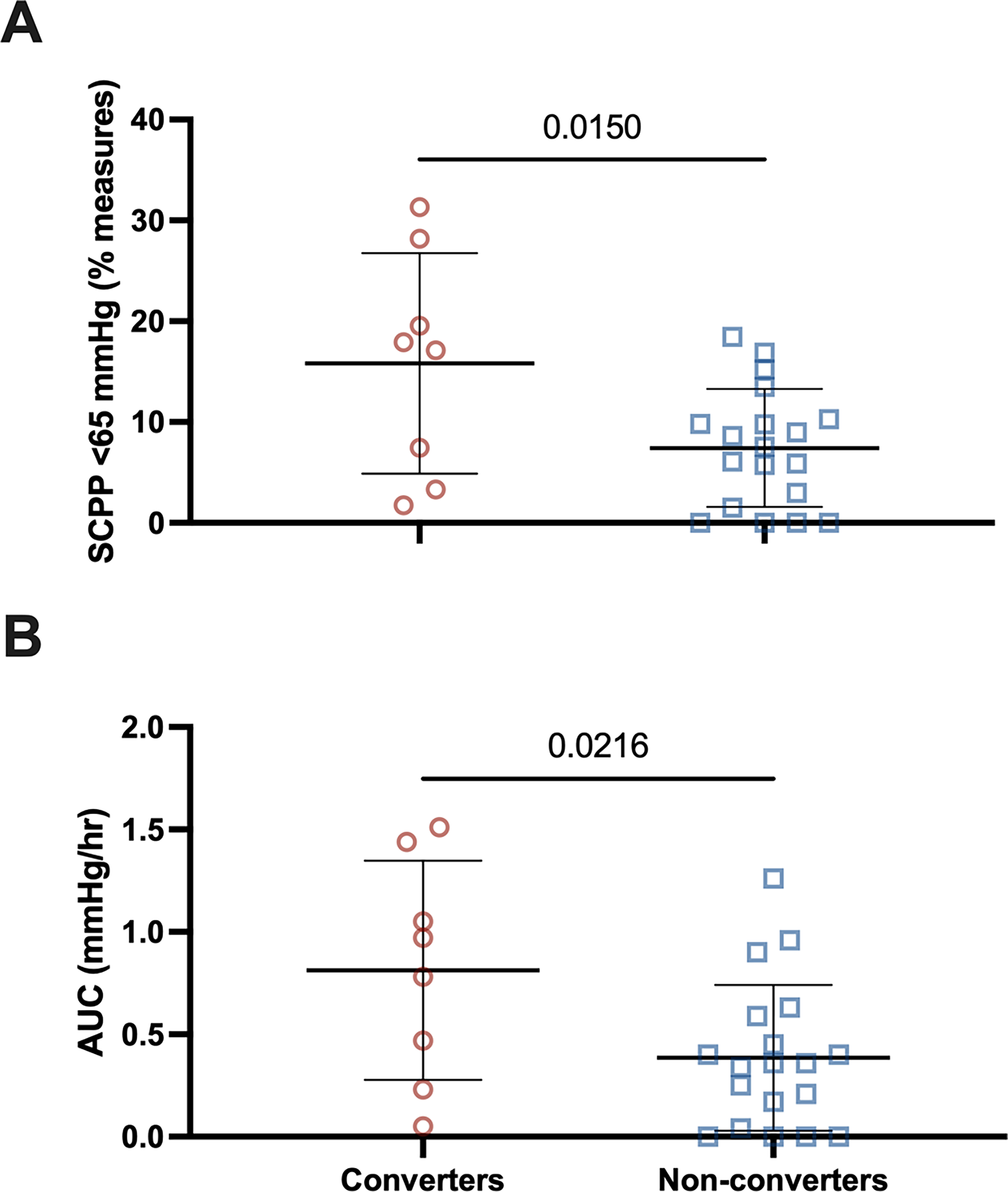
Distribution of spinal cord perfusion pressure. Each data point represents the mean value of one participant across 7 days of monitoring for
Converters received vasopressors on 100 ± 1% of observations, whereas nonconverters received vasopressors on 68 ± 42% of observations. However, this difference in vasopressor administration did not reach statistical significance (p = 0.071).
