
Abstract
Severe traumatic brain injury (TBI) is a leading cause of pediatric mortality. Evidence-based Brain Trauma Foundation (BTF) guidelines promote best practices for severe TBI in the intensive care unit (ICU). We examined guideline, patient, and clinical care characteristics associated with early ICU guideline adherence. We used prospectively collected data from September 2019 to July 2020 from Argentina, Paraguay, and Chile. Patients ≤18 years with computed tomography evidence of TBI and Glasgow Coma Scale (GCS) score ≤ 8 or GCS motor score ≤ 5 at admission or at deterioration after admission were included. Cumulative ICU guideline adherence achieved during the first 3 days after TBI was analyzed by guideline recommendation (n = 15), recommendation category (n = 3), and patient and clinical care characteristics. Intergroup differences were compared using multivariate logistic regression with site-cluster adjustment. Among 116 patients, children were 1–4 years (38; 32.7%), male (74; 63.8%), and had extracranial injuries (77; 66.4%). Overall cumulative 3-day ICU guideline adherence rate was 81.3% (standard deviation: 13.0). Among the three guideline categories, adherence to the threshold category was higher than monitoring or treatment categories (p < 0.001). Adherence to the threshold category was lower in patients 1–4 years than 10–14 years (p = 0.02). Adherence to the monitoring category was lowest in minor/moderate Abbreviated Injury Scale and Injury Severity Score groups (p = 0.012 and 0.03, respectively). Ninety-five (81%) patients had nonadherence (0% adherence) to 1–3 recommendations across applicable BTF guideline recommendations. Overall, daily adherence rate was highest on ICU day 3 (p < 0.01). Early overall ICU guideline adherence rate was high but varied by recommendation, recommendation category, and patient characteristics. Nonadherence to a few recommendations was common, highlighting key targets for improvement and strategies to optimize guideline adherence in severe pediatric TBI.
Introduction
Traumatic brain injury (TBI) is a major global public health problem. 1 Children with severe TBI benefit from evidence-based critical care. 2 The 2019 Brain Trauma Foundation (BTF) guidelines are a set of evidence-based recommendations for the acute care of infants, children, and adolescents with severe TBI. Achieving early guideline adherence after severe TBI improves outcomes.2–4 In addition to guideline characteristics, factors such as patient and clinical care characteristics may affect achieving adherence to guideline recommendations, but these factors have not been studied.
The pediatric BTF guidelines contain 15 recommendations: 3 address monitoring, 2 address thresholds, and 10 address treatments. Achieving adherence to the guidelines may vary by both guideline category and specific recommendation3,5,6 and assessing differences in adherence may identify reasons for low and high guideline adherence and focus areas to improve guideline adherence. Moreover, patient characteristics such as extracranial injuries and clinical care characteristics may be associated with achieving high guideline adherence rates but are understudied. 7 The guidelines are considered an objective summary of available information, but barriers to implementation (such as interdepartmental cooperation and organizational support) may contribute to variation in guideline adherence. 6
Between 2017 and 2019, we implemented the PEGASUS (Pediatric Guideline Adherence and Outcomes) program, consisting of prompts for bedside providers, quality improvement initiatives, and case reviews to improve adherence to the BTF guidelines 2 in one site in the United States. From this work, we found robust improvements in adherence rates. Examining whether PEGASUS is generalizable to other real-world contexts was the next step. 8 In this analysis, we examined cumulative first 3-day intensive care unit (ICU TBI guideline adherence rates for BTF guideline categories and recommendations at 16 study sites in South America before testing and implementation of the PEGASUS program.
Methods
Study design and participants
We prospectively collected data from 16 participating sites in Argentina, Chile, and Paraguay between 2019 and 2020. Inclusion criteria were age ≤18 years with severe TBI (Glasgow Coma Scale [GCS] score ≤8 or GCS motor score ≤ 5) diagnosed by head computed tomography (CT) at admission or those with mild-to-moderate TBI (GCS score 9–15) who deteriorated to GCS ≤ 8 after admission. This study was approved as minimal risk by the institutional review board (IRB) at the University of Washington (STUDY00005629) and by all local IRBs. Legal guardians provided written informed consent.
Outcome
The main outcome was the 3-day cumulative guideline adherence rate during the first 3 days of ICU care, by guideline, patient, and clinical care factors. We calculated guideline adherence rates for each day for each applicable (based on clinical decision-making) BTF recommendation per patient, resulting in three response categories (adherent, not adherent, and not applicable). For recommendations that were a one-time action, we considered any adherence during the first 3 days to be 100% adherent; other recommendations used average daily adherence during the first 3 days, resulting in partial adherence for continuous actions. Then, we determined average three-day ICU guideline adherence rates for all applicable recommendations per patient (Supplementary Data S1).
Characteristics
Guideline characteristics
Adherence rates were calculated for the three published BTF guideline categories: monitoring, thresholds, and treatments. The monitoring category included neuroimaging, intracranial pressure monitoring, and advanced neuromonitoring recommendations. The threshold category included cerebral perfusion pressure and treatment of intracranial hypertension recommendations. The treatment category included corticosteroids, ventilation, cerebrospinal fluid (CSF) drainage, temperature control/hypothermia, seizure prophylaxis, barbiturates, nutrition, analgesics/sedation, hyperosmolar therapy, decompressive craniectomy, advanced neuromonitoring, and temperature control. Calculation of adherence to the hyperosmolar therapy recommendation was conditional on the presence of intracranial hypertension.