ITP waveform morphology
Converters had a greater percentage of ITP waveform morphology recordings determined to be pulsatile (25 ± 19 vs. 6 ± 13%, p = 0.019 [Fig. 4]). Fewer flat waveforms were observed among converters (23 ± 35 vs. 31 ± 35%, p = 0.777).
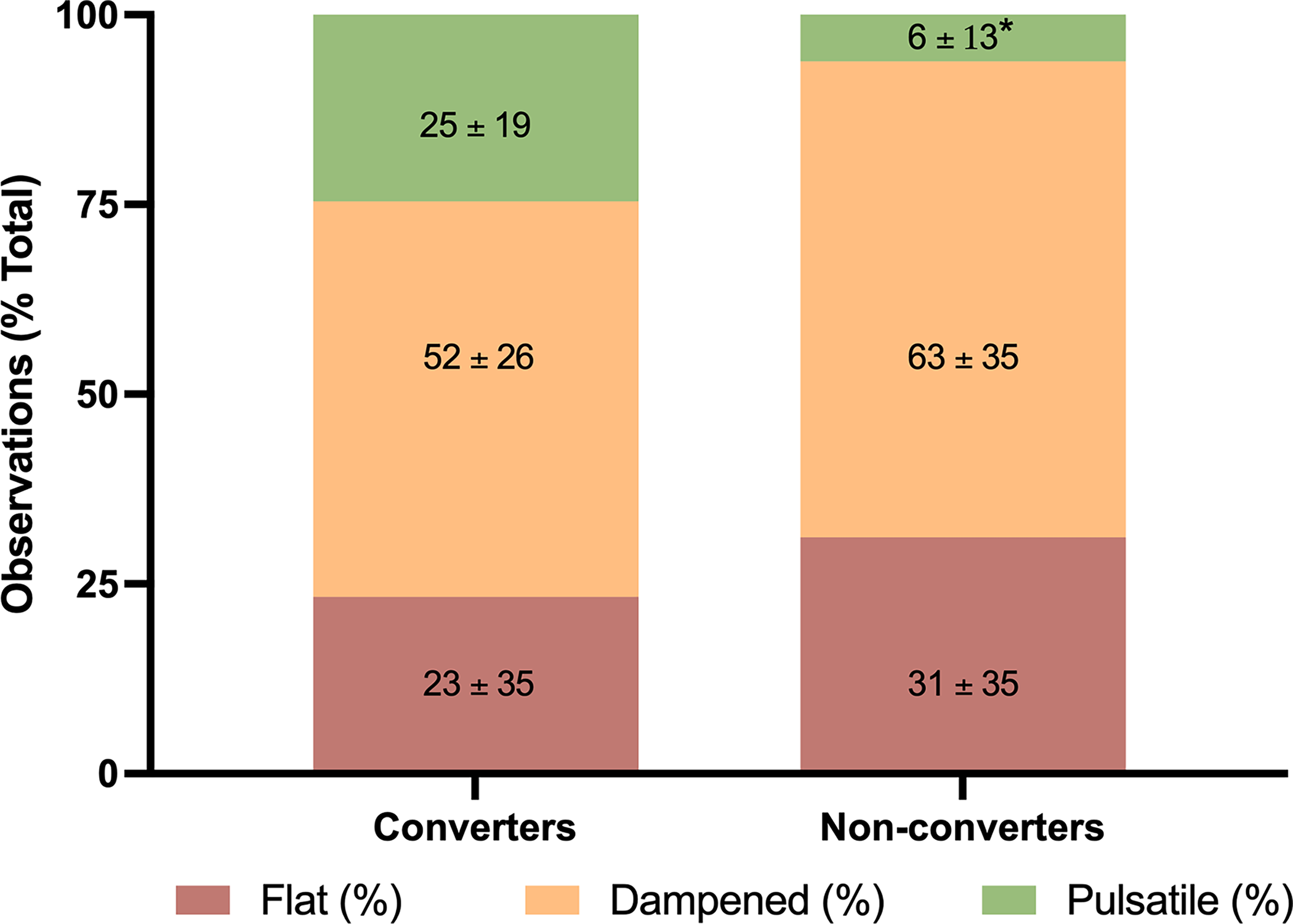
Intrathecal waveform morphology distribution. Data represent the mean ± SD percentage of waveform morphology measures as flat, dampened, or pulsatile for converters and non-converter groups across seven days of monitoring. Note that the converters had many more pulsatile ITP observations, suggesting that the SAS space was decompressed around the injury site. * indicates p = 0.019 vs. Converters.
CSF drainage
A larger volume of CSF was drained from participants who were converters compared to non-converters (median [IQR]: 695 [125–1611] vs. 343 [103–578] mL, p = 0.255)(Fig. 5). Post-hoc analysis did not reveal significant differences between groups on any one specific day post-injury. The drainage rate was also higher in converters than non-converters (median [IQR]: 4.2 [1.2–10.6] vs. 2.8 [0.8–5.1] mL/h, p = 0.308).
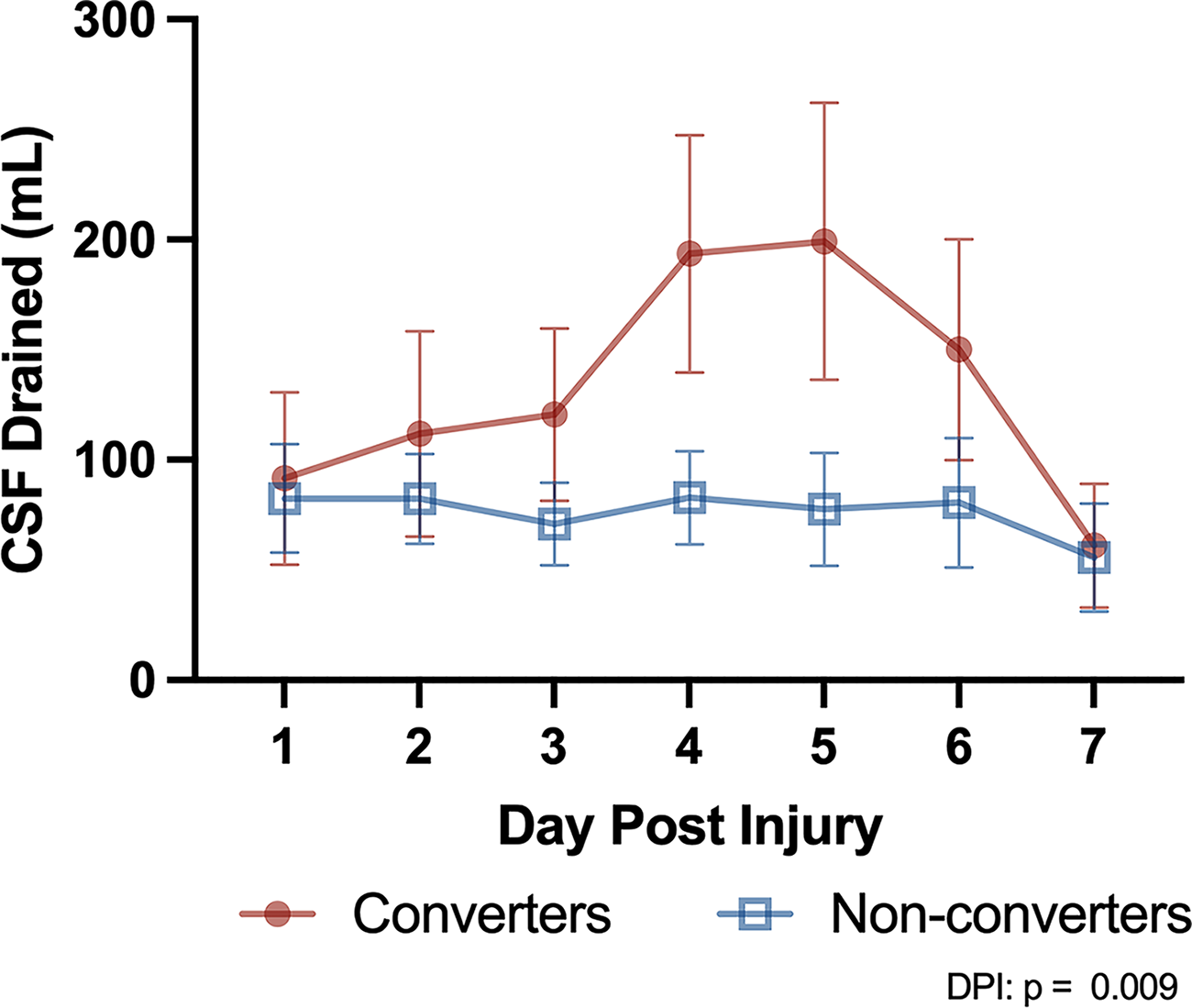
Cerebrospinal fluid drainage. Data represent the mean ± SEM volume of CSF drained each day for converters and non-converter groups across seven days of monitoring. Abbreviations: CSF, cerebrospinal fluid; DPI, day post-injury.