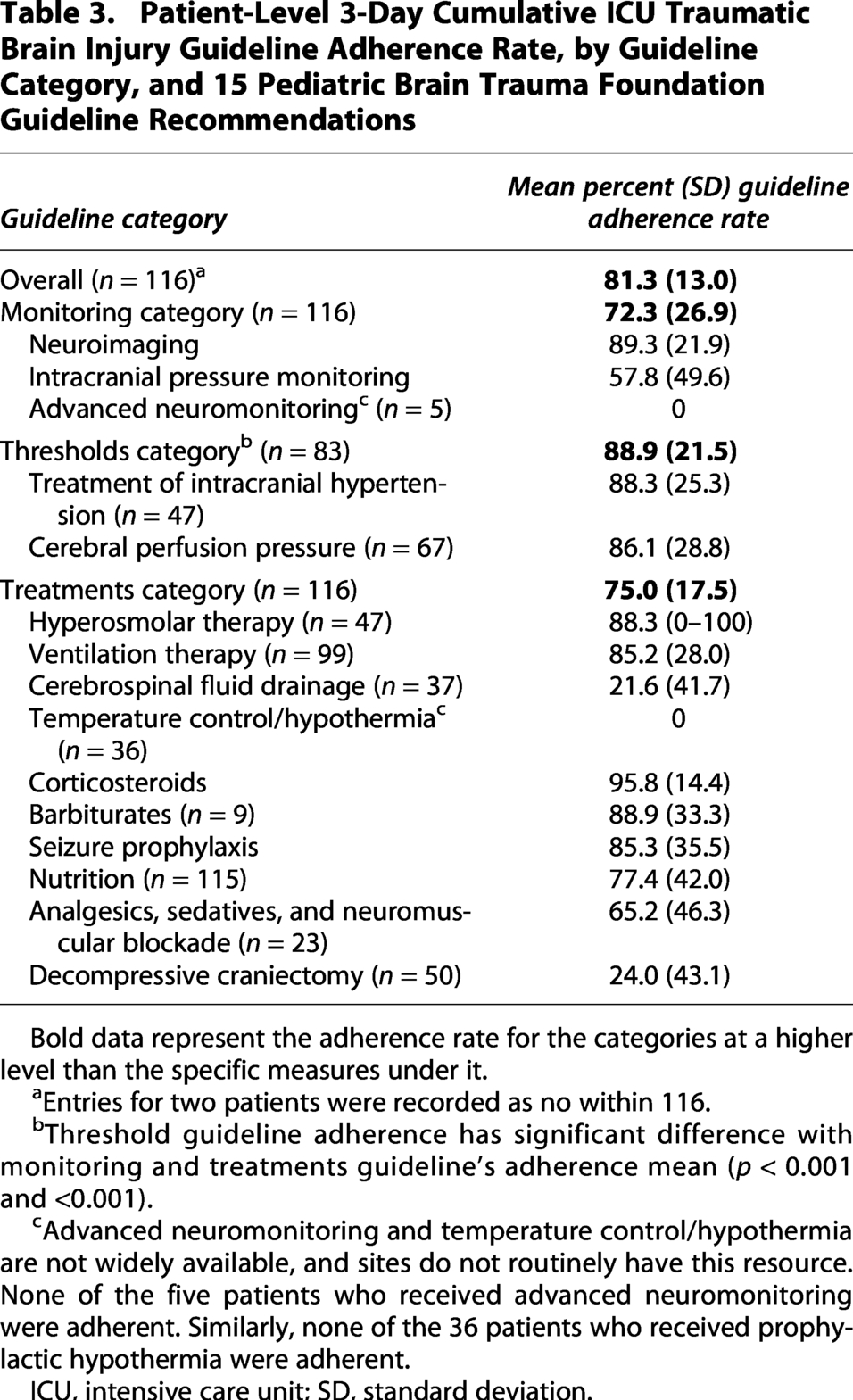
Patient-Level 3-Day Cumulative ICU Traumatic Brain Injury Guideline Adherence Rate, by Guideline Category, and 15 Pediatric Brain Trauma Foundation Guideline Recommendations
Bold data represent the adherence rate for the categories at a higher level than the specific measures under it.
Entries for two patients were recorded as no within 116.
Threshold guideline adherence has significant difference with monitoring and treatments guideline’s adherence mean (p < 0.001 and <0.001).
Advanced neuromonitoring and temperature control/hypothermia are not widely available, and sites do not routinely have this resource. None of the five patients who received advanced neuromonitoring were adherent. Similarly, none of the 36 patients who received prophylactic hypothermia were adherent.
ICU, intensive care unit; SD, standard deviation.
Patient characteristics
Patient characteristics were age, gender, extracranial injuries, and scores for total admission GCS, lowest (at admission or in-hospital deterioration) total GCS, lowest motor GCS, maximum head Abbreviated Injury Scale (AIS), injury severity (ISS), and Marshall CT classification. 9
Clinical care characteristics
Clinical care characteristics were the presence of any surgical procedure in the first 3 ICU days, ICU day of any such procedure, procedure type, and mechanical ventilation in the first 3 ICU days. Outcome characteristics were ICU length of stay and discharge Glasgow Outcome Scale (GOS) score.
Hospitals were categorized by hospital type, ICU beds per site, intensivists-to-bed ratio, and nurse-to-patient ratio. The intensivist-to-bed ratio was the number of full-time attending intensivists employed by the hospital per ICU bed, while the nurse-to-patient ratio was the number of on-duty nurses per ICU patient.
Statistical analysis
Using R programming and R Studio, we calculated frequencies and percentages for patient, outcome, and clinical care characteristics and summarized data using descriptive statistics. Mean and standard deviation (SD) were calculated for continuous variables, and counts (n) and percentage were used for categorical variables. Missing data were handled with complete case analysis.
For the TBI guideline adherence rates, we determined the mean and SD for overall guideline adherence, recommendation category (n = 3), and each guideline recommendation (n = 15) using equally weighted patient-level data. Next, we determined nonadherence (0% guideline adherence) for each guideline recommendation. We then determined the proportion of patients with nonadherence by the number of guideline recommendations.
To address the unequal sample sizes between guideline adherence categories, we used a linear regression model to determine differences in the mean percentage of guideline adherence rates among categories. The reference group was modified to compare each category with the other two, as linear regression with dummy variables requires adjusting the reference group to ensure all categories are fairly compared.
Total GCS score, surgery presence, extracranial injuries, hospital type (children’s only vs. mixed adult and children’s), and sex were coded as binary variables, with gender considered as biological sex. ISS, admission head CT results (Marshall score classification), discharge GOS score, and surgery type were coded as categorical variables. To examine differences across the age spectrum, children were categorized into groups: less than 1, 1–4 y, 5–9 y, 10–14 y, and 15–18. 10 AIS scores were stratified into three groups: minor/moderate (1, 2), serious/severe (3, 4), and critical/unsurvivable (5, 6). The lowest total GCS score at admission or in-hospital deterioration was categorized into four groups: 3–4, 5–6, 7–8, and 9–10. Additionally, the lowest motor GCS score at admission or in-hospital deterioration was categorized into three groups: 1, 2–4, and 5–6. The number of patients per study site and the number of ICU beds were treated as continuous variables.