To provide a visual representation of all data collected over the time that participants were monitored and to better demonstrate the differences described above, example case summaries from one participant who did experience AIS grade conversion and one who did not are provided in Figure 6. These case summaries from two AIS A participants with differing neurologic outcomes exemplify the different patterns of hourly data regarding pressure dynamics, vasopressor administration, ITP waveform morphology, and CSF drainage.
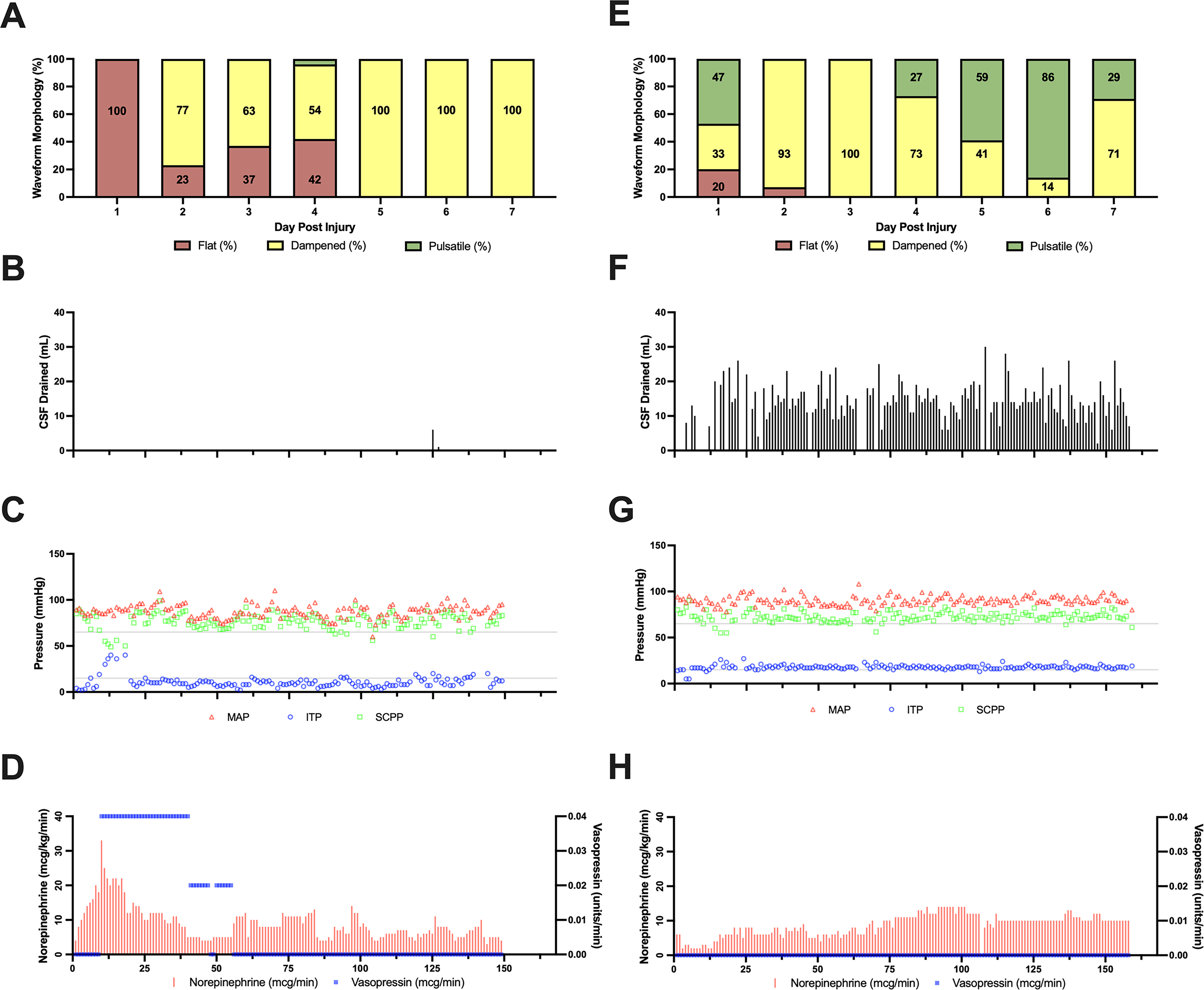
Example case summaries. These case summaries represent data collected in the Intensive Care Unit from a (left) 43-year old male admitted with a C6 motor-sensory complete SCI following a mountain biking accident who did not experience conversion and (right) 24-year old male admitted with a C4 motor-sensory complete SCI secondary to a C6 burst fracture from a diving accident who did experience conversion. Note that conversion was associated with the pattern of having a dampened or fully pulsatile ITP waveform, the ability to drain a significant amount of CSF, and a higher ITP.
Discussion
Our findings identify a set of hemodynamic management characteristics associated with neurological recovery following acute, traumatic, motor-sensory complete SCI. Positive AIS grade conversion was characterized by a more pulsatile ITP waveform morphology (reflective of a decompressed spinal cord and patent SAS around the injury site) that was associated with higher ITP, lower SCPP, and—in the context of individuals managed with CSF drainage—the ability to drain a greater volume of CSF. Additionally, converters had a greater percentage of MAP measures within the 85–90 mmHg range and MAP was less variable compared to nonconverters. These findings extend previous bedside observations on the relationship between surgical decompression, the ITP waveform morphology, pressure dynamics, and neurological recovery following acute traumatic SCI. 10