We examined the distribution of TBI guideline adherence rates for each recommendation based on patient, outcome, and clinical care characteristics. For the overall guideline adherence rate for all 15 recommendations and for each guideline recommendation category, we examined differences across characteristic groups (guideline, patient, and clinical care). We use linear regression models, and for variables with more than two categories, we tested by changing the reference group to compare each with the others. A p value of <0.05 was considered statistically significant for the models. We accounted for site differences, recognizing that patient care at each site is consistent for individual patients but independent from other sites. Due to the small sample size of site-specific data, we did not test between site differences in guideline adherence rate. The same limitation applied to the variables ICU days and mechanical ventilation, which have overlapping values. Guideline adherence across ICU days was evaluated daily using Analysis of Variance (ANOVA) and Tukey’s post hoc test, including only patients who received ICU care for at least 3 days.
Results
Patients and clinical care characteristics
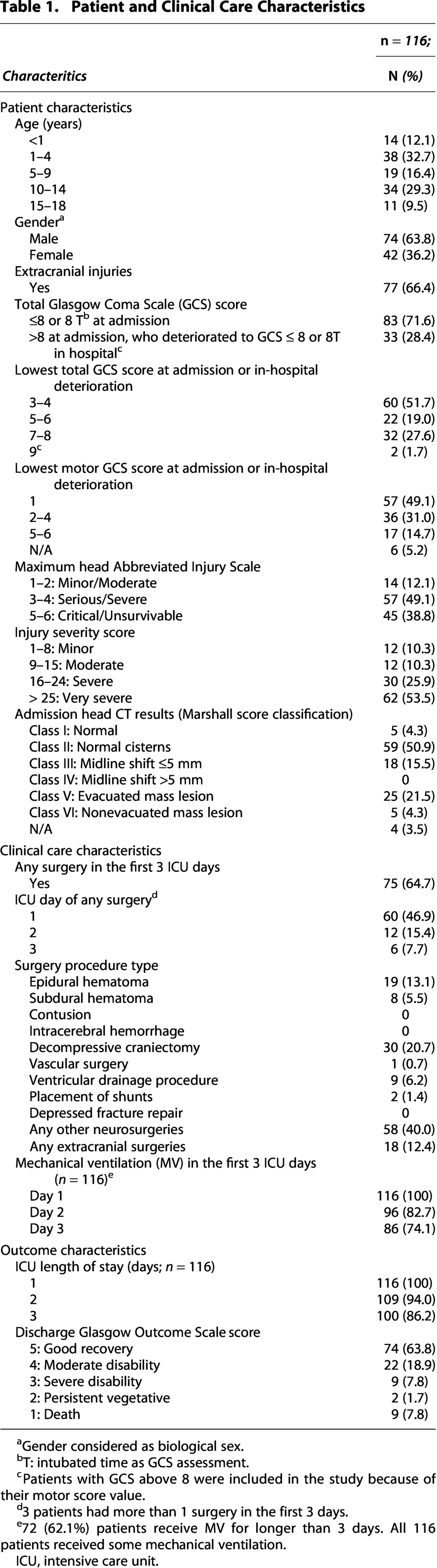
Eighty-three (71.6%) patients had GCS ≤ 8 at admission, 60 (51.7%) patients had the lowest total admission or deterioration GCS 3–4, and 57 (49.1%) patients had deterioration to motor GCS score 1. Fifty-seven (49.1%) patients had maximum head AIS 3–4, 63 (52.5%) patients had ISS > 25, and 59 (50.9%) patients had Class II Marshall score. Surgical procedures were performed in 75 (64.7%) patients, with neurosurgical interventions accounting for 87.6%. Seventy-four (63.8%) patients achieved good recovery at hospital discharge (Table 1).
Patient and Clinical Care Characteristics

Gender considered as biological sex.
T: intubated time as GCS assessment.
Patients with GCS above 8 were included in the study because of their motor score value.
3 patients had more than 1 surgery in the first 3 days.
72 (62.1%) patients receive MV for longer than 3 days. All 116 patients received some mechanical ventilation.
ICU, intensive care unit.
Ten of 16 sites (62.5%) were children’s only hospitals. Each site had a mean of 7 (median 5.5) ICU beds. Eight sites (50%) reported having one bed per full-time attending intensivist, and four (25%) had two beds per intensivist. None of the sites reported a 1:1 nurse-to-patient ratio, and 14 (87.6%) sites reported 1:2 (Table 2).
Hospital Characteristics
Full-time attending intensivists employed by the hospital.
ICU, intensive care unit; SD, standard deviation; ICP, intracanial pressure; IQR, Interquartile range.
Cumulative 3-day ICU overall guideline adherence rate
Across all patients and all guideline-specific recommendations, the overall cumulative 3-day ICU guideline adherence rate was 81.3% (SD: 13.0). Adherence to the recommendation to avoid corticosteroids was 100%, resulting in no patients with an overall guideline adherence rate of zero.
Guideline adherence rate by guideline characteristics
Of the three guideline categories, adjusted by site and across all patients, guideline adherence to thresholds was higher than either the monitoring or treatment category (Table 3). Four recommendations (corticosteroids, seizure prophylaxis, intracanial pressure (ICP) monitoring, neuroimaging) contributed to the calculation of 3-day cumulative guideline adherence in all 116 (100%) patients (Fig. 1). For 116 patients, guideline adherence rates considered a range of 6–13 applicable recommendations, reflecting the three prespecified options (adherent, not adherent, and not applicable; Table 3).

Proportion of 116 patients with nonadherence versus some patient-level 3-day cumulative intensive care unit traumatic brain injury guideline adherence rate, by guideline recommendations and recommendation categories.
After further excluding the steroids recommendation (100% adherence rate), nonadherence was observed across all three guideline categories and 14 recommendations, with a mean nonadherence rate of 35.5% (range 1.72–100). The four leading recommendations with >75% nonadherence were decompressive craniectomy (n = 50; 76%), CSF drainage (n = 37; 78.4%), hypothermia (n = 36; 100%), and advanced neuromonitoring (n = 5; 100%) (Fig. 1). One hundred four (98%) patients had nonadherence to at least one guideline recommendation, and 95 (81%) patients had nonadherence to 1–3 recommendations (Fig. 2). Twelve patients received 100% guideline-adherent care to their individually applicable recommendations.
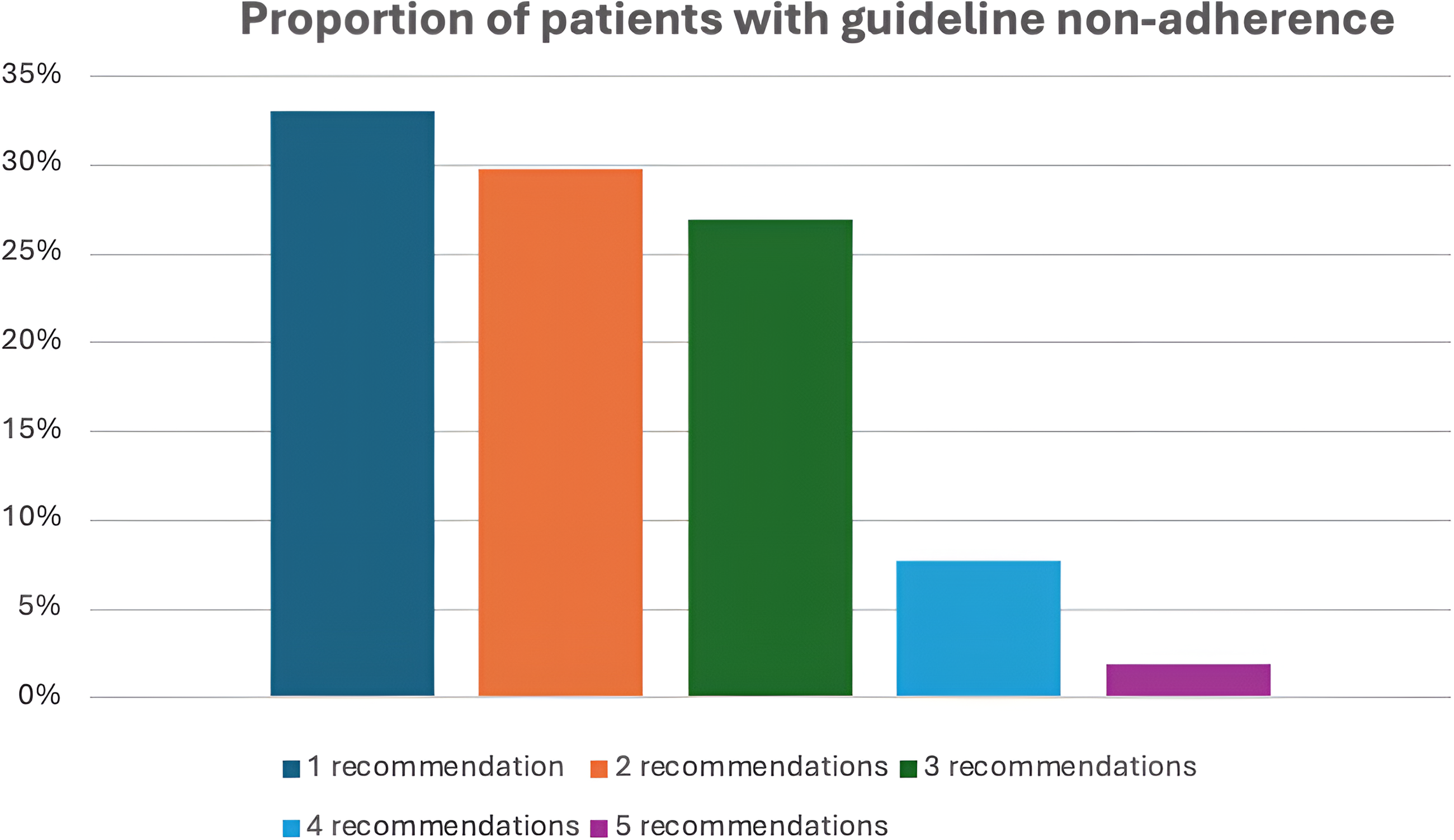
Patient-level 3-day cumulative ICU traumatic brain injury guideline adherence rate, by proportion of 116 patients with guideline nonadherence (0% guideline adherence rate) for 1 or more of individually applicable (range 6–13) guideline recommendations. *12 patients (10.34%) were either partially or fully adherent to all applicable recommendations, and hence are not included in the figure. ICU, intensive care unit.
Overall and category level guideline adherence rate by patient and clinical care characteristics
Adherence to the guideline recommendation categories did not vary by age group but adherence to the threshold category was higher in the 10- to 14-year group than in the 1–4 group (Table 4), which remained significant after adjusting for site clustering. The guideline adherence rate to the monitoring category varied significantly among those 1–4, 5–9, and 15–18 years, but was no longer significant after adjusting for site. Adherence to the treatment category did not vary by group. Gender and extracranial injury did not demonstrate differences of guideline adherence to any of the categories tested (Table 4).