Understanding predictors, and interventions that can be implemented in the acute setting to enhance the likelihood, of neurological recovery can provide surgeons and critical care staff with direction in the management and care of patients with acute SCI. We believe our observations may be of interest to clinicians at centers where access to post-operative imaging to determine whether the injury site has been appropriately decompressed is limited. Intrathecal monitoring may also be considered as a surrogate measure of SAS patency to avoid the challenges of transferring critically ill patients to and from magnetic resonance imaging (MRI). Future studies may quantify how injury characteristics change over the course of acute SCI and how this is reflected, and may be determined, by intrathecal monitoring. Whether the hemodynamic characteristics associated with AIS grade conversion described here are similar in individuals with incomplete or nontraumatic SCI remains to be determined. Because of the considerable heterogeneity in those with incomplete injuries and fairly common occurrence of AIS grade conversion in AIS B and C patients, we focused this study on those with AIS A injuries only.
The topic of MAP management in acute, traumatic SCI has received much attention with recent clinical guidelines suggesting MAP be managed between 75–80 and 90–95 mmHg to optimize spinal cord perfusion. 6 While our findings around differences in MAP distribution and variability are interesting, we are cautious to make conclusions on the optimal MAP target for neurological recovery given the small sample size in the present study compared with studies on which established guidelines were developed.
Hemodynamic management characteristics associated with neurological recovery
In interpreting these data, we wish to explicitly state that we
It is important to acknowledge that CSF drainage for reducing ITP and increasing SCPP is feasible when the SAS is patent (reflected by the higher ITP and pulsatile waveform) and limited when the SAS is occluded (reflected by the lower ITP and flat waveform). If one were only to consider CSF drainage volume as shown in Figure 5, it would be easy to infer that greater CSF drainage led to AIS grade conversion. But one needs to consider that such CSF drainage is only possible when the surgical decompression has achieved a patent SAS. Combined, these data suggest that the mainstays of early management for acute SCI—surgical decompression and hemodynamic management—are in fact intricately related. A completely decompressed spinal cord with a patent SAS at the injury site allows for a higher ITP in the lumbar cistern, the reflection of intracranial arterial pulsations as a pulsatile ITP waveform, and effective CSF drainage through the lumbar catheter (associated with a higher chance of AIS grade conversion). Conversely, a compressed spinal cord with an occluded SAS at the injury site results in a lower ITP in the lumbar cistern, a flattened ITP waveform, and the inability to drain CSF (associated with a lower chance of AIS grade conversion).
We present hour-by-hour data of a prime example of a participant who exhibited the hemodynamic characteristics of conversion in Figure 6 and contrast their data to that of a nonconverter. The converter had a C4 SCI at admission and underwent an anterior vertebrectomy at the C6 vertebral level. Post-operative imaging revealed a patent intrathecal space indicating complete surgical decompression. This decompression was associated with a pulsatile to dampened pulsatile ITP waveform (collectively representing 97% of all measures), a mean ITP of 17 mmHg (only 9% of measures < 15 mmHg), and 1998 mL of CSF was drained in accordance with the trial protocol (see Fig. 6E–H). Six months post-SCI, this participant was neurologically assessed to be a motor and sensory incomplete (AIS C) SCI at the C7 neurological level. On the other hand, the nonconverter had a C6 SCI at admission and underwent a C4-C6 laminectomy and posterior fixation of C2-T2. Post-operative imaging indicated an incomplete decompression of the injury and this was associated with an ITP waveform morphology that was typically flat or noted to be “very dampened pulsatile” by bedside nurses (Fig. 6A). The mean ITP was only 12 mmHg with 84% of measures being < 15 mmHg (Fig. 6C–D). No CSF could be drained except for 7 mL at one time point when clinical notes suggest the waveform was briefly pulsatile before returning to dampened pulsatile when the participant was repositioned (Fig. 6B). At 6-month follow-up, this participant’s injury remained a motor and sensory complete SCI at the C5 neurological level.
We also note that in our analysis, there was one outlier who experienced AIS grade conversion but presented with nonconverter characteristics. This participant had a T10 SCI and a mean ITP of only 7 mmHg, 0 mL of CSF was drained, and the ITP waveform morphology was reported to be flat on 100% of observations. Aside from this one participant who experienced AIS grade conversion, all others who had a similar pattern of a primarily flat ITP waveform, low ITP, and limited CSF drainage did not experience conversion. It may be that the ‘converter profile’ described here is more relevant to higher-level injuries. Given the preliminary nature of this work, we wish to be clear that we do not suggest all individuals who sustain a thoracic SCI should receive a full surgical laminectomy/decompression. We acknowledge that there may be instances where the displacement and comminution will influence the surgeon to avoid performing a complete laminectomy for fear of unleashing significant CSF leakage through an irreparable dural tear and/or possibly also considering such a laminectomy to be futile due to the displacement and comminution. However, occasionally an adequate indirect decompression with SAS restoration may be achieved by performing a realignment and stabilization.
The importance of monitoring the ITP waveform morphology
Prompt surgical decompression is one of the few interventions to be associated with improved neurological recovery following acute traumatic SCI. 21 However, while the definition of a complete versus incomplete surgical decompression proposed by Aarabi et al. make sense conceptually, 22 without a pressure monitoring probe within the SAS at the injury site (as per the “intraspinal pressure” monitoring of Papadopoulos and colleagues 23 ), it remains impossible to know how much pressure is truly being applied to the injured spinal cord when CSF is not visualized around the injury site on post-operative MRI. Given the findings of the present study, we suggest that the ITP waveform morphology may be used to characterize the degree of SAS occlusion and potential intradural or extradural cord compression in the setting of acute traumatic SCI.10,24 However, we did not collect repeated post-operative MRIs on all participants to confirm the decompressive status of the injury as that wasn’t part of the larger study protocol. Therefore, we are unable to report further on the accuracy of monitoring the ITP waveform to assess SAS patency.