Patient-Level 3-Day Cumulative Intensive Care Unit Traumatic Brain Injury Guideline Adherence Rate for Guideline Categories, by Patient and Clinical Care Characteristics
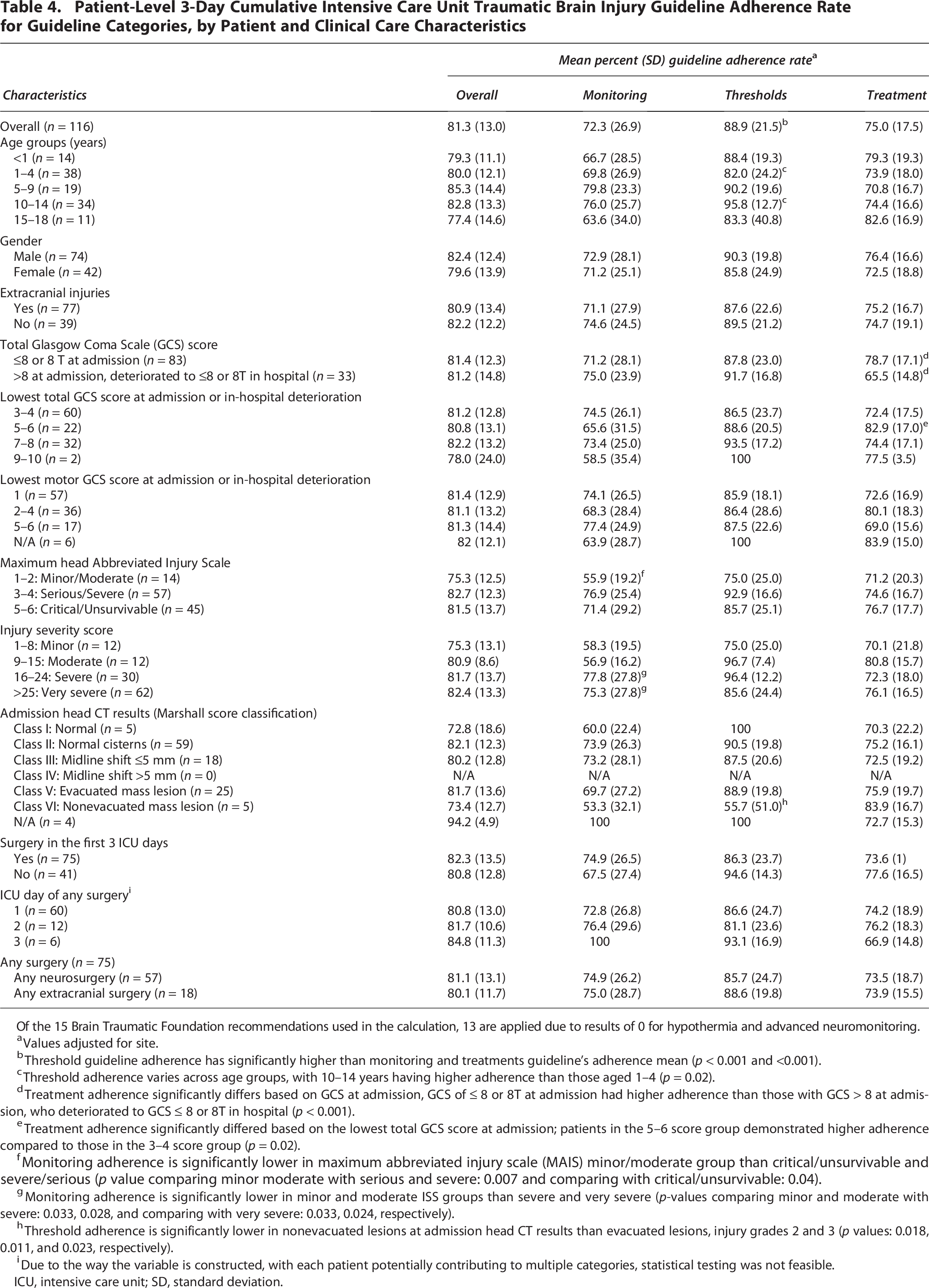
Of the 15 Brain Traumatic Foundation recommendations used in the calculation, 13 are applied due to results of 0 for hypothermia and advanced neuromonitoring.
Values adjusted for site.
Threshold guideline adherence has significantly higher than monitoring and treatments guideline’s adherence mean (p < 0.001 and <0.001).
Threshold adherence varies across age groups, with 10–14 years having higher adherence than those aged 1–4 (p = 0.02).
Treatment adherence significantly differs based on GCS at admission, GCS of ≤ 8 or 8T at admission had higher adherence than those with GCS > 8 at admission, who deteriorated to GCS ≤ 8 or 8T in hospital (p < 0.001).
Treatment adherence significantly differed based on the lowest total GCS score at admission; patients in the 5–6 score group demonstrated higher adherence compared to those in the 3–4 score group (p = 0.02).
Monitoring adherence is significantly lower in maximum abbreviated injury scale (MAIS) minor/moderate group than critical/unsurvivable and severe/serious (p value comparing minor moderate with serious and severe: 0.007 and comparing with critical/unsurvivable: 0.04).
Monitoring adherence is significantly lower in minor and moderate ISS groups than severe and very severe (p-values comparing minor and moderate with severe: 0.033, 0.028, and comparing with very severe: 0.033, 0.024, respectively).
Threshold adherence is significantly lower in nonevacuated lesions at admission head CT results than evacuated lesions, injury grades 2 and 3 (p values: 0.018, 0.011, and 0.023, respectively).
Due to the way the variable is constructed, with each patient potentially contributing to multiple categories, statistical testing was not feasible.
ICU, intensive care unit; SD, standard deviation.
Adherence to the treatment category was higher in patients with admission GCS ≤ 8 than in patients who deteriorated during hospitalization, even after site-level adjustment. Differences in adherence to the treatment category were observed between the 5–6 and 3–4 lowest total GCS groups, as well as between the 5–6 and 2–3–4 lowest motor GCS groups but only lowest total GCS groups differences were significant after site-level adjustment. Overall, other categories did not differ by GCS (Table 4).
Adherence to the monitoring category was lower in the head AIS minor/moderate group than in the head AIS severe/serious and critical/unsurvivable groups, regardless of site-level adjustment. Overall and other categories did not differ by head AIS (Table 4). Adherence to the monitoring category was higher in severe and very severe groups than in minor and moderate; however, no significant differences were observed between very severe and severe after adjusting for site. Threshold adherence was also higher in the very severe group than the severe group, this difference was not significant post adjustment. Overall, other categories did not differ by ISS (Table 4). As for CT scoring systems, adherence to the thresholds category was lower in the nonevacuated lesions group (VI) than in evacuated lesions (V) and injury grades II and III, regardless of site-level adjustment. Overall, other categories did not differ by Marshall score (Table 4).
Regardless of site-level adjustment, surgery presence, or surgery type, it was not associated with adherence rate to guideline category or overall guideline adherence (Table 4). Daily overall and treatment recommendation adherence rates varied across ICU days, with the highest on day 3 (Fig. 3). Guideline adherence for overall, monitoring, threshold, and treatment categories by hospital characteristics is presented in Table 5, but not tested for small sample size.
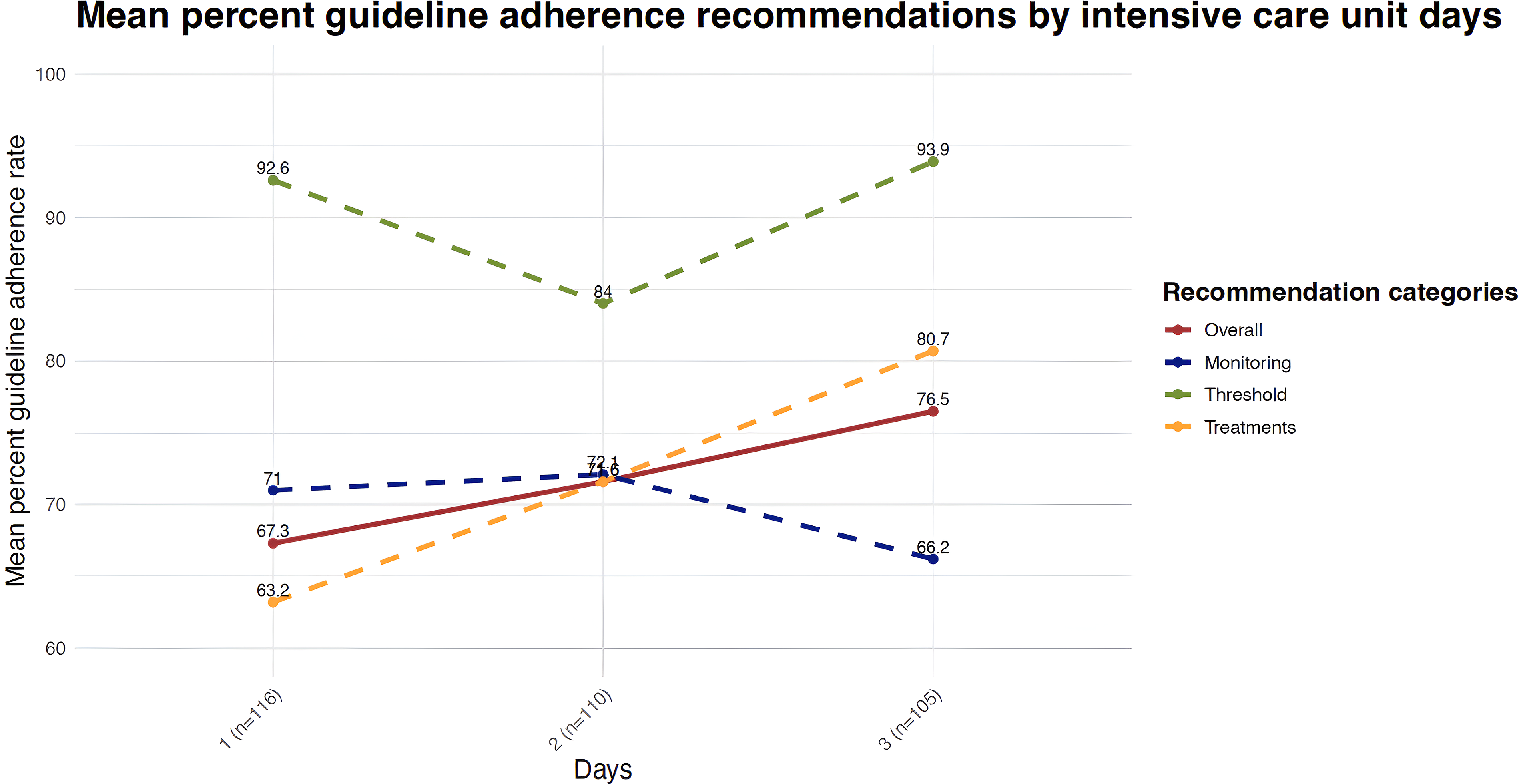
Daily patient-level intensive care unit traumatic brain injury mean percent guideline adherence rate for guideline categories, by intensive care unit days. Day 1 SD: 67.3 (46.9), 71.0 (29.5), 92.6 (21.6), and 63.2 (18.5). Day 2 SD: 71.6 (45.1), 72.1 (32.5), 84.0 (33.4), and 71.6 (20.8). Day 3 SD: 76.5 (42.4), 66.2 (33.2), 93.9 (19.1), and 80.7 (17.8).* *Overall adherence on day 1 was significantly lower than on days 2 and 3 (p value 0.03 and <0.01, respectively).* *Treatment adherence was significantly higher on days 2 and 3 compared to the previous days (p value < 0.01). SD, standard deviation.