Further, our findings highlight the importance of a pulsatile waveform (reflecting surgical decompression), in settings where clinicians wish to drain CSF to reduce pressure around the injury site. If CSF is drained when the SAS is occluded, it is likely being drained from an intrathecal compartment that has formed below the level of the injury and will not reduce pressure at the level of the injury. 25 Further, if the injury is not appropriately decompressed and the SAS is occluded then ITP is unlikely to be reflective of the pressure around the injury and therefore SCPP will be inaccurate as a measure of cord perfusion and oxygen delivery at the injury site. In such cases where the waveform is flat, it may be advised to base clinical decisions on the MAP, for which updated clinical practice guidelines have been recently published. 6 This insight reinforces the importance of considering approaches to achieve a patent SAS such as multilevel posterior laminectomy/decompression and/or expansile duraplasty, and imaging modalities like intraoperative ultrasound to confirm SAS patency; these aspects may be associated with increasing the likelihood of neurological recovery in patients with severe traumatic SCI. 22
Study limitations
The present study is not without limitations. First, we wish to note that as SCPP is a metric calculated based on both MAP and ITP, both of which are subject to variability, there may be even greater variability in SCPP itself. Further hypothesis-driven studies are needed to understand the association between lower SCPP, surgical decompression and AIS grade conversion. Second, the use of the ITP waveform morphology as a biomarker is not yet well established and a rigorous operational definition of flat, dampened, and pulsatile does not exist. We acknowledge that there may be inter-rater variability due to the subjective nature of interpreting the waveform morphology, though maintaining the “dampened” and “pulsatile” descriptions was advocated by bedside nurses who felt that such a distinction could be made by simply observing the waveform. There is evidence to suggest that waveform analysis of the ITP (or intraspinal pressure), similar to that used to measure ICP in the setting of TBI, may be an effective way to remove such subjectivity. 26 However, study sites did not have the software necessary to collect high-frequency pressure measurements for offline analysis, which was not necessary to answer the primary objectives of the larger study. Finally, we note that the small sample size in the present analysis limits our ability to make inferences from the data; our observations should be interpreted with caution and considered hypothesis-generating rather than clinical guidance.
Conclusions
To summarize, these data suggest that a more pulsatile ITP waveform morphology (suggesting a decompressed spinal cord with a patent SAS around the injury site), higher ITP and subsequently lower SCPP, and the ability to drain a greater volume of CSF is associated with neurological recovery in individuals with acute, motor and sensory complete, traumatic SCI. We reiterate that we
Transparency, Rigor, and Reproducibility Summary
The study design was preregistered at ClinicalTrials.gov (ClinicalTrials.gov ID: NCT03911492). Because the present article reports on a secondary analysis of data, an analytic plan was not preregistered nor was a sample size calculation performed regarding the data presented here. Data collection was performed in accordance with the Declaration of Helsinki and all procedures were approved by the Clinical Research Ethics Board at each institute. This secondary analysis report data from 27 participants with acute, traumatic, motor-, and sensory-complete SCI at enrolment and in whom 6-month follow-up data is available. The intervention of CSF drainage was performed by bedside nurses who collected all hourly data. Neurological examinations were performed by attending physicians and/or nurses who are members of the clinical research team. Normality of all outcome data was assessed by Shapiro–Wilk tests and if not normal underwent square-root transformation. Data are available from the corresponding author on reasonable request.
Authors’ Contributions
CMG and BKK conceived and/or designed the work that led to the submission, interpreted the results, and drafted and revised the article for important intellectual content. All authors revised and approved the final version of the article and agree to be held accountable for all aspects of the work.
Footnotes
Acknowledgements
The authors would like to acknowledge the support of our funders—Praxis Spinal Cord Institute, Vancouver Coastal Health Research Institute, and Mitacs—for their support. We thank the Vancouver Spine Research Program for managing the multi-center study, data review/clean-up, & study support. We also thank the participants and their families for providing consent to our data collection that formed the present article and the intensive care staff who helped in collection of the data.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
This work was supported by a grant from Praxis Spinal Cord Institute (G2019-21).
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.