Patient-Level 3-Day Cumulative Intensive Care Unit Traumatic Brain Injury Guideline Adherence Rate for Guideline Categories, by Hospital Characteristics for Specific Recommendations with Greater Than 0% Guideline Adherence Rate
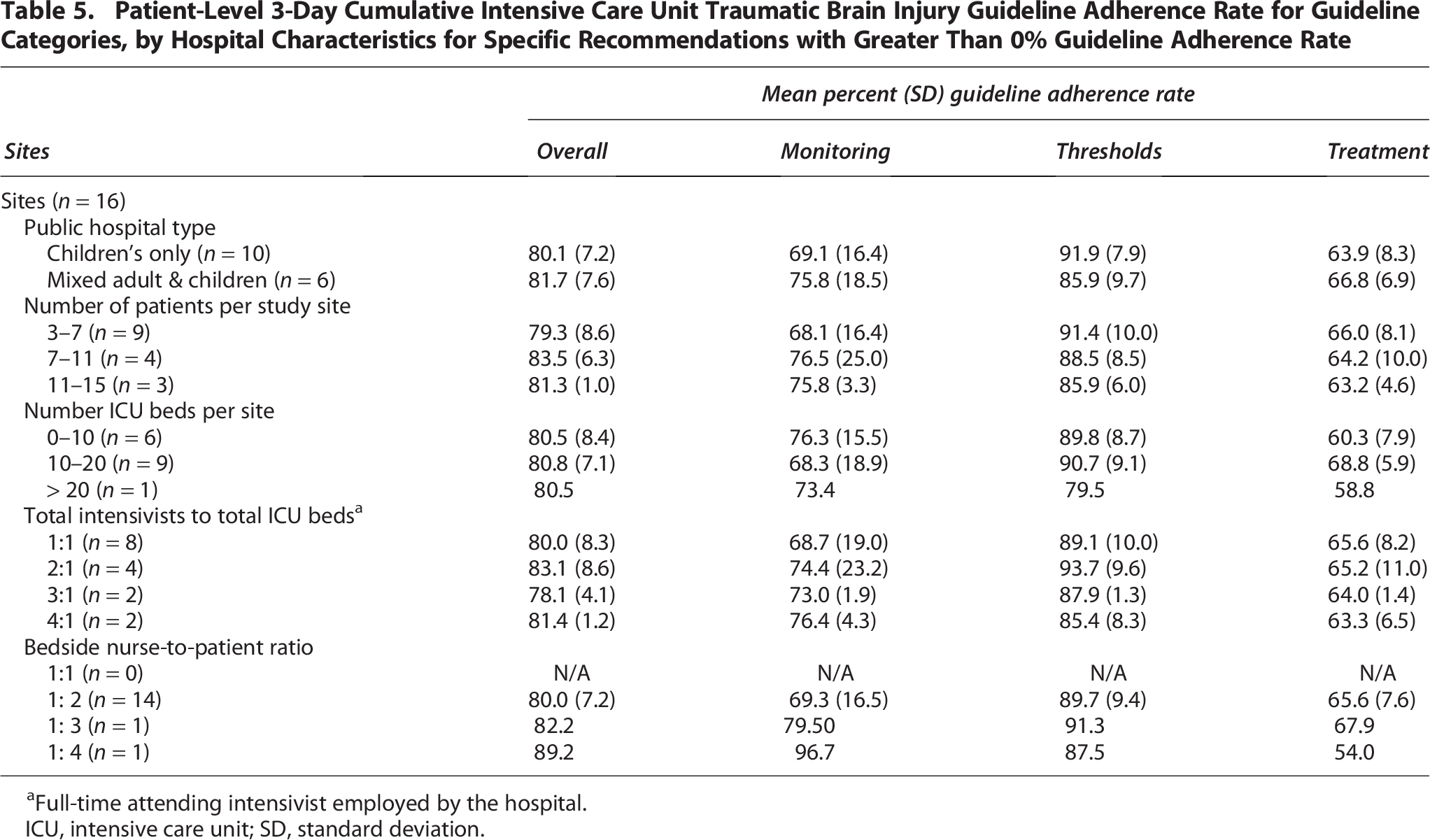
Full-time attending intensivist employed by the hospital.
ICU, intensive care unit; SD, standard deviation.
Discussion
We evaluated differences in achieving adherence to TBI guidelines during the first 3 days of ICU care by guideline category, specific guideline recommendation, and patient and clinical care factors in severe pediatric TBI. Main findings were: (1) overall guideline adherence exceeded 80%; (2) guideline adherence rates varied between guideline categories, by specific recommendations, and by some patient characteristics (age group, GCS, AIS, ISS, and Marshall CT); (3) nonadherence to some guideline recommendations commonly occurred, most often for craniectomy, CSF drainage, hypothermia, and advanced neuromonitoring; and (4) most patients were nonadherent to 1–3 applicable recommendations: most commonly decompressive craniectomy, hypothermia, neuromonitoring, ICP monitoring, seizure prophylaxis, and nutrition. This work identifies opportunities to improve early ICU guideline adherence rates after severe TBI. While most of the evidence that went into developing the BTF guidelines is from North America, many non-US geographic contexts may utilize these BTF recommendations as a reference for evidence-based practice. Studying guidelines developed in one context in another affords the opportunity to examine generalizability, feasibility, and effectiveness. This study provides new information on the degree to which the participating sites were adherent to the BTF guidelines. While outcomes may be favorable in non-US hospitals, care practices in one socioeconomic setting may or may not apply to another. This study helps us understand the degree to which there are similarities.
The overall guideline adherence rate was high, but our study identified areas for improvement.5,11 For example, since not all surgery is urgent/emergent, assumptions regarding the ability to achieve guideline adherence in surgical patients and in patients with coexisting treatments such as mechanical ventilation that may be associated with the timing and nature of other TBI care treatments may not be valid. Additionally, patient, hospital, and clinical care factors may variably impact provider delivery of guideline-based care. The variability in ICU guideline adherence, including nonadherence for some specific recommendations and categories, may reflect unwanted variation or lack of feasibility to achieve adherence, or controversies in early critical care for the recommendations being examined.
Except for the guideline recommendation to not use corticosteroids (100% adherence), guideline-based care was generally provided for the other 14 recommendations, and the range of nonadherence to recommendations was small (1–5 recommendations) and mostly for only 1–3 recommendations. Yet, all patients had nonadherence to at least one guideline recommendation. This observation suggests that redressing barriers to increasing guideline adherence may be feasible, and focusing on increasing guideline adherence rates for a few specific recommendations may improve overall guideline adherence rates early after severe pediatric TBI. Local observations should drive these focused efforts to reduce guideline nonadherence.
Of the specific 14 guideline recommendations with nonadherence, overall adherence was lowest for decompressive craniectomy, analgesics/sedatives/neuromuscular blockade, CSF drainage, and ICP monitoring. No patient achieved adherence to hypothermia and neuromonitoring recommendations, but the availability of these interventions was limited. These observations suggest that not all recommendations have the same evidentiary basis or feasibility to increase adherence.12–14 For example, it may be easier to adhere to select BTF guideline recommendations, such as cerebral perfusion pressure and nutrition. 2 The decision to use decompressive craniectomy as a treatment always requires neurosurgery leadership. Although CSF drainage contributes to improving adherence to other recommendations, such as ICP management, CSF drainage effectiveness is controversial in TBI care.15,16
Overall, TBI guideline adherence varied across guideline categories. Adherence to threshold category guidelines was higher than adherence to monitoring and treatment categories. These findings suggest that the use of threshold recommendations may depend on whether monitoring recommendations are followed, which in turn supports the appropriate application of BTF threshold-based guidance.
At the patient level, guideline adherence across categories varied among patient admission GCS and other injury severity measures. Results suggest that focus on improving adherence to recommendations in patients with less severe injuries and those who deteriorate during hospitalization may enhance overall early guideline adherence. Overall, treatment adherence rates were highest on ICU day 3, suggesting that enhancing early adherence may improve patient outcomes. None of our patients had a Marshall CT classification Class IV, and since patients with midline shift >5 mm are more likely to undergo surgery for evacuation, these patients were considered Class V. Patients with nonevacuated lesions (Class VI) showed the lowest adherence to the thresholds category. The presence of a nonevacuated lesion may reflect a clinical decision regarding its diagnostic and treatment necessity or the availability of alternative treatments.
Our findings did not reveal significant differences in overall guideline adherence or adherence within specific categories based on sex or the presence of extracranial injuries. We observed that adherence to the thresholds category varied by age group, with patients 1–4 years, achieving the lowest adherence rates, suggesting a need to focus efforts on improving guideline adherence rates in younger children. In this study, clinical care characteristics were not associated with guideline adherence. Our data suggest that early ICU guideline adherence may be influenced by hospital characteristics. Previous literature shows that a better nurse-to-patient ratio is associated with better outcomes. 17 For example, the American Academy of Pediatrics recommends a 1:1 nurse-to-patient ratio in critical care. 18 Most of our South American hospitals operated with a bedside nurse-to-patient ratio of 1:2, reflecting local health care delivery patterns that should be considered when measuring guideline adherence rate improvement efforts in various health care delivery contexts.
This study has some limitations and strengths. The guidelines are not all based on strong evidence, and the recommendations of the guidelines are not necessarily broad in scope. There may be factors important to guideline adherence that are not represented in our data collection. The sample size is modest, precluding definitive conclusions regarding findings from subgroups, which limit our analyses to describing patterns and performing univariate comparisons for our main outcomes. Additionally, hyperosmolar therapy is a conditional component of ICP treatment, so its inclusion may result in double counting within adherence metrics. The study is from one geographic region in several countries in South America. While this might limit generalizability, guideline adherence rates were high. We benchmarked ICU care in South America against the BTF recommendations, largely derived from North American and European evidence; some recommendations such as advanced neuromonitoring may not have been available for evaluation. This study was possible because we collected data for one year prior to launching the Pediatric Guideline Adherence and Outcomes (PEGASUS) randomized controlled trial.8,19
In conclusion, we provide new information on achieving early severe TBI ICU guideline adherence from pediatric ICUs in South America by guideline, patient, and clinical care characteristics. Results identify areas for future study and evaluation of strategies to improve early ICU guideline adherence, especially for young children and those who are admitted to the hospital who then deteriorate. Local identification of those BTF guideline recommendations that are feasible to benchmark as key performance indicators and tailoring strategies to optimize achieving high guideline adherence rates across geographic contexts is warranted.
Transparency, Rigor, and Reproducibility Summary
The primary study was registered at clinicaltrials.gov (NCT03896789). This secondary data analysis was not separately registered. The sample size of 116 subjects included in this analysis was based on the number of eligible patients admitted to the study sites during the preimplementation baseline stage (September 1, 2019, to July 13, 2020, prior to site randomization to primary intervention) and patients who consented to data collection of usual care indicators. Data were extracted from medical records. Overall, 127 potential participants were screened, and 116 were consented to data collection (five patients rejected consent and six died between screening and completion of the consent process). This data analysis used deidentified data and selected indicators relevant to the analyses. Investigators did not have access to participant codes linking to identifying information. No individual patient analyses were done. R/R Studio was used for all analyses. The key inclusion criteria and outcome evaluations are established standards. The indicators, deidentified data, and analytic code used in this analysis may be requested from the authors. The full data set for the research study will be made available in FITBIR (https://fitbir.nih.gov) after the associated primary outcome article is published.
PEGASUS Argentina Study Group Members
Silvina Ábalos, Mariela Alassia, Marianella Altamirano, Julieta Aranda, Anahí Natalia Aybar, Ma. Eugenia Baitaij, Sabrina Bollada, Rodrigo Burgos Pratx, Pablo Castellani, Sandra Chuchuy, Karina Cinquegrani, Carlos Dávila, Alejandra Depetris, Adriana Diettes, Fernando Español, Daniel Giordano, Natalia Gómez Arriola, Janessa Graves, María Virginia Leguina, Noelia López, Gabriela López Cruz, Claudia Lutkevicius, Alejandro Mansur, Ivana Marinelli, Paula Medici, Manuel Nogueira, Silvia Oliveri, Jessica Constanza Pedraza Coronel, Matías Penazzi, Andrea Piccirilli, Wildo Pino, Fernanda Podestá, Graciela Romero, Ernesto Sauer, Ariel Segado, Karen Segar, Marcelo Sorbo, Jin Wang, Bryan J. Weiner.
Authorship requirements have been met, and all authors have made substantial contributions to the conception and design of the study, acquisition of data, and/or analysis and interpretation of data. All authors have approved the final version of the article and take responsibility for its contents.
Authors’ Contributions
M.M.R.: Methodology, formal analysis, visualization, and writing original draft. J.V.: Methodology, project administration, data curation, and writing original draft. C.M.: Methodology, writing, review, and editing. N.G.: Project administration, investigation, data curation, writing review, and editing. S.L. and G.P.: Conceptualization, resources, investigation, writing, review, and editing. M.J.B.: Conceptualization, funding acquisition, writing, review, and editing. M.S.V.: Conceptualization, methodology, funding acquisition, supervision, and writing original draft. PEGASUS Argentina Study Group: Investigation, resources, writing, review, and editing.
Footnotes
Author Disclosure Statement
The authors have no competing interests to disclose.
Funding Information
This article is part of research funded by the National Institutes of Health
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.